
Abstract
Purpose of Review
Sensory over-responsivity (SOR) is an excessively unpleasant response to or avoidance of sensory stimuli, e.g., sound and light, which is prevalent among individuals with autism spectrum disorder (ASD). Despite its negative impacts on personal and social lives, knowledge about the occurrence of and mechanisms underlying SOR is inadequate. This review of studies on SOR in ASD summarizes the evidence on the close relationship of SOR with prenatal and genetic factors and presents information on neural mechanisms underlying SOR.
Recent Findings
Emerging studies have reported that SOR symptoms are related to abnormal structural connectivity in the brain, particularly decreased inter-hemispheric connectivity in subcortical regions (the thalamus and basal ganglia) and increased intra-hemispheric connectivity in the basal ganglia, especially in the right cerebral hemisphere, and with an enlarged amygdala. In the resting state, functional connectivity between the pulvinar and primary sensory regions, the basal ganglia, the limbic system (the amygdala and hippocampus), the temporal cortex, the prefrontal cortex, and sensorimotor regions is enhanced, while structural and functional connectivity between the thalamus and cortex is diminished.
Summary
These findings indicate that the functional abnormalities associated with SOR are probably due to reduced top-down regulation, which inhibits the reorientation of attention from external stimuli, thereby causing difficulty in filtering out and/or integrating sensory information and then lowering inhibition in generating excessive responses to the incoming sensory stimuli.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Autism spectrum disorder (ASD) is a widespread neurodevelopmental disorder marked by stereotyped and repetitive patterns of behavior and impairments in social communication and interaction [1]. Sensory abnormalities have been reported in as high as 90–95% of individuals with ASD [2,3,4] and in approximately 16% of the general population [5] and only 8% of the subjects in a sample of 8-year-old children without ASD [6]. Despite the high prevalence of sensory abnormalities in ASD, their occurrence and underlying mechanisms are not yet fully understood. The extent of sensory abnormalities has been found to be associated with the severity of autistic traits, such as repetitive behavior [7, 8] and stereotyped behavior [8,9,10,11].
Sensory features of ASD have received growing attention over the past two decades from specialists in a wide range of fields [12, 13]. The Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, already acknowledges the abnormal preoccupation with sensory aspects of the environment manifested by individuals with ASD (DSM-IV). As per the DSM-V published in 2013 [1], sensory reactivity is now included among the diagnostic criteria for ASD. There are three types of sensory response patterns: sensory over-responsivity (SOR, or sensory hyper-reactivity), sensory under-responsivity (SUR, or sensory hypo-reactivity), and sensation seeking (unusual sensory interests) [14]. Unusual interest shown by individuals with ASD in sensory aspects of the environment is already acknowledged in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV). In 2013, the DSM-V added sensory reactivity to the diagnostic criteria for ASD Sensory features can be classified into three sensory response patterns: sensory over-responsivity (SOR, refers to sensory hyper-reactivity), sensory under-responsivity (SUR, refers to sensory hypo-reactivity), and sensation seeking (unusual sensory interests) SUR refers to the lack of awareness of certain stimuli or slow response to sensory inputs such as sounds or spoken language [15, 16]. Conversely, SOR refers to the subjective experience of and hyper-reactivity to sensory overload that would typically not be regarded as troublesome to individuals without SOR [11, 16, 17]. In individuals with ASD, SOR has been reported to be more common than SUR, with prevalence ranging from 56 to 79% [18,19,20], and to affect almost all sensory modalities [2, 12, 21]. In fact, numerous individuals with ASD have more than one sensory response pattern.
Researchers have proposed theoretical frameworks such as the “weak central coherence” theory [22••], the “temporal binding deficit” hypothesis [23••], and the “excitatory/inhibitory imbalance” model [24••] to account for the SOR phenomenon. A common theme across these frameworks is that SOR is related to abnormal development of neuroanatomical structures crucial for processing visual, auditory, or tactile information [25, 26]. SOR is a form of sensory modulation disorder that falls within the sensory processing disorder umbrella[14]. SOR is a low-neurological-threshold-passive self-regulation method used in response to sensory stimuli, according to Dunn’s model of sensory processing [27•]. Because of their heightened sensitivity to their surroundings (caused by a lower-than-average neurological threshold), people with SOR often adopt a passive self-regulation strategy, choosing instead to remain in the current situation and respond to it as it unfolds. In some cases, they may aggravate responses to sensory input. Children with SOR to sounds may, for instance, cover their ears or request silence.
The specificity of and mechanisms underlying SOR in ASD are still under investigation. In this paper, we present a review of behavioral and clinical studies that have reported plausible neural mechanisms underlying SOR in individuals with ASD.
Prenatal and Genetic Influences on SOR
Studies have revealed that prenatal and genetic factors play a role in SOR-related symptoms. A study found that infants and toddlers who were small for gestational age manifested SOR-related behaviors more frequently than their typically developed counterparts [28]. Another study reported that subnormal neuroplasticity of premature babies [29] was associated with SOR. However, Keuler et al. (2011) did not find a wide spectrum of prenatal factors that significantly contributed to SOR symptoms in toddlers [30].
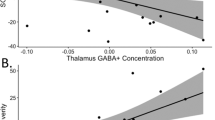
Changes in the internal environment during the prenatal period, such as intake of medication or alcohol, increase hormone production due to excessive stress [31, 32]. Increased secretion of testosterone in pregnant women [33] has been consistently shown to negatively affect neurodevelopmental outcomes in typically developed children without ASD. In children with ASD, mutations in genes encoding neuroligin-3 [34] and gamma-aminobutyric acid receptor subunit beta-3 [35] have been proven to be substantially linked to SOR-related symptoms, as these mutations disturbed the balance of gamma-aminobutyric acid (GABA) [36, 37] and glutamate [38, 39] in the brain. Imbalanced synthesis of GABA and glutamate, particularly the latter, results in excessive inhibitory or excitatory responses to sensory stimuli [24]. A recent magnetic resonance (MR) spectroscopy study reported close relationships between the GABA concentration in the cerebral cortex and visual perceptual functions of children with ASD. Compared with typically developed children, ASD children were found to have lower GABA concentrations in the visual cortices, which were associated with a stronger sensitivity to visual stimuli [40]. The mechanisms underlying the possible influences of GABA and glutamate imbalance, changes in brain structures, and modulations in neural functions on SOR in ASD are discussed below.
Possible Neural Mechanisms Underlying SOR
-
(1)
Sensory, emotion, and motor processing
Neurophysiological abnormalities may explain the problems encountered by children with SOR when exposed to sensory inputs [41]. To understand the neural mechanism underlying SOR in ASD, it is important to understand normal sensory to motor processing (the process from receiving sensory input to executing the motor and emotional response) in the brain. Wickens and Carswell (2012) suggested that sensorimotor processing includes three components: sensory, emotion, and motor processing (Fig. 1) [42••]. During sensory processing, sensory inputs first reach the short-term sensory store for temporary storage [43]. Selective attention allocates attentional resources to decode, discriminate, and organize the sensory input captured in sensory processing [44], and then to motor processing to select and generate an appropriate response to the sensory signal (Fig. 1) [45]. Emotion processing involves the awareness and appraisal of the experiences associated with incoming sensory information [46]. One study suggested that experiences arouse the emotion attached to related prior events stored in long-term memory [47]. In general, the generation of motor responses to the sensory input involves four steps: response selection [48, 49], response preparation [48, 50], response initiation [50], and response execution [49].

Summary of sensory-motor processing which has sensory, emotion, and motor components from the detection of the sensory input to make a response
There are many neural substrates associated with sensory, emotion, and motor processing. Sensory inputs arrive in the sensory organs, such as eyes and ears, and are converted into electrical signals that are further propagated to the thalamus and sensory cortices via the midbrain for sensory processing (Fig. 2) [51]. The electrical signals also travel to the amygdala and anterior insula, which are parts of the salience network (SN) for emotion processing [52]. Both the anterior insula (AI) and dorsal anterior cingulate cortex (dACC) within the SN contribute to the emotional processing of sensory stimuli [53]. Depending on the purpose of processing, sensory inputs may or may not be consolidated into long-term memory, which is subserved by the hippocampus and amygdala [54]. In addition, the SN has been shown to be implicated in motor responses [55]. The prefrontal cortex plays a crucial role in subserving working memory for maintaining the sensory input for further processing [56]. The thalamus, pre-supplementary, supplementary and primary motor cortex, and cerebellum mediate the different stages of motor processing [57, 58]. Abnormalities in any of these brain regions, such as abnormal activation or connection, are likely to cause SOR.
-
(2)
Neural abnormalities associated with SOR in ASD

Summary of neural substrates and their connectivity subserving sensory-motor processing. Neural substrates of the salience network are grouped within the blue dotted-line circle. The thalamus (shaded in blue) plays a prime role in sensory processing, while the amygdala (shaded in grey) plays a prime role in emotion processing and behavior selection
SOR in ASD is related to increased activation in the thalamus and brain areas subserving primary sensory processing (e.g., auditory, visual, and somatosensory cortices) as well as salience detection and attention (e.g., the insula and amygdala) (Fig. 3) [59•, 60•]. In addition to attention and sensory processing, three studies have found that the core facets of SOR in normal individuals are associated with deep sensory integration (e.g., in the prefrontal cortex, precuneus and inferior frontal gyrus), enhanced empathy and emotionality (e.g., involving the claustrum, anterior insula, amygdala, and cingulate cortex), and preparation for action (i.e., involving the premotor region as well as dorsolateral and medial prefrontal cortices) [61,62,63].
-
(3)
Functional connectivity abnormalities — the thalamus and amygdala

Abnormal neural substrates and specific functional and structural networks related to sensory over-responsiveness in individuals with ASD
The thalamus is a subcortical neural substrate functionally connected to the insula and somatosensory, motor, and premotor areas of the cortices [64]. It is essential for the transmission and integration of sensory information in the brain [65]. Children with sensory processing disorders, including SOR, have been found to have reduced structural connections between the cortex and thalamus, and decreased functional connections among the primary sensory regions and thalamus, compared with typically developed children [66, 67]. These findings are consistent with the aberrant intrinsic thalamus connection observed in ASD participants. [68]. In contrast, Cerliani et al. (2015), based on resting-state functional magnetic resonance imaging (fMRI), reported increased functional connections among primary sensory regions and the thalamus as well as basal ganglia. These differences in the results of the three studies may be due to the use of different sample populations (all individuals with sensory disorders vs. individuals with ASD) and/or the different age ranges of the participants. It is also possible that the brain itself can do its best to control and reinforce the functional connection when it needs to function, even though the fundamental structural connection is weakened.
Functional connectivity between the thalamus and sensorimotor regions is reduced in children and adolescents with ASD, while it is strengthened between the thalamus and the right temporal cortex [69]. During sensory processing (when exposed to slightly unpleasant tactile and auditory stimuli), adolescents with ASD and SOR showed reduced functional connection between the thalamus and cortex, according to a fMRI research [70•]. Reduced thalamocortical connectivity has been hypothesized to reflect impaired top-down regulation in ASDs with SOR [71], making it more challenging for those with the disorder to ignore irrelevant sensory data, integrate sensory data, and exercise selective inhibition and focus on relevant information [70•]. Individuals with ASD are more likely to feel overwhelmed by irrelevant stimuli or while receiving several stimuli simultaneously, which is consistent with sensory gating hypotheses showing abnormalities in sensory gating and selective attention of sensory stimuli [4].
Among the thalamic nuclei, the pulvinar appears to play a unique role in regulating and integrating sensory information [72, 73] and selective attention [74]. Individuals with ASD have been shown to have increased connection between the pulvinar and the temporal cortices, prefrontal cortex, and sensorimotor regions [75]. Compared with healthy controls, adolescent with ASD demonstrated increased activation in the pulvinar in response to slightly unpleasant tactile and auditory stimuli [59•, 60•]. In particular, individuals with ASD and SOR showed increased connectivity between the pulvinar and the putamen, hippocampus, and right amygdala [70•]. Another study found that individuals with ASD had larger right amygdala volumes than left amygdala volumes [76•]. The increased connection between the amygdala and pulvinar has been proposed to be responsible for the negative emotion associated with SOR. Taken together, the increased thalamocortical and pulvinar–amygdala connectivity in ASD offers plausible explanations for why excessive attention to distracting sensory stimuli is likely to be associated with negative emotion when processing the stimuli.
-
(4)
Structural connectivity abnormalities
Duan et al. (2020) and Cardon et al. (2017) reported that children with ASD showed reduced structural connectivity between the right and left hemispheres through the thalamus compared to typically developing children [76•, 77•]. Within the subcortical regions of individuals with ASD, Duan et al. (2020) found decreased connectivity between left nucleus accumbent and the right globus pallidus and between the right nucleus accumbent and left globus pallidus, whereas an increased structural covariance among the adjacent regions in the right globus pallidus. These abnormalities in connectivity may contribute to SOR symptoms, as these neural substrates play important roles in transmitting incoming information received from the sensory organs. For instance, the weakened connectivity between the two hemispheres suggests that sensory cortices do not communicate as well as required, leading to failure in integrating the sensory inputs for initiating adaptive responses. Reduced white matter integrity has been reported to lead to problems with the synchronization of action potential transmission, which is crucial for sensory processing and multisensory integration [67].
-
(5)
Summary of possible neural mechanisms underlying SOR in ASD
Our review of studies on attention and emotion regulation in ASD revealed an association between attention, neural substrates, and SOR, providing a plausible explanation of SOR from the perspective of connectivity among neural substrates. The specific findings are listed below. First, in individuals with ASD and SOR, resting-state functional connections are enhanced between the thalamus, sensory cortex, and amygdala. Involvement of these neural substrates in ASD with SOR suggests that SOR is associated with increased attention and emotional response to sensory stimuli. Second, abnormalities in structural connectivity leading to weaker connections between the left and right hemispheres and stronger connections within the respective hemispheres (between the ipsilateral thalamus and amygdala) lead to excessive attention to emotion stimuli and lack of timely communication and cooperation between the hemispheres. This prevents adequate regulation and integration of sensory information in the brain, leading to the output of excessive emotional responses and, consequently, more severe SOR symptoms in ASD. Thus, the possible neural mechanism underlying SOR in ASD can be summarized as follows: the abnormalities of functional and structural connectivity in the brain of individuals with ASD inhibits proper top-down regulation and integration of sensory inputs, leading to increased attention to extraneous sensory stimuli during sensory processing and, as a result, the output of excessive emotional response to these stimuli.
Conclusion
Our review revealed that SOR in ASD is associated with the following abnormalities in brain connectivity: (i) reduced inter-hemispheric structural covariance connection across subcortical areas and enhanced intra-hemispheric structural covariance connection, which is thought to cause symptoms of weak central coherence [77•]; (ii) increased structural covariance in the right cerebral hemisphere, which is associated with the theory of hemispheric functional lateralization [78]; and (iii) increased functional connection between the thalamus, sensory cortex, and amygdala and decreased functional connection between the thalamus and cortex, leading to reduced top-down regulation from the cortex to thalamus; this causes difficulty in filtering out and/or integrating sensory information and failure in selective inhibition and attention to external stimuli, causing lowered inhibition in generating excessive responses to the incoming sensory stimuli [70•]. The implications of these findings for the future of intervention research and development for children with ASD and SOR are substantial. Instead of working to restore normal sensory processing, effective interventions should instead train individuals to better manage their attention and emotional responses to outside stimuli [59•, 60•]. There are already effective interventions that teach coping strategies to individuals with ASD in order to decrease their anxiety [79, 80]. Due to the high prevalence of co-occurrence of anxiety and SOR in these individuals, it may be useful to adjust these therapies to focus on SOR [81]. More investigation into SOR’s mechanistic underpinnings is needed to inform the development of more efficient therapies and treatment strategies for ASD.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), Fifth edition; American psychiatric association: Washington, DC, 2013, ISBN 13: 9780890425558.
Crane L, Goddard L, Pring L. Sensory processing in adults with autism spectrum disorders. Autism. 2009;13:215–28. https://doi.org/10.1177/1362361309103794.
Leekam SR, Nieto C, Libby SJ, Wing L, Gould J. Describing the sensory abnormalities of children and adults with autism. J Autism Dev Disord. 2007;37:894–910. https://doi.org/10.1007/s10803-006-0218-7.
Marco EJ, Hinkley LBN, Hill SS, Nagarajan SS. Sensory processing in autism: a review of neurophysiologic findings. Pediatr Res. 2011;69:48R–54R. https://doi.org/10.1203/PDR.0b013e3182130c54.
Ben-Sasson A, Carter AS, Briggs-Gowan MJ. Sensory over-responsivity in elementary school: prevalence and social-emotional correlates. J Abnorm Child Psychol. 2009;37:705–16. https://doi.org/10.1007/s10802-008-9295-8.
Jussila K, Junttila M, Kielinen M, Ebeling H, Joskitt L, Moilanen I, Mattila M-L. Sensory abnormality and quantitative autism traits in children with and without autism spectrum disorder in an epidemiological population. J Autism Dev Disord. 2020;50:180–8. https://doi.org/10.1007/s10803-019-04237-0.
Baron-Cohen S, Ashwin E, Ashwin C, Tavassoli T, Chakrabarti B. Talent in autism: hyper-systemizing, hyper-attention to detail and sensory hypersensitivity. Philos Trans R Soc Lond Ser B Biol Sci. 2009;364:1377–83. https://doi.org/10.1098/rstb.2008.0337.
Sutherland A, Crewther DP. Magnocellular visual evoked potential delay with high autism spectrum quotient yields a neural mechanism for altered perception. Brain. 2010;133:2089–97. https://doi.org/10.1093/brain/awq122.
Blake R, Turner LM, Smoski MJ, Pozdol SL, Stone WL. Visual recognition of biological motion is impaired in children with autism. Psychol Sci. 2003;14:151–7. https://doi.org/10.1111/1467-9280.01434.
Joseph RM, Keehn B, Connolly C, Wolfe JM, Horowitz TS. Why is visual search superior in autism spectrum disorder? Dev Sci. 2009;12:1083–96. https://doi.org/10.1111/j.1467-7687.2009.00855.x.
Robertson CE, Kravitz DJ, Freyberg J, Baron-Cohen S, Baker CI. Tunnel vision: sharper gradient of spatial attention in autism. J Neurosci. 2013;33:6776–81. https://doi.org/10.1523/JNEUROSCI.5120-12.2013.
Ben-Sasson A, Gal E, Fluss R, Katz-Zetler N, Cermak SA. Update of a meta-analysis of sensory symptoms in ASD: a new decade of research. J Autism Dev Disord. 2019;49:4974–96. https://doi.org/10.1007/s10803-019-04180-0.
DuBois D, Lymer E, Gibson BE, Desarkar P, Nalder E. Assessing sensory processing dysfunction in adults and adolescents with autism spectrum disorder: a scoping review. Brain Sci. 2017;7. https://doi.org/10.3390/brainsci7080108.
Miller LJ, Anzalone ME, Lane SJ, Cermak SA, Osten ET. Concept evolution in sensory integration: a proposed nosology for diagnosis. Am J Occup Ther. 2007;61:135–40. https://doi.org/10.5014/ajot.61.2.135.
Miller LJ. Sensational kids: hope and help for children with sensory processing disorder (SPD). New York: The Penguin Group; 2014.
Tavassoli T, Miller LJ, Schoen SA, Nielsen DM, Baron-Cohen S. Sensory over-responsivity in adults with autism spectrum conditions. Autism. 2014;18:428–32. https://doi.org/10.1177/1362361313477246.
Liss M, Saulnier C, Fein D, Kinsbourne M. Sensory and attention abnormalities in autistic spectrum disorders. Autism. 2006;10:155–72. https://doi.org/10.1177/1362361306062021.
Baranek GT, David FJ, Poe MD, Stone WL, Watson LR. Sensory Experiences Questionnaire: discriminating sensory features in young children with autism, developmental delays, and typical development. J Child Psychol Psychiatry. 2006;47:591–601. https://doi.org/10.1111/j.1469-7610.2005.01546.x.
Ben-Sasson A, Cermak SA, Orsmond GI, Tager-Flusberg H, Carter AS, Kadlec MB, Dunn W. Extreme sensory modulation behaviors in toddlers with autism spectrum disorders. Am J Occup Ther. 2007;61:584–92. https://doi.org/10.5014/ajot.61.5.584.
Tomchek SD, Dunn W. Sensory processing in children with and without autism: a comparative study using the short sensory profile. Am J Occup Ther. 2007;61:190–200. https://doi.org/10.5014/ajot.61.2.190.
Fernández-Andrés MI, Sanz-Cerverza P, Salgado-Burgos C, Tárraga-Mínguez R, Pastor-Cerezuela G. Comparative study of sensory modulation vulnerabilities in children with and without ASD in family and school contexts. Journal of Occupational Therapy, Schools, & Early Intervention. 2018;11:318–28. https://doi.org/10.1080/19411243.2018.1432448.
•• Happé F. The weak central coherence account of autism. In Handbook of Autism and Pervasive Developmental Disorders; Volkmar FR, Paul R, Klin A, Cohen D, Eds.; Wiley, 2005; pp 640–649, ISBN 9780471716969. One of the most classical theories to explain the abnormal behavior of autism including SOR.
•• Brock J, Brown CC, Boucher J, Rippon G. The temporal binding deficit hypothesis of autism. Dev Psychopathol. 2002;14:209–24. https://doi.org/10.1017/S0954579402002018This study proposes a classical theory to interpret some autistic symptoms from the perspective of neural networks including SOR.
•• Rubenstein JLR, Merzenich MM. Model of autism: increased ratio of excitation/inhibition in key neural systems. Genes Brain Behav. 2003;2:255–67. https://doi.org/10.1034/j.1601-183X.2003.00037.xThis study combines various hypotheses about the causes of autism to propose a model that can also be used to explain sensory nervous system problems, including SOR, and suggests potential therapeutic interventions for this model.
Pelphrey KA, Shultz S, Hudac CM, Vander Wyk BC. Research review: Constraining heterogeneity: the social brain and its development in autism spectrum disorder. J Child Psychol Psychiatry. 2011;52:631–44. https://doi.org/10.1111/j.1469-7610.2010.02349.x.
Richardson H, Gweon H, Dodell-Feder D, Malloy C, Pelton H, Keil B, Kanwisher N, Saxe R. Response patterns in the developing social brain are organized by social and emotion features and disrupted in children diagnosed with autism spectrum disorder. Cortex. 2020;125:12–29. https://doi.org/10.1016/j.cortex.2019.11.021.
• Dunn W. The impact of sensory processing abilities on the daily lives of young children and their families: a conceptual model. Infants Young Child. 1997;9:23–35 This study proposes a model to define and classify sensory processing problems, including sensory sensitivity (SOR) from the perspective of behavioral response and neurological threshold.
Goldsmith HH, van Hulle CA, Arneson CL, Schreiber JE, Gernsbacher MA. A population-based twin study of parentally reported tactile and auditory defensiveness in young children. J Abnorm Child Psychol. 2006;34:393–407. https://doi.org/10.1007/s10802-006-9024-0.
Schneider ML, Moore CF, Gajewski LL, Larson JA, Roberts AD, Converse AK, DeJesus OT. Sensory processing disorder in a primate model: evidence from a longitudinal study of prenatal alcohol and prenatal stress effects. Child Dev. 2008;79:100–13. https://doi.org/10.1111/j.1467-8624.2007.01113.x.
Keuler MM, Schmidt NL, van Hulle CA, Lemery-Chalfant K, Goldsmith HH. Sensory overresponsivity: prenatal risk factors and temperamental contributions. J Dev Behav Pediatr. 2011;32:533–41. https://doi.org/10.1097/DBP.0b013e3182245c05.
Ji C. Advances and new concepts in alcohol-induced organelle stress, unfolded protein responses and organ damage. Biomolecules. 2015;5:1099–121. https://doi.org/10.3390/biom5021099.
Schneider ML, Moore CF, Adkins MM. The effects of prenatal alcohol exposure on behavior: rodent and primate studies. Neuropsychol Rev. 2011;21:186–203. https://doi.org/10.1007/s11065-011-9168-8.
van den Heuvel MI, Donkers FCL, Winkler I, Otte RA, van den Bergh BRH. Maternal mindfulness and anxiety during pregnancy affect infants' neural responses to sounds. Soc Cogn Affect Neurosci. 2015;10:453–60. https://doi.org/10.1093/scan/nsu075.
Tabuchi K, Blundell J, Etherton MR, Hammer RE, Liu X, Powell CM, Südhof TC. A neuroligin-3 mutation implicated in autism increases inhibitory synaptic transmission in mice. Science. 2007;318:71–6. https://doi.org/10.1126/science.1146221.
DeLorey TM, Sahbaie P, Hashemi E, Li W-W, Salehi A, Clark DJ. Somatosensory and sensorimotor consequences associated with the heterozygous disruption of the autism candidate gene, Gabrb3. Behav Brain Res. 2011;216:36–45. https://doi.org/10.1016/j.bbr.2010.06.032.
Coghlan S, Horder J, Inkster B, Mendez MA, Murphy DG, Nutt DJ. GABA system dysfunction in autism and related disorders: from synapse to symptoms. Neurosci Biobehav Rev. 2012;36:2044–55. https://doi.org/10.1016/j.neubiorev.2012.07.005.
Oblak A, Gibbs TT, Blatt GJ. Decreased GABAA receptors and benzodiazepine binding sites in the anterior cingulate cortex in autism. Autism Res. 2009;2:205–19. https://doi.org/10.1002/aur.88.
Burnashev N, Szepetowski P. NMDA receptor subunit mutations in neurodevelopmental disorders. Curr Opin Pharmacol. 2015;20:73–82. https://doi.org/10.1016/j.coph.2014.11.008.
Rojas DC, Wilson LB. γ-band abnormalities as markers of autism spectrum disorders. Biomark Med. 2014;8:353–68. https://doi.org/10.2217/bmm.14.15.
Robertson CE, Baron-Cohen S. Sensory perception in autism. Nat Rev Neurosci. 2017;18:671–84. https://doi.org/10.1038/nrn.2017.112.
Yung TWK, Lai CYY, Chan JYC, Ng SSM, Chan CCH. Neuro-physiological correlates of sluggish cognitive tempo (SCT) symptoms in school-aged children. Eur Child Adolesc Psychiatry. 2020;29:315–26. https://doi.org/10.1007/s00787-019-01353-1.
•• Wickens CD, Carswell CM. Information processing. In: Handbook of human factors and ergonomics, vol. 68. Wiley; 2021. pp. 114–158. https://doi.org/10.1002/9781118131350.ch5. This study well explains the different important stages of information processing, which requires multi-task performance, including perception, cognition, action and so on, so that we can understand the SOR process well.
Shiffrin RM. Short-term store: the basis for a memory system. In: Cognitive theory. 1st ed. Psychology Press; 2018. pp. 193–218. https://doi.org/10.4324/9780203781548-13.
Gazzaley A, Nobre AC. Top-down modulation: bridging selective attention and working memory. Trends Cogn Sci. 2012;16:129–35. https://doi.org/10.1016/j.tics.2011.11.014.
Młynarski WF, Hermundstad AM. Adaptive coding for dynamic sensory inference. Elife. 2018;7. https://doi.org/10.7554/eLife.32055.
Baker R. An emotional processing model for counselling and psychotherapy: a way forward. Counselling in Practice. 2001;7:8–11.
Baker R, Thomas S, Thomas PW, Owens M. Development of an emotional processing scale. J Psychosom Res. 2007;62:167–78. https://doi.org/10.1016/j.jpsychores.2006.09.005.
Brass M, Haggard P. The what, when, whether model of intentional action. Neuroscientist. 2008;14:319–25. https://doi.org/10.1177/1073858408317417.
Carbonnell L, Hasbroucq T, Grapperon J, Vidal F. Response selection and motor areas: a behavioural and electrophysiological study. Clin Neurophysiol. 2004;115:2164–74. https://doi.org/10.1016/j.clinph.2004.04.012.
Haith AM, Pakpoor J, Krakauer JW. Independence of movement preparation and movement initiation. J Neurosci. 2016;36:3007–15. https://doi.org/10.1523/JNEUROSCI.3245-15.2016.
Nakajima M, Halassa MM. Thalamic control of functional cortical connectivity. Curr Opin Neurobiol. 2017;44:127–31. https://doi.org/10.1016/j.conb.2017.04.001.
Islam R, Ahuja K, Karmakar S, Barbhuiya F. SenTion: a framework for sensing facial expressions. arXiv preprint. 2016; 1–6. https://doi.org/10.48550/arXiv.1608.04489
Geng H, Li X, Chen J, Li X, Gu R. Decreased intra- and inter-salience network functional connectivity is related to trait anxiety in adolescents. Front Behav Neurosci. 2015;9:350. https://doi.org/10.3389/fnbeh.2015.00350.
Swenson RS. Review of clinical and functional neuroscience. In: Holmes GL, editor. Educational review manual in neurology. New York: Castle Connolly Graduate Medical Publishing; 2006
Menon V, Uddin LQ. Saliency, switching, attention and control: a network model of insula function. Brain Struct Funct. 2010;214:655–67. https://doi.org/10.1007/s00429-010-0262-0.
Eriksson J, Vogel EK, Lansner A, Bergström F, Nyberg L. Neurocognitive architecture of working memory. Neuron. 2015;88:33–46. https://doi.org/10.1016/j.neuron.2015.09.020.
Nachev P, Kennard C, Husain M. Functional role of the supplementary and pre-supplementary motor areas. Nat Rev Neurosci. 2008;9:856–69. https://doi.org/10.1038/nrn2478.
Erickson LC, Zielinski BA, Zielinski JEV, Liu G, Turkeltaub PE, Leaver AM, Rauschecker JP. Distinct cortical locations for integration of audiovisual speech and the McGurk effect. Front Psychol. 2014;5:534. https://doi.org/10.3389/fpsyg.2014.00534.
• Green SA, Rudie JD, Colich NL, Wood JJ, Shirinyan D, Hernandez L, Tottenham N, Dapretto M, Bookheimer SY. Overreactive brain responses to sensory stimuli in youth with autism spectrum disorders. J Am Acad Child Adolesc Psychiatry. 2013;52:1158–72. https://doi.org/10.1016/j.jaac.2013.08.004This study indicates that SOR in ASD is highly associated with hyperactive primary sensory areas and emotional areas such as the amygdala and hippocampus.
• Green SA, Hernandez L, Tottenham N, Krasileva K, Bookheimer SY, Dapretto M. Neurobiology of sensory overresponsivity in youth with autism spectrum disorders. JAMA Psychiat. 2015;72:778–786. https://doi.org/10.1001/jamapsychiatry.2015.0737. This study provides evidence for abnormal brain functional connections in autistic with SOR, such as the negative functional connectivity between the amygdala and orbitofrontal cortex.
Acevedo BP, Aron EN, Aron A, Sangster M-D, Collins N, Brown LL. The highly sensitive brain: an fMRI study of sensory processing sensitivity and response to others' emotions. Brain Behav. 2014;4:580–94. https://doi.org/10.1002/brb3.242.
Acevedo BP, Jagiellowicz J, Aron E, Marhenke R, Aron A. Sensory processing sensitivity and childhood quality’s effects on neural responses to emotional stimuli. Clinical Neuropsychiatry: Journal of Treatment Evaluation. 2017;14(6):359–73.
Greven CU, Lionetti F, Booth C, Aron EN, Fox E, Schendan HE, Pluess M, Bruining H, Acevedo B, Bijttebier P, et al. Sensory processing sensitivity in the context of environmental sensitivity: a critical review and development of research agenda. Neurosci Biobehav Rev. 2019;98:287–305. https://doi.org/10.1016/j.neubiorev.2019.01.009.
Tomasi D, Volkow ND. Reduced local and increased long-range functional connectivity of the thalamus in autism spectrum disorder. Cereb Cortex. 2019;29:573–85. https://doi.org/10.1093/cercor/bhx340.
Sherman SM. Thalamus plays a central role in ongoing cortical functioning. Nat Neurosci. 2016;19:533–41. https://doi.org/10.1038/nn.4269.
Nair A, Treiber JM, Shukla DK, Shih P, Müller R-A. Impaired thalamocortical connectivity in autism spectrum disorder: a study of functional and anatomical connectivity. Brain. 2013;136:1942–55. https://doi.org/10.1093/brain/awt079.
Owen JP, Marco EJ, Desai S, Fourie E, Harris J, Hill SS, Arnett AB, Mukherjee P. Abnormal white matter microstructure in children with sensory processing disorders. Neuroimage Clin. 2013;2:844–53. https://doi.org/10.1016/j.nicl.2013.06.009.
Cerliani L, Mennes M, Thomas RM, Di Martino A, Thioux M, Keysers C. Increased functional connectivity between subcortical and cortical resting-state networks in autism spectrum disorder. JAMA Psychiat. 2015;72:767–77. https://doi.org/10.1001/jamapsychiatry.2015.0101.
Nair A, Carper RA, Abbott AE, Chen CP, Solders S, Nakutin S, Datko MC, Fishman I, Müller R-A. Regional specificity of aberrant thalamocortical connectivity in autism. Hum Brain Mapp. 2015;36:4497–511. https://doi.org/10.1002/hbm.22938.
• Green SA, Hernandez LM, Bowman HC, Bookheimer SY, Dapretto M. Sensory over-responsivity and social cognition in ASD: effects of aversive sensory stimuli and attentional modulation on neural responses to social cues. Dev Cogn Neurosci. 2018;29:127–39. https://doi.org/10.1016/j.dcn.2017.02.005This study suggests that abnormal functional connections affect the process of attention regulation of sensory stimuli, which leads to SOR in ASD.
Zalla T, Sperduti M. The amygdala and the relevance detection theory of autism: an evolutionary perspective. Front Hum Neurosci. 2013;7:894. https://doi.org/10.3389/fnhum.2013.00894.
Sherman SM, Guillery RW. Functional organization of thalamocortical relays. J Neurophysiol. 1996;76:1367–95. https://doi.org/10.1152/jn.1996.76.3.1367.
Shipp S. The functional logic of cortico-pulvinar connections. Philos. Trans. R. Soc. Lond. B Biol Sci. 2003;358:1605–24. https://doi.org/10.1098/rstb.2002.1213.
Zhou H, Schafer RJ, Desimone R. Pulvinar-cortex interactions in vision and attention. Neuron. 2016;89:209–20. https://doi.org/10.1016/j.neuron.2015.11.034.
Woodward ND, Giraldo-Chica M, Rogers B, Cascio CJ. Thalamocortical dysconnectivity in autism spectrum disorder: an analysis of the Autism Brain Imaging Data Exchange. Biol Psychiatry Cogn Neurosci Neuroimaging. 2017;2:76–84. https://doi.org/10.1016/j.bpsc.2016.09.002.
• Duan X, Wang R, Xiao J, Li Y, Huang X, Guo X, Cao J, He L, He C, Ling Z, et al. Subcortical structural covariance in young children with autism spectrum disorder. Prog Neuropsychopharmacol Biol Psychiat. 2020;99:109874. https://doi.org/10.1016/j.pnpbp.2020.109874This study provides evidence of structural connectivity abnormalities in autism, with decreased inter-hemispheric and increased intra-hemispheric structural connectivity in subcortices. These abnormal connections can predict abnormal behavior of ASD including SOR.
• Cardon GJ, Hepburn S, Rojas DC. Structural covariance of sensory networks, the cerebellum, and amygdala in autism spectrum disorder. Front. Neurol. 2017;8:615. https://doi.org/10.3389/fneur.2017.00615This study demonstrates that sensory dysfunction (including SOR) is strongly associated with abnormal structural connectivity in the brain, with decreased connectivity in sensory areas with the cerebellum and increased connectivity in sensory areas with the amygdala.
Kleinhans NM, Müller R-A, Cohen DN, Courchesne E. Atypical functional lateralization of language in autism spectrum disorders. Brain Res. 2008;1221:115–25. https://doi.org/10.1016/j.brainres.2008.04.080.
Russell AJ, Jassi A, Fullana MA, Mack H, Johnston K, Heyman I, Murphy DG, Mataix-Cols D. Cognitive behavior therapy for comorbid obsessive-compulsive disorder in high-functioning autism spectrum disorders: a randomized controlled trial. Depress Anxiety. 2013;30:697–708. https://doi.org/10.1002/da.22053.
Sukhodolsky DG, Bloch MH, Panza KE, Reichow B. Cognitive-behavioral therapy for anxiety in children with high-functioning autism: a meta-analysis. Pediatrics. 2013;132:e1341–50. https://doi.org/10.1542/peds.2013-1193.
Green SA, Ben-Sasson A. Anxiety disorders and sensory over-responsivity in children with autism spectrum disorders: is there a causal relationship? J Autism Dev Disord. 2010;40:1495–504. https://doi.org/10.1007/s10803-010-1007-x.
Funding
This work was supported by the Innovation and Technology Fund (ITF) of Hong Kong matching with Innovation Technology Company Limited (UIM381) awarded to Y-S Choy, and the Peter T. C. Lee Endowed Professorship fund to CCH Chan.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article contains no human or animal subjects studies conducted by any of the authors
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article was guest reviewed by Dr. Kannika Permpoonputtana
This article is part of the Topical Collection on Sensory Modulation
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yuan, HL., Lai, C.Y.Y., Wong, M.N.K. et al. Possible Neural Mechanisms Underlying Sensory Over-Responsivity in Individuals with ASD. Curr Dev Disord Rep 9, 89–97 (2022). https://doi.org/10.1007/s40474-022-00257-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40474-022-00257-1