
Abstract
Objectives
This article develops two inference procedures to calculate the inequality aversion and alpha parameters of a health-related social welfare function with constant elasticity (CES-HRSWF) using stated preferences. Based on the relative concept of inequality, a range of values were proposed for the trade-offs between improving total population health and reducing health inequalities.
Methods
A self-administered questionnaire was used to collect data from a sample of 422 college students in Portugal. Respondents faced three hypothetical allocation scenarios where they needed to decide between two health programmes that assign different health gains to two anonymous sub-groups of the population and to two sub-groups identified by socioeconomic class. Combinations of the median response to these three questions were used to estimate the parameters of the CES-HRSWF.
Results
Findings suggest that the quantification of the efficiency–equality trade-off is not independent of the inference procedure used. Plausible values for the inequality aversion and for the alpha parameters were obtained ranging from 2.24 to 4.85 and from 0.5 to 0.58, respectively.
Conclusions
Respondents revealed some aversion to health inequality. However, the extent of this aversion seems to be sensitive to (1) the identification of the groups by occupation status, (2) the size of the health gain, and (3) the inference procedure used.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
This study represents a methodological advance in measuring social stated preferences and the concomitant efficiency–equality trade-offs. |
The level of health inequality aversion seems to depend on the inference procedure used. |
Respondents of this study seem to be willing to sacrifice some efficiency in order to reduce inequalities among socioeconomic classes. |
1 Introduction
Inequalities in health between groups with different socioeconomic status constitute one of the main challenges for public health [1]. Any publicly funded health care system seeks to achieve the maximization of population health while reducing inequalities in health across groups within the population. This potential conflict between efficiency and equality in health outcomes is fuelled by the need to ration health care, given existing budget constraints. Policy makers face the challenge of knowing whether and how far society is willing to trade-off overall societal health for a more equitable distribution of health gains.
Analytically, a constant elasticity of substitution “health-related social welfare function” (CES-HRSWF) has been proposed in the health economics literature as a framework to accomplish such an assessment [2, 3]. This social welfare specification incorporates two separate parameters that summarize social preferences for equality: (1) overall strength of inequality aversion (r) and (2) overall difference in concern over the health status of each population group (α). What remains under discussion in the health economics literature is how to estimate both of these parameters through individual preferences, knowing that these parameters are interrelated.
In recent years, there have been some attempts to estimate these parameters from stated preferences of individuals [4,5,6,7,8]. The first attempt estimated solely the inequality aversion parameter by assuming the anonymity principle (α = 0.5) [4, 6]. Later, Dolan and Tsuchiya [5] estimated both parameters by taking together the preferences concerning responsibility for health and health inequalities. However, this approach defined each parameter through the stated preferences of different respondents, thereby confining any conclusions that could be drawn. Edlin et al. [7, 8] used an approach based on pairwise social preferences over states of the world with equal social welfare, but they only estimated the inequality aversion parameter along with the argument of the social welfare function (SWF).
The present article takes a more comprehensive approach by proposing two different inference procedures partly supported by approaches developed earlier [5, 6, 8]. With this article, we intend to overcome some of the methodological shortcomings identified. In contrast to previous work, which mainly used between-subject designs, participants of the current study faced a series of systematically varied questions in a within-subject design. Additionally, we recreate a hypothetical scenario that allows the estimation of both parameters of the health-related social welfare function (HRSWF), at the same time examining Portuguese preferences for reducing inequalities in the (average) age of death by occupation status in the active population. We explore whether these preferences fed into a CES-HRSWF and, importantly, if the efficiency–equality trade-off is sensitive to the inference procedures used.
2 Functional Form of the CES-HRSWF and Approaches to Estimate Its Parameters
In a seminal paper, Wagstaff [2] proposed a flexible functional form for an HRSWF to reflect different degrees of inequality aversion in health outcomes:
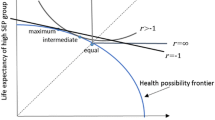
where W is the health-related social welfare; HA and HB are the average health levels of groups A and B (both groups are of equal size); and r and α define the curvature of the HRSWF, respectively. The α parameter reflects the weight given to the health outcome of one group relative to the other group for reasons beyond health differences. The r parameter reflects the degree of aversion to inequality in health outcomes. The contours of the iso-welfare curve depend on the values of r. It gives rise to a utilitarian-type SWF when r = − 1 (and α = 0.5). In this case, no importance is given to inequality in the sense that the health-related social welfare is just a sum of individuals’ health status. The opposite happens when r approaches infinity, representing Rawlsian preferences that indicate a disregard of anybody except for the worst off. Inequality aversion preferences are detected when r varies between − 1 and ∞, with growing importance given to equality as the value of the r parameter increases. Appendix A [see the electronic supplementary material (ESM)] reproduces a visual aid description of this methodology and adds some detailed explanations.
In short, the α and r parameters define the rate at which the health of each group enters the social welfare calculation. The definition of the implied weights given to a unit health gain to one of these groups relative to another is represented by the marginal rate of social substitution (MRSS) along the iso-welfare curve.
The computation of the MRSS requires the identification of two points [X(XA, XB) and Y(YA, YB)] lying on the same side of the 45° line judged as equally good in terms of social welfare [6]. Formally, the MRSS depends on both parameters of the CES-HRSWF (details of the mathematical expression can be found elsewhere [6]):
Further, by taking logarithms and solving for r:
The impetus given to the estimation of the MRSS through stated preferences was due to the pioneering work of Dolan et al. [4] (later published by Dolan and Tsuchiya [6]). The authors elicited social preferences using stylized questions specially designed to allow the identification of two points over the same social welfare contour [9]. The authors estimated the inequality aversion parameter and then the MRSS assuming the anonymity principle (α = 0.5). However, empirical evidence suggests that the anonymity principle is not a good representation of societal preferences. A growing amount of empirical literature [10,11,12,13,14,15] reports that, when establishing priorities between patients (or groups of patients), the general public does not value a health benefit equally irrespective of who gets it. Thus, in practice, the anonymity assumption does not hold in every circumstance. Therefore, both parameters of the CES-HRSWF should be uncovered if any meaningful conclusion about equality–efficiency trade-offs is to be drawn. Since the CES-HRSWF depends simultaneously on the values for r and for α, it might happen that any two individuals derive exactly the same level of well-being from a particular distribution of health not because the coefficient of inequality aversion (r) is the same, but because the same manifestation of preferences results from the combination of different values of both parameters (r and α). Thus, the approach used by Dolan and Tsuchiya [6] does not allow the individual identification of any of the parameters.
To circumvent this problem, and to identify both parameters for the same individual, this approach should be complemented. Based on the Atkinson relative inequality index, we propose two inference procedures that allow the estimation of each parameter of the HRSWF independently. As these two approaches do not necessarily result in the same values for the r and α parameters, we propose an empirical study to test and interpret the results of each inference procedure.
3 Methods: Study Design
3.1 Questionnaire
To elicit individuals’ preferences for the efficiency–equality trade-off, we used a self-administered questionnaire. The questionnaire comprises three hypothetical allocations giving rise to three different questions. These questions allow the identification of relevant points on the HA and HB plane.
The first two questions are related to inequalities in the (average) age of death in the active population. We used the average age of death in the active population as a metric for efficiency for two main reasons. Firstly, it is well known that profession plays a crucial role in understanding health inequalities [16, 17]. From the set of factors associated with the practice of a profession (beyond income and education), we have to consider the cumulative effects of working conditions on the health of the individual, namely infra-pathological problems (such as the exposure to risk factors) and the psychosocial relationship between health status and professional insertion [18]. Secondly, this is a metric of particular policy interest for Portugal due to the large difference that remains (comes from the past) in the average age of death between the top and bottom groups of the socio-professional pyramid [19]. This suggests that progress in reducing health inequalities has been limited. Furthermore, the increasing deregulation of the labour market (largely imposed by creditors) during the last few years is increasing the precariousness in working conditions, which may exacerbate this inequality.
In Portugal, in 2011, there was a difference of 7 years in the average age of death among socioeconomic classes in the active population (age below 65 years) [19]. We employed data from the top and the bottom classes which integrate roughly the same percentage of the relevant working population (10.2 and 12.2%, respectively). On average, and taking the upper limit of 65 years (retirement age), highest skilled workers (HSW) died at 55 years of age while the lowest skilled workers (LSW) died at 48 years of age [19]. This very early death age has a technical explanation. During the last 3 decades, the number of deaths in the labour force has been concentrated in intermediate ages as the percentage of the youngest and, above all, the percentage of the oldest in the active population are decreasing [16]. To test whether people’s aversion to inequality differs according to the amount of the initial difference in the average age of death in the active population and also to explore whether respondents are sensitive to the size of the health gains, as suggested in previous studies [20, 21], we conducted two versions of the survey. Half of the respondents faced the real difference of 7 years in the average age of death (version 7) in the active population between HSW and LSW, while the other respondents faced an initial difference of only 4 years (version 4).
The third question is related to the treatment of HSW and LSW.
All questions were presented in a graphical form and are reproduced in Appendix B (see the ESM). A brief description of each question is given below.
The first question (question 1) recreates an anonymity scenario (α = 0.5) where two unidentified groups (group A and group B) present a 7-year (group A = 48 years; group B = 55 years) or a 4-year (group A = 51 years; group B = 55 years) difference in the average age of death (version 7 and 4, respectively) in the active population. Respondents should decide between (or be indifferent to) two alternative health programmes with the same costs. Programme I increases years of life of both groups by the same amount (3.5 or 2 years for each group, in version 7 or version 4, respectively), maintaining the initial inequality in the average age of death in the active population. The alternative programme, programme II, eliminates the inequality in the average age of death in the active population between both groups by providing the disadvantaged group with the necessary increase in years of life (7 or 4 years, in each version). For respondents who selected programme I (or were indifferent), no further questions were asked as they reveal a concern with equality of health gains instead of equality in health outcomes. In the second stage, those respondents who selected programme II were faced with pairs of choices between the same programme I and a modified programme II assigning decreasing years of life to the group with less life expectancy (in 6-month decrements). This means that programme II reduces the inequalities in the average age of death in the active population across both groups, but at the expense of lower overall gains (efficiency). When respondents switch from programme II to programme I it means that they are no longer willing to lose health gains—efficiency. Thus, the trade-off between efficiency and equality is calculated when respondents switch from programme II to programme I. The inequality aversion parameter is identified through the indifference point, taken half way between the last choice of programme II and the switch to programme I. Respondents who never switch to programme I, even when programme II promotes a lesser health gain to the disadvantage group than programme I, reveal an extreme concern with inequality translated in the violation of the monotonicity principle [22, 23]. The pattern of responses given to this first question allows the definition of the r parameter, because the expressed preferences are entirely attributable to the inequality aversion parameter.
The second question (question 2), used by Dolan et al. [4], is exactly equal to the first one. The only difference rests in the identification of the groups involved. In this second question, the hypothetical scenario involves the groups identified as LSW and HSW (rather than the unidentified groups A and B in the first question). A detailed representation of the interactive process used in both questions can be found in Figure A2 in Appendix C (for version 7) (see the ESM).
Our analysis will focus on the median response rather than on the mean response. This is consistent with the median voter rule [24] and because the inequality aversion parameter approaches infinity for maximum responses [6].
The first inference procedure we propose is to combine the median responses of these two questions. This combination allows the identification of an implicit value for α. Through this method we can conclude that, if the median responses to both questions differ, any difference should be attributed to the identification of the groups and not to differences in health between them (which are exactly the same). If we assume that the “anonymity” scenario (question 1) estimates correctly the inequality aversion parameter (r), then the entire difference between the preferences in the two scenarios (with and without the identification of groups) can be explained by α. Therefore, by using the value of r defined in the question 1 (when α = 0.5) and the median response when the groups are identified (question 2), it is possible to define an implied value for α. In fact, equality in social welfare between the median response in question 1 and question 2 is achieved by varying α using the value for the inequality aversion parameter obtained previously from question 1. Generally, α can be calculated through:
where r is known (calculated in the anonymity scenario); XA and XB are the median choice made in the anonymity scenario (question 1); and YA and YB are the median choice made in the scenario where the two groups are identified (question 2).
The third question (question 3) was used by Dolan and Tsuchiya [5]. This question recreates a hypothetical scenario where the two groups, HSW and LSW, have the same health. Through a person trade-off technique, respondents must choose between (or be indifferent to) two alternative health programmes that have the same cost. Programme I saves the life of 100 HSW while the alternative programme II saves the life of 100 LSW. For those respondents who selected programme I (or were indifferent), no further questions were asked since it reveals that respondents desire to favour economically advantaged individuals or do not weight differently the life of individuals according to their professional class. On the contrary, respondents selecting programme II reveal a desire to favour economically disadvantaged individuals. In order to explore the weight attributed to the professional class, respondents were, in a second stage, faced with pairs of choices between the same programme I (saves 100 HSW) and a modified programme II that saves a decreasing number of LSW (95, 80, 75, 60, 40, and 25). The specific weight given to the professional class is calculated at the midpoint between the last choice of programme II and the switch to programme I. A detailed representation of this interactive process can be found in Figure A3 in Appendix C (see the ESM).
Responses to this question can be used to calculate the real value of α (in contrast to the implicit value obtained by comparing responses to the first and second questions). The value of α can be calculated through:
where q represents the number of LSW saved and p corresponds to 100 HSW saved.
The second inference procedure we propose here consists in combining the median response from the second and third questions. After quantifying the value of α through the median response of the third question, we can use Eq. 2 to calculate the implicit value for r.
Thus, using the median responses for these three questions allows us to build and compare two alternative inferences procedures for the CES-HRSWF parameters through stated preferences.
3.2 Participants
The questionnaire was administered during 2015, in a controlled environment, with a random sample of 422 college students (arguably, future opinion leaders) from public and private institutions located in the north and the centre of Portugal. The sample included students from different programmes: economics (19.5%), management (17.5%), law (14.5%), psychology (12.5%), medicine (19.5%), and nursing (16.5%). Students were brought together in small groups to fill the questionnaire without communicating with each other. The participation of all respondents was voluntary, and they were granted time to formulate reflective opinions, as suggested by Dolan et al. [25]. Following most of the studies in health economics, we also adopted a social perspective. Respondents were asked to overlook their self-interest and adopt a citizen-type perspective [26].
The majority of respondents (52.8%) were female, with ages ranging between 18 and 51. The majority of the students (52.5%) had ages between 18 and 25 years. Most respondents (74.5%) were single, and 56.5% had a net monthly income exceeding €1500. Regarding the perception of their health status, almost all respondents (89.6%) considered themselves to have good or very good health. On average, the sample was younger and had a higher income than the Portuguese population.
4 Results
Table 1 summarizes the findings for the first two questions in both versions of the questionnaire. The first row in the table reports the percentage of respondents who did not reveal inequality aversion or supported the equal distribution of health gains (selected programme I or were indifferent in the first stage); the second row reports the percentage of respondents who initially chose programme II, but switched to programme I at some point (accepted some trade–off), and the third row reports the percentage of respondents that always selected programme II, never switching to programme I.
We observe that the percentage of respondents willing to sacrifice efficiency in order to reduce inequality is, in both versions, higher when the identity of groups is defined by professional classes (question 2). The numbers in the last row of the table seem to support this idea, by indicating that nearly twice the number of respondents revealed an extreme aversion to inequality when the distribution of health gains between HSW and LSW is identified (question 2). Therefore, these respondents weighted differently the average year of death of HSW and LSW (α ≠ 0.5).
Detailed results of the responses to questions 1 and 2 in both versions (4 and 7) of the questionnaire are summarized in Table 2. For version 4 (top panel in Table 2) and under the anonymity scenario (question 1), the median response shows indifference between an average age of death in the active population of 53 and 57 years for groups A and B, respectively, and a corresponding average age of death in the active population of 54.75 and 55 years [(HA = 53; HB = 57) ≈ (HA = 54.75; HB = 55)]. Thus, the respondents appear to be willing to sacrifice 3 months in total life expectancy in order to reduce the current inequality in the average age of death between the two groups of individuals. For α = 0.5, and through Eq. 3, the value of r is then 2.45. From Eq. 2, the implied equity weight for a marginal health improvement at the initial point is 1.3 (MRSS = 1.3). This means that a marginal health gain for individuals who, on average, die earlier (53 years old) is about 1.3 times more valued than a marginal health gain for individuals who, on average, die later (57 years old).
This trade-off seems more pronounced when both groups are identified by professional classes (question 2). The median response shows a sacrifice of 9 months in total life expectancy to reduce the current inequality in the average age of death in the active population between HSW and LSW [(HLSW = 53; HHSW = 57) ≈ (HLSW = 54.25; HHSW = 55)].
For version 7 (bottom panel in Table 2) under the anonymity scenario (question 1), the median response represents preference for a neutral distribution of health gains [(HA = 51.5; HB = 58.5) ≈ (HA = 55; HB = 55)]. For α = 0.5, the value of r is equal to − 1, reflecting a utilitarian SWF and consequently an MRSS of 1. When groups are identified by LSW and HSW (question 2), the median response revealed a willingness to sacrifice 1.25 years of life expectancy in order to reduce the inequality in the age of death between both professional groups [(HLSW = 51.5; HHSW = 58.5) ≈ (HLSW = 53.75; HHSW = 55)].Footnote 1
It should be noted that using solely the results from the second question does not allow the definition of the values for r or α. However, according to our inference procedure, combining the median responses of the first and second questions, the implicit value of α can be calculated using Eq. 4 (for versions 4 and 7, respectively) as follows:
Therefore, the implicit values for α are 0.58 and 0.61 in version 4 and 7, respectively. By replacing these implicit values for α in Eq. 2, we can define the correct values for the MRSS as 1.8 and 1.6 (instead of the 1.3 and 1 obtained when α is assumed to be equal to 0.5) in versions 4 and 7, respectively.
Table 3 summarizes the results for the third question. The findings suggest a median response that weights equally both groups in each version, meaning support for the anonymity assumption (α = 0.5).
According to our second inference procedure, combining the median responses of the second and third questions, the values of r obtained from Eq. 3 are 9.85 and 4.85 for versions 4 and 7, respectively. These data translate into an MRSS of 2.3 and 2.2 for versions 4 and 7, respectively.
Table 4 synthesizes the main results of the empirical study. For each inference procedure, the values for the parameters α and r are presented and the corresponding MRSS calculated. Through our first inference procedure, which consists in comparing the pattern of responses to questions with and without identification of the groups (first and second questions), we identify a pair of α values (0.58 and 0.61) and a pair of r values (2.45 and − 1) in each version of the study (versions 4 and 7, respectively). Hence, the values of the MRSS calculated from Eq. 2 are 1.8 and 1.6 in versions 4 and 7, respectively. For version 7 (version 4), these findings indicate that extending by 1 year the average age of death of the LSW is weighted at least 1.6 (1.8) times more than extending by 1 year the life of the HSW. In other words, the median response suggests a willingness to accept a loss of 1.6 (1.8) life expectancy years of the HSW in order to guarantee an increase in 1 life expectancy year of the LSW. Although these differences between versions are not large, they suggest that respondents are to some extent sensitive to the initial difference in the average age of death in the active population amongst groups and to the respective size of the health gains, a feature that should be taken into account in empirical studies assessing efficiency–equality trade-offs in health.
According to our second inference procedure, which combines the median responses to the second and third questions, the computed values for r are substantially higher in both versions. This happens because the values found for α through the third question are lower (α = 0.5) than those obtained through our first inference procedure. Replacing these lower values for α in Eq. 3, and in order to attain the same social welfare level reached from answers to question 2, a greater degree of inequality aversion is required. This inference process, combining the responses to the second and third question, seems to increase substantially the degree of inequality aversion.
We therefore conclude that the two inference procedures produce different results concerning the r and α parameters of the CES-HRSWF, with the second procedure prompting higher levels of inequality aversion. From the application of the two versions and from the combination of the two inference procedures, our study allows the identification of plausible ranges for these median parameter values rather than just the median point estimates formed by each version and each inference procedure alone. This is an important result of our work.
A box plot depicting these value ranges, stratified by each version of the study, is presented in Fig. 1. For each parameter, the upper and lower limits of the blue boxes represent the minimum and maximum values obtained according to each inference procedure, and the red boxes demarcate the range of plausible parameter values resulting from the intersection of the relevant intervals. Thus, looking at the r parameter in version 4, the minimum value is 2.45, resulting from the first inference procedure (question 2 + question 1), and its maximum value is 9.85, resulting from the second inference procedure (question 2 + question 3); from version 7, the minimum r value is − 1, resulting from the first inference procedure (question 2 + question 1), and the maximum r value is 4.85, resulting from the second inference procedure (question 2 + question 3). The intersection of these values produces plausible values for the r parameter ranging from 2.45 up to 4.85. By the same reasoning, we obtain plausible values for the α parameter ranging from 0.50 up to 0.58, and plausible values for the MRSS ranging from 1.8 up to 2.2. Taken together, these results indicate that the majority of respondents express some inequality aversion between HSW and LSW, and when there are deviations from the anonymity principle, they clearly favour the more economically and/or socially disadvantaged groups in society.

Median value ranges for α, r and MRSS. Alpha weight given to the health status of one group relative to the other group, MRSS marginal rate of social substitution, Q question r inequality aversion parameter, Vers. version
5 Discussion and Conclusion
Much has been discussed in the health economic literature about whether publicly funded health care systems should treat all health gains as having the same social value. Although there is now a wide range of empirical evidence supporting the idea that people value not only efficiency, but also equity, little is known about the quantification of the trade-off between efficiency and equality in health. The purpose of this study was to develop new inference procedures that contribute to such quantification.
In the study reported in this paper, we sought to determine both parameters of the CES-HRSWF from peoples’ stated preferences over various efficiency–equality trade-offs between the average age of death in the active population of LSW and HSW. We proposed two distinct inference procedures to calculate these parameters. The inference procedures differ in the way used to calculate the α parameter. We either recreate an anonymity scenario or calculate directly the α parameter by assuming no inequality in health between LSW and HSW. The α value thus obtained ranges from that corresponding to the anonymity principle to values giving greater weight to LSW. The global results suggest that respondents of this study reveal some aversion to inequality. The extent of this aversion seems to be, however, sensitive to (1) identification of the groups by occupation status, (2) the size of the health gain and (3) the inference procedure used. Findings suggest that respondents’ preferences fed into the CES-HRSWF specification and that the quantification of the efficiency–equality trade-off is not independent of the inference procedure used. In general, the two inference procedures proposed produce different results concerning the values of the parameters of the SWF and, hence, the MRSS. However, the combination of these two inference procedures allows the identification of plausible ranges for median parameter values rather than just the median point estimates obtained by each procedure alone. This led us to conclude that empirical studies that attempt to estimate people’s stated preferences for inequality aversion in the health space should subject their results to sensitivity analysis to these sources of variation.
One key strength of our study is the methodological progress produced through the development of inference procedures with systematically varied questions in a within-subject design. The results should be interpreted with appropriate caution, however, given the non-random nature of the sample (college students). The findings cannot be generalized to the Portuguese general public. A large amount of empirical literature suggests that age and level of education affect people’s attitudes toward distributional preferences [15, 27]. However, the main aim here was not to achieve an accurate representation of the opinions of the Portuguese people in general, but to set up a new methodological approach to elicit social preferences through an SWF. Besides this sampling limitation, there are also limitations in quantifying psychosocial values in health [28]. It has been shown that very subtle changes in the framing of a question can result in different “revealed” preferences [29, 30]. In this context there are at least four reasons to treat the results with caution. First, some ordering bias may explain, at least in part, the differences in responses between the first two questions of the questionnaire. Responses to both questions may have been affected by individuals’ cognitive processing strategies and heuristic [31]. We believe we have minimized this order effect by first presenting the scenario with anonymity and only then the scenario with the identification of the groups. Second, the average age of death in the active population is attributable to a small minority within each group who die pre-retirement (the average age of death of the active population is much lower than the average age of death of the whole population). It is possible that some respondents (we believe a minority) could have worked this out. If so, we may have a bias because their answers may reflect not just aversion to inequality across groups, but also within groups. Third, eliciting preferences through person trade-off questions like the one we use in the third question may not be the most suitable method. The result for symmetry is not surprising insofar as we are aware of the difficulty respondents may feel about letting people die. Finally, the way in which the questions are presented may influence the results. In order to improve the understanding of the questions, we used the pictorial forms. However, to facilitate the visual representation in the first two questions, the scales on the graphs in the average age of death (in the active population) did not start at zero. This could have led some respondents to perceive that the relative difference between the groups was larger than it really was. This possible bias is even more likely in version 7 due to the scale used, which exaggerates the relative difference between the two groups.
We note that, although such framing effects are well acknowledged in the psychology literature, they are still under-explored in the elicitation of societal preferences [32].
Despite these limitations, we believe that this study represents an advance in terms of the methodology used and in terms of health policies definition. There have been a number of previous empirical studies of health inequality aversion using an identical questionnaire design in England [5, 6, 33, 34] and Spain [22, 23] as well as other instruments [8]. Many of these studies have found that the majority of respondents are willing to sacrifice total health in order to reduce health inequalities in life expectancy between social classes. However, the inequality aversion parameter reported in these studies was quite different from the one used here and is not comparable, due to different study designs and consequent inference procedures. We improved the inference procedures and found that some inequality aversion in life expectancy in active population exists between the top and bottom occupational classes. We also found that respondents seem to give weight to the professional class to which individuals belong, which accentuates the inequality aversion. This study demonstrates that, using an adequate questionnaire design, it is possible to use the SWF as a practical device to define inequality aversion parameters and to apply them to distributional cost-effectiveness analysis. A recent study illustrates how inequality aversion parameters can be used in practice [35]. This is particularly interesting for countries with low job quality, such as Portugal. Recent data revealed big differences across groups of workers in Portugal [36]: low-skilled workers tend to have the worst performance in terms of employment, lower earnings, considerably higher labour market insecurity and higher job strain.
In conclusion, this study (1) contributes to drawing attention to the importance of social stated preferences in formulating health policies and (2) represents a methodological advance in measuring such preferences and the concomitant trade-offs.
Notes
A reviewer cautioned that, in each version, the median responses to question 1 (Q1) and question 2 (Q2) may not be empirically correlated in the sense that they may belong to different respondents. While this behavioral hypothesis points to the development of different statistical analyses, we do not find this behavior in the current data. In fact, in version 4 (version 7) 78% (74%) of the 118 (129) participants whose response to Q1 was below or equal to the respective median response also responded below or equal to the median response to Q2 as identified in Table 2. Likewise, 79% (73%) of the 117 (130) participants whose response to Q2 was below or equal to the respective median response also responded below or equal to the median response to Q1 as identified in Table 2. This indicates a high degree of agreement between the ranking of respondents in Q1 and the ranking of respondents in Q2. Additional analysis (available upon request) confirms the statistical significance of this apparent agreement in each Version.
References
Marmot M. Social determinants of health inequalities. Lancet. 2005;365:1099–104.
Wagstaff A. QALYs and the equity-efficiency trade-off. In: Layard A, Glaister S, editors. Cost-benefit analysis. 2nd ed. Cambridge: Cambridge University Press; 1994 [(reprinted from Journal of Health Economics, 10 (1991) 21–41, with corrections)].
Dolan P. The measurement of individual utility and social welfare. J Health Econ. 1998;17:39–52.
Dolan P, Tsuchiya A, Smith P, Shaw R, Williams A. Determining the parameters in a social welfare function using stated preference data: an application to health. Sheffield Health Economics Group Discussion Paper Series. Ref 02/2. Sheffield: The University of Sheffield; 2002.
Dolan P, Tsuchiya A. The social welfare function and individual responsibility: some theoretical issues and empirical evidence. J Health Econ. 2009;28(1):210–20.
Dolan P, Tsuchiya A. Determining the parameters in a social welfare function using stated preference data: an application to health. Appl Econ. 2011;43(18):2241–50.
Edlin R, Tsuchiya A, Dolan P. Measuring the societal value of lifetime health. Sheffield Economics Research Papers. Series 2009010; 2009.
Edlin R, Tsuchiya A, Dolan P. Public preferences for responsibility versus public preferences for reducing inequalities. Health Econ. 2012;21(12):1416–26.
Shaw R, Dolan P, Tsuchiya A, Williams A, Smith P, Burrows R. Development of a questionnaire to elicit public preferences regarding health inequalities. York: Centre for health Economics, University of York; 2001.
Dolan P, Shaw R, Tsuchiya A, Williams A. QALY maximization and people’s preferences: a methodological review of the literature. Health Econ. 2005;14:197–208.
Whitty J, Lancsar E, Rixon K, Golenko X, Ratcliffe J. A systematic review of stated preferences studies reporting public preferences for healthcare priority setting. Patient Patient Cent Outcomes Res. 2004;7:365–86.
Gu Y, Lancsar E, Ghijben P, Butler J, Donaldson C. Attributes and weights in health care priority setting: a systematic review of what counts and to what extent. Soc Sci Med. 2015;146:41–52.
Pinho M, Borges A. Bedside healthcare rationing dilemmas: a survey from Portugal. Int J Hum Rights Healthc. 2015;8(4):233–46.
Pinho M, Borges A, Zahariev B. Bedside healthcare rationing dilemmas: a survey from Bulgaria and comparison with Portugal. Soc Theory Health. 2017;15(3):285–301.
Rogge J, Kittel B. Who should not be treated: public attitudes on setting health care priorities by person based criteria in 28 nations. Plos One. 2016;11(6):e0157018.
Ferreira P, Silva P. Diferenças sociais na morte: a evolução do número de óbitos na população activa Portuguesa (1981–2001). Revista Portuguesa de Saúde Pública. 2007;25(1):70–84.
Mackenbach J, Stirbu I, Roskam A, Schaap M, Menvielle G, Leinsalu M, Kunst A. Socioeconomic inequalities in health in 22 European countries. New Engl J Med. 2008;358:2468–81.
Volkof S, Thebaud-Mony A. Santé au travail: l’inégalité des parcours. In: Leclerc A, et al., editors. Les Inégalités socials de santé. Paris: Inserm/La Découverte; 2000.
INE-Instituto Nacional de Estatística. Estatísticas Demográficas 2012. Lisboa; 2012.
Cuadras-Morato X, Pinto-Prades J, Abellan-Perpinan J. Equity considerations in health care: the relevance of claims. Health Econ. 2001;10(3):187–205.
Abásolo I, Tsuchiya A. Understanding preference for egalitarian policies in health: are age and sex determinants? Appl Econ. 2008;1:1–11.
Abásolo I, Tsuchiya A. Exploring social welfare functions and violation of monotonicity: an example from inequalities in health. J Health Econ. 2004;23:313–29.
Abásolo I, Tsuchiya A. Is more health always better for society? Exploring public preferences that violate monotonicity. Theory Decis. 2013;74:539–63.
Mueller D. Public choice. Cambridge: Cambridge University Press; 1979.
Dolan P, Cookson R, Ferguson B. Effect of discussion and deliberation on the public’s views of priority setting in health care: Focus group study. Br Med J. 1999;318:916–9.
Dolan P, Olsen J, Menzel P, Richardson J. An inquiry into the different perspectives that can be used when eliciting preferences in health. Health Econ. 2003;12:545–51.
Winkelhage J, Diederich A. The relevance of personal characteristic in allocating health care resources—controversial preferences of laypersons with different educational backgrounds. Int J Environ Res Public Health. 2012;9:223–43.
Dolan P, Shaw R. A note on the relative importance that people attach to different factors when setting priorities in health care. Health Expect. 2003;6(1):53–9.
Rabin M. Psychology and economics. J Econ Lit. 1998;36(1):11–46.
Kahneman D, Slovic P, Tversky A, editors. Judgement under uncertainty: heuristics and biases. Cambridge: Cambridge University Press; 1982.
Lloyd A. Threats to the estimation of benefit: are preference elicitation methods accurate? Health Econ. 2003;12:393–402.
Rowen D, Brazier J, Keetharuth A, Tsuchiya A, Mukuria C. Comparison of modes of administration and alternative formats for eliciting societal preferences for burden of illness. Appl Health Econ Health Policy. 2016;14(1):89–104.
Dolan P, Tsuchiya A. Do NHS staff and members of the public share the same views about how to distribute health benefits? Soc Sci Med. 2007;64:2499–503.
Robson M, Asaria M, Cookson R, Tsuchiya A, Ali S. Eliciting the level of health inequality aversion in England. Health Econ. 2017;26:1328–34.
Asaria M, Griffin S, Cookson R, Whyte S, Tappenden P. Distributional cost-effectiveness analysis of health care programmes—a methodological case study of the UK Bowel Cancer Screening Programme. Health Econ. 2015;24:742–54.
OCDE-Employment. 2016. http://www.oecd.org/employment/the-crisis-has-had-a-lasting-impact-on-job-quality-new-oecd-figures-show.htm.
Data Availability Statement
Authors can confirm that all relevant data are included in the article and/or its supplementary information files. The authors declare that (the/all other) data supporting the findings of this study are available within the article (and its supplementary information files).
Author information
Authors and Affiliations
Contributions
MP conceived and designed the study and drafted the first draft of the paper. AB analysed the data and reviewed and suggested the structure of the manuscript. All authors contributed critically to the revision of the manuscript for intellectual content and approved its submission for publication.
Corresponding author
Ethics declarations
Funding
Micaela Pinho and Anabela Botelho disclose no receipt of any financial support for the research, authorship, and/or publication of this article.
Conflict of interest
Micaela Pinho and Anabela Botelho declare they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants before being included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Pinho, M., Botelho, A. Inference Procedures to Quantify the Efficiency–Equality Trade-Off in Health from Stated Preferences: A Case Study in Portugal. Appl Health Econ Health Policy 16, 503–513 (2018). https://doi.org/10.1007/s40258-018-0394-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40258-018-0394-6