
Abstract
Background
Hamstrings muscle morphology is determinant of muscle function (i.e. strength). Among individuals with ACL reconstruction (ACLR), less cross-sectional area (CSA) and volume in the ACLR-limb are associated with muscle weakness, and may contribute to lower rates of return to preinjury activity level and an increased risk for long-term sequelae.
Objectives
To effectively treat muscular impairments, an accurate understanding of differences in hamstrings morphology following ACLR is needed. A systematic review and meta-analysis were undertaken to describe the morphology of the hamstring muscle complex after ACLR.
Methods
We searched five databases for studies evaluating the difference between hamstrings size and architecture in individuals with ACLR. Two independent reviewers assessed each paper for inclusion and quality. Means and standard deviations were extracted from each included study to allow fixed-effect size meta-analysis calculations for comparison of results.
Results
Twenty-four studies were included for final review. Eight categories of morphological outcomes were identified, and studies were grouped accordingly: (1) volume, (2) cross-sectional area (CSA), (3) muscle length, (4) muscle thickness, (5) fascicle length, (6) pennation angle, (7) fiber area, and (8) fiber type. Meta-analysis demonstrated lower hamstrings volume in the ACLR-limb in both contralateral and control group comparisons, and lower CSA, length, and thickness in the ACLR-limb in contralateral comparisons. The semitendinosus and gracilis were most profoundly impacted. Limited moderate evidence demonstrated greater biceps femoris pennation angle in the ACLR-limb.
Conclusions
Individuals with ACLR demonstrated large deficits in semitendinosus and gracilis muscle CSA and volume in the ACLR-limb compared contralaterally, with no differences observed in the biceps femoris or semimembranosus. Clinical implications regarding assessment and treatment of individuals with ACLR are discussed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1. Moderate-to-high quality evidence demonstrates large ACLR-limb deficits in semitendinosus and gracilis muscle volume and cross-sectional area compared to the contralateral limb in both the short- and long-term post-surgery. |
2. Limited evidence suggests ACLR-limb differences in biceps femoris long head architecture compared to the contralateral limb despite no differences in size: specifically, shorter fascicle length and greater pennation angle without differences in cross-sectional area or volume. |
3. Although limited, moderate-to-high quality evidence demonstrates large ACLR-limb deficits in semitendinosus muscle volume compared to uninjured controls. |
1 Introduction
As a dynamic knee stabilizer against anterior tibial translation and the primary anterior cruciate ligament (ACL) agonist [1], hamstrings muscle function is a critical component of injury recovery following ACL reconstruction (ACLR) [2,3,4]. Despite this, individuals commonly fail to meet hamstrings-related (i.e. knee flexion) strength criteria at time of return to sport decision making [2]. These findings are concerning considering recent works demonstrating lower hamstrings muscle activity [3] and lower strength [5] are risk factors for secondary ACL injury. Muscular impairments like these are modifiable, yet continue into the chronic stages of recovery and life after ACLR [6, 7]. For example, lower hamstrings volume, a morphological impairment, is strongly associated with acute and chronic knee flexor weakness [8,9,10,11,12], a clinical impairment present up to 25 years following ACLR [12, 13]. Furthermore, these inter-limb morphological differences may be most pronounced in individuals with semitendinosus and gracilis tendon autograft [6, 7, 14, 15]. In order for clinicians to better address post-traumatic hamstrings dysfunction, the presence and degree of morphological impairments must be detailed.
Inter-limb differences in hamstrings morphology have been characterized relative to size (e.g. muscle volume, cross-sectional area [CSA], length, or thickness) or architecture (e.g. fascicle length, pennation angle, fiber area, and fiber type) using musculoskeletal imaging or muscle biopsy approaches (Table 1 contains a detailed description of each outcome). Studies characterizing hamstrings muscle size have independently detailed that lower ACLR-limb hamstrings size coincides with clinical impairments, such as ipsilateral knee flexor weakness [7, 9, 12, 16, 17]. More recently, authors have used muscle volume and CSA to help identify clinical targets by determining the extent of individual muscle contributions to joint action following ACLR [18]. In contrast, studies of hamstrings muscle architecture attempt to determine if mechanical (e.g. pennation angle, fiber size) and physiologic properties (e.g. fiber type) result in deficits in subclinical muscle behavior (e.g. lower force-generating capacity, reduced working range of motion, or altered oxidative capacity) (Table 1) [10, 17, 19]. Collectively, outcomes of muscle size and architecture can describe multidimensional morphological impairments and may implicate targeted clinical interventions following ACLR. Therefore, the purpose of this review was to compare the commonly described metrics of hamstrings morphology of the ACLR-limb relative to contralateral and uninjured control limbs. We hypothesized that the ACLR-limb would demonstrate hamstrings muscle size and architecture deficits compared to contralateral and control limbs, specifically of the muscles of grafted tendons (i.e. semitendinosus and gracilis).
2 Methods
2.1 Registration
We conducted this systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement and registered with PROSPERO prior to completion of the initial search (registration No: CRD42018110824, approval date: Oct 15th, 2018). PROSPERO was searched to ensure no similar reviews were ongoing at time of registration. As this systematic review was intended to serve as a comprehensive assessment of hamstrings neuromuscular function and morphology following ACLR, we performed the search collectively to exhaust the literature on the topic. Due to the scope of our preliminary findings, we divided the study results into two manuscripts based on categories of outcome measures and have presented all muscle morphology-derived outcome measures in this manuscript.
2.2 Search Strategy
Studies were included if (a) the study population included adults following primary unilateral ACLR, (b) graft types included autograft (bone-patellar tendon-bone [BTB] or hamstring tendon [HT]), and (c) outcomes regarding hamstrings muscle morphology were published. Studies were excluded if (a) the study populations included adolescents (under 18 years of age) or elderly (over 70 years or age) individuals, or (b) individuals underwent ACL revision surgery. Studies that also included a comparison group of individuals who were ACL deficient were included, but those data were not considered for meta-analysis.
We searched the electronic bibliographical databases of PubMed, Web of Science, SPORTDiscus, CINAHL, and EBSCOhost (MEDLINE) from inception to August 12th, 2020.
For morphological outcomes, the search strategy included key terms relating to the population (e.g. anterior cruciate ligament injury OR anterior cruciate ligament reconstruction OR anterior cruciate ligament injuries) and describing variables of interest (e.g. morphology OR stiffness OR cross-sectional area OR CSA OR pennation angle OR fiber length OR volume OR fascicle, etc.). Since there is no universal definition of morphological characteristics, this search strategy comprised a widespread spectrum to capture all potentially relevant studies. The search terms were adapted for database specific filters and language as appropriate. Electronic Supplementary Material Appendix S1 contains an example search for PubMed.
The search was restricted to English language studies. Unpublished research was not considered as it was deemed impractical to identify all unpublished work on hamstrings muscle morphology associated with ACLR.
2.3 Study Selection
A single investigator (DAS) exported all studies identified by the search strategy to Endnote X9 (Clarivate Analytics, Jersey). Any duplicates were then deleted using the deduplication feature. The titles and abstracts of all publications were then screened by a single investigator (DAS), and any further duplicates identified were removed during this step. Full texts were obtained where eligibility could not be determined by the abstract. Any uncertainties were reviewed by a second reviewer (JLR) and were resolved at a consensus meeting.
2.4 Quality Assessment
Two independent reviewers (DAS and JLR) assessed the quality of all the included studies using the modified Newcastle–Ottawa Scale (mNOS). Electronic Supplementary Material Appendix S2 contains the mNOS template. All criteria were defined, discussed in detail, and approved by all investigators during a consensus meeting prior to qualitative assessment. Although not developed specifically for ACL research, the mNOS is increasingly recommended for the qualitative assessment of observational studies [20]. The mNOS was applied using pen and paper. Discrepancies were resolved at a consensus meeting. Lack of agreement was resolved by a third reviewer (GEN).
The mNOS contains eight categories (total of 9 possible points) relating to methodological quality. A score of 0–3 points was considered a low quality study, a score of 4–6 points was considered a moderate quality study, and a score of 7–9 points was considered a high-quality study.
2.5 Outcome Measures
The outcome measures considered in this review are metrics of muscle morphology. For a description and utility of each, see Table 1.
2.6 Data Extraction
The following information was extracted from each of the publications by the primary investigator (DAS):
-
(a)
Publication information.
-
(b)
Patient descriptors: sample size, sex, age, height, weight, source of graft, sport (if any), level of participation (if specified).
-
(c)
Study methods: including study design, muscles assessed, method of assessment.
-
(d)
Filtering and processing technique applied to imaging data.
-
(e)
Outcome measures: muscle volume, muscle cross sectional area, muscle .thickness, muscle length, fascicle length, pennation angle, fiber area, and fiber type.
In individuals with ACLR, comparisons were made between limbs (ACLR-limb to contralateral) and to uninjured (control) individuals. In cases where longitudinal studies included multiple post-operative examinations, both time points were extracted. Corresponding authors were contacted for original data where publications did not report in text. Engauge Digitizer software (Open Source, Version 11.2) [21] was used to extract data from figures [10, 12, 22] when authors were unable to recover the original data files, or did not respond to requests.
2.7 Statistical Methods
Statistical analysis was completed using Review Manager 5 (The Cochrane Collaboration, Copenhagen, Denmark). Analyses were completed initially by one investigator (DAS). Standardized mean difference (SMD) and 95% confidence interval (CI) calculations are reported using Hedges’ g effect sizes. Calculated individual or pooled SMD were categorized as small (≤ 0.50), medium (0.51–0.79), or large (≥ 0.80) [23].
For studies that specified results for individual hamstrings muscles (e.g. semitendinosus [ST], biceps femoris long-head [BF LH], etc.), data were analyzed as subgroup comparisons. For studies that specified results based on sex or graft type, data were pooled and have been presented as a heterogeneous cohort. Where methods and outcome measures were comparable between studies, a meta-analysis was performed and the level of statistical heterogeneity for pooled data was established using the χ2 and I2 statistics (heterogeneity defined as I2 > 50%, p < 0.05).
The level of evidence, incorporating the methodological quality and I2 statistical analysis, was calculated for each outcome variable, following the recommendations of van Tulder et al. [24]. Pooled results from three or more studies, including two high quality homogenous studies, were classified as strong evidence. Pooled results from multiple studies, including at least one high-quality heterogeneous study or multiple moderate quality or low-quality homogenous studies, were classified as moderate evidence. Results from one high-quality or multiple moderate- or low-quality studies that were heterogeneous were classified as limited evidence. Results from one moderate- or low-quality study were classified as very limited evidence.
3 Results
3.1 Search Results
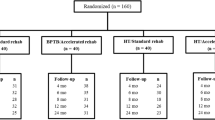
For detail of search results, including deduplication, exclusion, and full-text review, see Fig. 1. Following screening of titles and abstracts, 71 publications were retained, and full text reviewed. Twenty-four studies were included for final review.

Flow diagram summarizing study selection for inclusion
In total, the data from 443 unique individuals were considered with at least 55.3% of the sample being female (n ≥ 245). The majority of individuals underwent ACLR with HT autograft (84.9%, n = 376), followed by BTB (10.6%, n = 47), undefined graft source (3.6%, n = 16), and iliotibial band (0.9%, n = 4). Population sources, sample sizes, demographic descriptors are reported in Table 2. Study design, muscles, morphology variables, and acquisition techniques are reported in Table 3. The range of time from surgery was 3–142 months.
3.2 Methodological Quality Assessment
Results from the modified Newcastle Ottawa Scale (mNOS) are shown in Table 4. The median score was 5 (range 3–8) out of 9. Of the 24 studies, 4 (16.7%) were rated as high quality [9, 17, 22, 25], 17 (70.8%) were rated as moderate quality [6,7,8, 10,11,12, 14, 18, 19, 26,27,28,29,30,31,32,33], and 3 (12.5%) were rated as low quality [34,35,36].
3.3 Volume
Twelve studies [6,7,8,9,10,11,12, 18, 25, 28, 31, 35] evaluated hamstrings muscle volume (Fig. 2), specifically investigating the ST (n = 9), semimembranosus (SM) (n = 6), BF LH (n = 5), BF short head (BF SH) (n = 4), BF nonspecific (n = 2), gracilis (n = 4) and overall muscles (n = 2). Studies were of low (n = 1), moderate (n = 8), and high (n = 2) quality. The ACLR-limb demonstrated smaller hamstrings volume than the contralateral limb (g = − 0.36, 95% CI [− 0.48, − 0.23]). Specifically, there were large magnitude deficits in the ACLR-limb ST (g = − 0.98, 95% CI [− 1.22, − 0.74]) and gracilis (g = -– 0.83, 95% CI [− 1.19, − 0.48]) volume compared to the contralateral limb. Conversely, there were no differences in muscle volume of the SM or BF between ACLR and contralateral limbs. There was no discernible pattern in outcomes when considering the time from surgery from individual studies; for example, ST and gracilis volume were similarly smaller (majority with overlapping 95% CI) in the ACLR-limb at time points ≤ 9 months [6, 11] and > 4 years [7, 9, 18]. Of the 11 studies, 8 included only individuals with HT graft sources. To further determine the influence of HT graft type, we systematically eliminated studies with PT [35] or heterogenous samples [9, 25]. There were no changes in effect size when including only individuals with HT graft (i.e. ST: g = − 1.05, 95% CI [− 1.30, − 0.80], gracilis: g = − 1.15, 95% CI [− 1.72, − 0.58], overall: g = − 0.37, 95% CI [− 0.52, − 0.23]) (Electronic Supplementary Material Appendix S3).

Inter-limb comparison of hamstrings volume. (1) 6 months post-ACLR, (2) 12 months post-ACLR. ACLR-limb Anterior cruciate ligament reconstruction limb, SD Standard deviation, Std. standard, CI confidence interval
Three studies [6, 9, 11] evaluated ST, SM, and BF volume of the ACLR-limb in comparison to healthy controls. Two of these studies [9, 11] were entered in meta-analysis (Fig. 3). Here, the ACLR-limb demonstrated a negligible, but statistically significant, deficit in overall hamstrings volume (g = − 0.29, 95% CI [− 0.50, − 0.08]) compared to controls. This was characterized by large magnitude deficits in the ACLR-limb ST (g = − 1.01, 95% CI [− 1.40, − 0.62]) without differences in SM (g = 0.01, 95% CI [− 0.36, 0.37]) or BF (g = − 0.01, 95% CI [− 0.34, -− 0.32]).

Comparison of hamstring volume between ACLR-limb and controls. (1) 6 months post-ACLR, (2) 12 months post-ACLR, (3) biceps femoris long head, (4) biceps femoris short head. ACLR Anterior cruciate ligament reconstruction limb, SD Standard deviation, Std. standard, CI confidence interval
3.4 Cross-Sectional Area
Thirteen studies [7, 12, 14, 18, 19, 22, 26, 29,30,31,32,33, 36] evaluated hamstrings muscle CSA (Fig. 4), specifically investigating the ST (n = 10), SM (n = 6), BF LH (n = 2), BF SH (n = 2), BF nonspecific (n = 4), gracilis (n = 6) or overall muscles (n = 3). Studies were of low (n = 2) to moderate (n = 11) quality. The ACLR-limb demonstrated smaller hamstrings CSA than the contralateral limb (g = -– 0.41, 95% CI [− 0.51, − 0.31]). There were moderate and large magnitude deficits in the ACLR-limb ST (g = − 0.73, 95% CI [− 0.90, − 0.55]) and gracilis (g = − 1.01, 95% CI [− 1.26, − 0.77]) CSA compared to the contralateral limb. Conversely, there were no differences in CSA of the SM or BF muscles between limbs. There was no discernible pattern in outcomes when considering the time from surgery from individual studies; for example, ST and gracilis volume were similarly smaller (overlapping 95% CI) in the ACLR-limb at time points ≤ 9 months [19, 30] and > 2 years [7]. Of the 13 studies, 10 included only individuals with HT graft sources. To further determine the influence of HT graft type, we systematically eliminated studies with PT [22] or heterogenous samples [19, 34]. There were no changes in effect size when including only individuals with HT graft (ST: g = − 0.73, 95% CI [− 0.91, − 0.55], gracilis: g = − 1.01, 95% CI [− 1.26, − 0.77], overall: g = − 0.42, 95% CI [− 0.52, − 0.31]) between this and the original comparison (Electronic Supplementary Material Appendix S4).

Inter-limb comparison of hamstrings cross sectional area. (1) 3 months post-ACLR, (2) 6 months post-ACLR, (3) 12 months post-ACLR, (4) measured at 50% of femur length, (5) measured at 70% of femur length, (6) measured at 5 cm proximal to patella, (7) measured at 10 cm proximal to patella, and (8) measured at 15 cm proximal to patella. ACLR-limb Anterior cruciate ligament reconstruction limb, SD Standard deviation, Std. standard, CI confidence interval
One high-quality study [22] compared hamstrings CSA of the ACLR-limb to healthy controls. In five individuals with PT autografts, the ST was observed to have greater CSA than the control group, while the BF CSA was significantly lower.
3.5 Muscle Length
Three moderate quality studies [8, 18, 28] evaluated hamstrings muscle length using MRI (Fig. 5), specifically investigating the ST (n = 3), SM (n = 1), BF LH (n = 1), and BF SH (n = 1). The ACLR-limb demonstrated shorter hamstrings muscle length than the contralateral limb (g = − 0.74, 95% CI [− 1.06, – 0.41]). However, large deficits in ACLR-limb ST (g = − 1.72, 95% CI [− 2.22, − 1.23]) length drove this effect, as there were no differences in muscle length of the SM, BF LH, or BF SH between limbs.

Inter-limb comparison of hamstrings length. Abbreviations: ACLR-limb Anterior cruciate ligament reconstruction limb, SD Standard deviation, Std. standard, CI confidence interval
3.6 Muscle Thickness
Three studies [17, 27, 32] evaluated hamstrings muscle thickness using musculoskeletal ultrasound. Two included comparison to the contralateral limb (Fig. 6) investigating the semitendinosus (ST) [32] and long head of biceps femoris (BF LH) [17]. The ACLR-limb demonstrated smaller hamstrings muscle thickness than the contralateral limb (g = − 0.40, 95% CI [− 0.66, − 0.13]) with small magnitude deficits in ST (g = − 0.42, 95% CI [− 0.73, − 0.11]) and no difference in BF LH (g = − 0.35, 95% CI [− 0.86, 0.16]) muscle thickness. One study [17] also included comparison of the ACLR-limb BF LH thickness to controls and found no difference. The third study [27] reported a large magnitude difference in the ACLR-limb ST muscle thickness being higher at rest and during MVIC compared to controls [27].

Inter-limb comparison of hamstrings thickness. (1) 3 months post-ACLR, (2) 6 months post-ACLR, (3) 12 months post-ACLR, (4) measured at rest, (5) measured at 25% of maximum voluntary isometric contraction. ACLR-limb Anterior cruciate ligament reconstruction limb, SD Standard deviation, Std. standard, CI confidence interval
3.7 Fascicle Length
One high-quality study [17] evaluated BF LH fascicle length using musculoskeletal ultrasound [17], and reported a large magnitude deficit in the ACLR-limb (shorter fascicle length) compared to the contralateral limb and controls both at rest and during isometric contraction at 25% MVIC.
3.8 Pennation Angle
Two studies [17, 27] evaluated hamstrings pennation angle using musculoskeletal ultrasound. One study [27] reported no difference in ACLR-limb ST pennation angle at rest or during MVIC compared to controls. The second [17] included comparison of the ACLR-limb BF LH pennation angle to the contralateral side and controls. Here, the ACLR-limb demonstrated a greater pennation angle compared to the contralateral limb at rest, and during isometric contraction at 25% MVIC. Although there was no difference in pennation angle compared to controls, individuals with ACLR did demonstrate greater inter-limb asymmetry in pennation angle compared to controls.
3.9 Fiber Area and Fiber Type
One moderate-quality study [19] evaluated ST fiber area and type using biopsy. This study reported no differences in ST fiber area or fiber type distribution within-limbs or between-limbs from pre- to post-surgery.
3.10 Heterogeneity of Studies
Hamstrings volume (ACLR-limb to contralateral comparison I2 = 66.0%, ACLR-limb to control comparison I2 = 68.0%), CSA (I2 = 69.0%), and length (I2 = 94.0%) all demonstrated a high degree of heterogeneity upon meta-analysis. Muscle thickness demonstrated a low degree of heterogeneity (I2 = 0.0%).
4 Discussion
This systematic review and meta-analysis presents a broad spectrum of hamstrings morphological characteristics in individuals with ACLR. There is currently a moderate level of evidence that the ST and gracilis muscles demonstrate less volume and CSA in the ACLR-limb with inter-limb comparison. Lower volume is also present in the ACLR-limb compared to controls. In addition, there is limited to moderate evidence of shorter ST length and smaller thickness, as well as shorter BF LH fascicle length and greater pennation angle in the ACLR-limb compared contralaterally. Very limited evidence suggest ST fiber type distribution is preserved following ACLR. The included studies varied in methodological quality, acquisition techniques, muscle of interests, and operational definition of outcomes, likely contributing to the high degree of heterogeneity observed in meta-analysis of volume, CSA, and muscle length. Collectively, these findings suggest that inter-limb hamstrings morphological differences are present in individuals during both subacute and chronic stages of recovery following ACLR. Differences in size (volume, CSA, length, and thickness) seem to be unique to graft source musculature (ST and gracilis). As muscle morphology traditionally represents a modifiable clinical impairment, the results and the clinical implications of these findings are discussed by category.
4.1 Volume
The ACLR-limb to contralateral limb comparison demonstrated large magnitude deficits in ST and gracilis volume, whereas the SM and BF muscles were not different. Overall, there were small magnitude deficits in hamstrings volume in the ACLR-limb, driven by ST and gracilis differences. Similarly, the ACLR-limb to control comparison demonstrated a large magnitude deficit in the ACLR-limb ST without differences in SM or BF. As an estimate of three-dimensional muscle size, volumetric assessment is the most comprehensive assessment of muscle size and can account for post-operative changes in muscle length due to graft source, presence of neotendon (regeneration of grafted tendon), and proximal shift of the musculotendinous junction [6, 12, 31]. Collectively, these results demonstrate the scope of a profound loss of graft source muscle volume. This effect may have occurred due to the large percentage of the sample having undergone ACLR with HT autograft. Due to the low sample, we were unable to determine if this pattern of loss exists in those with PT graft. Three longitudinal studies reported significant muscle volume loss of the gracilis [6, 25] and ST [6] from pre-surgery to 6-months post-surgery despite rehabilitation. With regard to time from surgery, although limited by pooled analysis, there was no significant pattern of volumetric differences between the subacute [6, 11] and chronic [7, 9, 18] samples included in this meta-analysis, which suggests persistent impairment.
As the medial hamstrings are the primary dynamic restraint against tibial external rotation [37], these findings are particularly concerning and may indicate that hamstrings muscle impairments are overlooked in rehabilitation. These results suggest that clinicians should devote more attention to hamstrings hypertrophy exercise to specifically target ST and gracilis, such as eccentric training [38, 39]. Selected eccentric hip and knee dominant exercises have been shown to selectively activate the medial hamstrings [40, 41]. Furthermore, consideration must be given to evidence [18] that suggests persistent ST volume impairments (and low level of activation during supramaximal exercise [18]) indicate the ST is not loaded adequately to stimulate muscle growth following ACLR. Since the SM is also a knee internal rotator (as well as hip extensor) and is unimpaired according to our results, targeting SM hypertrophy to compensate for ST atrophy may be appropriate. Evidence-based treatment approaches to guide hamstrings recovery in this population are needed.
4.2 Cross-Sectional Area
Similar to volume, the ST and gracilis both demonstrated large magnitude deficits in CSA in the ACLR-limb compared to the contralateral limb, whereas no differences were observed in the SM and BF muscles. Overall, there were small magnitude deficits in total hamstrings CSA in the ACLR-limb compared to the contralateral limb of individuals with ACLR. Conversely, one study comparing the ACLR-limb to controls [22] reported a small increase in ST and decrease in BF CSA. These findings suggest an individualized muscle response and appear to detail selective atrophy of the ST and gracilis as an autogenous graft source [14]. With regard to time from surgery, although limited by pooled analysis, there was no significant pattern of CSA differences between the subacute [19, 30] and chronic [7] samples included in this meta-analysis, which suggests persistent impairment.
Hamstrings CSA is strongly associated with knee flexion strength and represents a clinically relevant and accessible assessment [12, 42]. However, differences in acquisition technique must be considered when interpreting results. For example, the relative location of peak CSA may differ between-limb and between-individuals [12, 22]. While MRI acquisition allows for scanning of the entire muscle length and statistical consideration of the CSA at the largest point [12], musculoskeletal ultrasound is limited by assessment at standardized anatomical locations [32]. Regardless, muscle CSA captured by panoramic musculoskeletal ultrasound constitutes a clinically accessible and reliable technique for quantifying hamstrings muscle size [32, 43]. Despite considerable barriers posed by sonographer experience and imaging processing training [43], the potential benefits of muscle size assessment in the clinic and during activity [17, 27, 32] warrant future investigation.
4.3 Muscle Length
There is limited evidence reporting large magnitude deficit in ST muscle length was observed in the ACLR-limb compared to the contralateral limb. Although outside the scope of this review, greater neotendon cross-sectional area and length were described in two studies compared to the contralateral limb [8, 28]. Collectively, increased tendon length and shorter muscle length indicate that there is a significant change in muscle–tendon morphology of the ST, constituting a proximal shift of the distal musculotendinous junction. This directly influences the length–tension curve of the hamstrings [8] and manifests clinically as weakness in deep knee flexion (e.g. active insufficiency) [8, 28].
4.4 Muscle Thickness
There is limited evidence reporting small magnitude deficit in ST muscle thickness was observed in the ACLR-limb compared to the contralateral limb [32], whereas no differences were observed in the BF LH [17]. Muscle thickness captured by musculoskeletal ultrasound constitutes a clinically accessible technique for quantifying muscle size deficits [32]. In particular, hamstrings muscle thickness at 50% thigh length has been shown to be highly associated with both MRI CSA and volumetric assessments [42]. However, limitations in the assessment technique and population-specific considerations (i.e. proximal shift of distal musculotendinous junction [12]) may have contributed to conflicting results. Namely, one-dimensional assessment fails to consider muscle width or length [43], such as potential changes in location of maximal muscle CSA along its length following ST/gracilis graft [12]. Considering the magnitude of impairments in higher dimensional morphological analyses (e.g. CSA and volume as discussed), additional research regarding the clinical utility of this approach in this population is warranted.
4.5 Fascicle Length
There is limited evidence reporting BF LH fascicle length in individuals with ACLR. The one included study [17] reported a large magnitude deficit in the ACLR-limb compared contralaterally and to controls both at rest and during isometric contraction at 25% MVIC. In combination with shorter hamstrings length, shorter fascicle length represents fewer sarcomeres in series, which shortens a muscle’s active range of motion and may theoretically contribute to hamstring strain injuries [44, 45]. However, research is needed to determine whether such fascicle length deficits influence hamstrings injury risk after ACLR. Recent evidence demonstrates that eccentric exercise training effectively increases fascicle length (see Bourne et al. 2018 for review) [39, 41, 46], suggesting a clinically relevant intervention for addressing fascicle length deficits.
4.6 Pennation Angle
There is very limited evidence reporting pennation angle of the hamstrings in individuals with ACLR. In one study [27], the pennation angle of the fusiform ST muscles were not different to that of controls. Conversely, greater BF LH pennation angle coincides with the observed decreases in fascicle length reported above [17], indicating a shift towards sarcomere alignment in parallel rather than in series. The relationship between fascicle length and pennation angle is a well known architectural determinant of muscle function, with larger, pennate muscles being more powerful through shorter ranges of active motion. These results indicate the BF LH may adapt by increasing pennation angle and decreasing fascicle length. This may represent an adaptive strategy to increase muscle strength and power.
4.7 Fiber Area and Fiber Type
There is very limited evidence reporting ST fiber area and fiber type distribution are preserved pre-operatively to post-operatively in individuals with ACLR. The one included study [19] concluded that these findings indicate there is no denervation of hamstrings muscle tissue or changes in hamstrings muscle oxidative metabolism following ACLR. However, considering the low sample size, future work detailing pre- to post-operative fiber area and type of the neighboring knee flexor muscles would be informative.
4.8 Heterogeneity of Results
These meta-analyses were characterized by a large degree of heterogeneity (an I2 statistic greater than 50%), which indicates a large degree of variability in the results. This is likely a representation of the nuances of acquisition or comparison techniques and inclusion of individual hamstring muscle results represented in the collective sample (Table 3). For example, several studies reported mean CSA throughout the entire muscle length, whereas others used a priori defined locations based on femur length, or simply peak CSA. This may also indicate a heterogeneity of individual muscle morphologies following ACLR. We have included subgrouping by hamstring muscles in effort to demonstrate the drivers of this heterogeneity for each outcome of interest. The means and standard deviations from included studies represent either reporting of overall volume or percent difference between limbs. Although use of standardized mean difference is not considered a limitation in meta-analysis, this prevented use of the more clinically meaningful mean differences in our analysis.
4.9 Methodological Quality, Limitations, and Directions for Future Research
There were many methodological limitations identified using the mNOS. For example, only six of the included studies included an uninjured control group (mNOS items 3–5), resulting in the inability to compare each outcome to a control group with meta-analysis. Most notably, this could result in inappropriate comparisons of outcomes to the contralateral limb, a practice that is flawed due to bilateral deficits existing with ACL injury [6, 12, 47, 48]. Some outcomes were represented by only a few studies (i.e. muscle length and thickness, pennation angle, fascicle length, and fiber type and area). Additionally, comparisons of muscle length and thickness were further limited by few studies reporting outcomes for individuals’ muscles. Lastly, changes of architecture over time (and from pre- to post-ACLR) are not clear. These limitations should be addressed in future research.
Musculoskeletal ultrasound is increasingly common in clinical assessment [32, 42, 43]. These results demonstrate that deficits in ACLR-limb CSA, fascicle length, and pennation angle are clinically meaningful and can be identified using this technique [32, 43]. As hamstrings CSA is highly associated with knee flexion strength, the clinical utility of using panoramic musculoskeletal ultrasound to monitor clinical progress toward hypertrophy goals is established [17, 32, 43].
Demographic factors such as sex, age, and graft-type are known to influence muscle recovery [49] and passing traditional return to sport tests following ACLR [2]. Although the majority of the included sample underwent ACLR with HT autograft (84.5%), our primary aim was to characterize the overall effect of ACLR. To this end, the influence of these factors on hamstrings morphology following ACLR is not fully understood. This could not be explored as part of the review and remains an area of further research. Lastly, our inclusion and exclusion criteria did not control for the possibility of multiple confounders, such as contralateral graft sources or rehabilitation regimen.
5 Conclusion
Moderate evidence suggests that individuals with ACLR demonstrate smaller ST and gracilis CSA and volume, shorter ST length, and smaller thickness in the ACLR compared to the contralateral limb. The presence of profound deficits in ST and gracilis may indicate selective atrophy and shortening of graft source muscles. There is limited evidence to suggest that the ACLR-limb BF LH demonstrates shorter fascicle length and greater pennation angle compared contralaterally and to controls. There is very limited evidence indicating that ST fiber area or fiber type distribution are not different between limbs following ACLR. Collectively, these morphological characteristics align with known clinical (e.g. decreased hamstrings muscle strength) impairments, all of which may contribute to poor outcomes seen in this population. The largest of these impairments, ST and gracilis CSA and volume, may be modifiable (or compensated for) by clinical emphasis on medial hamstring hypertrophy. Musculoskeletal ultrasound offers a clinically feasible modality for assessment of both muscle size and architecture. Future research should detail longitudinal architecture changes and determine the utility of clinical morphology assessment techniques (i.e. musculoskeletal ultrasound) in this population.
References
MacWilliams BA, Wilson DR, DesJardins JD, Romero J, Chao EY. Hamstrings cocontraction reduces internal rotation, anterior translation, and anterior cruciate ligament load in weight-bearing flexion. J Orthop Res. 1999;17(6):817–22. https://doi.org/10.1002/jor.1100170605.
Norte GE, Goetschius JW, Slater LV, Hart JM. Influence of patient demographics and surgical characteristics on pass rates of return-to-activity tests in anterior cruciate ligament-reconstructed patients before physician clearance. Clin J Sport Med. 2020. https://doi.org/10.1097/JSM.0000000000000790 (Publish Ahead of Print).
Palmieri-Smith RM, Strickland M, Lepley LK. Hamstring muscle activity after primary anterior cruciate ligament reconstruction-a protective mechanism in those who do not sustain a secondary injury? a preliminary study. Sports Health. 2019;11(4):316–23. https://doi.org/10.1177/1941738119852630.
Sherman D, Birchmeier T, Kuenze CM, Garrison C, Hannon J, Bothwell J, et al. Thigh-muscle and patient-reported function early after anterior cruciate ligament reconstruction: clinical cutoffs unique to graft type and age. J Athl Train. 2020;55(8):826–33. https://doi.org/10.4085/1062-6050-370-19.
Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med. 2016;50(15):946–51. https://doi.org/10.1136/bjsports-2015-095908.
Norte GE, Knaus KR, Kuenze C, Handsfield GG, Meyer CH, Blemker SS, et al. MRI-based assessment of lower-extremity muscle volumes in patients before and after ACL reconstruction. J Sport Rehabil. 2018;27(3):201–12. https://doi.org/10.1123/jsr.2016-0141.
Snow BJ, Wilcox JJ, Burks RT, Greis PE. Evaluation of muscle size and fatty infiltration with MRI nine to eleven years following hamstring harvest for ACL reconstruction. J Bone Jt Surg Am. 2012;94(14):1274–82. https://doi.org/10.2106/JBJS.K.00692.
Nomura Y, Kuramochi R, Fukubayashi T. Evaluation of hamstring muscle strength and morphology after anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 2015;25(3):301–7. https://doi.org/10.1111/sms.12205.
Rush JL, Norte GE, Lepley AS. Limb differences in hamstring muscle function and morphology after anterior cruciate ligament reconstruction. Phys Ther Sport. 2020;45:168–75. https://doi.org/10.1016/j.ptsp.2020.06.012.
Makihara Y, Nishino A, Fukubayashi T, Kanamori A. Decrease of knee flexion torque in patients with ACL reconstruction: combined analysis of the architecture and function of the knee flexor muscles. Knee Surg Sports Traumatol Arthrosc. 2006;14(4):310–7. https://doi.org/10.1007/s00167-005-0701-2.
Konishi Y, Fukubayashi T. Relationship between muscle volume and muscle torque of the hamstrings after anterior cruciate ligament reconstruction. J Sci Med Sport. 2010;13(1):101–5. https://doi.org/10.1016/j.jsams.2008.08.001.
Konrath JM, Vertullo CJ, Kennedy BA, Bush HS, Barrett RS, Lloyd DG. Morphologic characteristics and strength of the hamstring muscles remain altered at 2 years after use of a hamstring tendon graft in anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(10):2589–98. https://doi.org/10.1177/0363546516651441.
Tengman E, Brax Olofsson L, Stensdotter AK, Nilsson KG, Hager CK. Anterior cruciate ligament injury after more than 20 years. II. Concentric and eccentric knee muscle strength. Scand J Med Sci Sports. 2014;24(6):e501–9. https://doi.org/10.1111/sms.12215.
Janssen RP, van der Velden MJ, Pasmans HL, Sala HA. Regeneration of hamstring tendons after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):898–905. https://doi.org/10.1007/s00167-012-2125-0.
Viola RW, Sterett WI, Newfield D, Steadman JR, Torry MR. Internal and external tibial rotation strength after anterior cruciate ligament reconstruction using ipsilateral semitendinosus and gracilis tendon autografts. Am J Sports Med. 2000;28(4):552–5. https://doi.org/10.1177/03635465000280041801.
Tsifountoudis I, Bisbinas I, Kalaitzoglou I, Markopoulos G, Haritandi A, Dimitriadis A, et al. The natural history of donor hamstrings unit after anterior cruciate ligament reconstruction: a prospective MRI scan assessment. Knee Surg Sports Traumatol Arthrosc. 2017;25(5):1583–90. https://doi.org/10.1007/s00167-015-3732-3.
Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Biceps femoris architecture and strength in athletes with a previous anterior cruciate ligament reconstruction. Med Sci Sports Exerc. 2016;48(3):337–45. https://doi.org/10.1249/MSS.0000000000000783.
Messer DJ, Shield AJ, Williams MD, Timmins RG, Bourne MN. Hamstring muscle activation and morphology are significantly altered 1–6 years after anterior cruciate ligament reconstruction with semitendinosus graft. Knee Surg Sports Traumatol Arthrosc. 2020;28(3):733–41. https://doi.org/10.1007/s00167-019-05374-w.
Eriksson K, Hamberg P, Jansson E, Larsson H, Shalabi A, Wredmark T. Semitendinosus muscle in anterior cruciate ligament surgery: Morphology and function. Arthroscopy. 2001;17(8):808–17. https://doi.org/10.1016/s0749-8063(01)90003-9.
Hootman JM, Driban JB, Sitler MR, Harris KP, Cattano NM. Reliability and validity of three quality rating instruments for systematic reviews of observational studies. Res Synth Methods. 2011;2(2):110–8. https://doi.org/10.1002/jrsm.41.
Open-Source. Engauge digitizer software. In: Mitchell M, Muftakhidinov B, Winchen T, van Schaik B, Wilms A, Kensington, et al., editors.: GitHub; 2015. p. Windows 10.
Kellis E, Karagiannidis E, Patsika G. Patellar tendon and hamstring moment-arms and cross-sectional area in patients with anterior cruciate ligament reconstruction and controls. Comput Methods Biomech Biomed Engin. 2015;18(10):1083–9. https://doi.org/10.1080/10255842.2013.869323.
Hedges L, Olkin I. Statistical methods for meta-analysis. Orlando: Academic Press; 1985.
van Tulder M, Furlan A, Bombardier C, Bouter L, Editorial Board of the Cochrane Collaboration Back Review G. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine (Phila Pa 1976). 2003;28(12):1290–9. https://doi.org/10.1097/01.BRS.0000065484.95996.AF.
Gerber JP, Marcus RL, Dibble LE, Greis PE, Burks RT, LaStayo PC. Effects of early progressive eccentric exercise on muscle structure after anterior cruciate ligament reconstruction. J Bone Joint Surg Am. 2007;89(3):559–70. https://doi.org/10.2106/JBJS.F.00385.
Irie K, Tomatsu T. Atrophy of semitendinosus and gracilis and flexor mechanism function after hamstring tendon harvest for anterior cruciate ligament reconstruction. Orthopedics. 2002;25(5):491–5. https://doi.org/10.3928/0147-7447-20020501-15.
Karagiannidis E, Kellis E, Galanis N, Vasilios B. Semitendinosus muscle architecture during maximum isometric contractions in individuals with anterior cruciate ligament reconstruction and controls. Muscles Ligaments Tendons J. 2017;7(1):147–51. https://doi.org/10.11138/mltj/2017.7.1.147.
Nishino A, Sanada A, Kanehisa H, Fukubayashi T. Knee-flexion torque and morphology of the semitendinosus after ACL reconstruction. Med Sci Sports Exerc. 2006;38(11):1895–900. https://doi.org/10.1249/01.mss.0000230344.71623.51.
Burks RT, Crim J, Fink BP, Boylan DN, Greis PE. The effects of semitendinosus and gracilis harvest in anterior cruciate ligament reconstruction. Arthroscopy. 2005;21(10):1177–85. https://doi.org/10.1016/j.arthro.2005.07.005.
Setuain I, Izquierdo M, Idoate F, Bikandi E, Gorostiaga EM, Aagaard P, et al. Differential effects of 2 rehabilitation programs following anterior cruciate ligament reconstruction. J Sport Rehabil. 2017;26(6):544–55. https://doi.org/10.1123/jsr.2016-0065.
Williams GN, Snyder-Mackler L, Barrance PJ, Axe MJ, Buchanan TS. Muscle and tendon morphology after reconstruction of the anterior cruciate ligament with autologous semitendinosus-gracilis graft. J Bone Joint Surg Am. 2004;86(9):1936–46. https://doi.org/10.2106/00004623-200409000-00012.
Gandolfi M, Ricci M, Sambugaro E, Vale N, Dimitrova E, Meschieri A, et al. Changes in the sensorimotor system and semitendinosus muscle morphometry after arthroscopic anterior cruciate ligament reconstruction: a prospective cohort study with 1-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2018;26(12):3770–9. https://doi.org/10.1007/s00167-018-5020-5.
Yoshii R, Konishi Y, Ando D, Ochiai S, Hagino T, Dobashi S. Effect of subcutaneous tissue on changes in thigh circumference following anterior cruciate ligament reconstruction. Int J Sports Med. 2019;40(8):544–50. https://doi.org/10.1055/a-0893-5838.
Arangio GA, Chen C, Kalady M, Reed JF 3rd. Thigh muscle size and strength after anterior cruciate ligament reconstruction and rehabilitation. J Orthop Sports Phys Ther. 1997;26(5):238–43. https://doi.org/10.2519/jospt.1997.26.5.238.
Rebai H, Barra V, Laborde A, Bonny JM, Poumarat G, Coudert J. Effects of two electrical stimulation frequencies in thigh muscle after knee surgery. Int J Sports Med. 2002;23(8):604–9. https://doi.org/10.1055/s-2002-35525.
Takeda Y, Kashiwaguchi S, Matsuura T, Higashida T, Minato A. Hamstring muscle function after tendon harvest for anterior cruciate ligament reconstruction: evaluation with T2 relaxation time of magnetic resonance imaging. Am J Sports Med. 2006;34(2):281–8. https://doi.org/10.1177/0363546505279574.
Flaxman TE, Alkjaer T, Simonsen EB, Krogsgaard MR, Benoit DL. Predicting the functional roles of knee joint muscles from internal joint moments. Med Sci Sports Exerc. 2017;49(3):527–37. https://doi.org/10.1249/MSS.0000000000001125.
Bourne MN, Opar DA, Williams MD, Shield AJ. Eccentric knee flexor strength and risk of hamstring injuries in rugby union: a prospective study. Am J Sports Med. 2015;43(11):2663–70. https://doi.org/10.1177/0363546515599633.
Pollard CW, Opar DA, Williams MD, Bourne MN, Timmins RG. Razor hamstring curl and Nordic hamstring exercise architectural adaptations: Impact of exercise selection and intensity. Scand J Med Sci Sports. 2019;29(5):706–15. https://doi.org/10.1111/sms.13381.
Bourne MN, Williams MD, Opar DA, Al Najjar A, Kerr GK, Shield AJ. Impact of exercise selection on hamstring muscle activation. Br J Sports Med. 2017;51(13):1021–8. https://doi.org/10.1136/bjsports-2015-095739.
Bourne MN, Timmins RG, Opar DA, Pizzari T, Ruddy JD, Sims C, et al. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med. 2018;48(2):251–67. https://doi.org/10.1007/s40279-017-0796-x.
Abe T, Loenneke JP, Thiebaud RS. Ultrasound assessment of hamstring muscle size using posterior thigh muscle thickness. Clin Physiol Funct Imaging. 2016;36(3):206–10. https://doi.org/10.1111/cpf.12214.
Palmer TB, Akehi K, Thiele RM, Smith DB, Thompson BJ. Reliability of panoramic ultrasound imaging in simultaneously examining muscle size and quality of the hamstring muscles in young, healthy males and females. Ultrasound Med Biol. 2015;41(3):675–84. https://doi.org/10.1016/j.ultrasmedbio.2014.10.011.
Opar DA, Serpell BG. Is there a potential relationship between prior hamstring strain injury and increased risk for future anterior cruciate ligament injury? Arch Phys Med Rehabil. 2014;95(2):401–5.
Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016;50(24):1524–35. https://doi.org/10.1136/bjsports-2015-095362.
Timmins RG, Ruddy JD, Presland J, Maniar N, Shield AJ, Williams MD, et al. Architectural changes of the biceps femoris long head after concentric or eccentric training. Med Sci Sports Exerc. 2016;48(3):499–508. https://doi.org/10.1249/MSS.0000000000000795.
Lisee C, Lepley AS, Birchmeier T, O’Hagan K, Kuenze C. Quadriceps strength and volitional activation after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Sports Health. 2019;11(2):163–79. https://doi.org/10.1177/1941738118822739.
Hiemstra LA, Webber S, MacDonald PB, Kriellaars DJ. Contralateral limb strength deficits after anterior cruciate ligament reconstruction using a hamstring tendon graft. Clin Biomech (Bristol, Avon). 2007;22(5):543–50. https://doi.org/10.1016/j.clinbiomech.2007.01.009.
Kuenze C, Pietrosimone B, Lisee C, Rutherford M, Birchmeier T, Lepley A, et al. Demographic and surgical factors affect quadriceps strength after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019;27(3):921–30. https://doi.org/10.1007/s00167-018-5215-9.
Acknowledgements
The authors would like to acknowledge all participants that contributed to the original research reviewed in this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflicts of Interest
David Sherman, Justin Rush, Neal Glaviano and Grant Norte declare that they have no conflicts of interest relevant to the content of this review.
Standards of reporting
PRISMA
Ethics approval
This is a systematic review. The University of Toledo Institutional Review Board for Biomedical Research has confirmed that no ethical approval is required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Authors' contributions
All authors (DAS, JLR, NRG, and GEN) have contributed equally and demonstrated significant involvement in the planning and carrying out of this review and manuscript. Material preparation and data extraction were performed by David Sherman. Methodological quality review was performed by David Sherman and Justin Rush. Data analysis was performed by David Sherman. The first draft of the manuscript was written by David Sherman and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sherman, D.A., Rush, J.L., Glaviano, N.R. et al. Hamstrings Muscle Morphology After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. Sports Med 51, 1733–1750 (2021). https://doi.org/10.1007/s40279-021-01431-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-021-01431-y