
Abstract
The practice of permitting incarcerated individuals to become living organ donors in exchange for commuted sentences has been posed as a solution to the persistent organ shortage in recent legislation. We conducted a survey to assess transplant professionals’ attitudes toward organ donation by incarcerated individuals. A 12-item survey was developed and emailed to transplant professionals from 3/15/23 − 4/12/23. We calculated descriptive statistics overall and by surgeons vs. non-surgeons and geographic region. Of the 294 respondents, 80% indicated that incarcerated individuals should be allowed to participate in directed solid organ living donation and 55% indicated that incarcerated individuals should be allowed to participate in non-directed solid organ living donation. Among respondents who supported donation, 70% indicated that they would not support donation in exchange for a commuted sentence, citing ethical concerns related to coercion (27%) and legality (22%). Although the majority of respondents in our sample supported directed donor organ donation, most opposed allowing donations in return for commuted sentences. These results can be used to inform future legislation surrounding organ donation in the carceral system.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
For years, the number of individuals requiring an organ transplant has vastly exceeded the number of available organs. With 105,800 people on the national transplant waitlist, and the addition of another person every ten minutes, the transplant community is in need of creative solutions. To address the persistent organ shortage, policymakers, ethicists, and members of the transplant community have begun exploring alternative organ sources. One possible solution, that has garnered considerable media attention in recent months, involves permitting incarcerated individuals to become living donors, and at times in exchange for a commuted sentence.
On January 20, 2023, members of the Massachusetts House of Representatives proposed a bill that would allow prison inmates to donate organs or bone marrow in exchange for a sentence commutation of up to one year (MA – HD3822) [1].
Any proposed legislation that allows incarcerated individuals to donate an organ, particularly for a reduced sentence, raises a myriad of legal, ethical, and health concerns [2]. Federal law prohibits the acquisition of organs for “valuable consideration” but does not define the term. Statutory interpretation suggests that the phrase addresses organ transfers that would ordinarily constitute a “purchase” rather than all donations that may involve some exchange [3]. The main legal concern is that offering an incarcerated individual a reduced sentence in exchange for donating an organ amounts to a payment [4]. The primary ethical concern is that, because of situational circumstances that place incarcerated individuals at a greater risk for exploitation, they may feel coerced into donating an organ [5, 6]. For example, for most death row inmates, the decision to become a living organ donor in exchange for a commuted sentence could not be considered coercion-free, given the alternative [7]. Lastly, the leading health concern is the heightened risk rapid of disease transmission and circulation among prison populations [8]. In an environment with a heightened risk of rapid disease transmission, a recovering donor would be more susceptible to contracting illnesses post-donation than a non-incarcerated recovering donor.
Though the ethics of prisoner organ donation is a hotly debated and controversial topic, there is a lack of literature assessing prisoners’ perspectives on the practice. The primary reason for this gap in the literature is that, historically, prison-based research has been limited due to concerns that prisoners represent a vulnerable population, as outlined in the Department of Health and Human Services regulations for the protection of human subjects in research [9]. Transplant surgeons and other professionals (i.e. physicians, researchers, scientists, members of the transplant team etc.) are also uniquely positioned to provide a great deal of insight on the issues surrounding prisoner organ donation; however literature assessing transplant professionals’ perspectives on the practice is similarly lacking. We conducted an online survey assessing transplant professionals’ attitudes toward allowing incarcerated individuals to be solid organ donors, specifically in exchange for reduced sentences.
Methods
Study Population and Survey Distribution
The survey was emailed on March 15th, 2023, to individuals listed in the American Society of Transplant Surgeons member directory using REDCap, and could be accessed on both mobile devices and computer desktops [10, 11]. This email included a summary of the study, study contact information, and a link to the survey. Respondents were eligible if they were English-speakers, aged 18 or older, and were able to read and see. Respondents were screened at the beginning of the survey to confirm age and eligibility. All respondents received three recruitment emails: one initial email requesting participation in this study and two follow-up emails. Data was collected from 3/15/23 − 4/12/23. Participation in the survey was voluntary and consent language was included at the start of the survey. This study (s23-00175) was deemed exempt by the NYU Langone Health Institutional Review Board.
Survey Design
The survey was developed by experts in the fields of transplantation and bioethics. Literature reviews and group discussions informed survey constructs. The survey was pre-tested among transplant surgeons, and was designed to: (1) assess respondents’ attitudes toward allowing incarcerated individuals to become living donors, (2) assess whether respondents believe that incarcerated individuals can recover from the procurement surgery without risking their physical safety, (3) assess respondents’ attitudes towards allowing incarcerated individuals to become living donors in exchange for a commuted sentence, and (4) assess respondents’ attitudes towards including the opinions of incarcerated individuals in the decision to allow them to donate.
The survey included 12 closed-ended questions (including one screener question to ensure respondents were over the age of 18). Three questions were related to profession and state of residence, and eight questions asked respondents to indicate their attitudes toward various scenarios related to incarcerated donation. Respondents who believed that incarcerated individuals should be allowed to partake in solid organ donation were asked if this should include an exchange for a commuted sentence. If they supported the exchange, respondents answered additional questions about the type of crime and sentence reduction. Those who responded that they do not think incarcerated individuals should be permitted to donate in exchange for a reduced sentence were asked to select the reasons informing their opinion from a predetermined list.
Statistical Analysis
Descriptive statistics (frequencies and percentages) were calculated for each question. We aggregated survey results and stratified them by role (surgeon vs. non-surgeon) and U.S. region of residence (South, Northeast, North Central, West). States were assigned regions using the U.S. Department of Commerce, Bureau of the Census (1977) County and City Data Book. We compared responses from surgeons vs. non-surgeons using Wilcoxon rank-sum tests by assigning the response “yes” to 1, “not sure” to 0.5, and “no” to 0. A p-value of 0.05 was considered statistically significant and all tests were two-sided. All analyses were performed using R Studio (v.4.0.3).
Results
Study Population
Out of the 1597 transplant professionals contacted to participate in the study, 308 filled out the survey (19.3% response rate). In the final analysis, 14 participants were excluded as they did not answer any of the eight survey questions concerning incarcerated donor ethics, despite completing the eligibility screener and/or demographic questions. The final study population included 294 respondents, of which 98.3% fully completed the survey.
The study population was predominantly surgeons (67%). The remaining respondents consisted of surgical fellows (5.4%), non-physician scientists (5.1%), physicians (3.7%), resident post-doctoral fellows (3.7%), students (0.3%), and those who categorized their profession as “other” (14.6%). 92.9% of respondents lived within the US; 32.0% of these respondents lived in the South, 22.1% lived in the Northeast, 19.4% lived in the North Central, and 16.3% lived in the West. (Table 1) When stratifying by surgeon vs. non-surgeon and residence in the US vs. outside the US, we found no statistically significant differences in survey responses (Table 2).
Attitudes Toward Allowing Incarcerated Individuals to Participate in Solid Organ Living Donation as a Living Donor
Of the 294 respondents, 79.9% expressed support for incarcerated individuals being permitted to engage in directed solid organ living donation, such as donating to a friend or family member. Additionally, 54.8% of respondents believed that incarcerated individuals should have the opportunity to participate in non-directed solid organ living donation (Table 3). Among respondents who supported directed donation, 67.7% supported non-directed donation.
Compared to surgeons, non-surgeons were more likely to endorse both directed and non-directed incarcerated solid organ donation (directed: 78.7% vs. 82.5% (p = 0.39); non-directed: 51.8% vs. 60.8% (p = 0.06)) (Table 2). Of the four U.S. regions, respondents residing in the Northeast were the most receptive to permitting directed and non-directed solid organ donation, while those in the West were the least receptive (directed: 90.8% vs. 72.9%; non-directed: 60.0% vs. 47.9%).
Opinions on Whether Incarcerated Individuals can Recover from the Donation Surgery Without Risking their Physical Safety
Respondents were divided when asked whether they believed that most incarcerated individuals would be able to recover from donation surgery without risking their physical safety and have adequate access to healthcare; 24.1% responded “yes”, 43.9% responded “no”, and 32.0% responded “not sure” (Table 3). Although not statistically significant, non-surgeons were less likely to believe that prisoners would receive sufficient healthcare than surgeons (non-surgeon: 17.5%, surgeon: 27.4%, p = 0.37) (Table 2).
Attitudes Toward Allowing Incarcerated Individuals to be Solid Organ Living Donors in Exchange for a Commuted Sentence
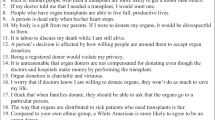
Among respondents who supported the practice of allowing prisoners to be living organ donors, 70.0% opposed the practice in exchange for commuted sentences (Table 3). Of these participants, the primary concerns cited were the possibility of coercion (27%) and the legality of the practice with regard to the National Organ Transplant Act (22%) which explicitly prohibits the exchange of organs for valuable consideration (Fig. 1) [12].

Rationale for commuted sentence exchange disapproval
70.5% of surgeons and 69.1% of non-surgeons opposed the practice of allowing prisoners to become living donors in exchange for a commuted sentence (Table 2). Though differences were not statistically significant, 15.4% of surgeons indicated that they would the practice, while only 7.4% of non-surgeons indicated that they would support the practice (p = 0.85) (Table 2). 5.9% of respondents who reside outside the US believed in allowing donation for a commuted sentence vs. 13.2% of respondents in the US, however this difference was not statistically significant (p = 0.1). Of the 30 respondents who indicated that they would support donation in exchange for a commuted sentence, 56.7% believed that the type of crime should impact whether a sentence can be commuted, and 63.3% believed that there should be restrictions on sentence reductions (Table 3).
Attitudes Toward Including the Opinions of Incarcerated Individuals in the Decision to Allow them to Donate
65.9% of participants believed that the opinions of incarcerated individuals matter when developing living donation policies for incarcerated individuals (Table 3). However, 27.8% of surgeons and 20.8% of non-surgeons did not think the opinions of incarcerated individuals were necessary when developing policies related to their ability to donate (p = 0.59) (Table 2). In the North Central region of the US, 19.0% of respondents indicated that the opinions of incarcerated individuals did not matter when developing policies about their ability to donate, in contrast to 28.7% of respondents in the South.
Discussion
Although there is a paucity of data reporting transplant professionals’ attitudes toward organ donation by incarcerated individuals, including their views on donation in exchange for a commuted sentence, there is ample literature describing the ethical considerations surrounding this practice [4, 13, 14]. The results of this national survey of transplant professionals is intended to add to the growing body of literature on the subject. Results revealed strong support for the practice of permitting incarcerated individuals to be both directed and non-directed living donors. However, opinions on whether these individuals could recover from the donation surgery safely, without risking their physical health, with 44% expressing doubt, 32% remaining uncertain, and 24% affirming belief in the feasibility of recovery.
A 2013 survey of 100 Polish male prisoners found that 82% trusted the medical and transplant communities and 60% would consider donating their own organs [15]. While no such study has ever been conducted in the U.S., most respondents surveyed for this study agreed that the opinions of incarcerated individuals should be considered when establishing prisoner donation policies. As such, future research should attempt to assess incarcerated individuals’ own attitudes towards organ donation and their willingness to become living donors while incarcerated.
The results of this survey must be framed in the context of their limitations. The survey instrument was not validated. However, survey items were created based on existing literature, vetted by experts in the field of transplant ethics, and pre-tested with members of the study population to assess clarity and face-validity. Our survey questions were not designed to account for the varying conditions at different correctional facilities (i.e. recovery post-donation in a low-level security facility with high levels of inmate violence vs. recovery post-donation in a high-security facility with greater inmate safety). Additionally, the low response rate could have introduced non-response bias. Furthermore, over 14% of the study sample reported their profession as “other”, so it is impossible to report whether these respondents were psychologists, coordinators, advocates, or other members of transplant community. Lastly, our survey asked about coercion without defining the term for respondents. While most respondents were likely familiar with the term as described in the Belmont Report, it is possible that some did not understand what coercion mean in the context of the question.
Although most respondents supported the concept of incarcerated individuals becoming both directed and non-directed living donors, most were opposed to the concept of donation in exchange for a reduced or commuted sentence. Future research in this area should attempt to understand the attitudes of not only transplant surgeons and physicians, but also coordinators, social workers, psychologists, administrators, and ethicists to provide a broader range of transplant professionals’ opinions. The opinions of psychologists, particularly those responsible for evaluating living donors, could also provide a great deal of insight, as a great majority of inmates often have psychiatric disorders that make them ineligible for organ donation or that can cause major post-donation complications [16,17,18,19]. Because only 40% of U.S. carceral systems have accessible policies surrounding organ donation by incarcerated individuals, the results of this survey can be used to inform future organ donation policies for other U.S. carceral systems [20].
Data Availability
No datasets were generated or analysed during the current study.
Abbreviations
- U.S:
-
United States
References
An Act to establish the Massachusetts incarcerated individual bone marrow and organ donation program, HD3822, Massachusetts House of Representatives, 193 sess. (2023). Accessed June 16, 2023. https://trackbill.com/bill/massachusetts-house-docket-3822-an-act-to-establish-the-massachusetts-incarcerated-individual-bone-marrow-and-organ-donation-program/2332133/.
Caplan A, Sisti D. Asking incarcerated people for their organs is exploitative. Boston Globe (Online). Feb. 8, 2023. Accessed June 27, 2023. https://www.bostonglobe.com/2023/02/08/opinion/asking-incarcerated-people-their-organs-is-exploitative/.
Legality of Alternative Organ Donation Practices Under 42 U.S.C. § 274e. (2007).
Caplan A. The Use of Prisoners as Sources of Organs–An Ethically Dubious Practice. Am. J. Bioeth. 2011/10/01 2011;11(10):1–5. https://doi.org/10.1080/15265161.2011.607397.
Gordon BG. Vulnerability in Research: basic ethical concepts and General Approach to Review. Ochsner J Spring. 2020;20(1):34–8. https://doi.org/10.31486/toj.19.0079.
Ethical. and Policy issues in Research Involving Human participants. National Bioethics Advisory Commission; 2001.
Organ Procurement & Transplantation Network (OPTN); U.S. Department of Health and Human Services; Health Resources and Services Administration. The Ethics of Organ Donation from Condemned Prisoners. Accessed May 9. 2024. https://optn.transplant.hrsa.gov/professionals/by-topic/ethical-considerations/the-ethics-of-organ-donation-from-condemned-prisoners/.
Kendig NE, Bur S, Zaslavsky J. Infection Prevention and Control in Correctional Settings. Emerg Infect Dis. 2024;30(13):88–93. https://doi.org/10.3201/eid3013.230705.
45 CFR. § 46; Part 46—Protection of Human Subjects.
Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inf Jul. 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inf Apr. 2009;42(2):377–81. https://doi.org/10.1016/j.jbi.2008.08.010.
National Organ Transplant Act, No PL. PL 98–507, 42 98 §§ 273–274 (U.S. Government Publishing Office 1984). Accessed June 27, 2023. https://www.govinfo.gov/app/details/STATUTE-98/STATUTE-98-Pg2339.
Bagatell SJ, Owens DP, Kahn MJ. Organ donation by a prisoner: legal and ethical considerations. J La State Med Soc Jan-Feb. 2010;162(1):44–6.
Miller FG. Is It Ethical to Reduce Prison Sentences in Exchange for Organ Donation. February 3, 2023. Accessed June 20, 2023. https://www.thehastingscenter.org/is-it-ethical-to-reduce-prison-sentences-in-exchange-for-organ-donation/.
Durczyński A, Pietrzak M, Strzelczyk J. Preliminary report from a prison survey: should prisoners be considered as organ donors? Ann Transpl Nov. 2013;8:18:604–8. https://doi.org/10.12659/aot.889634.
Fazel S, Hayes AJ, Bartellas K, Clerici M, Trestman R. Mental health of prisoners: prevalence, adverse outcomes, and interventions. Lancet Psychiatry. 2016;3(9):871–81. https://doi.org/10.1016/S2215-0366(16)30142-0.
Baranyi G, Fazel S, Langerfeldt SD, Mundt AP. The prevalence of comorbid serious mental illnesses and substance use disorders in prison populations: a systematic review and meta-analysis. Lancet Public Health. 2022;7(6):e557–68. https://doi.org/10.1016/S2468-2667(22)00093-7.
Baranyi G, Scholl C, Fazel S, Patel V, Priebe S, Mundt AP. Severe mental illness and substance use disorders in prisoners in low-income and middle-income countries: a systematic review and meta-analysis of prevalence studies. Lancet Global Health. 2019;7(4):e461–71. https://doi.org/10.1016/S2214-109X(18)30539-4.
Trzepacz PT, DiMartini AF. The transplant patient: Biological, psychiatric and ethical issues in organ transplantation. Cambridge University Press; 2000.
Iwai Y, Behne MF, Long JM, Brinkley-Rubinstein L. US Prison policies on Organ Donation for individuals who are incarcerated. JAMA Netw Open. 2023;6(3):e232047–232047. https://doi.org/10.1001/jamanetworkopen.2023.2047.
Acknowledgements
This work was supported by grant number K24AI144954 (Segev) from the National Institute of Allergy and Infectious Diseases (NIAID). The analyses described here are the responsibility of the authors alone and do not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products or organizations imply endorsement by the U.S. Government. The editors would like to thank Dr. Ana Iltis for handling the review of this manuscript.
Author information
Authors and Affiliations
Contributions
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work: MLL, KK, SBK, SSP, ABM, CNS, DLS, AC, BP. Drafting the work or revising it critically for important intellectual content: KK, SBK, SSP. Final approval of the version to be published: MLL, KK, SBK, SSP, ABM, CNS, DLS, AC, BP. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: MLL, KK, SBK, SSP, ABM, CNS, DLS, AC, BP.
Corresponding author
Ethics declarations
Competing interests
The authors of this manuscript have no conflicts of interest to disclose as described by Transplantation Direct.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Katya Kaplow and Samantha B. Klitenic Co-first author.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kaplow, K., Klitenic, S.B., Patel, S.S. et al. Understanding Transplant Professionals’ Attitudes Toward Organ Donation by Incarcerated Individuals: A First Look. Curr Transpl Rep 11, 169–175 (2024). https://doi.org/10.1007/s40472-024-00437-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40472-024-00437-5