
Abstract
The National Institute for Health and Care Excellence (NICE) invited the manufacturer of daclatasvir (Bristol-Myers Squibb) to submit clinical and cost-effectiveness evidence for daclatasvir in combination with other medicinal products within its licensed indication for the treatment of chronic hepatitis C, as part of the Institute’s single technology appraisal process. The Centre for Reviews and Dissemination and Centre for Health Economics at the University of York were commissioned to act as the independent Evidence Review Group (ERG). This article presents the ERG’s critical review of the evidence presented in the company submission in the context of a description of the company submission, and the resulting NICE guidance. The main clinical effectiveness data for daclatasvir in combination with sofosbuvir (daclatasvir + sofosbuvir) were derived from two uncontrolled open-label trials. Among patients with genotype 1 infection, 98–100 % of patients had a sustained virologic response at week 12 (SVR12), overall. Among genotype 3 patients, between 85 and 100 % had SVR12 across patient populations and regimens. The main evidence for daclatasvir + pegylated interferon-α and ribavirin (PR) came from one randomised controlled trial comparing daclatasvir + PR with PR in patients with genotype 4. This found an SVR12 rate of 82 % in previously untreated patients. Serious adverse event rates associated with daclatasvir were low. The lack of comparative trial evidence for daclatasvir + sofosbuvir and many of the comparators defined in the NICE scope meant that established methods for comparing interventions either directly via head-to-head trial comparisons or via adjusted indirect comparisons were not feasible. Comparisons of SVR rates were therefore largely based on unadjusted estimates drawn from individual trial arms and subgroups of individual trial arms. The ERG concluded that, despite limited evidence, daclatasvir in combination with other treatments appeared to be associated with a high SVR rate. Daclatasvir + sofosbuvir was unlikely to be inferior to comparator treatments in genotype 1 patients; but, due to limited evidence, the relative efficacy of daclatasvir and other treatments in genotype 3 and 4 patients or patients with compensated cirrhosis was uncertain. The economic evaluation compared daclatasvir + sofosbuvir and daclatasvir + PR with a wide range of NICE-approved treatments for hepatitis C. The company submission focused on a series of subgroups defined by disease severity (METAVIR fibrosis stage F3, compensated cirrhosis), genotype and treatment history. In the cost-effectiveness analysis, daclatasvir-containing regimens were cost effective at a £20,000–£30,000 per QALY threshold in the following F3 populations: genotype 1 treatment naïve (Incremental cost-effectiveness ratio [ICER] = £19,739/QALY) and treatment experienced (£15,687/QALY) and genotypes 1, 3 and 4 interferon ineligible or intolerant (£5906–£9607/QALY depending on subgroup). In patients with cirrhosis, daclatasvir-containing regimens were not cost effective. The ERG found the company’s economic analyses to be highly uncertain and in places biased. However, the ERG found that daclatasvir-containing regimens were cost effective in certain populations with significant fibrosis, and following new analyses by the company after a price reduction, in certain populations with cirrhosis, including patients who were not eligible for or who were intolerant to interferon therapy. The NICE Appraisal Committee’s preliminary recommendation was that daclatasvir + sofosbuvir should be available as an option in genotype 1 and 4 patients with significant fibrosis but without cirrhosis, who had either been treated previously or were ineligible or intolerant to interferon. In response to the preliminary recommendation, the manufacturer submitted additional information including comparator SVR rates and a revised confidential price. Following this, the Committee expanded its original recommendation in its Final Appraisal Determination. The recommendation was expanded to include daclatasvir + sofosbuvir as an option for patients with significant fibrosis but without cirrhosis (in previously untreated patients with genotype 1, and genotype 3 patients ineligible or intolerant to interferon) and genotype 1, 3 and 4 cirrhotic patients who were ineligible or intolerant to interferon. Daclatasvir + PR was also recommended as an option for genotype 4 patients who had significant fibrosis or compensated cirrhosis.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Daclatasvir in combination with other treatments for the treatment of chronic hepatitis C virus (HCV) is effective for treating adults with chronic HCV with genotypes 1, 3 and 4. |
Daclatasvir + sofosbuvir is unlikely to be inferior to other licensed treatments for patients with genotype 1. The relative efficacy of daclatasvir with other treatments in genotype 3 and 4 patients or in patients with advanced liver disease is uncertain due to limited evidence. |
There were few serious adverse events associated with daclatasvir. |
The ERG found the company’s economic analyses to be highly uncertain and in places biased. |
The ERG found that daclatasvir-containing regimens were cost effective in certain populations with significant fibrosis, and after a price reduction, in certain populations with cirrhosis, including patients who were not eligible or who were intolerant to interferon therapy. |
The NICE Appraisal Committee concluded that daclatasvir in combination with other treatments should be recommended as an option for treating chronic HCV in adults in specific populations. |
1 Introduction
The National Institute for Health and Care Excellence (NICE) is an independent organisation responsible for providing national guidance to the National Health Service (NHS) in England and Wales on the use of selected new health technologies. Single technology appraisals evaluate a single product, device or other technology that has a single indication; for example, a new pharmaceutical product or new licensed indication. The manufacturer (or sponsor of the technology) submits the principal evidence supporting the clinical and cost effectiveness of the product, and an external independent academic organisation, the Evidence Review Group (ERG), is commissioned to produce a review and critique of the evidence submitted. Clinical specialists, NHS commissioning experts and patient experts also provide evidence for consideration by the NICE Appraisal Committee in formulating their guidance. Once published, NICE technology guidance provides a legal obligation for NHS providers to reimburse technologies that have been approved [1].
NICE invited the manufacturer of daclatasvir (Bristol-Myers Squibb) to submit clinical and cost-effectiveness evidence for daclatasvir in combination with other medicinal products within its licensed indication for the treatment of chronic hepatitis C, as part of the Institute’s single technology appraisal process. The Centre for Reviews and Dissemination and Centre for Health Economics at the University of York were commissioned to act as the independent ERG.
This article presents a summary of the ERG’s independent critique of the company’s submission to NICE and the subsequent development of NICE guidance for the use of daclatasvir for the treatment of chronic hepatitis C virus (HCV). Full details of the appraisal and the relevant documents can be found on the NICE website [2].
2 The Decision Problem
Hepatitis C is an infectious liver disease caused by HCV. Persistence of HCV infection for at least 6 months is referred to as chronic HCV [3]. Approximately 214,000 individuals have chronic HCV in the UK [4]. The rate of disease progression in those with chronic HCV is variable and occurs over several decades. Chronic HCV infection can cause gradual scarring (fibrosis) of the liver tissue, and leads to cirrhosis and liver failure in about 10–20 % of cases within a mean time of 20 years, and hepatocellular carcinoma in about 1–5 % of chronically infected individuals. About 5 % of infected people die from the consequences of long-term infection [3, 5–7].
There is no published NICE guideline for the treatment of chronic HCV, although a guideline is currently being developed [8] and NICE has conducted several technology appraisals (TAs) and issued guidance. At the start of the daclatasvir appraisal, the treatment options for chronic HCV recommended by NICE were telaprevir + pegylated interferon-α and ribavirin (PR) or boceprevir + PR for patients with HCV genotype 1, and PR alone for HCV genotypes 1–6 [9–11]. Four additional treatments were approved by NICE for adults with chronic HCV in 2015, and final appraisal determination information of these treatments was published after the daclatasvir manufacturer submission. Simeprevir + PR is now recommended by NICE within its marketing authorisation as a treatment option for genotype 1 and 4 patients [12]. Sofosbuvir is also recommended as an option in combination with ribavirin ± peginterferon-α for certain subpopulations of patients with genotypes 1–6 [13]. Ledipasvir + sofosbuvir is recommended as an option for previously untreated adults with genotype 1 with or without cirrhosis or genotype 4 with cirrhosis, and for genotype 1 and 4 patients who had insufficient response to previous HCV treatment [14]. Ombitasvir + paritaprevir + ritonavir ± dasabuvir and ± ribavirin is recommended as an option for genotype 1 and 4 patients [15].
Daclatasvir (brand name Daklinza®) is an inhibitor of non-structural protein 5A which is an essential component in HCV replication. It is licensed for use in combination with other medicinal products for the treatment of chronic HCV infection in adults. The product licence recommends daclatasvir in combination with other treatments including sofosbuvir, ribavirin and peginterferon-α in patients with genotypes 1, 3 and 4 [16]. The marketing authorisation was updated during the course of the appraisal. This resulted in the treatment duration shortening from 24 to 12 weeks for non-cirrhotic treatment-experienced genotype 3 patients.
The NICE appraisal scope requested clinical and cost-effectiveness evidence for daclatasvir in combination with other medicinal products within its licensed indication for treating chronic HCV, compared with PR, telaprevir + PR, boceprevir + PR, sofosbuvir + ribavirin or PR, simeprevir + PR, simeprevir + sofosbuvir ± ribavirin, and best supportive care (watchful waiting). The scope specified a number of subgroups for consideration: HCV genotype, co-infection with HIV, presence of cirrhosis, liver transplantation, response to prior treatment and eligibility for interferon.
The manufacturer considered patients with HCV genotypes 1, 3 and 4 who were treatment naïve, treatment experienced or interferon ineligible or intolerant, had liver fibrosis at METAVIR stages F0–F4, F0–F2, F3–F4 (non-cirrhotic) and those with compensated cirrhosis. The manufacturer submission focussed primarily on patients with METAVIR F3–F4 (non-cirrhotic) and on the patients with compensated cirrhosis.
3 The Independent Evidence Review Group (ERG) Review
The company provided a submission to NICE on the use of daclatasvir for the treatment of chronic HCV. The ERG critically reviewed the evidence presented in the company’s submission by assessing (1) whether the submission conformed to NICE methodological guidelines; (2) whether the manufacturer’s interpretation and analysis of the evidence were appropriate; and (3) the presence of other evidence or alternative interpretations of the evidence. In addition, the ERG identified areas requiring clarification, for which the manufacturer provided additional evidence [2].
3.1 Clinical Evidence
3.1.1 Summary of the Clinical Evidence
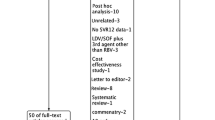
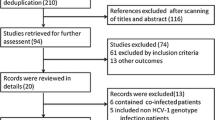
The company’s submission on clinical effectiveness contained four reviews: a review to identify studies of daclatasvir and three other reviews focused on estimating the comparative effectiveness of daclatasvir-based treatment and a range of alternative treatments (a benchmarking review, a matching adjusted indirect comparison and an unadjusted indirect comparison). Standard methods of assessing comparative effectiveness such as meta-analysis, indirect comparison and network meta-analysis were not feasible due to a lack of randomised controlled trial evidence comparing daclatasvir + sofosbuvir with other interventions, and a lack of randomised controlled trial evidence for many of the comparator treatments.
Review of studies of daclatasvir The manufacturer’s systematic review of daclatasvir studies included four studies examining the efficacy of daclatasvir in treating chronic HCV. AI444-040 [17] compared different treatment regimens of daclatasvir + sofosbuvir (± ribavirin); ALLY-3 [18] evaluated daclatasvir + sofosbuvir; and AI444-042 [19] and AI444-010 [20] compared daclatasvir + PR versus placebo + PR. All studies addressed NICE’s final scope. In addition, an ongoing long-term study was identified following up patients who had received daclatasvir with PR or with sofosbuvir (AI444-046) [21]. The five studies are listed in Table 1.
Sustained virologic response (SVR) was the primary outcome in all trials. Tables 2 and 3 summarise the daclatasvir SVR results presented in the submission, for the whole trial populations and for patients with METAVIR F4/compensated cirrhosis, and shows generally high SVR rates across genotypes 1, 3 and 4, including in patients with previous treatment experience, although there was no efficacy data available for a number of subpopulations.
Overall, there were few serious adverse events associated with interferon-free daclatasvir regimens. Rates appeared comparable to placebo + PR in the two trials that evaluated daclatasvir + PR. Serious adverse event rates associated with daclatasvir were low, and there was no evidence that daclatasvir use led to any increase in mortality.
Benchmarking review This consisted of a review and synthesis of studies of PR in HCV genotypes 1–4 and telaprevir with PR and boceprevir with PR in HCV genotype 1 to identify the expected SVR at 24 weeks follow-up (SVR24) for these treatments and to identify a ‘benchmark’ SVR24 rate at which daclatasvir could reasonably be considered non-inferior to or superior to these treatments. These benchmark SVR rates were compared with the observed response with daclatasvir in trial AI444-040 [17], to determine whether daclatasvir is superior or not inferior to the other treatments.
This analysis found that daclatasvir + sofosbuvir was superior to telaprevir + PR, boceprevir + PR and PR alone in genotype 1 patients. Daclatasvir with sofosbuvir was not found to be superior to PR in genotype 3 patients, but data in genotype 3 was limited. This evidence was not used by the manufacturer when summarising the clinical effectiveness of daclatasvir.
Matched adjusted indirect comparison (MAIC) review This analysis consisted of a review of all studies of telaprevir, boceprevir, sofosbuvir or simeprevir, all combined with PR or ribavirin, or PR alone, to identify the expected SVR24 or SVR12 response for these treatments. Results were presented separately for patients with significant fibrosis (F3–F4 non-cirrhotic), compensated cirrhosis, and the overall population (F0–F4). This was compared with the observed response to daclatasvir + sofosbuvir (±ribavirin) in trials AI444-040 [17] and ALLY-3 [18], adjusted to match the characteristics of patients in the other trials. Incidence of adverse events and treatment discontinuations were also compared.
The MAIC analysis found that SVR rates were higher for daclatasvir (combined with sofosbuvir ± ribavirin) than for other treatment combinations that used sofosbuvir, telaprevir or boceprevir in genotype 1 patients. In genotype 3 patients, daclatasvir + sofosbuvir had higher SVR rates than PR alone, but no statistically significant difference in rates was found when daclatasvir + sofosbuvir was compared with sofosbuvir + ribavirin.
Adverse events rates were generally similar to or lower with the interferon-free daclatasvir regimen than in the interferon-containing regimens. The MAIC analysis informed the manufacturer’s clinical effectiveness review and economic analyses.
Unadjusted trial comparisons A review of ‘best available evidence’ identified trials of relevant comparator combinations including sofosbuvir, simeprevir, telaprevir, boceprevir and PR. The SVR rates for the selected trials were reported according to patient genotype, treatment history and eligibility and baseline fibrosis severity. SVR results were presented in tables, side by side with daclatasvir trial results, with no formal conclusions made on the relative effectiveness of different treatments. Most results were not based on randomised trial evidence or matched adjusted indirect comparisons and instead represented absolute SVR rates in individual trial arms. These tables were used to inform the review of clinical evidence and the economic analyses.
3.1.2 Critique of the Clinical Evidence
Review of studies of daclatasvir The company’s submitted evidence on clinical effectiveness broadly addressed NICE’s final scope. The review of daclatasvir trials was of reasonable quality and appeared to have included all relevant trials. Baseline demographics of recruited patients were broadly comparable to the demographics of patients with chronic hepatitis that may be offered treatment in the UK, although difficult-to-treat populations such as patients with HIV, post-liver transplant, and patients with current or recent substance abuse were excluded.
The clinical evidence had a number of limitations. The two studies that evaluated daclatasvir + sofosbuvir did not have a control group. Despite the objective endpoints employed in the trials, the lack of a control group meant that the true efficacy of daclatasvir + sofosbuvir relative to alternative treatments was uncertain. For key subpopulations such as patients with compensated cirrhosis and those who had previously received treatment, data were all based on small subgroups and the efficacy of daclatasvir in these important patient subgroups was therefore highly uncertain. Finally, evidence was unavailable for daclatasvir in several patient subgroups in which daclatasvir was licensed, including daclatasvir + sofosbuvir 12 weeks in genotype 1 treatment-experienced patients, genotype 3 treatment-experienced cirrhotic patients receiving 24 weeks of treatment, genotype 4 patients, interferon ineligible or intolerant patients across genotypes and daclatasvir + PR in genotype 4 treatment-experienced patients.
Benchmarking review The searches for and the selection of studies included in the benchmarking analysis were considered generally acceptable, and the analysis approach was considered to be reasonable. The ERG considered the results of this analysis to be reasonably reliable.
Matched adjusted indirect comparison (MAIC) review The MAIC analyses were not based on randomised evidence as the two daclatasvir trials AI444-040 [17] and ALLY-3 [18] had no placebo or other comparator arm, and placebo arms from the trials of other treatments were not included in the analysis. Although the MAIC method aims to adjust results to account for possible differences between trials, the adjustment may be flawed if important unobserved characteristics were not accounted for.
The MAIC analyses results for genotype 1 patients were strongly dependent on the fact that AI444-040 [17] achieved a near perfect SVR12 success rate, and any adjustments to SVR rate were dependent on the characteristics of the one patient who did not achieve SVR. Data on patients with genotype 3 were limited. The ERG therefore considers the MAIC analysis to be unreliable and should be treated as if it were an unadjusted comparison of results from different trials, with substantial potential for bias or misleading conclusions.
Unadjusted trial comparisons Due to limited reporting of methods, and despite clarifications from the manufacturer, it was not clear whether the review of studies informing the ‘best available evidence’ efficacy tables was either systematic or comprehensive. It is therefore unclear whether the trials included were all the relevant trials of HCV treatments, or whether those included were representative of likely effects of the treatments. However, the ERG found no evidence to suggest that significant trials had been omitted.
Most results presented in the ‘best available evidence’ efficacy tables were not based on formal comparisons such as head-to-head or adjusted indirect comparisons. Therefore, most comparisons are observational and have significant limitations. In addition, there were concerns about the appropriateness and consistency of assumptions made to address missing data (such as assuming equivalence across genotypes, disease severity and treatment experience status). The ERG concluded that the limited evidence (particularly for patients with compensated cirrhosis) means that it was largely unclear whether the results for other treatments were comparable with those presented for daclatasvir-based regimens.
3.2 Cost-Effectiveness Evidence
3.2.1 Summary of Cost-Effectiveness Evidence
The company developed a new decision analytic model to compare daclatasvir-containing regimens, daclatasvir + sofosbuvir ± ribavirin, and daclatasvir + PR, with the comparators defined in the NICE scope: PR, telaprevir + PR, boceprevir + PR, simeprevir + PR, sofosbuvir + PR, sofosbuvir + ribavirin, simeprevir + sofosbuvir and best supportive care (considered by the manufacturer as equivalent to no treatment).
The model predicted the NHS costs and the quality-adjusted life-years (QALYs) over the patients’ lifetime for each treatment option. It consisted of a decision tree combined with a Markov model. The decision tree modelled the effectiveness and costs for the first year of the model, during which treatment occurs. The Markov model simulated the natural history of the disease over the patients’ lifetime. In the model, SVR improved health-related quality of life (HRQoL) and halted disease progression. The SVR rates of daclatasvir + sofosbuvir ± ribavirin and daclatasvir + PR were obtained from subgroups of the individual trial arms of AI444-040 [17], AI444-042 [19] and ALLY-3 [18]. SVR rates were obtained from the unadjusted trial comparison of individual trial arms described above.
The company submission presented deterministic results for a total of 27 subpopulations. Daclatasvir-containing regimens were cost effective under the £20,000–£30,000 per QALY gained threshold in the F3–F4 non-cirrhotic and compensated cirrhotic subpopulations as presented in Table 4.
The cost-effectiveness drivers were SVR rates, drug prices and treatment duration. SVR was associated with a halt in disease progression, greater HRQoL and zero costs in the long term. Treatment duration was a key determinant of total drug acquisition costs, which was the largest driver of incremental lifetime costs. Hence, treatments with greater SVR rates and lower treatment durations had more favourable cost-effectiveness profiles.
3.2.2 Critique of Cost-Effectiveness Evidence Submitted
The manufacturers’ cost-effectiveness analysis generally followed the NICE reference case and the NICE scope, and the development of a de novo cost-effectiveness model was found to be appropriate and necessary for this appraisal. The model had an appropriate structure and captured most relevant health outcomes.
The manufacturer presented results stratified by disease severity as well as an analysis in the entire population (F0–F4). The analysis in the entire patient population was considered uninformative given the heterogeneity across METAVIR fibrosis states in SVR rates, the natural history of the disease, and the licensed treatment options. The remainder of this section therefore focuses on the analysis stratified by disease severity.
The ERG considered the cost-effectiveness submission to have a number of limitations. The three key issues relate to the subgroup analysis of the F0–F2 subgroup, the exclusion of relevant comparators and the clinical effectiveness (SVR) data used in the model.
The F0–F2 analysis presented by the manufacturer was limited to a subset of selected pairwise comparisons, was not informed by SVR data specific to the F0–F2 population and did not include a watchful waiting strategy (i.e. a ‘no treatment’ option until a patient reaches F3 or F4). The ERG therefore considers that insufficient evidence was presented for the F0–F2 subpopulations and the methods and results for these subgroups were not explored further by the ERG.
The ERG identified a number of concerns with the analyses presented for the F3/F4 (non-cirrhotic) and compensated cirrhosis populations. The manufacturer excluded important comparators. Sofosbuvir + PR and simeprevir + sofosbuvir were omitted from a number of analyses on the basis of a lack of data on effectiveness. While this is reasonable given the available evidence during the period in which the manufacturer developed its submission, for some subpopulations these comparators were recommended by NICE during the course of the appraisal process. ‘Best supportive care (watchful waiting)’ was interpreted as no treatment. In reality, watchful waiting amongst less severe patients is likely to involve a period of observation followed by treatment if patients reach more severe disease stages. This treatment strategy was not included as a comparator. In treatment-naïve patients, the possibility of further treatment following initial treatment failure was not considered.
Efficacy data used in the model were at high risk of bias and were highly uncertain as they were not based on randomised or adjusted comparisons. Where data were not available for specific comparators in specific subpopulations, they were extrapolated from populations with different disease severities, treatment histories and genotypes.
Other limitations were: (1) the failure to explore the impact of prior treatment response within the treatment-experienced subgroup, as suggested in the NICE scope; (2) the modelling of the experience of cirrhosis patients with SVR, who were assumed to experience a greater improvement in HRQoL due to SVR than less severe patients, and no further disease progression or HCV-related costs (however, evidence suggests that patients with SVR experience disease progression, albeit at a much lower rate than patients without SVR, and there is no evidence that achievement of SVR offers greater HRQoL benefits in more severe patients [22]); and (iii) the progression rates used in the model, which may not reflect the natural history of patients in the UK.
3.2.3 ERG’s Additional Analyses
The ERG conducted a number of changes to the manufacturer’s model that, together with some minor corrections to the implementation of the model, constitutes the ERG’s base case. The ERG’s changes included:
-
the inclusion of all relevant comparators and exclusion of the treatment regimens not recommended by NICE;
-
alternative SVR estimates for specific subgroups and treatment combinations;
-
using alternative progression rates for genotype 4 patients;
-
allowing cirrhotic patients with SVR to progress to decompensated cirrhosis or hepatocellular cancer;
-
assigning a reduced improvement in HRQoL to cirrhotic patients with SVR;
-
assigning lifetime monitoring costs for cirrhotic patients with SVR.
Table 4 also shows the results of the ERG’s base case. Daclatasvir-containing regimens were cost-effective under the £20,000-£30,000 per QALY gained threshold in the following F3 populations: genotype 1 treatment naïve, treatment experienced and interferon ineligible or intolerant; genotype 3 interferon ineligible or intolerant; genotype 4 treatment experienced or interferon ineligible or intolerant. In F4 (cirrhotic) patients, daclatasvir-containing regimens are not cost-effective in any of the subpopulations. The difference in results between the manufacturer’s and the ERG’s base case was driven by the addition of relevant comparators and removal of comparators not recommended by NICE, and by the use of alternative SVR estimates. The results were sensitive to changes in SVR rates, changes to treatment durations as permitted by the licences for daclatasvir and comparators, and inclusion of slower rates of progression to cirrhosis. The cost effectiveness of daclatasvir + sofosbuvir in genotype 1 treatment-naïve F3 patients was found to be dependent on the comparators included in the analysis. In an analysis conducted by the ERG, comparators comprising treatment sequences were included. The treatment sequences reflected the reality that patients can be trialled on a cheaper, less effective regimen followed by a more expensive treatment for those who failed to achieve SVR. This analysis suggested that it may be cost effective to offer PR as first-line treatment and reserve daclatasvir + sofosbuvir for those who fail first-line treatment.
3.3 Conclusions of the ERG Review
The ERG concluded that in genotype 1 treatment-naïve patients, the evidence suggests that daclatasvir (+sofosbuvir, ±ribavirin) has higher SVR rates than PR, telaprevir + PR, boceprevir + PR, and possibly simeprevir + PR and sofosbuvir + PR, although this conclusion should be treated with caution due to potential for bias. However, it is reasonable to conclude that daclatasvir + sofosbuvir ± ribavirin is unlikely to be inferior to other treatments in genotype 1 patients. Evidence was too limited in a number of subpopulations, including patients with compensated cirrhosis, previous treatment experience and in those of genotypes 3 and 4, so the ERG does not think any conclusions can be safely made on the relative efficacy of daclatasvir and other treatments in these patients.
Daclatasvir + sofosbuvir was cost effective only in some F3 subgroups: those infected with genotype 1, those infected with genotype 3 interferon ineligible or intolerant, and those infected with genotype 4 who are treatment experienced or interferon ineligible or intolerant. Daclatasvir was not cost effective in combination with PR either in any subgroups or in combination with sofosbuvir in cirrhotic patients. Reserving daclatasvir + sofosbuvir as second-line treatment after failure with PR may be a more cost-effective option in genotype 1 treatment-naïve patients.
The main sources of uncertainty regarding the clinical effectiveness evidence for daclatasvir included (1) the lack of a control group in the two studies evaluating daclatasvir + sofosbuvir; (2) the lack of randomised or controlled comparisons between daclatasvir and relevant comparators; and (3) the limited data for SVR12–24 results in patients with compensated cirrhosis or with prior treatment experience, which were all based on small subgroups.
The main areas of uncertainty for the cost-effectiveness assessment were the effectiveness of daclatasvir and comparator treatments and their treatment durations. The uncertainty in SVR rates arose as data were obtained from individual trial arms and were therefore subject to bias if these trials were not comparable in all factors that affect outcomes. Treatment duration was uncertain as the marketing authorisations for daclatasvir and comparator drugs allow for changes in treatment duration depending on the patient’s characteristics. These two issues made the cost effectiveness of daclatasvir uncertain for some subgroups.
3.4 Company’s Additional Evidence
The company submitted evidence from five worldwide compassionate use and early-access programmes on people with cirrhosis and decompensated cirrhosis. The five cohort studies submitted were (A) French compassionate use programme (CUP); (B) NHS England early access programme (EAP); (C) EU CUP; (D) ANRS CO22 HEPATHER cohort (France); and (E) HCV-TARGET cohort.
Cohorts A, B, C and D reported SVR12 data on daclatasvir + sofosbuvir and daclatasvir + sofosbuvir + ribavirin and included patients who had generally more severe liver disease than in the original manufacturer’s submission, including patients with decompensated cirrhosis. Cohort B also included patients treated with ledipasvir + sofosbuvir. Cohort D included patients who received a range of sofosbuvir-based treatments, including combinations with simeprevir. Cohort E did not use daclatasvir, but reported on other sofosbuvir-based treatments. SVR results from cohorts evaluating daclatasvir were reported by genotype and are presented in Table 5. Results from cohort A were commercial in confidence and therefore could not be reported.
The company presented an additional cost-effectiveness analysis in people with cirrhosis and HCV genotype 3 who are interferon ineligible. This analysis differed from the manufacturer base case in as it used SVR rates from the French CUP programme and dropped one comparator (sofosbuvir + ribavirin). Daclatasvir + sofosbuvir was shown to be cost effective, with an incremental cost-effectiveness ratio (ICER) of £14,037 per QALY gained. The manufacturer also submitted cost-effectiveness evidence for patients with decompensated cirrhosis using data from NHS England EAP and HCV-TARGET and their decision model.
3.4.1 ERG’s Critique of the Additional Evidence
The data from the new cohort studies are broadly consistent with the trials in the original submission, but provided additional supporting evidence, particularly for patients of genotype 3. The new data suggested that daclatasvir-based regimens were highly effective for treating HCV infection, and that daclatasvir + sofosbuvir (±ribavirin) may be slightly less effective in genotype 3 than genotype 1. The UK EAP data suggests that daclatasvir-based treatment may also be effective in patients with decompensated cirrhosis, but SVR rates may be lower than for compensated cirrhosis. The ERG concluded that even with these additional cohorts, the numbers of patients across studies remains limited for specific subgroups, so it is not possible to draw firm conclusions about differences across genotypes or other subgroups of patients. The lack of formal comparative trials in the original evidence base or this additional evidence means any comparisons between different treatments may not be reliable.
The additional cost-effectiveness evidence submitted on the use of daclatasvir + sofosbuvir ± ribavirin in patients with HCV genotype 3 with cirrhosis who are ineligible for interferon was considered to be biased. The analysis compared daclatasvir + sofosbuvir ± ribavirin with no treatment, although sofosbuvir + ribavirin is licensed for this subgroup and has been recommended by NICE [23].
The ERG considered the cost-effectiveness analyses on the decompensated cirrhosis subgroups to be unreliable. The model structure did not allow for patients with decompensated cirrhosis to be treated. Hence, the company modelled treatment as occurring in the cirrhotic health state. The model did not therefore reflect the different prognosis of patients with decompensated cirrhosis. Furthermore, the use of daclatasvir in patients with decompensated cirrhosis was not considered in the original submission nor is daclatasvir explicitly recommended for this group in its product licence. For these reasons, the ERG concluded that the company did not make an adequate case to consider daclatasvir in this subgroup.
4 Consideration of All Available Evidence
The NICE Appraisal Committee reviewed the evidence on the clinical and cost effectiveness of daclatasvir and the value placed on the benefits and harms of daclatasvir by patients, those who represent them and clinical specialists. It also took into account the effective use of NHS resources.
4.1 Preliminary Guidance
The Committee recommended daclatasvir + sofosbuvir (12 weeks duration) as an option for treating chronic HCV in adults with genotypes 1 or 4, in patients who are treatment experienced or interferon ineligible/intolerant and have significant fibrosis (METAVIR fibrosis stage F3–F4) but no cirrhosis [24]. These recommendations aligned with the ERG base-case cost-effectiveness analysis, except for genotype 1 treatment-naïve F3 and genotype 3 interferon-ineligible F3 populations. Although the ERG base-case analysis found daclatasvir + sofosbuvir to be cost effective in these subpopulations, the Committee concluded that the ICERs were not sufficiently robust to plausible changes in SVR rates.
4.2 Manufacturer’s Response to the Appraisal Consultation Document (ACD) Consultation
The manufacturer submitted a response to the consultation, which included additional cost-effectiveness analyses on genotype 3 patients and changes to the originally submitted model. The model was revised to incorporate nationally available price discounts for daclatasvir, and to use alternative SVR data for sofosbuvir + ribavirin in genotype 3 interferon-ineligible or -intolerant cirrhotic patients. As the revised marketing authorisation for daclatasvir had been granted by this point, a 12-week treatment duration for daclatasvir + sofosbuvir was used in all non-cirrhotic genotype 3 subgroups.
4.3 ERG Critique of the Response Submitted by the Manufacturer in Response to the ACD Consultation
The ERG raised concerns with the use of nationally agreed price discounts for daclatasvir but not for other comparators which are known to have similar agreements with the Department of Health.
The ERG considered the alternative SVR sources for sofosbuvir + ribavirin provided by the manufacturer to be clinically plausible. The ERG conducted a threshold analysis to estimate the difference in SVR between daclatasvir + sofosbuvir and sofosbuvir + ribavirin required for daclatasvir + sofosbuvir to be cost effective at £20,000 and £30,000 per QALY in patients with genotype 3 who are F4 (cirrhotic) and interferon ineligible or intolerant, and found that using the revised cost for daclatasvir, daclatasvir + sofosbuvir was likely to be cost effective in this population (though not at the list price).
5 NICE Guidance
Following the consultation on the preliminary guidance, the NICE Appraisal Committee released the following final guidance to the NHS (TA364) on 25 November 2015 [2]:
“Daclatasvir is recommended as an option for treating chronic HCV in adults, as specified in Table 1, only if the company provides daclatasvir at the same price or lower than that agreed with the Commercial Medicines Unit.”
Further details of the guidance and appraisal committee’s consideration of the evidence is available on the NICE website [2].
6 Interpretation of the Guidance
This single technology appraisal highlights some important challenges faced by NICE in appraising drugs in the rapidly evolving hepatitis C treatment landscape. The new drugs for hepatitis C entered the market in quick succession: simeprevir, sofosbuvir, ledipasvir + sofosbuvir, daclatasvir, and ombitasvir + paritaprevir + ritonavir ± dasabuvir were all granted marketing authorisation in 2014–15. NICE appraised the new drugs under the STA process and compared each drug with the treatments available in the NHS at the time of scoping. As a result, treatments appraised concurrently with daclatasvir (e.g. ledipasvir + sofosbuvir) were not directly compared with daclatasvir. Further relevant comparators may also not have been included. These include using the new drugs as second-line treatment following treatment failure with PR, and watchful waiting at milder disease stages followed by treatment upon progression. Process improvements to facilitate inclusion of all potentially relevant comparators should be considered to minimise the risks of comparing only a subset of treatment options.
The clinical data supporting the marketing authorisation for daclatasvir was highly uncertain. Naïve comparisons of single-arm studies are at high risk of bias since patient characteristics that affect prognosis may not be evenly balanced [25]. Methods to adjust the cohorts for differences in prognostic characteristics have been suggested [26]. However, these methods have not been widely applied or evaluated and within this appraisal were found to be subject to significant limitations, particularly when sample sizes were small. This uncertainty means that treatments that appear cost effective under the current evidence may not be cost effective as new evidence emerges. Rigorous validation and further guidance regarding the use and appraisal of statistical methods to account for biases arising from comparisons of single trial arms and to reflect the additional uncertainty arising from such comparisons are required [26].
The new drugs for hepatitis C have the potential to impose a large upfront demand on NHS resources. The patient population in the UK has been estimated at 214,000 people, although only 5000 or less are currently treated per year [4]. NHS England expressed concerns during this appraisal that up to 20,000 people per year could access hepatitis C treatment, and argued this would not be affordable given the NHS budget [27]. An increase in demand for hepatitis C treatment may cause the displacement of higher value treatments than implied by the NICE cost-effectiveness threshold. If these displaced interventions offer more health benefits than the new treatments for hepatitis C, uptake of the new treatments may result in a net loss of health NHS-wide. In the case of daclatasvir, the NICE Appraisal Committee concluded that these scenarios were unlikely and that the financial impact of the new drugs could be adequately managed by the existing mechanisms, such as tendering and the 2014 Pharmaceutical Price Regulation Scheme [27]. However, it has been argued that lower cost-effectiveness thresholds or alternative financing mechanisms may be relevant for drugs with large short-term budget impacts, although there are ethical implications on whether it is acceptable to discriminate against high-prevalence conditions [28]. The implementation of the new hepatitis C drugs may provide some insight on how best to manage a large and uncertain financial burden within the NICE process and UK NHS.
References
National Institute for Health and Care Excellence. Guide to the methods of technology appraisal. London: NICE; 2013.
National Institute for Health and Care Excellence. Daclatasvir for treating chronic hepatitis C. London: National Institute for Health and Care Excellence; 2015.
World Health Organization. Hepatitis C. Fact sheet N 164; 2015.
Public Health England. Hepatitis C in the UK: 2015 report. London: Public Health England; 2015.
European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatitis C virus infection. J Hepatol. 2014;60(2):392–420. doi:10.1016/j.jhep.2013.11.003.
Esteban JI, Sauleda S, Quer J. The changing epidemiology of hepatitis C virus infection in Europe. J Hepatol. 2008;48(1):148–62. doi:10.1016/j.jhep.2007.07.033.
Seeff LB. Natural history of chronic hepatitis C. Hepatology. 2002;36(S1):S35–46. doi:10.1002/hep.1840360706.
National Institute for Health and Care Excellence. Hepatitis C. 2015. https://www.nice.org.uk/guidance/indevelopment/gid-cgwave0666. Accessed 30 Nov 2015.
National Institute for Health and Care Excellence. Evaluation report for telaprevir for hepatitis C (chronic) [TA252]. 2012. http://www.nice.org.uk/guidance/TA252 Accessed 12 Jan 2015.
National Institute for Health and Care Excellence. Evaluation report for boceprevir for hepatitis C (chronic) [TA253]. 2012. http://www.nice.org.uk/guidance/ta253/documents Accessed 12 Jan 2015.
National Institute for Health and Care Excellence. Technology Appraisal 200. Peginterferon alfa and ribavirin for the treatment of chronic hepatitis C. 2010. http://www.nice.org.uk/guidance/TA200. Accessed 12 Jan 2015.
National Institute for Health and Care Excellence. Evaluation report for simeprevir for hepatitis C (chronic) [ID668]. 2014. http://www.nice.org.uk/guidance/gid-tag455/documents/hepatitis-c-chronic-simeprevir-id668-evaluation-report2. Accessed 12 Jan 2015.
National Institute for Health and Care Excellence. Evaluation report for sofosbuvir for hepatitis C (chronic) [ID654]. 2014. http://www.nice.org.uk/guidance/gid-tag445/documents/hepatitis-c-chronic-sofosbuvir-evaluation-report2. Accessed 12 Jan 2015.
National Institute for Health and Care Excellence. Ledipasvir–sofosbuvir for treating chronic hepatitis C. London: National Institute for Health and Care Excellence; 2015.
National Institute for Health and Care Excellence. Ombitasvir–paritaprevir–ritonavir with or without dasabuvir for treating chronic hepatitis C. London: National Institute for Health and Care Excellence; 2015.
Bristol-Myers Squibb Pharmaceuticals Ltd. Summary of Product Characteristics. Daklinza® 30 mg and 60 mg film-coated tablets. 2014. http://www.medicines.org.uk/emc/medicine/29129. Accessed 3rd Feb 2015.
Sulkowski MS, Gardiner DF, Rodriguez-Torres M, Reddy KR, Hassanein T, Jacobson I, et al. Daclatasvir plus sofosbuvir for previously treated or untreated chronic HCV infection. N Engl J Med. 2014;370(3):211–21. doi:10.1056/NEJMoa1306218.
Nelson DR, Cooper JN, Lalezari JP, Lawitz E, Pockros PJ, Gitlin N, et al. All-oral 12-week treatment with daclatasvir plus sofosbuvir in patients with hepatitis C virus genotype 3 infection: ALLY-3 phase III study. Hepatology. 2015;61(4):1127–35.
Hézode C, Alric L, Brown A, Hassanein T, Rizzetto M, Buti M et al. Randomized controlled trial of the NS5A inhibitor daclatasvir plus peginterferon and ribavirin for HCV genotype-4 (COMMAND-4). Antivir Ther. 2015. doi:10.3851/IMP2985.
Hézode C, Hirschfield GM, Ghesquiere W, Sievert W, Rodriguez-Torres M, Shafran SD et al. Daclatasvir plus peginterferon alfa and ribavirin for treatment-naive chronic hepatitis C genotype 1 or 4 infection: a randomised study. Gut. 2015;64(6):948–56. doi:10.1136/gutjnl-2014-307498.
Reddy KR, Pol S, Thuluvath PJ, Kumada H, Toyota J, Chayama K, et al., editors. Long-term follow-up of patients treated with daclatasvir-based regimens in phase 2 and 3 studies. Hepatology. Hoboken: Wiley; 2014.
Cardoso AC, Moucari R, Figueiredo-Mendes C, Ripault MP, Giuily N, Castelnau C, et al. Impact of peginterferon and ribavirin therapy on hepatocellular carcinoma: incidence and survival in hepatitis C patients with advanced fibrosis. J Hepatol. 2010;52:652–7.
National Institute for Health and Care Excellence. Sofosbuvir for treating chronic hepatitis C. London: National Institute for Health and Care Excellence; 2015.
National Institute for Health and Care Excellence. Appraisal consultation document. Daclatasvir for treating chronic hepatitis C. London: National Institute for Health and Care Excellence; 2015.
Faria R, Hernandez Alava M, Manca A, Wailoo AJ. NICE DSU technical support document 17: the use of observational data to inform estimates of treatment effectiveness for technology appraisal: methods for comparative individual patient data. Sheffield: NICE Decision Support Unit; 2015.
Batson S, Mitchell S, King D. The use and acceptance of novel statistical analyses to support technology submissions to hta authorities. Value Health. 2014;17(7):A576–7.
National Institute for Health and Care Excellence. Final appraisal determination—daclatasvir for treating chronic hepatitis C. London: National Institute for Health and Care Excellence; 2015.
Woods B, Faria R, Griffin S. Assessing the value of new treatments for hepatitis C: are international decision makers getting this right? PharmacoEconomics. 2015;34(5):427–33. doi:10.1007/s40273-015-0369-5.
Acknowledgments
This project was funded by the National Institute for Health Research (NIHR) Health Technology Assessment (HTA) programme (project number 14/148/01). See the HTA programme website (http://www.hta.ac.uk) for further project information. This summary of the Evidence Review Group (ERG) report was compiled after the Appraisal Committee’s review and incorporates additional information and comment from the authors on the single technology appraisal (STA) process and iterations of the NICE guidance not covered by the STA report. The ERG would like to thank Prof. Will Irving and Dr. Steve Ryder for providing clinical and technical advice throughout the project. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of NICE or the Department of Health. This work is Crown copyright (UK).
Authors contributions
AL, RF, BW, MS, JL, NW and SG all formed part of the ERG that produced the ERG report that this paper describes. AL, RF and BW drafted the manuscript. All authors commented on the manuscript and approved the final version.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The University of York has received funding relating to hepatitis C from the Department of Health via the Policy Research Unit in Economic Evaluation of Health Care Interventions (EEPRU). As part of this research, BW, RF and SG have worked with NHS England to inform a strategy for implementing NICE guidance for hepatitis C. SG is a member of the NICE Technology Appraisal Committee and has sat in Committee meetings that appraise the use of treatments for hepatitis C in the NHS. SG receives no financial support from NICE for her role as Committee member but is reimbursed for travel expenses incurred to attend Committee meetings. Neither NICE nor SG have any financial interest in the subject matter of this paper.
Conflict of interest
The authors have no other conflicts of interest that are directly relevant to the content of this article.
Rights and permissions
About this article

Cite this article
Llewellyn, A., Faria, R., Woods, B. et al. Daclatasvir for the Treatment of Chronic Hepatitis C: A Critique of the Clinical and Economic Evidence. PharmacoEconomics 34, 981–992 (2016). https://doi.org/10.1007/s40273-016-0418-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40273-016-0418-8