
Abstract
Background
Lower body positive pressure treadmills (LBPPTs) aim to reduce musculoskeletal loading during running. As LBPPTs have become more commercially available, they have become integrated into athletic performance and clinical rehabilitation settings. Consequentially, published research examining the biomechanical and physiological responses to unweighted running has increased.
Objective
The purpose of this systematic review was to synthesize the literature in an attempt to provide researchers and clinicians with a comprehensive review of physiologic and biomechanical responses to LBPPT running.
Methods
Through a generic search of PubMed, CINAHL, MEDLINE, and SPORTDiscus using a comprehensive list of search terms related to LBPPT, unweighting, and body weight support during running, we identified all peer-reviewed publications that included LBPPT running. Two reviewers independently evaluated the quality of studies using a modified Downs and Black checklist for non-randomized studies.
Results
A total of 15 articles met the inclusion criteria for this review. Peak and active vertical ground-reaction forces were consistently reduced with unweighting, but regional loading within the foot was also altered towards a forefoot strike. LBPPTs also provide some horizontal assistance. Neuromuscular activation is generally reduced with LBPPTs, but the stabilizer muscle groups may respond differently than the propulsive muscle groups. Submaximal heart rate and volume oxygen consumption are reduced with unweighting, but physiologic response remains generally unchanged at maximal intensities.
Conclusions
The current literature suggests that LBPPTs are effective in allowing individuals to achieve a given metabolic stimulus with reduced musculoskeletal loading. However, LBPPTs not only reduce impact but also change neuromuscular activation and biomechanics in a complex manner. Thus, clinicians must account for the specific biomechanical and physiological alterations induced by LBPPTs when designing training programs and rehabilitation protocols.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Lower body positive pressure treadmills (LBPPTs), such as the AlterG, are effective for reducing impact during running. |
To achieve an aerobic intensity similar to that of normal treadmill running, faster speeds must be used when performing reduced-impact training on an LBPPT. |
The magnitude of biomechanical and physiological alterations appears to become more exaggerated at body weight settings <70 %; thus, individuals looking to train while receiving the benefits of unweighting while minimizing changes in running mechanics are encouraged to stay above this threshold. |
Although LBPPTs reduce impact during running, mechanics and muscle activation pattern changes are complex. |
1 Introduction
Running may be viewed as a healthy activity because it ultimately provides cardiometabolic benefits, but lower extremity musculoskeletal overuse injuries are very common in runners at various competitive levels [1, 2]. Epidemiological data also demonstrate that running is the most frequent cause of exercise- and sport-related injuries in the military [3]. Likewise, there is a high incidence of overuse injuries in recreational athletes, with around 10 % of novice runners reporting injury within a 6-week supervised training program [4]. These injuries ultimately lead to decreased training, with a median recovery time of 71 days reported in one study focused on novice runners [5]. Some specific injuries, such as stress fractures, are associated with particularly significant morbidity [6], and one study reported that nearly 5 % of injured novice runners underwent surgical treatment [5]. Further, numerous studies have demonstrated that the main risk factor for running injuries is a previous history of other running injuries [7–9]. This suggests that some running injuries may not necessarily be new injuries, but rather re-occurrences of previous injuries that were not fully healed.
Given the high prevalence of running injuries, there is great interest in researching interventions that may decrease the risk of injury and improve rehabilitation of existing injury. One common approach to achieve this has been through reducing musculoskeletal loading. Recent prospective evidence indicates that biomechanical variables related to impact are lower in runners who have not sustained musculoskeletal injuries, and this supports data from numerous retrospective studies that have demonstrated greater loading parameters in injured runners [10]. In the past decade, lower body positive pressure treadmills (LBPPTs) have emerged as a novel tool to reduce loading on the musculoskeletal system during walking and running. Originally, LBPPTs were one of many technological approaches used to simulate the microgravity environment experienced by astronauts [11]. However, unweighted running provides a novel form of exercise training for athletes and may also be highly beneficial in the rehabilitation of clinical populations. Case reports and pilot studies suggest LBPPTs can be utilized in return-to-play programs for individuals with various musculoskeletal injuries [12–14]. Additionally, LBPPTs are often used as training tools to allow for more training with decreased ground-reaction forces and for training at faster than normal paces [15].
Commercially available LBPPTs are now found in various healthcare and sports performance settings, which allows greater accessibility to patient and athletic populations. The devices have a simple interface, such that the user adjusts settings on the treadmill’s control panel to select a desired percentage of body weight at which to run. The LBPPT then applies an upward force on the user by increasing the air pressure inside the chamber [16]. In this way, LBPPTs can enable users to run with decreased downward forces acting on their musculoskeletal system. Although no clinical trials to determine the efficacy of LBPPTs in preventing or rehabilitating running injuries are currently available, a wealth of published research articles have reported the biomechanical and physiological effects of unweighted running on LBPPTs. However, direct comparisons between studies are complicated by differences in sample populations and running protocols. As research in this field has been rapidly developing, the literature in this realm has not yet been collectively evaluated to provide clinicians with a more comprehensive understanding of how the LBPPT influences running. Thus, we performed a systematic review to synthesize the literature in an attempt to provide researchers and clinicians with a comprehensive review of physiologic and biomechanical responses to LBPPT running. The synthesis of information provided through this systematic review can provide valuable insight for developing individualized training and rehabilitation programs utilizing an LBPPT, and for the design of clinical trials to determine the clinical efficacy of LBPPTs for preventing and rehabilitation of musculoskeletal injuries.
2 Methods
This systematic review was conducted and reported according to the protocol outline by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [17].
2.1 Identification and Selection of the Literature
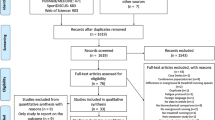
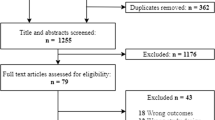
To comprehensively identify all peer-reviewed publications that utilized an LBPPT, we used a generic search strategy using PubMed, CINAHL, MEDLINE, and SPORTDiscus databases through 12 June 2015 (Fig. 1). References from each of the articles selected for inclusion were also searched to ensure that all possible articles regarding LBPPTs were accounted for.

PRISMA diagram of search strategy
2.2 Selection Criteria
An article was eligible for inclusion if it met all of the following criteria: (1) Outcome measures included at least one physiologic or biomechanical response to running on an LBPPT; (2) Article was original research (i.e., not a case study or case series); (3) Article was available as full text (i.e., not a poster or abstract); (4) Article was written in English. An article was excluded if the study population consisted of (1) clinical patients (e.g., individuals with neurologic disease, patients with osteoarthritis) or (2) any population that would have different physiological or biomechanical responses compared with a healthy, active population (e.g., individuals with advanced age, individuals with prosthetic limbs).
2.3 Quality Assessment
Two reviewers independently evaluated the quality of the included studies using a modified version of the Downs and Black checklist for non-randomized studies [18]. Specifically, 11 items of the original checklist were excluded as they were not applicable to the selected studies. Thus, articles had a maximum possible score of 16 points, which evaluated reporting (eight items), external validity (one item), internal validity bias (five items), and internal validity confounding (selection bias) (two items). Reviewers discussed any disagreements until they reached agreement.
2.4 Data Extraction
Two reviewers (KAF, JMS) extracted information and data concerning the study population and subject demographics, design, and results and major findings. The main data extracted included physiological parameters (heart rate [HR], ventilation, and volume of oxygen consumption [\( \dot{V} \)O2]) and biomechanical parameters (ground-reaction forces and impact-related variables, stride characteristics, and muscular activation). To minimize confusion for the reader, we have used consistent terminology throughout this paper and propose this nomenclature be used in future research regarding LBPPTs (Table 1).
2.5 Statistical Analysis of Volume of Oxygen Consumption (\( \dot{V} \)O2) Response
We determined that \( \dot{V} \)O2 was the only variable that was consistently measured and reported across multiple studies to allow for a pooled quantitative analysis. We developed a generalized estimating equation model with autoregressive covariance structure to determine the relationship between \( \dot{V} \)O2 (dependent variable), running speed, and unweighting (percent body weight) on an LBPPT. Running speed and unweighting were modeled as within-subject continuous variables (main effects), and study was used as a subject variable. We then used linear regression to compare the predicted values with observed values across studies.
3 Results
A total of 15 studies met inclusion for systematic review (Fig. 1). Table 2 shows the sample population, study design, and summary of general findings. See Table S1 in the electronic supplementary material (ESM) for the risk of bias/quality assessment scores for each study. Only nine of the 15 studies achieved a quality assessment score >50 % (≥9 of 16 criteria).
3.1 Biomechanical Variables
3.1.1 Kinetic Parameters
Six studies [15, 16, 19–22] met the inclusion criteria for this review and addressed kinetic parameters; each reported decreases in peak ground-reaction force with a lower body weight setting (BWSet). Additionally, two studies [15, 20] consistently found that the magnitude of active peak decreased below that of impact peak at lower BWSet, although one additional study demonstrated this through a figure [21], and another demonstrated that mean ground-reaction forces decreased [16]. Only two studies [15, 20] described horizontal forces, and both reported disproportionate decreases in propulsive impulse compared with braking impulse.
Two studies [15, 20] examined the effects of reloading at 100 % BWSet following previous unweighting. Sainton et al. [20] also reported that impact peak and loading rate decreased during reloading at 100 % BWSet following prior unweighted running. Grabowski and Kram [15] reported no significant changes in kinetics at 100 % BWSet following an unloading protocol. A summary of the kinetic parameter findings from each study is presented in Table 3.
3.1.2 Kinematic Parameters
Two studies [19, 20] reported kinematic data. Sainton et al. [20] found that vertical displacement during the brake phase was reduced significantly at 60 and 80 % BWSet. Cutuk et al. [19] found that unweighting on an LBPPT did not significantly change knee or ankle range of motion during running; however, they did observe some non-significant trends.
3.1.3 Stride Characteristics
Five studies [15, 16, 19, 20, 23] met the inclusion criteria for discussion of stride characteristics, but the findings were conflicting. Gojanovic et al. [23] reported stride rate increased in males and remained unchanged in females, whereas Grabowski and Kram [15], Raffalt et al. [16], and Sainton et al. [20] reported decreased stride frequency with unweighting. Grabowski and Kram [15] reported increased contact time, whereas Raffalt et al. [16] reported decreased contact time, and Sainton et al. [20] reported no changes in contact time. Raffalt et al. [16] and Sainton et al. [20] were in agreement that flight duration increased.
Two studies examined the effects of reloading at 100 % BWSet following previous unweighting. Sainton et al. [20] found flight time increased and step frequency decreased during reloading at BWSet 100 % following unweighted running. Grabowski and Kram [15] found contact time, but not stride frequency, at 100 % BWSet was increased following the entire unweighting protocol.
A summary of the stride characteristics findings from each study is presented in Table 4.
3.2 Neuromuscular Activation
Four studies [20, 24–26] met inclusion criteria that were used to evaluate muscle activation. All studies found that, as BWSet increased, muscle activity generally decreased across most muscles studied, with some key exceptions. Mercer et al. [26] found that the biceps femoris was not significantly altered by unweighting. Likewise, Hunter et al. [24] reported that unweighting did not have a significant impact on medial and lateral hamstring activity during stance, or hip adductor activity during swing. Sainton et al. [20] found that changes in muscle activity across various phases of the stride cycle differed by muscle (i.e., gastrocnemius activity was actually increased during the braking phase during unweighting) and were dependent upon the magnitude of unloading. Additionally, Sainton et al. [20] reported slight alterations occurred during reloading at 100 % BWSet following unweighting. A summary of the neuromuscular activation findings from each study is presented in Table 5.
3.3 Physiologic Variables
Eight studies [16, 20, 22, 23, 27–30] met the inclusion criteria for evaluation of metabolic parameters. All studies that examined \( \dot{V} \)O2 and HR during submaximal running found these parameters to decrease with unweighting. Raffalt et al. [16] reported decreased minute ventilation during unweighted submaximal running, despite unchanged respiratory rate. McNeill et al. [29] also reported a decreased respiratory exchange ratio. McNeill et al. [29] and Ruskstuhl et al. [30] both reported decreased rating of perceived exertion (RPE) with unweighted submaximal running, whereas Sainton et al. [20] reported no changes in RPE. Rather than examining changes in RPE across unweighting levels, Hoffman and Donaghe [22] showed that HR and RPE remained the same for a given \( \dot{V} \)O2 across various BWSet.
Two studies reported that \( \dot{V} \)O2max can be achieved using an LBPPT provided a sufficient speed is used to compensate for unweighting. Raffalt et al. [16] reported that all measured cardiorespiratory parameters remained unchanged at maximal aerobic intensity across BWSet, whereas Gojanovic et al. [23] reported decreased maximal HR and increased RPE at certain BWSet in men and women, as well as decreased lactate at 85 % BWSet in men.
Two studies [27, 28] provided sufficient \( \dot{V} \)O2 data in tabular format, and we obtained tabular data from one published study directly from the author [22]. The generalized estimating equation model was statistically significant for both speed and BWSet (p < 0.001 for both). The equation developed was as in Eq. 1:
When observed values were compared with predicted values, the coefficient of determination was r 2 = 0.880, indicating the derived equation was generally a very good fit.
Table 6 presents a summary of physiological findings from each study.
3.4 Running Performance
One study [31] was included in the discussion of improving running performance. Gojanovic et al. [31] found that high-intensity interval training on an LBPPT (90 % BWSet) can lead to improvements in \( \dot{V} \)O2max, velocity at \( \dot{V} \)O2max, and time to exhaustion at \( \dot{V} \)O2max; however, over-ground 2-mile time trial time did not improve compared with similar training on a standard treadmill.
4 Discussion
The available research collectively demonstrates that running on an LBPPT is effective in allowing individuals to achieve a given metabolic stimulus with reduced musculoskeletal loading, though with apparent alterations in neuromuscular activation patterns, kinetics, and stride parameters.
4.1 Kinetic Responses
A primary goal of using an LBPPT is to reduce forces imposed upon the musculoskeletal system by providing upward vertical force to counter gravity. The available research indicates that an LBPPT does indeed achieve the desired effect of musculoskeletal unloading, as evidenced by decreased ground-reaction forces and in-shoe loading, and that sufficient unweighting (<60 to 80 %) reduces the active peak below that of the impact peak. Future research examining kinetic responses to using an LBPPT must consider peak ground-reaction force, must differentiate between impact and active peaks, and should also consider impulse. Additionally, as unweighting is increased, a shift in in-shoe regional loading towards the forefoot occurs that may result in altered running patterns (most prominent <80 % BWSet) [21]. Thus, future studies exploring biomechanical responses to LBPPT running should account for foot strike type.
While positive pressure is meant to provide vertical body weight support, Grabowski and Kram [15] and Sainton et al. [20] both reported braking impulses exceeded propulsive impulses, and thus horizontal stabilization also influences biomechanical and physiological responses to LBPPT running. Previous research on normal treadmills demonstrated that a small amount of horizontal assistance decreases metabolic demands and increases peak impact force and vertical loading rate without influencing active peak force [32, 33]. While these findings suggest that the LBPPT apparatus provides some horizontal stability in the anterior–posterior direction, it is possible that it also provides mediolateral stability. The added mediolateral stability may contribute to the decreased metabolic cost of running. While this seems likely, no published research has yet explored this possibility.
It is important for LBPPT users and clinicians to be aware that biomechanical alterations to unweighting do not necessarily occur proportionately to BWSet. For instance, Smoliga et al. [21] reported that BWSet on the LBPPT does not represent the actual percentage of maximum ground-reaction force but rather the percentage of maximum ground-reaction force beyond the user’s standing body weight. For instance, while running at preferred training speed at the 100 % BWSet, the user lands at approximately 2.3 times his/her body weight, which is 1.3 body weights more than standing at rest. At 20 % BWSet, users landed at 1.2 body weights, which is 0.2 body weights, or 20 % more force, than standing at rest. However, this is approximately 50 % of the actual maximal ground-reaction force compared with 100 % BWSet (1.20 ÷ 2.32 = 51.7 %). In other words, 20 % BWSet does not equate to 20 % of maximal ground-reaction force, and thus biomechanical responses do not scale directly proportionately to BWSet. On this note, it is important to recognize that unweighting does not simply reduce the magnitude of a given biomechanical parameter but rather causes a complex series of kinetic changes. For instance, three studies [15, 20, 21] demonstrated that the active peak is reduced disproportionately greater than the impact peak, and one study [21] demonstrated that the relative load within different regions of the foot is also altered.
4.2 Neuromuscular Responses
The available LBPPT literature indicates that muscles respond differently to different magnitudes of unweighting, and there is variability in muscle activation response to unweighting between muscles, which may depend on the function of the specific muscles during running. The data from Sainton et al. [20] indicate that activation is not significantly decreased in certain muscles until considerable unweighting occurs (e.g., significant differences present at 60 % BWSet, but not 80 % BWSet). Interestingly, other muscles actually experience significant changes with some unweighting (i.e., 80 % BWSet) but not with further unweighting (i.e., 60 % BWSet). While some muscles consistently experience decreased activation with greater unweighting (e.g., tibialis anterior, rectus femoris), Hunter et al. [24] and Mercer et al. [26] both reported that hamstring activity did not continue to decline with reduced BWSet. Hunter et al. [24] also reported that hip adductor muscles remained relatively unchanged with unweighting, which is likely related to unweighting having less of an influence on the need for stabilization within the frontal plane compared with propulsion.
4.3 Kinematic Responses
Kinematic adjustments to LBPPT running are not as well defined and, in the case of stride parameters, are inconsistent. Use of an LBPPT requires the user to wear tight neoprene shorts that are then attached to the treadmill. This may directly and indirectly change the range of motion of certain joints. For instance, the waist seal of the LBPPT may limit upward displacement during ambulation, which could secondarily decrease knee range of motion [19]. Further, conflicting findings in kinetic and kinematic responses between studies strongly indicate that the nature of biomechanical responses may depend on the magnitude of unloading (e.g., 40 % BWSet may produce different results than 80 % BWSet), running speed, fitness levels, treadmill running experience, and perhaps previous LBPPT experience. This is likely the case for stride parameters, where conflicting findings may be a result of vastly different speeds between protocols. Indeed, there is evidence of an accommodation effect, such that multiple trials of unweighted running may be necessary to achieve stable metabolic measurements [34].
4.4 Cardiometabolic Responses
These biomechanical changes seen with the LBPPT all contribute to less metabolic cost. Specifically, if the body’s mechanical power output requirement is lowered, neuromuscular activation is reduced, and therefore there is a decreased need for adenosine triphosphate (ATP) production. Thus, it is not surprising that, as BWSet is reduced within a given speed, \( \dot{V} \)O2 demand is decreased, and thus, HR and ventilation are also reduced. Kline et al. [27] reported that the proportion of metabolic demand to BWSet was found to be near equivalent for 70–90 % BWSet; however, at the extreme ends, the proportion of metabolic demand differed significantly from the proportion of BWSet. Thus, individuals training on an LBPPT with the goal of achieving a specific metabolic stimulus while unweighted may need to increase the treadmill speed or incline to achieve the desired overall metabolic stimulus, and it is even possible to achieve \( \dot{V} \)O2max at reduced BWSet. According to Hoffman and Donaghe [22], the relationship between HR and \( \dot{V} \)O2 remained unchanged with alterations in BWSet, which suggests that HR monitoring may be effective for monitoring running intensity on an LBPPT. This is also consistent with the recommendation by McNeill et al. [29] to base exercise prescription on HR due to individual variability. However, given that unweighting elicits different responses between muscles (i.e., neuromuscular activation in the rectus femoris to a greater magnitude than the hamstring group), unweighting may produce a different profile of local muscular metabolic demands, which ultimately result in a similar whole-body \( \dot{V} \)O2. This further echoes the notion that individuals participating in unweighted training on an LBPPT should be cognizant of the alterations in muscular stimulus compared with normal unweighted running.
It is important to note that the cardiometabolic demands of running at 100 % BWSet on an LBPPT are lower than running on a regular treadmill. McNeill et al. [34] attributed the decreased metabolic demand at 100 % BWSet to the inflation of the chamber, which likely did have physiological effects by decreasing vertical ground-reaction force ~7 %. However, it is also possible the added two-dimensional horizontal support of the LBPPT apparatus may also contribute to decreased metabolic demand at 100 % BWSet. Although the magnitude of the additional vertical and horizontal support at 100 % BWSet may seem minor, it can have major physiological implications. For instance, Raffalt et al. [16] found that time to exhaustion during a \( \dot{V} \)O2max test was 34.5 % longer when performed on an LBPPT at 100 % BWSet than on a standard treadmill, which suggests the supporting apparatus itself influenced running performance.
4.5 Training Implications
Given that LBPPTs are intended for rehabilitating injured individuals, preventing injuries, and enhancing performance, it is imperative that training benefits achieved on LBPPTs translate to over-ground running. Two studies reported some acute adjustments that occurred during reloading (i.e., running at 100 % BWSet following unweighting). Sainton et al. [20] found reloading altered stride characteristics following 60 % BWSet, altered stride kinetics following 80 % BWSet, and increased neuromuscular activity and physiologic intensity following both unweighting conditions. Conversely, Grabowski and Kram [15] found kinetics remained unchanged but contact time increased following an unweighting protocol. Conflicting findings may reflect different research protocols but nonetheless suggest that prior unweighting does acutely influence normal running mechanics, though the duration of such alterations remains unknown. Likewise, these studies only utilized a few minutes of LBPPT training, and the results may not be representative of the alterations that would occur following a typical training session. Thus, research is insufficient to determine whether neuromuscular and biomechanical alterations that occur on LBPPTs influence over-ground running and the consequences of long-term LBPPT training on over-ground running mechanics.
Gojanovic et al. [31] found 4 weeks of high-intensity interval training on an LBPPT (90 % BWSet) improved multiple physiologic performance parameters, including \( \dot{V} \)O2max and velocity at \( \dot{V} \)O2max, but resulted in similar over-ground 2-mile time trial performance compared with training on a normal treadmill. This suggests that even if LBPPTs do modify running mechanics as described above, they do not do so in a way that negatively or positively influences running performance. It remains unknown whether LBPPT training can simply replicate the benefits of over-ground running, albeit with a lower musculoskeletal impact, or whether strategically designed unweighted running protocols can actually enhance performance beyond that attainable through over-ground running alone. Although one study alone is not sufficient to draw conclusions regarding longer-term performance adaptations to unweighting, the results do suggest that LBPPT training does translate to over-ground running performance (i.e., training on an LBPPT can be beneficial for improving track or road race performance). Thus, it may be possible for injured or injury-prone athletes to realize improvements through training on an LBPPT; however, the faster speeds (or inclines) necessary to achieve sufficient physiologic stimulus during unweighting may ultimately negate some of the desired musculoskeletal unloading. In addition, there may be potential for increased injury risk via the faster speeds altering running mechanics or requiring different neuromuscular activation patterns than would normally be used. Thus, further research should examine long-term effects of LBPPT training on both injury risk and performance in both healthy and injured athletes. The effect of incline on LBPPT running should also be explored.
Through evaluating the available data, we determined that three studies [22, 27, 28] could be used to develop an equation to predict \( \dot{V} \)O2 based on running speed and BWSet (Eq. 1). Figure 2 shows a graph of the equation at BWSet 100, 75, and 50 % with corresponding speeds and \( \dot{V} \)O2. As shown by Fig. 2, to achieve a \( \dot{V} \)O2 of approximately 30 ml O2/kg/min, a speed of 2.5 m/s would be required at 100 % BWSet, 3.8 m/s would be needed at 75 % BWSet, and 5 m/s would be needed at 50 % BWSet. This equation also shows that within a given running speed, each 10 % decrease in BWSet is associated with an approximately 3.4 ml O2/kg/min reduction in \( \dot{V} \)O2. However, this model only represents three datasets, with treadmill speeds ranging from 1.79 to 5.36 m/s and LBPPT settings of 50–100 % BWSet and should not be extrapolated beyond these limits. Nonetheless, the strong coefficient of determination indicates that the \( \dot{V} \)O2 response to various BWSet and running speeds was generally consistent between these three studies, which suggests that physiological response may also be consistent across individuals.

Predicted relationship between running speed and \( \dot{V} \)O2 at BWSet 50, 75, and 100 % based on pooled data from three studies. This figure may be used to visualize what running speed would need to be prescribed at a given LBPPT BWSet to elicit an equivalent \( \dot{V} \)O2 at another BWSet. For example, to achieve a \( \dot{V} \)O2 of approximately 30 ml/kg/min, a speed of 2.5 m/s could be used at 100 % body weight (30.1 ml/kg/min), 3.8 m/s could be used at 75 % body weight (30.5 ml/kg/min), and 5 m/s could be used at 50 % body weight (30.1 ml/kg/min). BW Set body weight setting, LBPPT lower body positive pressure treadmill, \( \dot{V} \) O 2 volume of oxygen consumption
4.6 Clinical Implications
The wealth of research on biomechanical and physiological responses to LBPPT provides some insight for clinical usage. As noted in Sect. 4.1, the BWSet does not accurately reflect the absolute magnitude of peak ground-reaction force production, and clinicians must be aware that running at 50 % BWSet is not actually equivalent to half of the musculoskeletal impact of normal running. Likewise, LBPPTs alter regional in-shoe loading, such that reductions in ground-reaction force do not necessarily result in uniformly distributed musculoskeletal loads [21]. As such, caution may be warranted in excessive use of LBPPTs for individuals with foot pathology (e.g., metatarsal stress fractures, plantar fasciitis), until more research in this area is available. The available neuromuscular data [20, 24–26] have important implications for clinicians utilizing LBPPTs for rehabilitating injured athletes. The findings by Sainton et al. [20] emphasize the notion that LBPPT unweighting has a complex effect on neuromuscular activation, and reducing BWSet does not simply reduce muscle activity in a linear manner. Based on neuromuscular activation patterns in healthy athletes, individuals with calf or Achilles tendon injuries may benefit from unweighting, whereas individuals with groin or hamstring injuries may not receive any benefit from LBPPT running. While this concept seems sound, future clinical trials will be needed to confirm this. It is especially important for clinicians to appreciate this concept, as the reduced perception of overall exertion [29, 30] and impact [15, 16, 19–22] provided by unweighting on LBPPTs may provide athletes with a false sense that these specific muscle groups are also under less stress. The available research does indicate that LBPPTs produce favorable responses for training [31], and case studies [13, 14] and pilot studies [12] support its benefit in rehabilitation, but long-term studies in both realms are necessary for developing strong evidence-based recommendations for clinical use.
4.7 Terminology
The terminology used across the LBPPT literature varies significantly, and it is often difficult to distinguish whether the methods refer to the amount of body weight support provided (e.g., 20 % upward vertical force), the reduction in body weight relative to normal gravity (e.g., 80 % of standard conditions), the targeted body weight setting on the LBPPT, or the actual measured body weight on the treadmill. For example, some authors refer to no body weight support from the LBPPT as 0 %, while others refer to this as 100 % because the LBPPT setting would be set to 100. Thus, the terminology used can be very unclear and even misinterpreted. While both “unweighting” and “body weight support” may be applicable to LBPPTs, we believe the term “unweighting” is preferable in the context of LBPPTs. Harness systems and LBPPTs can be considered a more general type of “body weight support” but are unlike other ambulation aids, such as walkers and canes, which also redistribute forces to other areas of the body. However, the body weight support offered by harness systems and LBPPTs is external, such that users do not need to contract musculature elsewhere to support their lower body (i.e., activating the torso and arm musculature to support the body when walking with a cane). As such, we use the terminology in Table 1, and propose that this nomenclature be used throughout the LBPPT literature to minimize confusion.
4.8 Limitations
Synthesis of research regarding LBPPTs reveals considerable insight into the integration of biomechanical and physiological responses to unweighting; however, there are some limitations to the current body of research. All but two of the studies that met inclusion criteria for this systematic review included a limited number of sessions using an LBPPT, and therefore did not explore chronic adaptations to LBPPT running. Most of the studies used men only, yet Gojanovic et al. [23] demonstrated that men and women do respond differently to using an LBPPT in some parameters. Thus, further research examining responses to LBPPT training in females may be necessary, as sex differences in anthropometric factors may be influential. Additionally, the diversity of LBPPT protocols used, combined with the different types of comparisons performed within a study, makes it difficult to compare results between studies. For instance, Sainton et al. [20] and Grabowski and Kram [15] were in agreement about active peak being the most responsive kinetic parameter in response unweighting. Changes in loading rate seemed to be more responsive to unweighting in the study by Sainton et al. [20] than in the work by Grabowski and Kram [15]. However, Sainton et al. [20] measured changes between 60 and 80 % BWSet, and between 80 and 100 % BWSet, whereas, Grabowski and Kram [15] compared changes between 50 and 75 %. Additionally, the kinetic studies only examined ground-reaction forces and do not provide any insight into how unweighting influences joint moments or joint compression forces. Finally, the majority of the studies included in this systematic review used products made by Alter-G; however, slight updates have been made in the design of their LBPPT devices. Although the methodology from early and recent studies suggests that the same general principles all apply, it is possible that some changes in biomechanical or physiological responses could arise from differences in design.
5 Conclusions
The commercial availability of LBPPTs has increased accessibility to unweighted running; thus, research on this topic has rapidly expanded. This is the first systematic review on this topic, and the results reveal that the collective body of literature is sufficient to describe general biomechanical and physiological responses to unweighted running. Running on an LBPPT is associated with a variety of kinetic adjustments, most notably disproportionate reductions in the active vertical ground-reaction force peak relative to the impact peak and propulsive impulses relative to braking impulse, as well as a shift in in-shoe regional loading towards the forefoot. The synthesis of the literature provides evidence that lower BWSets are associated with decreased musculoskeletal and metabolic demands, and that faster treadmill speeds can be used to raise the physiologic stimulus without fully countering the reduced musculoskeletal loading provided by the LBPPT. Although external mechanical support from the LBPPT apparatus ultimately reduces metabolic stimulus, the loads on the hamstring and hip adductor muscle groups are not reduced to the same magnitude as that of other leg muscles. As such, clinicians must be aware that LBPPT does not simply ‘reduce impact’ but also changes biomechanics and musculoskeletal loading in a rather complex manner, and that caution may be warranted when using the LBPPT for treating certain types of musculoskeletal injuries. The magnitude of biomechanical and physiological alterations appears to become more exaggerated at BWSet <70 %, thus, individuals looking to train while receiving the benefits of unweighting while minimizing changes in running mechanics are encouraged to stay above this threshold. There is some evidence that unweighted training on an LBPPT can effectively translate into improved performance during over-ground running, though more research in this area is needed. Further research is needed regarding the efficacy of LBPPT for individuals with specific musculoskeletal injuries so that optimized rehabilitation protocols can be developed.
References
Pierpoint LA, Williams CM, Fields SK, et al. Epidemiology of injuries in United States High School Track and Field: 2008–2009 through 2013–2014. Am J Sports Med. 2016;44(6):1463–8.
Kerr ZY, Kroshus E, Grant J, et al. Epidemiology of National Collegiate Athletic Association men’s and women’s cross-country injuries, 2009–2010 through 2013–2014. J Athl Train. 2016;51(1):57–64.
Hauret KG, Bedno S, Loringer K, et al. Epidemiology of exercise- and sports-related injuries in a population of young, physically active adults: a survey of military service members. Am J Sports Med. 2015;43(11):2645–53.
Kluitenberg B, van Middelkoop M, Smits DW, et al. The NLstart2run study: Incidence and risk factors of running-related injuries in novice runners. Scand J Med Sci Sports. 2015;25(5):e515–23.
Nielsen RO, Ronnow L, Rasmussen S, et al. A prospective study on time to recovery in 254 injured novice runners. PLoS One. 2014;9(6):e99877.
Changstrom BG, Brou L, Khodaee M, et al. Epidemiology of stress fracture injuries among US high school athletes, 2005–2006 through 2012–2013. Am J Sports Med. 2015;43(1):26–33.
Wright AA, Taylor JB, Ford KR, et al. Risk factors associated with lower extremity stress fractures in runners: a systematic review with meta-analysis. Br J Sports Med. 2015;49(23):1517–23.
van der Worp MP, ten Haaf DS, van Cingel R, et al. Injuries in runners; a systematic review on risk factors and sex differences. PLoS One. 2015;10(2):e0114937.
Saragiotto BT, Yamato TP, Hespanhol Junior LC, et al. What are the main risk factors for running-related injuries? Sports Med. 2014;44(8):1153–63.
Davis IS, Bowser BJ, Mullineaux DR. Greater vertical impact loading in female runners with medically diagnosed injuries: a prospective investigation. Br J Sports Med. 2015;. doi:10.1136/bjsports-2015-094579.
Schlabs T, Rosales-Velderrain A, Ruckstuhl H, et al. Comparison of cardiovascular and biomechanical parameters of supine lower body negative pressure and upright lower body positive pressure to simulate activity in 1/6 G and 3/8 G. J Appl Physiol (1985). 2013;115(2):275–84.
Saxena A, Granot A. Use of an anti-gravity treadmill in the rehabilitation of the operated achilles tendon: a pilot study. J Foot Ankle Surg. 2011;50(5):558–61.
Tenforde AS, Watanabe LM, Moreno TJ, et al. Use of an antigravity treadmill for rehabilitation of a pelvic stress injury. PM R. 2012;4(8):629–31.
Moore MN, Vandenakker-Albanese C, Hoffman MD. Use of partial body-weight support for aggressive return to running after lumbar disk herniation: a case report. Arch Phys Med Rehabil. 2010;91(5):803–5.
Grabowski AM, Kram R. Effects of velocity and weight support on ground reaction forces and metabolic power during running. J Appl Biomech. 2008;24(3):288–97.
Raffalt PC, Hovgaard-Hansen L, Jensen BR. Running on a lower-body positive pressure treadmill: VO2max, respiratory response, and vertical ground reaction force. Res Q Exerc Sport. 2013;84(2):213–22.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2010;8(5):336–41.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Cutuk A, Groppo ER, Quigley EJ, et al. Ambulation in simulated fractional gravity using lower body positive pressure: cardiovascular safety and gait analyses. J Appl Physiol. 2006;101(3):771–7.
Sainton P, Nicol C, Cabri J, et al. Influence of short-term unweighing and reloading on running kinetics and muscle activity. Eur J Appl Physiol. 2015;115(5):1135–45.
Smoliga JM, Wirfel LA, Paul D, et al. Effects of unweighting and speed on in-shoe regional loading during running on a lower body positive pressure treadmill. J Appl Biomech. 2015;48(10):1950–6.
Hoffman MD, Donaghe HE. Physiological responses to body weight: supported treadmill exercise in healthy adults. Arch Phys Med Rehabil. 2011;92(6):960–6.
Gojanovic B, Cutti P, Shultz R, et al. Maximal physiological parameters during partial body-weight support treadmill testing. Med Sci Sports Exerc. 2012;44(10):1935–41.
Hunter I, Seeley MK, Hopkins JT, et al. EMG activity during positive-pressure treadmill running. J Electromyogr Kinesiol. 2014;24(3):348–52.
Liebenberg J, Scharf J, Forrest D, et al. Determination of muscle activity during running at reduced body weight. J Sports Sci. 2011;29(2):207–14.
Mercer JA, Applequist BC, Masumoto K. Muscle activity while running at 20 %–50 % of normal body weight. Res Sports Med. 2013;21(3):217–28.
Kline JR, Raab S, Coast JR, et al. A conversion table for running on lower body positive pressure (LBPP) treadmills. J Strength Cond Res. 2015;29(3):854–62.
McNeill DK, de Heer HD, Williams CP, et al. Metabolic accommodation to running on a body weight-supported treadmill. Eur J Appl Physiol. 2015;115(5):905–10.
McNeill DK, Kline JR, de Heer HD, et al. Oxygen consumption of elite distance runners on an anti-gravity treadmill(R). J Sports Sci Med. 2015;14(2):333–9.
Ruckstuhl H, Kho J, Weed M, et al. Comparing two devices of suspended treadmill walking by varying body unloading and Froude number. Gait Posture. 2009;30(4):446–51.
Gojanovic B, Shultz R, Feihl F, et al. Overspeed HIIT in lower body positive pressure treadmill improves running performance. Med Sci Sports Exerc. 2015;47(12):2571–8.
Chang YH, Hamerski CM, Kram R. Applied horizontal force increases impact loading in reduced-gravity running. J Biomech. 2001;34(5):679–85.
Chang YH, Kram R. Metabolic cost of generating horizontal forces during human running. J Appl Physiol (1985). 1999;86(5):1657–62.
McNeill DK, de Heer HD, Bounds RG, et al. Accuracy of unloading with the Anti-Gravity (R) treadmill. J Strength Cond Res. 2015;29(3):863–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflict of interest
Kathryn Farina, Alexis Wright, Kevin Ford, Leah Anne Wirfel, and James Smoliga have no conflicts of interest relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Farina, K.A., Wright, A.A., Ford, K.R. et al. Physiological and Biomechanical Responses to Running on Lower Body Positive Pressure Treadmills in Healthy Populations. Sports Med 47, 261–275 (2017). https://doi.org/10.1007/s40279-016-0581-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-016-0581-2