
Abstract
Introduction
Herbal medicines are used worldwide and with an increasing popularity in Western countries. Although often perceived as ‘naturally safe’, herbals may cause severe adverse drug reactions (ADRs), with immediate allergic reactions being particularly life threatening.
Objectives
The aim of this study was to analyse immediate allergy-like ADRs to herbals documented in VigiBase®, the WHO international pharmacovigilance database.
Methods
The documentation of all suspected ADRs in association with herbal exposure reported to VigiBase® from 1969 to August 2014 was retrieved. Among all reports in which WHO-ART reaction terms were indicative of acute allergic reactions, those classified as ‘suspect’ with a documented causality assessment and latency time of ≤1 day were selected. For the most frequent specific herbal–ADR combinations, the information component (IC) as a measure of disproportionality based on Bayesian statistics was calculated.
Results
We identified 757 reports out of 1039 ADRs. Products with mixed herbals (36.0 %) as well as those administered orally (63.2 %) were predominant. The most frequent reactions were urticaria and rash (49.2 %). Anaphylactic reactions accounted for 9.5 %. Disproportionally frequent reporting of mouth edema (IC = 1.81) and anaphylactic reactions (IC = 1.24) to Phleum pretense were noted.
Conclusion
Our findings indicate that herbal medicines for oral use carry a risk of causing immediate allergy-like ADRs. Studies using the Vigibase® database can identify specific combinations of particular herbs and adverse reactions. Healthcare professionals and patients should be aware of these risks and report any serious adverse experiences.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
While herbal medicines for oral use are generally regarded as safe, international pharmacovigilance data indicate that many such products carry a risk of causing acute allergy-like adverse reactions. |
The recognition of the possibility of such reactions with the use of specific products is needed for timely diagnosis as well as for prevention of problems. |
1 Introduction
There is an increased prevalence in the use of herbal medicines among the adult population in many Western countries [1–3]. The most recent 2012 US National Health Interview Survey showed that 18 % of adults used natural products including at least one herbal medicine during the past 12 months [3]. Herbal medicines are generally considered harmless since they are natural and thus the general public is unaware that Complementary and Alternative Medicines (CAM) are not tested by regulatory agencies for their safety and efficacy [4, 5]. In most countries, herbal medicines are defined as dietary supplements and as such do not have to meet pre- and postmarketing drug policy regulations [6]. Nevertheless, the use of certain herbal medicines has been associated with the occurrence of severe adverse reactions as a result of the complex chemistry of herbals as well as through their inappropriate use and a lack of quality control [7, 8]. In addition, patients may not disclose self-medication with herbal medicines to their healthcare professionals, who themselves may have limited information about potential adverse reactions and interactions with concomitantly used prescription drugs [9, 10].
In the absence of systematic and comprehensive safety evaluations of herbal medicines, spontaneous reporting systems of adverse drug reactions (ADRs) serve a major function in terms of worldwide safety surveillance and signal detection [11]. Although there have been many case reports of ADRs associated with herbals in the literature, the majority of reports are documented in large pharmacovigilance databases; thus, these valuable resources should be systematically analyzed for ADRs associated with herbals [8, 12, 13]. ADRs to herbals cover a wide range of manifestations that are typically mild and followed by full recovery. Nevertheless, immediate allergic reactions are also often potentially life threatening; thus, these effects represent the most clinically relevant adverse reactions to herbal medicines. Our study of the results of more than 40 years of international pharmacovigilance was conducted with the goal of investigating reporting patterns as well as basic characteristics of immediate allergic adverse reactions associated with herbal medicines.
2 Methods
2.1 Study Settings
The WHO Global Individual Case Safety Report database (VigiBase®), the largest international pharmacovigilance database of spontaneous ADR reports, was the source examined in our study. VigiBase® is maintained by the Uppsala Monitoring Centre (UMC) in association with the World Health Organization’s (WHO) international pharmacovigilance program. The UMC is an independent foundation and a center for international service and scientific research which currently collaborates with 122 member countries around the world in the collection and evaluation of spontaneous ADR reports [14]. These centers forward anonymized ADR reports received from various primary reporting sources to the UMC in a standardized format containing structured information on adverse events; that is, patients and drugs involved, including standardized semi-quantitative causality assessments [15].
Vigibase, the UMC’s database, currently contains over 11 million case reports (May, 2015). The WHO Adverse Drug Reaction Terminology (WHO-ART) and WHO Drug Dictionary/WHO Herbal Dictionary are used for the coding of clinical information in relation to drug therapy featuring the reported drugs [14]. MedDRA® terminology was introduced to VigiBase in 1994; automated algorithms that convert the codes form those two dictionaries in both directions [16].
Herbal medicine refers to herbs, herbal materials, herbal preparations as well as finished herbal medicines. Herbal medicines are assigned herbal anatomical-therapeutic-chemical (HATC) codes specifying their therapeutic use according to the Guidelines for Herbal ATC classification [17]. HATC classification aggregates herbal medicines according to their medical uses that have been found in the literature, but does not indicate that a given remedy has been proven effective or safe [14]. Herbal pharmacovigilance terminology is used in accordance with WHO guidelines [18].
2.2 Study Design and Selection of Cases
A flowchart of the study design and case selection process is presented in Fig. 1. The aim of our study was to focus on immediate allergic ADRs associated with herbals, as these are more often potentially life threatening and therefore highly relevant clinically. The level of documentation within VigiBase® is heterogeneous, thus it may be difficult to form an exact medical diagnosis based on the available information. With this limitation in mind, case selection criteria were defined through likely indicators of immediate allergic reactions.

Flowchart of study design and case selection process. ADR adverse drug reactions, UMC Uppsala Monitoring Centre, WHO-ART World Health Organization Adverse Reactions Terminology
Because VigiBase® does not allow for a validation of type 1 immediate hypersensitivity reactions according to comprehensive clinical diagnostic criteria, the cases included have been judiciously referred to as ‘allergy-like immediate reactions’ in our study. For inclusion in the study population, the following inclusion criteria were used: (1) exposure to manually validated herbal medicines, a category classified by the primary reporter as ‘suspect’ with regard to the reported ADRs; (2) a documented causality assessment of ‘possible,’ ‘probable’ or ‘certain’ between a herbal product and ADRs; (3) a documented latency time of no more than 1 day from herbal exposure to ADR onset; (4) manual selection of WHO-ART preferred terms indicating an ADR that is a likely symptom of an immediate hypersensitivity reaction.
In contrast, reaction terms that are compatible with but have a low specificity for immediate allergic reactions such as cough, dyspnea, larynx pain, gastrointestinal symptoms or pruritus were on their own not considered sufficient for inclusion. Furthermore, ADRs associated with the HATC term ‘herbal pollen not otherwise specified’ were excluded from the main analysis because these are likely to refer to desensitization vaccines for the treatment of pollen allergies (ADRs that may have a distinct special relationship to the indication for the suspected herbal medicines). Of note, this HATC term does not include Phleum pratense (Timothy grass), although it is also used for desensitization. It is of interest that anaphylaxis has not been reported in clinical trials and reviews on Phleum pretense [19, 20], and we therefore explored such a possible association in the main analysis. WHO-ART terms were further divided into asthma-like and allergy-like reaction groups. Asthma-like reactions were defined by the preferred WHO-ART terms ‘asthma,’ ‘stridor’ or ‘bronchospasm.’ All remaining WHO-ART terms with high specificity for immediate allergic reactions constituted the applicable allergy-like reaction group.
2.3 Statistical Analysis
Descriptive statistics was used to analyze the characteristics of case reports. Unexpected ADRs to herbals were quantitatively analyzed using a measure of disproportionality based on the shrinkage of observed-to-expected ratios expressed as the Information Component (IC) [21]. The IC is computed as the base 2 logarithm of an (O + 0.5)/(E + 0.5) ratio with an observed number of events (O) and expected number of events (E) of reports on the drug–ADR combination. E is given by (N A × N D)/N, where N A is the number of all reports on the ADR, N D is the number of all reports on the drug, and N is the number of all reports. Credibility intervals for the IC are obtained via Gamma distribution, with IC α denoting the α percentile of the posterior distribution for the IC. A drug–ADR combination was considered disproportionally reported when IC025 >0 for the whole database. IC025 denotes the lower limits of 95 % credibility intervals for the IC [21, 22]. For the IC analysis we used the dataset of all reports that met our inclusion criteria and calculated the IC for all specific combinations that occurred with a frequency of 10 or more. Data management and analyses were performed using STATA Version 13.1 (StataCorp LP, College Station, TX, USA).
3 Results
The initial dataset extracted from VigiBase® comprised 26,909 unique ADR reports received between 1969 and August 2014 following exposure to herbal medicines. After the application of exclusion criteria, 757 unique reports remained containing 1039 ADRs (i.e., more than one reaction term could be reported per case) related to herbal medicines.
3.1 Case Report Characteristics
The characteristics of the 757 reports are presented in Table 1. Women were overrepresented among included cases (68.6 %), and more than one third of the cases fell into the age category from 18 to 44 years. More than 50 % of all the included reports came from only three countries: Germany (22.3 %), Australia (14.9 %) and Thailand (11.2 %). The most frequent primary reporters were physicians (32.1 %), followed by hospitals (24.7 %) and pharmacists (14.1 %).
The chronology of the receipt of those reports is presented in Fig. 2. A pronounced increase in reporting frequency in recent years can be identified, a finding which reflects an overall trend in the database as well.

Number of reports of immediate allergy-like adverse reactions after the use of herbals per year (N = 757)
3.2 Immediate Allergy-Like Reactions
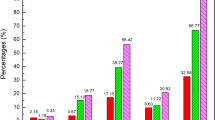
The characteristics of immediate allergy-like reactions to herbal medicines are presented in Table 2. The likelihood of a causal connection in the 1039 reported ADRs has been assessed as ‘possible,’ ‘probable,’ and ‘certain’ in 59.2, 32.2, and 8.6 %, respectively.
Asthma-like reactions accounted for only 4.8 % of all ADRs. The most commonly reported allergy-like immediate adverse reactions associated with herbals were ‘rash’ (16.2 %), ‘urticaria’ (15.3 %) and ‘rash erythematous’ (13.4 %). Anaphylactic and anaphylactoid reactions accounted altogether for 9.5 % of reported ADRs (anaphylactic reaction 4.5 %, anaphylactic shock 2.8 %, anaphylactoid reaction 2.2 %). Table 2 shows other serious ADRs such as bronchospasm and larynx edema.
Outcome was favorable (i.e., with recovery noted in 77.7 % of all ADRs) and no deaths were reported. It should be noted, however, that no information was available on the outcome for 9.2 %.
3.3 Suspect Herbals
Descriptions of specific herbals associated with the reported ADRs and their route of administration are presented in Table 3. Preparations that contained a mixture of several herbals were the suspected cause in 36 % of all ADRs and therefore by far were the most frequently reported, followed by the single herbals Phleum pratense (common name: Timothy grass, 6.5 %), Andrographis paniculata (several common names including Kalmegh, 5.0 %), Echinacea purpurea (3.8 %) and Ginkgo biloba (3.6 %).
Oral administrations accounted for almost two thirds of ADRs, followed by topical/cutaneous and sublingual administrations in 9.0 and 6.4 % of the cases, respectively.
3.4 Disproportionality Analysis
Calculations of IC values for all 16 specific herbal allergy-like reaction combinations that had been reported at least 10 times are presented in Table 4. Accordingly, significantly higher frequencies than expected by chance were found for Phleum pratense (Timothy grass) linked to edema of the mouth (IC = 1.81, 95 % CI 0.67–2.86) and to anaphylactic reactions (IC = 1.23, 95 % CI 0.03–2.33).
4 Discussion
Our study consists of an analysis of a series of 757 case reports indicative of allergy-like adverse reactions during the use of herbal medicines as recorded in the VigiBase® database of spontaneous ADR reports representing 42 countries since 1969. Our findings indicate a large number of different herbal medicines causing immediate allergy-like reactions in the population. Among all reports, mixed herbals, Phleum pratense and Andrographis paniculata were most frequently reported in association with ADRs. Phleum pratense has previously not been associated with anaphylaxis [19, 20], although two case reports of anaphylactic reaction after the first dose of grass pollen tablet containing Phleum pretense were reported [23]. It is therefore important new information that our study found reports of anaphylaxis related to Phleum pratense in VigiBase®, and that the disproportionality analysis even indicated a stronger association compared with other herbals, while evidence on its efficacy for immunotherapy is weak [19]. Andrographis paniculata is highly valued in Ayurvedic medicine and is typically used for the treatment of the common cold [24]. In relation to our work, previously reported findings from Thailand investigating the safety of Andrographis paniculata showed a similar range of hypersensitivity reactions ranging from skin reactions to anaphylaxis [25]. Case reports indicative of hypersensitivity to several other herbals most frequently reported in our study have also been previously published [26–31].
A high proportion of reports concerned women between the age of 18 and 44. The two most frequently reported manifestations of immediate allergy-like reactions were skin reactions and anaphylactic/anaphylactoid reactions, both of which were most frequently observed after oral administration. This finding is surprising since severe ADRs are rarely seen after the oral use of herbals. The occurrence of allergic reactions is rather more likely to be expected after cutaneous and mucosal exposure, which presents a known risk factor for sensitization to allergens [32]. It is reasonable to assume that rather easy to diagnose reactions with a short onset time (e.g., skin manifestations), as well as serious reactions, have more frequently been reported in comparison with other reactions [33]. Oral administration of herbals in females may be most common in the population, an observation which is often made in CAM/herbal use prevalence studies [1–3]. It is therefore expected that this population would also be overrepresented in all included reports. A higher reporting rate of ADRs by females could be another factor contributing to such a pattern [34]. On the other hand, the higher proportion of females experiencing an adverse reaction in our study may confirm results of other studies in which a higher incidence of hypersensitivity reaction in females compared with males was found [35, 36]. Nevertheless, this finding does not allow conclusions to be drawn regarding the role of these characteristics as risk factors, although they are further discussed in the literature.
Asthma-like reactions were found in 4.8 % of the reports. Some commonly used herbals display a wide spectrum of cross-reactivity to other common inhalation or food allergens [7]. Therefore, a preexisting diagnosis of asthma and other atopic diseases may be a risk factor for the development of allergic reactions to herbals [37]. There exists a relevant higher incidence of herbal use among patients with known allergies [38]. For example, herbal medicine was shown to be the third most popular choice among patients suffering from asthma,with a prevalence of 60–70 % in patients with a history of moderate or severe asthma in the UK [39]. These findings imply that in the presence of known atopic diseases, health professionals and patients should use herbals only with great care in order to prevent severe allergic reactions.
Other relevant factors not recorded that could have contributed to the development of allergy-like reactions could be the patient’s genetics, nutrition status, concurrent medication, disease states (e.g., food allergies) as well as exercise-induced anaphylaxis [37, 40]. Also, unrecognized herbal–drug interactions could result in a lack of allergy control and the manifestation of allergy symptoms [41].
The strengths of our study design include the international collection of reports from 42 countries over more than four decades as well as the use of standardized HATC drug classification, WHO-ART nomenclature, and formal causality assessment for adverse reactions. At the same time it is important to recognize the special characteristics and the inherent limitations of this data source regarding the interpretation of findings. Most importantly, spontaneous reporting data do not provide information on the actual exposure to herbals in a population nor on the incidence of related ADRs. Therefore, qualitative descriptive analyses and signal detection for previously unknown drug safety issues are the primary strength of spontaneous reporting systems rather than quantitative analyses. Furthermore, the level of documentation in VigiBase® is heterogeneous, as the extracted reports do not contain original detailed free-text descriptions by the primary reporters. Particularly for the earliest reports, formal causality assessment may not be available, thus these reports had to be excluded from our study population. It must also be taken into consideration that a standardized reaction term has many advantages, but it is not the same as a clinical diagnosis based on established clinical diagnostic criteria [42]. In light of those limitations, we used a restrictive study design emphasizing high specificity with regard to the likely diagnosis of immediate allergic reactions and consequently excluded the majority of reports from the extracted original raw dataset. Such a conservative approach implies reduced sensitivity for signal detection, but we believe that overall it improves the interpretability of our findings.
There are several other challenges that pharmacovigilance studies investigating risks associated with herbal medicines face in general. As a result of insufficient herbal product regulations, some ADRs may be attributable to a lack of standardization, contamination, adulteration, plant misidentification/substitution as well as improper use of herbal medicines including their inappropriate labeling rather than the pharmacological/toxicology effects of the herbals themselves [6–8, 43]. Further, innovative preparation methods of traditionally used herbal medicines may alter their pharmacological/toxicological properties and thus lead to toxicity rather than therapeutic use. In the era of market globalization, a base knowledge of the traditional preparation and use of herbals is therefore necessary given the increase in use of these remedies outside of their culture of origin. An estimate of the frequency of ADRs to herbals is not possible based on analyses of spontaneous reporting data, but it must be assumed that our findings represent just the tip of the iceberg regarding safety issues with herbal medicines [10]. Moreover, the particular underreporting of adverse events with herbals by patients as well as healthcare professionals remains high, with health professionals themselves not always being aware of potential safety issues associated with herbal use [9–11, 44, 45].
5 Conclusion
We believe that studies using the WHO-UMC pharmacovigilance database can identify specific associations between particular herbals and adverse reactions; thus, this study has attempted to demonstrate how certain herbal medicines for oral use carry risks for immediate allergy-like ADRs. As the prevalence of herbal use is increasing, healthcare professionals as well as patients need to become better informed about the possible risks associated with these substances. When healthcare professionals record drug histories, they should also actively solicit information from their patients about all self-administered herbal medicines.
In addition, further studies are needed to establish associations and risk factors that are related to herbal use and allergic reactions.
References
Eardley S, Bishop FL, Prescott P, Cardini F, Brinkhaus B, Santos-Rey K, et al. A systematic literature review of complementary and alternative medicine prevalence in EU. Forsch Komplement. 2012;19:18–28.
MacLennan AH, Myers SP, Taylor AW. The continuing use of complementary and alternative medicine in South Australia: costs and beliefs in 2004. Med J Aust. 2006;184(1):27–31.
Wu CH, Wang CC, Tsai MT, Huang WT, Kennedy J. Trend and pattern of herb and supplement use in the United States: results from the 2002, 2007, and 2012 national health interview surveys. Evid Based Complement Altern Med eCAM. 2014;2014:872320.
Nissen N, Schunder-Tatzber S, Weidenhammer W, Johannessen H. What attitudes and needs do citizens in Europe have in relation to complementary and alternative medicine? Forsch Komplement. 2012;19:9–17.
Calixto JB. Efficacy, safety, quality control, marketing and regulatory guidelines for herbal medicines (phytotherapeutic agents). Braz J Med Biol Res. 2000;33(2):179–89.
Wiesener S, Falkenberg T, Hegyi G, Hok J, Roberti di Sarsina P, Fonnebo V. Legal status and regulation of complementary and alternative medicine in Europe. Forsch Komplement. 2012;19:29–36.
Posadzki P, Watson L, Ernst E. Contamination and adulteration of herbal medicinal products (HMPs): an overview of systematic reviews. Eur J Clin Pharmacol. 2013;69(3):295–307.
Posadzki P, Watson LK, Ernst E. Adverse effects of herbal medicines: an overview of systematic reviews. Clin Med. 2013;13(1):7–12.
Faith J, Thorburn S, Tippens KM. Examining the association between patient-centered communication and provider avoidance, CAM use, and CAM-use disclosure. Altern Ther Health Med. 2015;21(2):30–5.
Ventola CL. Current issues regarding complementary and alternative medicine (CAM) in the United States: Part 1: the widespread use of CAM and the need for better-informed health care professionals to provide patient counseling. P & T Peer Rev J Formul Manag. 2010;35(8):461–8.
Shaw D, Graeme L, Pierre D, Elizabeth W, Kelvin C. Pharmacovigilance of herbal medicine. J Ethnopharmacol. 2012;140(3):513–8.
Jacobsson I, Jonsson AK, Gerden B, Hagg S. Spontaneously reported adverse reactions in association with complementary and alternative medicine substances in Sweden. Pharmacoepidemiol Drug Saf. 2009;18(11):1039–47.
Menniti-Ippolito F, Mazzanti G, Santuccio C, Moro PA, Calapai G, Firenzuoli F, et al. Surveillance of suspected adverse reactions to natural health products in Italy. Pharmacoepidemiol Drug Saf. 2008;17(6):626–35.
WHO Uppsala Monitoring Centre. [cited 2015]. http://www.who-umc.org. Accessed 20 Feb 2016.
WHO Uppsala Monitoring Centre. The use of the WHO-UMC system for standardised case causality assessment. [cited 2015]. http://www.who-umc.org/Graphics/26649.pdf. Accessed 20 Feb 2016.
WHO Uppsala Monitoring Centre. WHO-ART - MedDRA Cross Reference Tool. [cited 2015]. http://www.umc-products.com/DynPage.aspx?id=73560&mn1=1107&mn2=1664&mn3=6045. Accessed 20 Feb 2016.
Farah MH, Olsson S, Bate J, Lindquist M, Edwards R, Simmonds MS, et al. Botanical nomenclature in pharmacovigilance and a recommendation for standardisation. Drug Saf. 2006;29(11):1023–9.
WHO. WHO Guidelines on Safety Monitoring of Herbal Medicines in Pharmacovigilance Systems. [cited 2015]. http://apps.who.int/medicinedocs/en/d/Js7148e/. Accessed 20 Feb 2016.
Murphy K, Gawchik S, Bernstein D, Andersen J, Pedersen MR. A phase 3 trial assessing the efficacy and safety of grass allergy immunotherapy tablet in subjects with grass pollen-induced allergic rhinitis with or without conjunctivitis, with or without asthma. J Negat Results Biomed. 2013;12:10.
Kay AB. An extract of Timothy-grass pollen used as sublingual immunotherapy for summer hay fever. Review. Drugs Today (Barc). 2007;43(12):841–8.
Norén GN, Hopstadius J, Bate A. Shrinkage observed-to-expected ratios for robust and transparent large-scale pattern discovery. Stat Methods Med Res. 2013;22(1):57–69.
Caster O, Juhlin K, Watson S, Norén GN. Improved statistical signal detection in pharmacovigilance by combining multiple strength-of-evidence aspects in vigiRank. Drug Saf. 2014;37(8):617–28.
de Groot H, Bijl A. Anaphylactic reaction after the first dose of sublingual immunotherapy with grass pollen tablet. Allergy. 2009;64(6):963–4.
Andrographis paniculata. In: Jellin JM, Gregory PJ, Calvillo A, et al. Natural medicines comprehensive database. Stockton, CA: Therapeutic Research Center. http://www.naturaldatabase.com/. Accessed 15 Oct 2015.
Suwankesawong W, Saokaew S, Permsuwan U, Chaiyakunapruk N. Characterization of hypersensitivity reactions reported among Andrographis paniculata users in Thailand using Health Product Vigilance Center (HPVC) database. BMC Complement Altern Med. 2014;14:515.
Bauer C, Oppel T, Rueff F, Przybilla B. Anaphylaxis to viscotoxins of mistletoe (Viscum album) extracts. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. 2005;94(1):86–9.
Bregnbak D, Menne T, Johansen JD. Airborne contact dermatitis caused by common ivy (Hedera helix L. ssp. helix). Contact Dermat. 2015;72(4):243–4.
de Boer HJ, Hagemann U, Bate J, Meyboom RH. Allergic reactions to medicines derived from Pelargonium species. Drug Saf. 2007;30(8):677–80.
Munoz X, Culebras M, Cruz MJ, Morell F. Occupational asthma related to aescin inhalation. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. 2006;96(3):494–6.
Ozdemir C, Schneider LA, Hinrichs R, Staib G, Weber L, Weiss JM, et al. Allergic contact dermatitis to common ivy (Hedera helix L.). Hautarzt. 2003;54(10):966–9.
Schapowal A. Efficacy and safety of Echinaforce(R) in respiratory tract infections. Wien Med Wochenschr. 2013;163(3–4):102–5.
Warrington R, Dan FS. Drug allergy. Allergy Asthma Clin Immunol. 2011;7(1):10.
Thiessard F, Roux E, Miremont-Salamé G, Fourrier-Réglat A, Haramburu F, Tubert-Bitter P, et al. Trends in spontaneous adverse drug reaction reports to the French pharmacovigilance system (1986–2001). Drug Saf. 2005;28(8):731–40.
Barsky AJ, Peekna HM, Borus JF. Somatic symptom reporting in women and men. J Gen Intern Med. 2001;16(4):266–75.
Alomar MJ. Factors affecting the development of adverse drug reactions (Review article). Saudi Pharm J SPJ Off Publ Saudi Pharm Soc. 2014;22(2):83–94.
Thong BY, Tan TC. Epidemiology and risk factors for drug allergy. Br J Clin Pharmacol. 2011;71(5):684–700.
Food allergy: A practice parameter update—2014. [cited 2015]. http://www.aaaai.org/Aaaai/media/MediaLibrary/PDF%20Documents/Practice%20and%20Parameters/Food-Allergy-A-Practice-Parameter-Update-2014.pdf. Accessed 20 Feb 2016.
George M, Topaz M. A systematic review of complementary and alternative medicine for asthma self-management. Nurs Clin N Am. 2013;48(1):53–149.
Ernst E. Complementary therapies for asthma: what patients use. J Asthma. 1998;35(8):667–71.
Simons FE, Ebisawa M, Sanchez-Borges M, Thong BY, Worm M, Tanno LK, et al. 2015 update of the evidence base: World Allergy Organization anaphylaxis guidelines. World Allergy Organ J. 2015;8(1):32.
Izzo AA, Ernst E. Interactions between herbal medicines and prescribed drugs: an updated systematic review. Drugs. 2009;69(13):1777–98.
Rive CM, Bourke J, Phillips EJ. Testing for drug hypersensitivity syndromes. Clin Biochem Rev Aust Assoc Clin Biochem. 2013;34(1):15–38.
Byard RW. A review of the potential forensic significance of traditional herbal medicines. J Forensic Sci. 2010;55(1):89–92.
Cellini M, Attipoe S, Seales P, Gray R, Ward A, Stephens M, et al. Dietary supplements: physician knowledge and adverse event reporting. Med Sci Sports Exerc. 2013;45(1):23–8.
Hazell L, Shakir SA. Under-reporting of adverse drug reactions: a systematic review. Drug Saf. 2006;29(5):385–96.
Acknowledgments
We would like to thank Niklas Norén, PhD, Chief Science Officer, and other colleagues at the UMC especially Marie Lindguist, MSc, PhD; Hon FRCP, Pia Caduff-Janosa, MD; Anders Viklund, MSc Pharm; Monica Ploën, BSc Pharm; and Mohamed Farah, Pharm D, for their support as well as the WHO National Pharmacovigilance Centers for providing additional information.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was supported by grant SVV 260 295.
Conflicts of interest
Jitka Pokladnikova, Ronald H. B. Meyboom, Ricarda Meincke, David Niedrig, and Stefan Russmann have no conflicts of interest that are directly relevant to the content of this study.
Rights and permissions
About this article

Cite this article
Pokladnikova, J., Meyboom, R.H.B., Meincke, R. et al. Allergy-Like Immediate Reactions with Herbal Medicines: A Retrospective Study Using Data from VigiBase® . Drug Saf 39, 455–464 (2016). https://doi.org/10.1007/s40264-016-0401-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-016-0401-5