
Abstract
Neo-angiogenesis plays a key role in colorectal cancer, with the vascular endothelial growth factor family proteins and their receptors in particular triggering multiple signaling networks that result in endothelial cell survival, migration, mitogenesis, differentiation, and vascular permeability. Anti-angiogenic therapies have improved colorectal cancer prognosis within the past 15 years. Bevacizumab demonstrated efficacy in combination with chemotherapy under different conditions, including as first- and second-line therapies, and also as a maintenance treatment strategy. Other drugs targeting angiogenesis effectors (e.g., ramucirumab and aflibercept) were approved after bevacizumab failure, confirming the concept of “continuous anti-angiogenic blocking”. Recently, a number of new orally available multiple receptor tyrosine kinase inhibitors have been tested in late-stage clinical trials, with modest efficacy. Due to the availability of several anti-angiogenic agents, we need well-designed prospective randomized trials to optimize therapeutic sequencing. The place of biosimilars in the therapeutic armamentarium remains unclear at the moment. Further research is warranted to identify robust predictive biomarkers of efficacy and innovative clinically meaningful anti-angiogenic drugs that are cost-efficient.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Anti-angiogenic therapies have significantly improved metastatic colorectal cancer prognosis, demonstrating efficacy in combination with chemotherapy under different conditions (e.g., first- and second-line settings, maintenance strategy). |
Recently, several orally available multiple receptor tyrosine kinase inhibitors have been tested in later stages of the disease, with modest efficacy. |
Current ways of research encompass the identification of robust predictive biomarkers of efficacy and the possibility of substituting biosimilars for original drugs. |
1 Introduction
Incidence rates of colorectal cancer (CRC) have been falling on average by 2.7% each year over the last decade [1], but it is estimated that almost 135,500 new cases were diagnosed in the USA in 2017 [2]. Although commonly associated with good outcomes, 5-year overall survival (OS) is about 65% across all stages, and decreases to 15% in case of distant metastases [2]. Despite strong hereditary components, extrinsic factors such as physical activity, sedentary behavior, and diet seem to be key factors in colorectal carcinogenesis [3].
At a molecular level, most CRCs (85%) show a microsatellite stable (MSS) or low-level microsatellite instability (MSI-L) phenotype, and are characterized by chromosomal changes, leading to the classic adenoma–carcinoma pathway [4]. About 15% of colorectal tumors have a high-level microsatellite instability (MSI-H) phenotype as a result of DNA mismatch repair deficiency. Among MSI-H tumors, 3% are related to Lynch syndrome and 12% correspond to sporadic tumors [4]. There is increasing evidence demonstrating a relationship between molecular pathogenesis, prognosis, and therapy response. A more refined classification based on gene expression was recently developed thanks to an international consortium of experts, defined as the “consensus molecular subtypes” (CMSs) of CRC [5]. Four subtypes were thus identified: CMS1 (microsatellite instability immune), CMS2 (canonical), CMS3 (metabolic), and CMS4 (mesenchymal). The latter represents almost one-quarter of the CRCs, and is characterized by high expression of mesenchymal genes, stromal infiltration, transforming growth factor beta (TGF-β) activation, and angiogenesis. CMS4 tumors display worse overall and relapse-free survival compared with other molecular subtypes, underlying the essential role of angiogenesis in CRC progression [5]. However, in the pan-GI TCGA analysis, the CMS subtypes did not map well, casting some doubt regarding their long-term utility [6]. Additionally, a significant proportion of CRC tumors do not classify in the CMS categories.
When neo-angiogenesis is not possible for several reasons, cancer stem cells are able to reprogram themselves to form blood vessels as a backup strategy. Activation of the transforming growth factor beta (TGF-β) pathway thus seems to play a key role in the initiation of angiogenesis in colon cancer stem cells [7], opening the way to potential novel therapeutic approaches.
The relationship between neo-angiogenesis and tumor proliferation was first described almost 50 years ago [8], but the clinical efficacy of bevacizumab [a monoclonal antibody against vascular endothelial growth factor (VEGF)] in CRC patients was only demonstrated in 2004 [9]. Several growth factor receptor pathways have been implied to promote tumor angiogenesis, but the VEGF family proteins and their receptors play a central role, triggering multiple signaling networks that result in endothelial cell survival, migration, mitogenesis, differentiation, and vascular permeability [10]. We currently know of six effectors in the VEGF family secreted by tumor cells (VEGF-A to D and placental growth factor (PIGF) 1 and 2), binding to three different types of receptors (VEGFR-1, VEGFR-2, and VEGFR-3). The interaction between VEGF and its receptor leads to the dimerization of two receptors. Subsequently, the tyrosine kinase domain of each receptor phosphorylates the other, which initiates a signaling cascade involving the activation of several pathways such as Ras-Raf-MAPK, Scr-FAK, or AKT-mTOR. The VEGF pathway is upregulated by several growth factors, including epidermal growth factor (EGF), platelet-derived growth factors (PDGFs), hepatocyte growth factor (HGF), and other cytokines [11]. The presence of elevated circulating levels of VEGF has been shown to be predictive of liver and lung metastasis [12]. High VEGF serum level was associated with poorer survival in case of CRC. In a meta-analysis published in 2014, hazard ratio (HR) for death was 2.25 (95% confidence interval (CI) 1.35–3.74) [13].
Tumor angiogenesis can be blocked through several ways. Anti-angiogenic monoclonal antibodies bind to and therefore neutralize a specific target such as VEGF-A (bevacizumab) or VEGFR-2 (ramucirumab). Aflibercept is a recombinant fusion protein inhibiting the VEGF-A, VEGF-B, and PIGF pathways, which may help to overcome tumor escape mechanisms to bevacizumab treatment. Novel antiangiogenic agents, essentially oral tyrosine kinase inhibitors (TKI), seem promising in targeting several signaling pathways, even in heavily pretreated CRC patients. In this review, we discuss and highlight current and future approaches in angiogenic targeting for CRC.
2 Bevacizumab
2.1 First-Line Treatment
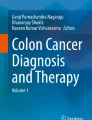
Bevacizumab is a recombinant humanized (93% human and 7% murine) monoclonal immunoglobulin G1 antibody that binds to all isoforms of VEGF-A (Fig. 1) with a reported half-life of 17–21 days, preventing the interaction between VEGF-A and VEGFR-1 and -2 [14]. AVASTIN® (Roche) was the first anti-VEGF agent approved as first-line therapy for metastatic CRC (mCRC) patients, In the first-line setting, bevacizumab was associated with an increased median OS compared with placebo in 813 patients with previously untreated mCRC (HR 0.66; p < 0.001) [9]. (Table 1) All patients received IFL (irinotecan, bolus fluorouracil, and leucovorin) as backbone chemotherapy, but capecitabine plus oxaliplatin (XELOX) or fluorouracil/folinic acid plus oxaliplatin (FOLFOX) were also valuable choices [15]. A recent phase III study confirmed the absence of difference between FOLFIRI (5-fluoruracil, leucovorin, and irinotecan) and FOLFOX in addition to bevacizumab in treatment-naïve mCRC patients [16]. The 2016 ESMO guidelines recommend any chemotherapy doublet with bevacizumab as first-line treatment, especially in patients with a RAS mutated tumor [17]. In a meta-analysis of nine studies and 3710 patients with mCRC, the addition of bevacizumab to chemotherapy significantly prolonged progression-free survival (PFS) (HR 0.66, 95% CI 0.55–0.77; p < 0.0001) and OS (HR 0.84, 95% CI 0.77–0.92; p = 0.0001) [18].

Vascular endothelial growth factor (VEGF) pathway and targeted therapies. PIGF placental growth factor, VEGFR vascular endothelial growth factor receptor, PI3K phosphoinositide 3-kinase, Akt protein kinase B, NFκB nuclear factor kappa-light-chain-enhancer of activated B cells, RAS rat sarcoma, RAF rapidly accelerated fibrosarcoma, MEK mitogen-activated protein kinase, ERK extracellular signal-regulated kinases. *Regorafenib also inhibits multiple targets in addition to VEGFR-2, not shown in this figure: PDGFR, FGF, KIT, RET, RAF1, B-RAF, and B-RAF-V600E
The concept of intensive chemotherapy associated with high response rates has recently emerged, with the aim of surgery in patients with potentially resectable liver metastases. In the TRIBE study, 508 patients with untreated mCRC received FOLFIRI plus bevacizumab or FOLFOXIRI plus bevacizumab [19]. The objective response rate (ORR) was 65% in the experimental group and 53% in the control group (p = 0.006). The median PFS was significantly increased (HR 0.75, 95% CI 0.62–0.90; p = 0.003), but incidences of grade 3 or 4 neurotoxicity, stomatitis, diarrhea, and neutropenia were significantly higher in cases of triplet chemotherapy (Table 2). These results were confirmed in a randomized phase II trial with FOLFOX as control treatment [20]. In a systematic review with pooled analysis, including 11 FOLFOXIRI-bevacizumab studies (n = 889), the ORR was 69% [21]. The rate of overall surgical conversions was 39%, and the rate of R0 surgical conversions was 28%.
Elderly patients are often under-represented in clinical trials although they represent a significant proportion of patients seen at our practices. In the phase III AVEX trial, 280 patients aged 70 years and older who were not deemed to be candidates for oxaliplatin-based or irinotecan-based chemotherapy regimens were randomly assigned to capecitabine alone or with bevacizumab [22]. Median PFS was significantly longer with bevacizumab and capecitabine than with capecitabine alone (9.1 months vs. 5.1 months, HR 0.53, 95% CI 0.41–0.69; p < 0.0001). Bevacizumab was generally well tolerated, albeit with more grade 3 or worse treatment-related adverse events compared with placebo (40% vs. 22%), especially hemorrhage (25% vs. 7%), hand-foot syndrome (16% vs. 7%), and venous thromboembolic events (8% vs. 4%). A phase II study recently confirmed the possibility for treating elderly patients effectively and safely with chemotherapy doublets and bevacizumab in the first-line setting [23].
Finally, in the adjuvant setting the addition of bevacizumab to the standard FOLFOX regimen failed to improve disease-free survival in two large phase III studies conducted in stage II and III CRC patients [24, 25].
2.2 Maintenance Treatment
The optimum duration of first-line treatment for mCRC is complex. On the one hand, the longer the chemotherapy duration is, the higher the cumulative toxicity is, with potential impaired quality of life and increasing treatment cost. On the other hand, longer duration of treatment is associated with a longer PFS, and potentially increases OS. In the phase III CAIRO3 study, 558 patients with previously untreated mCRC and stable disease or better after induction treatment with six 3-weekly cycles of capecitabine, oxaliplatin, and bevacizumab (CAPOX-B) were randomly assigned to either maintenance treatment with capecitabine and bevacizumab (CAP-B) or observation [26]. Median PFS between randomization and first progression was significantly improved in case of maintenance therapy compared with observation (8.5 months vs. 4.1 months). The AIO 0207 study was a non-inferiority randomized phase III trial comparing standard maintenance treatment with a fluoropyrimidine plus bevacizumab, bevacizumab alone, or no treatment in 472 mCRC patients without disease progression after 24 weeks of induction therapy with either fluorouracil plus leucovorin plus oxaliplatin or capecitabine plus oxaliplatin, both with bevacizumab [27]. Median time to failure of strategy was 6.9 months for the fluoropyrimidine plus bevacizumab group, 6.1 months for the bevacizumab-alone group, and 6.4 months for the no-treatment group. In a post hoc analysis, CAP-B maintenance treatment after six cycles of CAPOX-B is effective in mCRC across all mutational subgroups (RAS wild-type/RAS mutant, BRAF wild-type/BRAF mutant, MSS/MSI tumors) [28]. A recent meta-analysis of these two phase III trials confirmed that maintenance treatment with fluoropyrimidine plus bevacizumab is effective in all patients, regardless of the investigated subgroups (sex, age, performance status, response to induction treatment, primary tumor location, number of metastatic sites, disease stage and primary tumor resection, serum LDH, platelet count, CEA, and RAS/BRAF mutation status) [29]. The 2016 ESMO guidelines recommend that patients receiving FOLFOX or CAPOX plus bevacizumab-based therapy as induction therapy should be considered for maintenance therapy after six cycles of CAPOX and eight cycles of FOLFOX [17]. The optimal maintenance treatment is therefore a combination of a fluoropyrimidine plus bevacizumab, whereas bevacizumab as monotherapy is not recommended.
2.3 Second-Line Treatment
In bevacizumab-naïve mCRC patients previously treated with FOLFIRI, the combination of FOLFOX and bevacizumab was associated with a reduced risk of death (HR 0.75; p = 0.0011) compared with FOLFOX alone [30]. PFS and ORR were also significantly improved. Preclinical data also suggest that VEGF has a continuous expression during tumor progression and that a prolonged exposure to anti-angiogenic agents beyond progression could delay tumor growth [31]. After promising retrospective data [32, 33], several prospective studies confirmed the concept of “continuous anti-angiogenic blocking”. In the ML18147/TML study, 409 patients with mCRC progressing up to 3 months after discontinuing first-line bevacizumab plus chemotherapy were randomly assigned to second-line chemotherapy with or without bevacizumab [34]. Median OS was 11.2 months for bevacizumab plus chemotherapy and 9.8 months for chemotherapy alone (p = 0.0062). A possible resistance mechanism to anti-angiogenic agents may include increased levels of circulating VEGFA levels, able to interact once again with VEGFR. The BEBYP study had a similar design but was prematurely stopped after 185 randomized patients in consideration of the results of the ML18147 trial [35]. The median PFS was 5.0 months in the chemotherapy group and 6.8 months in the bevacizumab group (p = 0.010). An improved OS was also observed in the bevacizumab arm (adjusted HR = 0.77; 95% CI 0.56–1.06; p = 0.043). To conclude, the ESMO recommendations state that patients who received bevacizumab first line should be considered for treatment with bevacizumab as a post-discontinuation strategy [17].
3 Ramucirumab
Ramucirumab is a fully human IgG1 monoclonal antibody targeting VEGFR-2, considered as the primary VEGF family receptor driving angiogenesis [36]. As a consequence, the blockade of VEGFR-2 induced by ramucirumab prevents the interaction of all VEGF ligands and receptor activation. After an interesting activity profile and acceptable tolerance were shown in a phase I study [37], ramucirumab was tested in combination with FOLFIRI vs. placebo as second-line treatment in mCRC patients in a large phase III study (RAISE) [38]. Eligible patients had disease progression during or within 6 months of the last dose of first-line combination therapy with bevacizumab and FOLFOX. In the 1072 enrolled patients (536 in each arm), median OS was significantly improved with ramucirumab compared with placebo (13.3 months vs. 11.7 months, HR 0.84, p = 0.0219). Median PFS was increased in the ramucirumab group (5.7 months vs. 4.5 months, HR 0.79, p = 0.0005). Interestingly, this advantage persisted in patients with fast-growing tumors (time to progression after start of first-line treatment < 6 months), who were not included in the TML study, in which bevacizumab was evaluated in the same setting as ramucirumab. Main grade 3 or worse adverse events were neutropenia (38% vs. 23%, with febrile neutropenia incidence of 3% vs. 2%), hypertension (11% vs. 3%), diarrhea (11% vs. 10%), and fatigue (12% vs. 8%). In a recent meta-analysis including 4996 patients treated with ramucirumab, arterial/venous thromboembolic events and high-grade bleeding were not significantly increased compared with placebo [39]. On the other hand, a higher percentage of hypertension, proteinuria, low-grade bleeding, GI perforation, infusion-related reaction, and wound-healing complications were confirmed in the ramucirumab group.
Contrary to the RAS status with anti-EGFR antibodies, robust predictive biomarkers of efficacy are lacking with anti-angiogenic therapies. Recently, the RAISE biomarker program post hoc analysis found that the median OS in the ramucirumab arm compared with the placebo arm showed an improvement of 2.4 months in the high VEGF-D subgroup (13.9 months vs. 11.5 months, respectively) [40]. PFS results were consistent with OS, but no trends were evident with the other antiangiogenic candidate biomarkers (VEGF-C, sVEGFR-1, sVEGFR-2, sVEGFR-3 in plasma, and VEGFR-2 in tumor tissue). The RAISE trial supports the hypothesis that inhibition of tumor angiogenesis beyond initial disease progression is an effective treatment strategy. However, in a phase II randomized study, combining ramucirumab or icrucumab (anti-VEGFR-1) with FOLFOX did not achieve the predetermined improvement in PFS in patients with mCRC after disease progression on first-line therapy with FOLFIRI [41]. The ESMO guidelines consider ramucirumab in combination with FOLFIRI as a second-line treatment in patients who received bevacizumab first line, especially in those with fast-growing tumors [17].
4 Aflibercept
Aflibercept is an anti-angiogenic agent and its mechanism of action consists of binding to the endogenous circulating VEGF molecules and to the placental growth factor (PIGF). It is a recombinant fusion protein of the VEGF-binding parts of the extracellular domains of human VEGF receptors 1 and 2, and the Fc portion of the human IgG1 immunoglobulin. It therefore inhibits the activity of VEGF A and B and the formation of new blood vessels within the tumor [42]. By inhibiting the formation of new blood vessels, tumor growth and proliferation are compromised as a result of nutrient deprivation, and its proliferation and invasion is halted.
Aflibercept was approved for the treatment of metastatic colorectal cancer based on the VELOUR study, a phase III randomized double-blind placebo-controlled global multicenter trial, in patients who were resistant to or had progressed following an oxaliplatin-containing regimen, with or without prior bevacizumab [43]. In this trial, 1226 patients were randomized at a 1:1 ratio to receive either aflibercept 4 mg/kg intravenously or placebo, in combination with FOLFIRI. Patients were treated until disease progression or unacceptable toxicity, primary endpoint was OS and secondary endpoints were PFS and ORR. The addition of aflibercept to FOLFIRI significantly improved OS as compared to placebo and the median OS was 13.5 months vs. 12.1 months (HR 0.82, 95% CI 0.71–0.94, p = 0.003). PFS was also significantly improved (HR 0.76, 95% CI 0.66–0.87, p < 0.001). The improvement of survival was consistent across subgroups, including bevacizumab-pretreated patients. Aflibercept was generally well tolerated and the reported adverse effects were the usual characteristic ones related to other anti-VEGF agents as well as an increase in some chemotherapy-related toxicities.
There are currently several, mostly phase II, clinical trials evaluating the effect of aflibercept first line in locally advanced or mCRC in different combinations with chemotherapy ongoing, among which are two trials with FOLFIRI (NCT02181556 and NCT02624726), one with LV5FU2 (NCT02384759), and another with oxaliplatine/fluoropyrimidine combinations (NCT01802684). There is also a phase II trial evaluating the impact of a personalized marker-driven (based on a cytokines/angiogenic factor profile) treatment approach using aflibercept with FOLFOX after first-line treatment with FOLFOX-bevacizumab (NCT02331927), a phase I study of aflibercept in combination with pembrolizumab for advanced solid tumors (NCT02298959), and two phase II trials with aflibercept in combination with FOLFOX for advanced rectal cancer (NCT02340949, NCT03043729).
5 Regorafenib
Regorafenib is an orally bioavailable multikinase inhibitor targeting several different protein kinases that are involved in important steps of tumor growth and proliferation. Its anti-angiogenic activity is due to its dual targeted VEGFR2-TIE2 tyrosine kinase inhibition. The agent also targets oncogenic factors (KIT, RET, RAF1, B-RAF, and B-RAF-V600E) and acts on the tumor microenvironment and stroma by targeting platelet-derived growth factor receptor and fibroblast growth factor [44]. Regorafenib has demonstrated anti-angiogenic, anti-proliferative, and pro-apoptotic effects in patient-derived murine models of gastric cancer [45].
In the phase III randomized placebo-controlled global multicenter trial (CORRECT), 760 patients with mCRC were randomized to receive oral regorafenib or placebo plus best supportive care [46]. All patients should have progressed within 3 months after several lines of standard treatments, including chemotherapy, bevacizumab, cetuximab, or panitumumab. Regorafenib significantly improved OS compared with placebo (6.4 months vs. 5.0 months, HR 0.77, 95% CI 0.64–0.94, p < 0.005). PFS was also significantly improved (HR 0.45, 95% CI 0.42–0.58, p < 0.001). Interestingly, the survival benefit was observed across all subgroups irrespective of KRAS status. The major adverse events were hand and foot skin reaction, fatigue, diarrhea, hypertension, and rash/desquamation.
Two other phase III studies (CONSIGN and CONCUR) demonstrated a survival benefit. The CONSIGN trial was a large prospective, open-label, single-arm, global multicenter trial conducted at 188 sites in 25 countries for patients with mCRC who progressed after standard therapies [47]. Its primary endpoint was safety. After analysis of data from 2864 patients who received regorafenib, the safety profile was consistent with data from the CORRECT trial. PFS was in the range of that previously reported and comparable across KRAS wild-type and mutant patient groups. CONCUR was another randomized, double-blind, placebo-controlled, phase III trial that compared regorafenib and placebo in Asian patients with previously treated mCRC [48]. Two hundred and forty-three patients were enrolled, and after a median follow-up of 7.4 months, OS was significantly improved with regorafenib (HR 0.55, 95% CI 0.40–0.77, p < 0.001). Adverse events were generally consistent with the known safety profile of regorafenib.
When prescribing regorafenib, physicians may have to face toxicity concerns, especially fatigue, hand-foot syndrome, abdominal pain, or hypertension, in heavily pre-treated patients. In the randomized phase II ReDOS study, a weekly dose escalation of regorafenib from 80 mg to 160 mg/day (Arm A: 80 mg for 1 week, escalation to 120 mg at week 2, and final escalation to 160 mg at week 3) was compared with standard dosing (Arm B: 160 mg/day immediately) [49]. The primary endpoint was the proportion of patients who completed two cycles of treatment and initiated the third in Arm A (n = 54) vs. Arm B (n = 62). Forty-three percent of patients in Arm A initiated the third cycle vs. only 25% of patients in Arm B (one-sided p value 0.028). Median OS was improved in Arm A vs. Arm B (9.0 months vs. 5.9 months; p = 0.094), whereas median PFS was similar. Overall rates of grade 3/4 toxicity were more favorable for Arm A vs. Arm B (hand-foot syndrome 15% vs. 16%, hypertension 7% vs. 15%, and fatigue 13% vs. 18%). Multiple quality-of-life parameters were improved in arm A vs. B primarily at week 2 of the first cycle. This dose-escalation strategy with regorafenib must be confirmed in further studies, but it is considered as a new standard for many prescribers.
Recently, a randomized phase II trial (REVERCE) tried to find the optimal treatment sequence in 101 KRAS exon 2 wild-type mCRC patients, after failure of fluoropyrimidine, oxaliplatin, and irinotecan [50]. Patients were randomized to receive sequential treatment with regorafenib followed by cetuximab ± irinotecan (R–C arm) or the reverse sequence (C ± irinotecan followed by R; C–R arm). Bevacizumab had been previously administered in 96% and 98% of patients in R–C and C–R, respectively. Median OS in R–C and C–R were 17.4 and 11.6 months, respectively (stratified log rank, p = 0.0293), with an HR of 0.61 (95% CI 0.39–0.96). Additional studies are warranted to confirm these results but once again, it could be explained by continuous anti-angiogenic pressure.
There are many ongoing clinical trials with regorafenib, including a phase II trial assessing potential biomarkers (NCT01949194) and a phase II as second-line treatment in RAS-mutant CRC (NCT02619435). Another prospective translational phase II trial is investigating molecular predictors of resistance and response to regorafenib in RAS-mutant mCRC (NCT03010722).
6 Other Small-Molecule Tyrosine Kinase Inhibitors
Newly developed VEGFR inhibitors are being evaluated in several trials. Firstly, nintedanib is an oral agent that inhibits VEGFR 1–3, platelet-derived growth factor receptors (PDGFR α and β), and fibroblast growth factor receptors (FGFR 1–3). Nintedanib was reported to be effective for non-small-cell lung carcinoma, but not for CRC [51, 52]. The LUME-Colon 1 trial randomized 768 mCRC patients after failure of standard therapies into nintedanib plus best supportive care group (n = 386) and best supportive care group only (n = 382) [52]. Nintedanib led to statistically significant improvement in PFS; median PFS in the nintedanib group and placebo group were 1.51 months and 1.38 months, respectively (HR = 0.58, p < 0.0001). However, there was no difference in OS; median OS in nintedanib group and placebo group was 6.44 months and 6.05 months, respectively (HR = 1.01, p = 0.87). This result suggests that using nintedanib in a clinical setting might be difficult. Secondly, fruquintinib is a highly selective small molecule inhibitor for VEGFR-1–3, and several preclinical studies demonstrated its efficacy [53, 54]. Phase I trials demonstrated safety of fruquintinib, based on which a phase II trial was performed [55,56,57]. Seventy-one patients treated with more than second-line therapy were randomized to fruquintinib (n = 47) or placebo (n = 24) [56]. PFS was significantly improved in the fruquintinib group compared with the placebo group; median PFS in the fruquintinib group and placebo group were 4.73 months and 0.99 months, respectively (HR = 0.30, 95% CI 0.15–0.59, p < 0.001). The median OS was 7.72 vs. 5.52 months (HR 0.71, 95% CI 0.38–1.34) [56]. Thus, a randomized phase III study with fruquintinib is expected.
7 Conclusions
Over the past 15 years, anti-angiogenic therapies have significantly improved the prognosis of mCRC patients. Bevacizumab clearly demonstrated efficacy in the first-line setting in association with doublet chemotherapy (FOLFOX or FOLFIRI) or capecitabine alone in elderly patients. Bevacizumab was also associated with high ORR when combined with triplet chemotherapy (FOLFOXIRI) in patients with potentially resectable liver metastases. After disease progression with first-line chemotherapy combined with bevacizumab, several prospective studies confirmed the concept of “continuous anti-angiogenic blocking” with bevacizumab, aflibercept, or ramucirumab. This approach may be applied in patients who progressed after two or more lines of standard treatments, as demonstrated with regorafenib, an orally bioavailable multi-kinase inhibitor. Indirect arguments for continuous anti-angiogenic blocking were provided by strategic studies. In the French multicenter, prospective, open randomized PRODIGE 18 trial, wild-type (wt) KRAS mCRC patients who progressed after first-line therapy with bevacizumab and chemotherapy were randomized to receive bevacizumab or cetuximab in combination with crossover chemotherapy [58]. Continuation beyond progression with bevacizumab was associated with a numerically higher but not statistically significant median PFS and OS compared to cetuximab plus chemotherapy. The Italian phase III COMETS trial also suggested that anti-EGFR therapy would not be the best choice of targeted therapy after failure with chemotherapy plus bevacizumab in wtKRAS mCRC [59]. Results were similar in the randomized phase II SPIRITT study [60]. As a consequence, the ESMO recommendations state that patients who received bevacizumab first line should be considered for treatment with bevacizumab or ramucirumab post-continuation strategy [17].
Another issue concerns the identification of predictive biomarkers of efficacy. Angiogenesis is a continuous and dynamic process, and some pre-clinical and clinical studies showed a shift in balance in cytokines and angiogenic factors after anti-angiogenic exposure. For example, recruitment of basic fibroblast growth factor, HGF, PIGF, stromal-derived factor-1, and macrophage chemoattractant protein-3 is significantly increased in mCRC patients treated with FOLFIRI-bevacizumab in the first-line setting [61]. The rise in alternate pro-angiogenic actors may represent a mechanism of resistance, suggesting that a different tumor angiogenesis inhibitor could be prescribed in the second-line setting. However, robust clinical trials assessing this concept are missing and therefore the decision is essentially based on objective response, toxicity profile, and patients’ preference.
Another contemporary issue is the place of biosimilars. Patents protecting bevacizumab in the USA and Europe are expected to expire soon, opening the way to the approval of several biosimilars. The US Food and Drug Administration (FDA) approved the VEGF inhibitor bevacizumab-awwb (MVASI®, Amgen/Allergan) in September 2017 [62], followed by the EMA in January 2018. We can expect better access to bevacizumab at a global level, with lower health costs. After the approval of filgrastim biosimilars in Europe, the average price per treatment-day dropped by 32% [63]. A biosimilar is a biologic that is deemed to be highly similar to a licensed originator product, with no clinically meaningful differences in safety, purity, or potency, following a rigorous comparison exercise. When a potential biosimilar demonstrates a high degree of similarity to the originator, it can be approved for indications initially not studied during the clinical study. This concept, known as extrapolation, was used for bevacizumab because most of the studies were conducted in lung cancer patients [64], although two potential bevacizumab biosimilars (BEVZ92 and BI 695502) are being studied in patients with mCRC (NCT02069704 and NCT02776683, respectively). In a recent survey, almost 50% of physicians reported they “definitely” or “probably” would prescribe a bevacizumab biosimilar if available, underlying potential barriers and required efforts to implement this new therapeutic approach [65].
Finally, orally available multi-receptor TKIs with activity against several angiogenesis effectors are currently intensively tested in mCRC, with disappointing results in most of the cases, except for famitinib, fruquintinib, and nintedanib, which are in later stages of development.
Targeting angiogenesis provided convincing evidence for improving survival in mCRC patients at different moments of their disease journey, but we need further investigations to identify the optimal therapeutic sequence, predictive biomarkers of efficacy, the place of biosimilars, and new clinically meaningful anti-angiogenic drugs.
References
Siegel RL, Fedewa SA, Anderson WF, Miller KD, Ma J, Rosenberg PS, et al. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. Journal of the National Cancer Institute. 2017;109(8) (Epub 2017/04/05).
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30.
Kerr J, Anderson C, Lippman SM. Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence. Lancet Oncol. 2017;18(8):e457–71 (Epub 2017/08/02).
Brenner H, Kloor M, Pox CP. Colorectal cancer. Lancet. 2014;383(9927):1490–502 (Epub 2013/11/15).
Guinney J, Dienstmann R, Wang X, de Reynies A, Schlicker A, Soneson C, et al. The consensus molecular subtypes of colorectal cancer. Nat Med. 2015;21(11):1350–6 (Epub 2015/10/13).
Liu Y, Sethi NS, Hinoue T, Schneider BG, Cherniack AD, Sanchez-Vega F, et al. Comparative molecular analysis of gastrointestinal adenocarcinomas. Cancer Cell. 2018;33(4):721–735 e8 (Epub 2018/04/07).
Zubeldia IG, Bleau AM, Redrado M, Serrano D, Agliano A, Gil-Puig C, et al. Epithelial to mesenchymal transition and cancer stem cell phenotypes leading to liver metastasis are abrogated by the novel TGFbeta1-targeting peptides P17 and P144. Exp Cell Res. 2013;319(3):12–22 (Epub 2012/11/17).
Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med. 1971;285(21):1182–6 (Epub 1971/11/18).
Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–42 (Epub 2004/06/04).
Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr Rev. 1997;18(1):4–25 (Epub 1997/02/01).
Prat A, Casado E, Cortes J. New approaches in angiogenic targeting for colorectal cancer. World J Gastroenterol. 2007;13(44):5857–66 (Epub 2007/11/09).
Divella R, Daniele A, De Luca R, Simone M, Naglieri E, Savino E, et al. Circulating levels of VEGF and CXCL1 are predictive of metastatic organotropismin in patients with colorectal cancer. Anticancer Res. 2017;37(9):4867–71 (Epub 2017/09/06).
Liu Z, Zhang Y, Niu Y, Li K, Liu X, Chen H, et al. A systematic review and meta-analysis of diagnostic and prognostic serum biomarkers of colorectal cancer. PLoS One. 2014;9(8):e103910 (Epub 2014/08/12).
Ferrara N, Hillan KJ, Gerber HP, Novotny W. Discovery and development of bevacizumab, an anti-VEGF antibody for treating cancer. Nat Rev Drug Discov. 2004;3(5):391–400 (Epub 2004/05/12).
Saltz LB, Clarke S, Diaz-Rubio E, Scheithauer W, Figer A, Wong R, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26(12):2013–9 (Epub 2008/04/19).
Passardi A, Nanni O, Tassinari D, Turci D, Cavanna L, Fontana A, et al. Effectiveness of bevacizumab added to standard chemotherapy in metastatic colorectal cancer: final results for first-line treatment from the ITACa randomized clinical trial. Ann Oncol. 2015;26(6):1201–7 (Epub 2015/03/05).
Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27(8):1386–422 (Epub 2016/07/07).
Jang HJ, Kim BJ, Kim JH, Kim HS. The addition of bevacizumab in the first-line treatment for metastatic colorectal cancer: an updated meta-analysis of randomized trials. Oncotarget. 2017;8(42):73009–16 (Epub 2017/10/27).
Loupakis F, Cremolini C, Masi G, Lonardi S, Zagonel V, Salvatore L, et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med. 2014;371(17):1609–18 (Epub 2014/10/23).
Gruenberger T, Bridgewater J, Chau I, Garcia Alfonso P, Rivoire M, Mudan S, et al. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: the OLIVIA multinational randomised phase II trial. Ann Oncol. 2015;26(4):702–8 (Epub 2014/12/30).
Tomasello G, Petrelli F, Ghidini M, Russo A, Passalacqua R, Barni S. FOLFOXIRI plus bevacizumab as conversion therapy for patients with initially unresectable metastatic colorectal cancer: a systematic review and pooled analysis. JAMA Oncol. 2017;3(7):e170278 (Epub 2017/05/26).
Cunningham D, Lang I, Marcuello E, Lorusso V, Ocvirk J, Shin DB, et al. Bevacizumab plus capecitabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX): an open-label, randomised phase 3 trial. Lancet Oncol. 2013;14(11):1077–85 (Epub 2013/09/14).
Aparicio T, Bouche O, Taieb J, Maillard E, Kirscher S, Etienne PL, et al. Bevacizumab + chemotherapy versus chemotherapy alone in elderly patients with untreated metastatic colorectal cancer: a randomized phase II trial-PRODIGE 20 study results. Ann Oncol. 2018;29:133–8 (Epub 2018/05/03).
de Gramont A, Van Cutsem E, Schmoll HJ, Tabernero J, Clarke S, Moore MJ, et al. Bevacizumab plus oxaliplatin-based chemotherapy as adjuvant treatment for colon cancer (AVANT): a phase 3 randomised controlled trial. Lancet Oncol. 2012;13(12):1225–33 (Epub 2012/11/22).
Allegra CJ, Yothers G, O’Connell MJ, Sharif S, Petrelli NJ, Colangelo LH, et al. Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: results of NSABP protocol C-08. J Clin Oncol. 2011;29(1):11–6 (Epub 2010/10/14).
Simkens LH, van Tinteren H, May A, ten Tije AJ, Creemers GJ, Loosveld OJ, et al. Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): a phase 3 randomised controlled trial of the Dutch Colorectal Cancer Group. Lancet. 2015;385(9980):1843–52 (Epub 2015/04/12).
Hegewisch-Becker S, Graeven U, Lerchenmuller CA, Killing B, Depenbusch R, Steffens CC, et al. Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for patients with metastatic colorectal cancer (AIO 0207): a randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol. 2015;16(13):1355–69 (Epub 2015/09/13).
Goey KKH, Elias SG, van Tinteren H, Lacle MM, Willems SM, Offerhaus GJA, et al. Maintenance treatment with capecitabine and bevacizumab versus observation in metastatic colorectal cancer: updated results and molecular subgroup analyses of the phase 3 CAIRO3 study. Ann Oncol. 2017;28(9):2128–34 (Epub 2017/09/16).
Goey KKH, Elias SG, Hinke A, Oijen MGH, Punt CJA, Hegewisch-Becker S, et al. Clinicopathological factors influencing outcome in metastatic colorectal cancer patients treated with fluoropyrimidine and bevacizumab maintenance treatment vs. observation: an individual patient data meta-analysis of two phase 3 trials. Br J Cancer. 2017;117(12):1768–76 (Epub 2017/11/11).
Giantonio BJ, Catalano PJ, Meropol NJ, O’Dwyer PJ, Mitchell EP, Alberts SR, et al. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. J Clin Oncol. 2007;25(12):1539–44 (Epub 2007/04/20).
Bergers G, Benjamin LE. Tumorigenesis and the angiogenic switch. Nat Rev Cancer. 2003;3(6):401–10 (Epub 2003/06/05).
Grothey A, Sugrue MM, Purdie DM, Dong W, Sargent D, Hedrick E, et al. Bevacizumab beyond first progression is associated with prolonged overall survival in metastatic colorectal cancer: results from a large observational cohort study (BRiTE). J Clin Oncol. 2008;26(33):5326–34 (Epub 2008/10/16).
Bendell JC, Bekaii-Saab TS, Cohn AL, Hurwitz HI, Kozloff M, Tezcan H, et al. Treatment patterns and clinical outcomes in patients with metastatic colorectal cancer initially treated with FOLFOX-bevacizumab or FOLFIRI-bevacizumab: results from ARIES, a bevacizumab observational cohort study. Oncologist. 2012;17(12):1486–95 (Epub 2012/09/28).
Bennouna J, Sastre J, Arnold D, Osterlund P, Greil R, Van Cutsem E, et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trial. Lancet Oncol. 2013;14(1):29–37 (Epub 2012/11/22).
Masi G, Salvatore L, Boni L, Loupakis F, Cremolini C, Fornaro L, et al. Continuation or reintroduction of bevacizumab beyond progression to first-line therapy in metastatic colorectal cancer: final results of the randomized BEBYP trial. Ann Oncol. 2015;26(4):724–30 (Epub 2015/01/21).
Fontanella C, Ongaro E, Bolzonello S, Guardascione M, Fasola G, Aprile G. Clinical advances in the development of novel VEGFR2 inhibitors. Ann Transl Med. 2014;2(12):123 (Epub 2015/01/09).
Spratlin JL, Cohen RB, Eadens M, Gore L, Camidge DR, Diab S, et al. Phase I pharmacologic and biologic study of ramucirumab (IMC-1121B), a fully human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2. J Clin Oncol. 2010;28(5):780–7 (Epub 2010/01/06).
Tabernero J, Yoshino T, Cohn AL, Obermannova R, Bodoky G, Garcia-Carbonero R, et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015;16(5):499–508 (Epub 2015/04/17).
Arnold D, Fuchs CS, Tabernero J, Ohtsu A, Zhu AX, Garon EB, et al. Meta-analysis of individual patient safety data from six randomized, placebo-controlled trials with the antiangiogenic VEGFR2-binding monoclonal antibody ramucirumab. Ann Oncol. 2017;28(12):2932–42 (Epub 2017/09/28).
Tabernero J, Hozak RR, Yoshino T, Cohn AL, Obermannova R, Bodoky G, et al. Analysis of angiogenesis biomarkers for ramucirumab efficacy in patients with metastatic colorectal cancer from RAISE, a global, randomized, double-blind, phase III study. Ann Oncol. 2018;29:602–9 (Epub 2017/12/12).
Moore M, Gill S, Asmis T, Berry S, Burkes R, Zbuk K, et al. Randomized phase II study of modified FOLFOX-6 in combination with ramucirumab or icrucumab as second-line therapy in patients with metastatic colorectal cancer after disease progression on first-line irinotecan-based therapy. Ann Oncol. 2016;27(12):2216–24 (Epub 2016/10/14).
Bridgewater Ns-aUSL. Zaltrap (ziv-aflibercept)—drug development technology. ZALTRAP Prescribing Information; 2016. http://www.drugdevelopment-technology.com. Accessed 10 Apr 2018.
Van Cutsem E, Tabernero J, Lakomy R, Prenen H, Prausova J, Macarulla T, et al. Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J Clin Oncol. 2012;30(28):3499–506 (Epub 2012/09/06).
Wilhelm SM, Dumas J, Adnane L, Lynch M, Carter CA, Schutz G, et al. Regorafenib (BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int J Cancer. 2011;129(1):245–55 (Epub 2010/12/21).
Huynh H, Ong R, Zopf D. Antitumor activity of the multikinase inhibitor regorafenib in patient-derived xenograft models of gastric cancer. J Exp Clin Cancer Res. 2015;34:132 (Epub 2015/10/31).
Grothey A, Van Cutsem E, Sobrero A, Siena S, Falcone A, Ychou M, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381(9863):303–12 (Epub 2012/11/28).
Van Cutsem ECF, Seitz J-F, et al. Results from the large, open-label phase 3b CONSIGN study of regorafenib in patients with previously treated metastatic colorectal cancer. Ann Oncol. 2015;26(suppl_4):LBA-05.
Li J, Qin S, Xu R, Yau TC, Ma B, Pan H, et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015;16(6):619–29 (Epub 2015/05/20).
Bekaii-Saab TSOF, Anderson DM, et al. Regorafenib dose optimization study (ReDOS): Randomized phase II trial to evaluate dosing strategies for regorafenib in refractory metastatic colorectal cancer (mCRC): an ACCRU Network study. J Clin Oncol. 2018;36(4_suppl):611.
Shitara KYT, Denda T, et al. Reverce: randomized phase II study of regorafenib followed by cetuximab versus the reverse sequence for metastatic colorectal cancer patients previously treated with fluoropyrimidine, oxaliplatin, and irinotecan. J Clin Oncol. 2018;36(4_suppl):557.
Reck M, Kaiser R, Mellemgaard A, Douillard JY, Orlov S, Krzakowski M, et al. Docetaxel plus nintedanib versus docetaxel plus placebo in patients with previously treated non-small-cell lung cancer (LUME-Lung 1): a phase 3, double-blind, randomised controlled trial. Lancet Oncol. 2014;15(2):143–55 (Epub 2014/01/15).
Van Cutsem E, Yoshino T, Lenz HJ, Lonardi S, Falcone A, Limon ML, et al. Nintedanib for the treatment of patients with refractory metastatic colorectal cancer (LUME-Colon 1): a phase III, international, randomized, placebo-controlled study. Ann Oncol. 2018;29(9):1955–63 (Epub 2018/07/17).
Sun Q, Zhou J, Zhang Z, Guo M, Liang J, Zhou F, et al. Discovery of fruquintinib, a potent and highly selective small molecule inhibitor of VEGFR 1, 2, 3 tyrosine kinases for cancer therapy. Cancer Biol Ther. 2014;15(12):1635–45 (Epub 2014/12/09).
Gu Y, Wang J, Li K, Zhang L, Ren H, Guo L, et al. Preclinical pharmacokinetics and disposition of a novel selective VEGFR inhibitor fruquintinib (HMPL-013) and the prediction of its human pharmacokinetics. Cancer Chemother Pharmacol. 2014;74(1):95–115 (Epub 2014/05/13).
Li JCJ, Xu R-H, et al. A phase 1b study of VEGFR inhibitor fruquintinib in patients with pretreated advanced colorectal cancer. J Clin Oncol. 2014;32(15_suppl):3548.
Xu RH, Li J, Bai Y, Xu J, Liu T, Shen L, et al. Safety and efficacy of fruquintinib in patients with previously treated metastatic colorectal cancer: a phase Ib study and a randomized double-blind phase II study. J Hematol Oncol. 2017;10(1):22 (Epub 2017/01/21).
Cao J, Zhang J, Peng W, Chen Z, Fan S, Su W, et al. A Phase I study of safety and pharmacokinetics of fruquintinib, a novel selective inhibitor of vascular endothelial growth factor receptor-1, -2, and -3 tyrosine kinases in Chinese patients with advanced solid tumors. Cancer Chemother Pharmacol. 2016;78(2):259–69 (Epub 2016/06/15).
Hiret SBC, Bertaut A, et al. Bevacizumab or cetuximab plus chemotherapy after progression with bevacizumab plus chemotherapy in patients with wtKRAS metastatic colorectal cancer: a randomized phase II study (Prodige 18–UNICANCER GI). J Clin Oncol. 2016;34(15_suppl):3514.
Cascinu S, Rosati G, Nasti G, Lonardi S, Zaniboni A, Marchetti P, et al. Treatment sequence with either irinotecan/cetuximab followed by FOLFOX-4 or the reverse strategy in metastatic colorectal cancer patients progressing after first-line FOLFIRI/bevacizumab: an Italian Group for the Study of Gastrointestinal Cancer phase III, randomised trial comparing two sequences of therapy in colorectal metastatic patients. Eur J Cancer. 2017;83:106–15 (Epub 2017/07/25).
Hecht JR, Cohn A, Dakhil S, Saleh M, Piperdi B, Cline-Burkhardt M, et al. SPIRITT: a randomized, multicenter, phase II study of panitumumab with FOLFIRI and bevacizumab with FOLFIRI as second-line treatment in patients with unresectable wild type KRAS metastatic colorectal cancer. Clin Colorectal Cancer. 2015;14(2):72–80 (Epub 2015/05/20).
Kopetz S, Hoff PM, Morris JS, Wolff RA, Eng C, Glover KY, et al. Phase II trial of infusional fluorouracil, irinotecan, and bevacizumab for metastatic colorectal cancer: efficacy and circulating angiogenic biomarkers associated with therapeutic resistance. J Clin Oncol. 2010;28(3):453–9 (Epub 2009/12/17).
FDA approves first biosimilar to treat cancer. Cancer Discov. 2017;7(11):1206 (Epub 2017/10/07).
IMS Health. The impact of biosimilar competition. 2016. http://ec.europa.eu/DocsRoom/documents/17325/attachments/1/translations/en/renditions/native42. Accessed 10 Apr 2018.
Thatcher NTM, Paz-Ares L, et al. Randomized, double-blind, phase 3 study evaluating efficacy and safety of ABP 215 compared with bevacizumab in patients with non-squamous NSCLC. J Clin Oncol. 2016;34(15_suppl):9095.
Monk BJ, Lammers PE, Cartwright T, Jacobs I. Barriers to the access of bevacizumab in patients with solid tumors and the potential impact of biosimilars: a physician survey. Pharmaceuticals (Basel). 2017;10(1) (Epub 2017/01/31).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No external funding was used in the preparation of this manuscript.
Conflict of interest
Anthony Lopez has received research funding from Roche, has served as consultant for Amgen, received lecture fees from Vifor Pharma, and received travel accommodation expenses (not for this work) from Abbvie, Amgen, MSD, Vifor-Pharma. Jaffer A. Ajani has received honoraria from Lilly, Bayer, Novartis, Five Prime Therapeutics, Taiho Pharmaceutical, Genentech, and Roche, received research funding from Novartis, Bristol-Myers Squibb, Taiho Pharmaceutical, Roche/Genentech, MedImmune, Amgen, Lilly/ImClone, Merck, Delta-Fly Pharma, Gilead Sciences, and Takeda, and received travel accommodation expenses (not for this work) from Novartis, Bayer, and Five Prime Therapeutics. Kazuto Harada, Maria Vasilakopoulou, and Namita Shanbhag declare that they have no conflicts of interest that might be relevant to the contents of this manuscript.
Rights and permissions
About this article

Cite this article
Lopez, A., Harada, K., Vasilakopoulou, M. et al. Targeting Angiogenesis in Colorectal Carcinoma. Drugs 79, 63–74 (2019). https://doi.org/10.1007/s40265-018-1037-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-018-1037-9