
Abstract
Purpose
The aim of this study was to evaluate the same kidney before and after transplantation to assess the ability of the allograft to restore blood flow, time required to achieve functional recovery after surgery and the possibility of differentiating normal from pathological allografts using color Doppler ultrasound (CDUS) flow indices: resistive index (RI)/renal cortical ratio (RCR) and scintigraphy.
Materials and methods
79 living donors and 79 recipients. Donors underwent renal CDUS and scintigraphy. CDUS was repeated on the allograft 24 h, 3, 15 and 30 days after transplantation, and scintigraphy 3–5 days after transplantation. Recipients were divided into two groups on the basis of clinical and biochemical values: (A) well-functioning allografts and (B) acute pathology. Results of CDUS, RI and RCI were compared to results of scintigraphy, biochemical values and biopsy.
Results
Group (A) n = 60 (76 %), group (B) n = 19 (24 %); RI sensitivity was 93 %, specificity 83 %. In group (A) positive predictive value (PPV) was 94 % and in group (B) 90 %. RCR using receiver operating characteristic curve analysis yielded sensitivity 100 % and specificity 98.3 %. Scintigraphy mean values of glomerular filtration ratio and T max before transplantation were in group (A): 50.32 ml/min and 4.87 min; after transplantation 46.88 ml/min and 4.96 min; in group (B): 48.68 ml/min and 4.63 min, after transplantation 27.89 ml/min and 10.53 min, respectively. Pearson’s correlation coefficient between preoperative and postoperative results of scintigraphy was significant in group (A) (glomerular filtration ratio = 0.85, T max = 0.70) and not significant in group (B) (glomerular filtration ratio = 0.40, T max = 0.08).
Conclusion
This study shows that CDUS, RI and RCR are useful in postoperative evaluation of transplanted kidneys as these parameters can, after only 24 h, confirm the good condition of the allograft despite still excessive blood parameter values.
Riassunto
Scopo
Scopo di questo studio è stato di valutare lo stesso rene prima e dopo il trapianto al fine di valutare la capacità dell’organo trapianto di ripristinare il flusso sanguigno, il tempo richiesto per raggiungere il recupero funzionale dopo l’intervento chirurgico e per differenziare nell’innesto il tessuto normale dal patologico con l’uso degli indici di flusso del color Doppler (CD): l’indice di resistenza (IR)/renal cortical ratio (RCR) e la scintigrafia.
Materiali e Metodi
79 donatori viventi e 79 riceventi. I donatori sono stati sottoposti a CD renale e a scintigrafia. Il CD è stato ripetuto sul tessuto trapiantato 24 ore, 3, 15 e 30 giorni dopo il trapianto e la scintigrafia, 3-5 giorni dopo il trapianto. I pazienti sono stati divisi in due gruppi sulla base dei dati clinici e biochimici: A) trapianto ben funzionante e B) patologia acuta. I risultati del CD, IR e RCR sono stati confrontati con i risultati della scintigrafia, i valori biochimici e la biopsia.
Risultati
Gruppo A) n = 60 (76 %), gruppo B) n = 19 (24 %); la sensibilità del IR è stata del 93 %, la specificità del 83 %. Nel gruppo A) il valore predittivo positivo (VPP) è stato: 94 %, gruppo B): 90 %. Utilizzando una analisi delle curve ROC (Receiver Operating Characteristic) lo RCR ha prodotto una sensibilità del 100 % e una specificità del 98,3 %. I valori medi della scintigrafia del rapporto di filtrazione glomerulare e T max prima del trapianto nel gruppo A): 50.32 ml/min e 4.87 min; dopo trapianto 46.88 ml/min e 4.96 min; nel gruppo B): 48.68 ml/min e 4.63 min, dopo trapianto di 27,89 ml/min e 10.53 minuti, rispettivamente. Il coefficiente di correlazione di Pearson tra i risultati preoperatori e postoperatori della scintigrafia è stato significativo nel gruppo A) (rapporto di filtrazione glomerulare = 0,85, T max = 0,70) e non significativa nel gruppo B) (rapporto di filtrazione glomerulare = 0.40, T max = 0,08).
Conclusione
Questo studio dimostra che CD, IR e RCR sono utili nella valutazione postoperatoria dei reni trapiantati in quanto tali parametri possono, dopo solo 24 ore, confermare la buona condizione del tessuto trapiantato nonostante i valori ematochimici ancora alterati.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Perfusion of a renal allograft may be different from perfusion of the same organ in the living donor, as numerous physical and physiological factors affect the perfusion during and after transplantation. Renal vascularity is characterized by a duplex system of closely connected capillaries. The glomerular and peritubular capillaries situated around the renal arteries and renal veins as well as the hemodynamic conditions of the micro circle have an important role in the regulation of ultrafiltration and fluid reabsorption [1].
Color Doppler US (CDUS) and scintigraphy cannot evaluate the exact volume of perfusion, but they show blood flow and perfusion changes, which may be a sign of allograft dysfunction. These techniques are therefore frequently used in the assessment of allograft hemodynamics, not only in the presence of symptoms indicating acute pathology (allograft rejection, acute tubular necrosis, cyclosporine intoxication, renal vessel thrombosis) but also in the follow-up of normally functioning allografts [2–4]. The first days after transplantation are usually crucial.
The aim of this study was to evaluate the same kidney before transplantation in the living donor and after transplantation in the recipient to assess possible perfusion changes, the ability of the allograft to restore blood flow, time required to achieve functional recovery after surgery and the possibility of differentiating normal from pathological allografts at an early stage using CDUS, RI and RCR. CDUS outcome was then compared to results of scintigraphy, biochemical parameters and biopsy [5].
Materials and methods
A total of 79 living donors, 32 males and 47 females, mean age 43 years (range 30–55 years), were enrolled in this study. The donors underwent standard selection procedures and clinical biochemical examinations as well as diagnostic examinations.
Ethical approval for this study was granted by the Medical Research Ethics Committee of our university, and informed consent was obtained from all donors and recipients.
Of the 79 recipients, 51 were males and 28 females, mean age 45 years (range 32–54 years). All recipients were first transplantated; patients with surgical or urological complications were excluded from this study.
Before surgery, both donor kidneys were evaluated with CDUS and scintigraphy. CDUS was repeated on the allograft 24 h, 3, 15 and 30 days after transplantation, and scintigraphy was performed 3–5 days after transplantation.
The following clinical parameters were evaluated: general condition, blood pressure and daily urine output. Biochemical parameters: plasma creatinine, blood urea nitrogen, creatinine clearance, fractional excretion of sodium (FENa), plasma cyclosporine (normal value in the first month 600–800 ng/ml) and plasma tacrolimus (normal value in the first month 6–9 ng/ml).
After transplantation, the patients were divided into two groups on the basis of clinical and biochemical values: (A) well-functioning allografts and (B) acute pathology.
In all donors and recipients, CDUS was performed on the renal artery, interlobar artery and arcuate artery. The following parameters were studied: blood flow resistive index (RI) (cut-off 0.70) and renal cortical ratio (RCR).
RCR is defined as the RI value variation, expressed in percentage:
RCR1 = (RIra − RIia)/RIra × 100
RCR2 = (RIia − RIaa)/RIia × 100
RIra = RI in the renal artery, RIia = RI in the interlobar artery, RIaa = RI in the arcuate artery.
All CDUS examinations were performed on ATL 5000 HDL (Philips, USA) and Technos (Esaote Biomedica, Italy) using convex 3.5 MHz and linear 7.5 MHz probes. CDUS was performed with scanning parameters set for maximum sensitivity to the flow velocities at the different levels, while power output was increased to maximum. Color gain was increased until just prior to the appearance of random noise. The pulse repetition frequency was set at the lowest possible level. Multiple axial, longitudinal and oblique scans were used to sample the renal artery and its branches (interlobar and arcuate artery) at different levels (renal poles, mid kidney and hilum). In order to study the arcuate artery with the best efficiency, a 7.5 MHz probe was used with the maximum possible magnification of renal cortex. Renal vein and artery were also assessed to exclude the presence of thrombosis or stenosis.
Renal scintigraphy with 99mTc-DTPA was performed using a large field-of-view digital gamma camera (G.E. Millennium) equipped with a low-energy all-purpose collimator. Dynamic acquisitions of the renal area were carried out in posterior view (4 frame/s for 1 min and 100 frame/s for 24 min). Elaboration of scintigraphic data was carried out using Gates algorithm. Glomerular filtration rate (GFR) and time of maximum tracer uptake (T max) were assessed for the purpose of the study. The following values were considered as normal: GFR ≥ 40 ml/min in women, GFR ≥ 50 ml/min in men, and maximum accumulation time of the nephrographic curve (T max) ≤ 6 min independently of gender. Scintigraphic studies with 99mTc-DTPA were repeated in the recipients 3–5 days after surgery, and the outcome was compared to preoperative results (GFR, T max).
Biopsy was performed in all patients with acute pathologies. Histopathological examination and staging of the allografts were performed according to the BANFF classification system.
Statistical analysis
RI values were expressed as mean values ± SD. Flow-metric indices pertaining to each group were compared using the two-tailed Student’s t test to evaluate statistical significance of correlation between RI values and the patients’ clinical condition.
RCR was calculated as well as statistical significance related to each group and the explored vascular area. PPV was calculated for each group.
RI ratio was calculated by dividing preoperative renal artery RI values and by postoperative renal artery RI values measured 24 h, 3, 15 and 30 days after transplantation. The RI ratios obtained in the two groups were compared using the Student’s t test. To evaluate the utility of RI ratios in predicting development of acute pathology after transplantation, receiver operating characteristics (ROC) analysis was applied. The areas under the curve were calculated. Cut-off values for RI ratio were determined to identify patients who would develop acute pathology. Sensitivity and specificity with 95 % confidence intervals (95 % CI) were calculated. Pearson’s correlation coefficient was carried out on the scintigraphic data to compare GFR and T max values of the kidney before and after transplantation.
Results
On the basis of clinical and biochemical results, the 79 recipients were divided into two groups: (A) well-functioning allografts n = 60 (76 %) and (B) acute pathology n = 19 (24 %).
In group (A), mean creatinine serum level 24 h after transplantation was 9.02 ± 1.17 mg/dl and FENa was 1.43 ± 1.16 %. In group (B), mean creatinine serum was 11 ± 1.23 mg/dl and FENa was 1.66 ± 0.58 % (Table 1).
RI
Analysis of RI values was performed in the donors before surgery and in the recipients 24 h, 3, 15 and 30 days after transplantation.
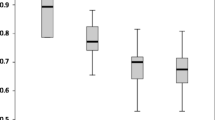
In the donors, RI mean values were renal artery 0.67 ± 0.02, interlobar artery 0.65 ± 0.03, arcuate artery 0.61 ± 0.06. Twenty-four hours after transplantation, RI mean values measured on the renal allografts in group (A) (well-functioning grafts) were renal artery 0.69 ± 0.03, interlobar artery 0.64 ± 0.03, arcuate artery 0.60 ± 0.04, whereas RI mean values obtained in group (B) (acute pathology) were renal artery 0.78 ± 0.07, interlobar artery 0.79 ± 0.07, arcuate artery 0.77 ± 0.07. The mode value obtained in group (B) was near cut-off value 0.70 (renal artery 0.74, interlobar artery 0.72 and arcuate artery 0.71).
On the third day, the difference between the two patient groups became more evident, and this trend was confirmed at follow-up examinations after 15 and 30 days (Table 2).
Sensitivity of RI was 93 % and specificity 83 %. PPV in group (A) was 94 % and in group (B) 90 %.
RCR
Analysis of RI values was performed according to the RCR concept. In group (A), RI values decreased by 3.5 % from the renal artery to the interlobar artery and by 2 % from the interlobar artery to the arcuate artery. Group (B) (acute pathology) showed a decrease of 1.2 % from the renal artery to the interlobar artery and a further decrease of 1.2 % from the interlobar artery to the arcuate artery.
PPV of RCR in group (A) was 100 % and in group (B) 98 %. These values were confirmed during the follow-up.
Statistical analysis of RCR values using the Student’s t test evidenced the usefulness of this method for differentiating the two groups (p ≤ 0.0001 for all arteries). Student’s t test performed on both groups to evaluate the significance of RI values measured on each vessel showed a high statistical significance in group (A) (well-functioning), while significance was lower in group (B) (acute pathology), where the RI curve tended to be flat .
On day three, the RCR values presented a difference between the two patient groups, and this trend was confirmed at follow-up examinations after 15 and 30 days.
ROC analysis revealed an Az value of 0.91. Using a cut-off value of 1.051, prediction of acute pathology reached a sensitivity of 100 % (95 % CI = 83.2–100 %) and a specificity of 76.7 % (95 % CI = 64.6–85.6 %). Twenty-four hours after transplantation, mean RI ratios in groups (A) and (B) were 1.03 ± 0.05 and 1.15 ± 0.06, respectively (p < 0.0001; Student’s t test). On the third day after transplantation, mean RI ratios in groups (A) and (B) were 0.99 ± 0.08 and 1.2 ± 0.08, respectively (p < 0.0001; Student’s t test). ROC analysis revealed an Az value of 0.99. Using a cut-off value of 1.09, prediction of acute pathology reached a sensitivity of 100 % (95 % CI = 83.2–100 %) and a specificity of 98.3 % (95 % CI = 91.1–99.7 %) (Table 3).
Scintigraphy
Scintigraphic results are shown in (Table 4). In group (A), mean values and standard deviations of GFR and T max before transplantation were 50.32 ± 3.82 ml/min and 4.87 ± 0.35 min, respectively. After transplantation, the values were 46.88 ± 4.7 ml/min and 4.96 ± 0.31 min, respectively. In group (B), mean values and standard deviations of GFR and T max before transplantation were 48.68 ± 2.85 ml/min and 4.63 ± 0.33 min, respectively; after transplantation 27.89 ± 3.52 ml/min and 10.53 ± 2.24 min, respectively. There was no statistically significant difference between scintigraphic parameters before and after transplantation.
Discussion
At transplantation, the kidney is inserted into a completely different circulatory, hemodynamic and humoral environment. The recipient usually has higher blood pressure and higher biochemical values than the healthy donor. In order to restore these values to normal level, the allograft is overburdened with filtration and reabsorption immediately after transplantation. A self-regulating mechanism re-establishes the perfusion and allows the well-functioning allograft to maintain the filtration flow, which almost immediately restores the excretory functions [6].
Early recognition of transplantation dysfunction is a crucial problem in the management of renal transplantation. In this study, CDUS follow-up was carried out 24 h, 3, 15 and 30 days after transplantation. It should be pointed out that all recipients were receiving triple therapy of steroids, mycophenolate and cyclosporine or tacrolimus.
A first differentiation between well-functioning and pathological allografts was made on the basis of clinical data. However, particularly in the first 24 h after transplantation, creatinine and FENa values are high, also in well-functioning allografts [7]. At the second follow-up, the recipients in both groups presented higher serum creatinine levels, urea nitrogen and FENa values and higher blood pressure than the donors due to pre-existing renal insufficiency. At the third follow-up, these values were still high although they were tending towards normality in all recipients, and at the 30-day follow-up values were nearly normal. This happened for two different reasons: in group (A) because the allografts were well-functioning; in group (B) because the therapy was effective. Group (B) patients who did not respond to therapy eventually underwent repeated transplantation.
Gray-scale US and CDUS are valid tools in the diagnosis of vascular, urological and surgical complications. However, data concerning the value of CDUS in the diagnosis of parenchymatous renal allograft dysfunctions are controversial, because these pathologies often occur concomitantly appearing mainly as glomerular–tubular damages and vascular lesions [8–10].
In the literature, the use of CDUS flow indices is reported mainly in the study of renal diseases [peak systolic velocity (PSV), pulsatility index (PI) and RI] [11].
During transplantation, the kidney is exposed to different circulatory conditions and this has a strong influence on the PSV, which is higher in the recipients than in the donors. PSV is a quantitative index that depends directly on the systolic jet, heartbeat and blood pressure. This parameter also seems strongly influenced by the general condition of the renal microcirculation, therefore it is not useful for defining specific allograft problems [12, 13]. In the present study PI yielded results similar to RI. For these reasons and due to the low inter-observer variability, RI was considered as the most reliable flow index [14–16].
RI values provide valid information regarding the vascular status in the explored area but not about the glomerular function and the specific pathology [4]. RI is furthermore influenced by extra-renal factors such as hypertension, heart rate and shock. For a correct evaluation of the RI data, it is therefore important to know if the patient is affected by these conditions.
In group (A) (well-functioning) our results showed that only 24 h after transplantation, RI values were similar to those measured in the donors. Statistical analysis confirmed that there was no significant difference between recipient and donor values in any of the sites of measurement (renal artery, interlobar artery and arcuate artery) as linear regression analysis showed a good correlation between the data obtained before and after transplantation.
Statistical analysis comparing RI values obtained in the donors and in the recipients furthermore showed that PPV was nearly 100 %, and already 24 h after transplantation it was, thus, possible to identify patients who would develop pathology while biochemical parameters (creatinine, urea nitrogen, FENa) were still high in both groups. Our results show that analysis of RI values obtained before and after transplantation permits distinction between normal and pathological recipients and that a well-functioning kidney can re-establish normal hemodynamic conditions within 24 h.
RI is in itself a static parameter. However, correlation between RI values obtained on the renal artery, interlobar artery and arcuate artery of the same kidney provides data for a dynamic analysis (RCR) [17, 18].
In the well-functioning allografts, RI values obtained on the renal artery and the arcuate artery decreased by 3.5 and 2 %, respectively. In acute pathologies, tissue edema, macrophages and cellular reaction affect all vessels, but the small-caliber vessels are generally the first to show the effect of this process. For this reason, the RI curve tends to become flat. In this study, 70 % of group (B) patients (acute pathology) presented RI values near the cut-off threshold of 0.70 (mode values: renal artery 0.74, interlobar artery 0.72, and arcuate artery 0.71). These values provided no valid distinction between the two groups, whereas the flat RCR curve provided early differentiation between acute pathology and normally functioning allografts [PPV in group (A) was 100 % and in group (B) 98 %]. CDUS is a non-invasive, inexpensive, fast and easily repeatable examination, which can be carried out also at the bedside.
In group (A), scintigraphic evaluation of the transplanted kidney performed 3–5 days after transplantation showed functional parameters, such as GFR and T max, similar to those obtained on the same kidney before transplantation in the donor. Results obtained in group (B) showed a significant postoperative decrease in both functional parameters. Overall, scintigraphic results were in agreement with clinical findings and confirmed data obtained at CDUS [5, 19].
The lack of variation in waveform morphology between donors and recipients confirmed the restoration of a regular low-resistance flow pattern of a normal kidney [20, 21]. CDUS evaluation of the intraparenchymal renal resistance is useful alongside the monitoring of biochemical parameters in the follow-up of normally functioning allografts. Biochemical parameters, such as serum creatinine and urea nitrogen level as well as urine output and blood pressure measurements, allow the clinician to follow the function of the allograft, but CDUS and scintigraphy permit an early evaluation of the hemodynamic self-regulation [5, 22–24]. The results of our study may lead to an extended future use of these techniques in postoperative evaluation of transplanted kidneys. In addition to this, the use of contrast-enhanced US will permit a more accurate investigation of renal transplant vascularity in line with the monitoring of other organs [25]. CDUS after only 24 h, confirms the good condition of the allograft, even if still excessive blood parameter values indicate a possible renal allograft dysfunction.
References
Falchuk KH, Brenner BM, Tadokoro M et al (1971) Oncotic and hydrostatic pressure in peritubular capillaries and fluid reabsorption by proximal tubules. Am J Physiol 220:1427–1433
Gruenewald S, Skerrett D, Dolimier D, Nankivell B (2002) Technique of color Doppler quantification of vascularity in transplanted kidneys. J Clin Ultrasound 30(3):151–157
Jimenez C, Ovidea Lopez M, Gonzalez E, Selgas R (2009) Ultrasonography in kidney transplantation: values and new developments. Transpl Rev 23:209–213
Datta R, Sandhu M, Saxena AK et al (2005) Role of duplex Doppler and power Doppler sonography in transplanted kidneys with acute renal parenchymal dysfunction. Australas Radiol 49:15–20
Gates GF (1983) Split renal function testing using Tc99m-DTPA. A rapid technique for determining differential glomerular filtration. Clin Nucl Med 8:400–406
Cherif M, Ounissi M, Karoui CT et al (2010) Short- and long-term outcomes of living donors in Tunisia: a retrospective study. Transpl Proc 42(10):4311–4313
Naqvi HN, Zafar MN, Hussain A et al (2005) Cyclosporine induced nephrotoxicity in renal transplant recipients: clinical significance of fractional excretion of sodium, potassium and magnesium. J Pak Med Assoc 55(4):161–165
Gao J, Ng A, Shih G et al (2007) Intrarenal color duplex ultrasonography: a window to vascular complications of renal transplants. J Ultrasound Med 26(10):1403–1418
Friedewald SM, Molmenti EP, Friedewald JJ et al (2005) Vascular and nonvascular complications of renal transplants: sonographic evaluation and correlation with other imaging modalities, surgery, and pathology. J Clin Ultrasound 33(3):127–139
Tarzamni MK, Argani H, Nurifar M, Nezami N (2007) Vascular complication and Doppler ultrasonographic finding after renal transplantation. Transpl Proc 39:1098–1102
Nezami N, Tarzamni MK, Argani H, Nourifar M (2008) Doppler ultrasonographic indices after renal transplantation as renal function predictors. Transpl Proc 40:94–99
Frauchiger B, Bock A, Eichlisberger R et al (1995) The value of different resistance parameters in distinguishing biopsy-proved dysfunction of renal allografts. Nephrol Dial Transpl 10:527–532
Radmehr A, Jandaghi AB, Hashemi Taheri AP, Shakiba M (2008) Serial resistive index and pulsatility index for diagnosing renal complications in the early posttransplant phase: improving diagnostic efficacy by considering maximum values. Exp Clin Transpl 6(2):161–167
Quarto di Palo F, Rivolta R, Elli A, Castagnone D (1996) Relevance of resistive index ultrasonographic measurement in renal transplantation. Nephron 73:357–370
Rodrigo E, López-Rasines G, Ruiz JC et al (2010) Determinants of resistive index shortly after transplantation: independent relationship with delayed graft function. Nephron Clin Pract 114(3):178–186 Epub 2009 Nov 28
Mehrsai A, Salem S, Ahmadi H et al (2009) Role of resistive index measurement in diagnosis of acute rejection episodes following successful kidney transplantation. Transpl Proc 41(7):2805–2807
Thalhammer C, Aschwanden M, Mayr M et al (2006) Duplex sonography after living donor kidney transplantation: new insights in the early postoperative phase. Ultraschall Med 27(2):141–145
Drudi FM, Pretagostini R, Padula S et al (2004) Color Doppler ultrasound in renal transplant: role of resistive index versus renal cortical ratio in the evaluation of renal transplant diseases. Nephron Clin Pract 98:67–72
Schwenger V, Hinkel UP, Nahm AM et al (2006) Color Doppler ultrasonography in the diagnostic evaluation of renal allografts. Nephron Clin Pract 104:107–112
Gottlieb RH, Lieberman JL, Pabico RC, Waldman DL (1995) Diagnosis of renal artery stenosis in transplanted kidneys: value of Doppler waveform analysis of the intrarenal arteries. AJR 165:1441–1446
Krejčí K, Zadražil J, Tichý T et al (2009) Sonographic findings in borderline changes and subclinical acute renal allograft rejection. Eur J Radiol 71:288–295
Kahraman S, Genctoy G, Cil B et al (2004) Prediction of renal allograft function with early Doppler ultrasonography. Transpl Proc 36:1348–1351
Khosroshahi HT, Heris HK, Makhdami N et al (2011) Time-dependent Doppler ultrasonographic findings in transplanted kidneys from living donors: A 5-year follow-up study. Transpl Proc 43(2):482–484
Adibi A, Ramezani M, Mortazavi M, Taheri S (2012) Color Doppler indexes in early phase after kidney transplantation and their association with kidney function on six month follow up. Adv Biomed Res 1:62
Drudi FM, Cantisani V, Liberatore M (2010) Role of low-mechanical index CEUS in the differentiation between low and high grade bladder carcinoma: a pilot study. Ultraschall Med 31(6):589–595
Conflict of interest
Francesco Maria Drudi, Mauro Liberatore, Vito Cantisani, Flavio Malpassini, Fabrizio Maghella, Nicola Di Leo, David Fasciolo, Ferdinando D’Ambrosio declare that they have no conflict of interest related to this study as they have no financial or personal relationship with a third party whose interest could be positively or negatively influenced by the article’s contents.
Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients.
Animal Studies
This article does not contain any studies involving human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Drudi, F.M., Liberatore, M., Cantisani, V. et al. Role of color Doppler ultrasound in the evaluation of renal transplantation from living donors. J Ultrasound 17, 207–213 (2014). https://doi.org/10.1007/s40477-014-0077-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-014-0077-6