
Abstract
Two global epidemics, diabetes mellitus (DM) and tuberculosis (TB), have converged making their control even more challenging. We herein have reviewed metformin’s (MTF) effect on patients with active and latent TB, as well as discussed its newly discovered biological mechanisms in mycobacteria. Mounting evidence suggests that MTF provides better outcomes in TB patients, especially those with DM. The mechanisms by which MTF produces its benefits are multiple. Though metformin’s potential has been proven in patients with DM, larger and more thorough clinical trials, in DM and non-DM-TB patients, need to be conducted. MTF could be added to the arsenal of anti-TB drugs, aiding in the goal of TB eradication worldwide.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The worldwide co-epidemic of tuberculosis (TB) and diabetes mellitus (DM) is still a global health concern. Metformin (MTF) is an approved drug for the treatment of type 2 DM. Recent literature has shown the benefits of MTF in TB patients, as well as in its prevention. As our knowledge in this field keeps progressing, we here provide a comprehensive overview on the multiple effects this drug has on the host (at various levels), and in the mycobacteria.
Tuberculosis in the diabetic patient
TB continues to be one of the world’s most costly and deadly infectious diseases, with almost 25% of the human population currently infected with either latent or active TB [1]. Although the disease burden by TB has been declining, this has not occurred fast enough [2]. Type 2 DM is a complicated metabolic disorder characterized by hyperglycemia and glucose intolerance. There are many comorbidities associated with DM; one in particular is an increased risk for developing an active TB [3] and TB recurrence after preventive treatment [4]. With DM recognized as a worldwide epidemic, and TB affecting one-third of the world population, efforts in controlling both diseases appear as urgent global priorities.
Diabetic patients have a much more likelihood of developing more severe forms of TB and worsened TB outcomes after treatment [5]. TB also hinders proper glycemic control [6]. Atypical clinical presentations of TB in the diabetic patient [7, 8], along with impaired drug clearance [9], an increased risk of drug resistance, lower exposure to anti-tuberculosis drugs, treatment failure, and recurrent TB, make diagnosis and treatment challenging.
A recent cross-sectional study aimed to study the prevalence of latent TB in DM patients found that not only this was close to 30%, but that age > 60 years, any comorbidity and ischemic heart disease were associated with latent TB, while the use of MTF was inversely correlated with it [10].
Metformin in anti-tuberculous treatment
Derived from the legume Galega officinalis, MTF is an insulin sensitizer medication that is used predominantly in the treatment of type 2 DM [11]. MTF exerts its primary effect at the molecular level as a reversible inhibitor of nicotinamide dinucleotide (NADH) dehydrogenase activity of the respiratory chain, resulting in suppression of ATP production [12, 13]. AMP-activated protein kinase is one of the key molecules by which MTF exerts its pleiotropic effects [14].
MTF is the first drug of choice for lowering glucose in diabetic patients with tuberculosis. It lacks clinically meaningful interactions with rifampicin, does not have a risk of hypoglycemia, and provides important cardiovascular benefits [15].
Fairly recent epidemiological studies have shown that MTF decreases the risk of developing active TB. In a nationwide study from Taiwan, this decreased risk was directly proportional to the MTF dosages in a comparison group of low versus high users [16]. A large retrospective cohort, also from Taiwan, showed that MTF use was associated with a reduced risk of developing TB in a dose pattern in patients with type 2 DM [17]. A large 12-year longitudinal cohort study, also from Taiwan, found that MTF use was an independent factor for predicting a reduced risk of active TB, after adjusting for comorbidities, diabetes complications, oral anti-diabetic therapy type and statin use [18].
A few studies on the usefulness of MTF in anti-TB therapy have recently been published (Table 1). A case–control study from India found that poor glycemic control is a risk factor for TB occurrence, and MTF has a protective effect against TB in diabetic patients [19]. A retrospective study from China sought to investigate whether MTF exhibited more efficacy in combination with anti-TB regimens for DM-TB patients and found a higher proportion of treatment success in the MTF group, as well as lower relapse rates as compared to the non-metformin group [20]. Two studies from Indonesia have shown that adding MTF to the intensive phase of anti-TB therapy leads to sputum smear reversion [21, 22]. A smaller retrospective study from South Korea did not find an effect of MET on sputum culture conversion or recurrence after 1 year, but found improvement in the sputum conversion rate in patients with cavitary pulmonary TB [23]. Most importantly, MTF may reduce mortality in diabetic patients. A retrospective cohort study from Taiwan showed that DM poses an increased risk of adverse TB treatment outcomes and MTF can reverse mortality related with DM during TB therapy [24].
Anti-TB drugs, however, can alter MTF levels. Rifampicin increases MTF systemic exposure, possibly by increased absorption [25], without affecting its glucose-lowering efficacy [26].
Metformin against drug-resistant Mtb
Despite global efforts to control TB, the World Health Organization has estimated that 4.1% of new and 19% of previously treated TB cases in the world have rifampicin or multidrug-resistant TB [27]. Studies in a mouse model of TB have shown that MTF decreases the bacillary load in vivo, reducing also lung tissue pathology [28]. It seems that MTF inhibits intracellular growth of mycobacteria by inducing mitochondrial reactive oxygen species (ROS) [28].
As mentioned above, MTF is an inhibitor of mitochondrial complex I [29]. This respiratory chain complex is similar to bacterial NADH dehydrogenase NDH-1 complex used by persister Mycobacterium tuberculosis (Mtb) phenotypes [30]. Bacterial persistence has been proposed as one of the mechanisms leading to antibiotic resistance [31] (Fig. 1). MTF could be potentially used as a combination drug with existing anti-tuberculous therapy [32]. Such adjunct therapy may even be utilized in non-diabetic individuals [33], targeting drug-tolerant Mtb [30, 34]. MTF increases reactive oxygen species and facilitates phago-lysosome fusion leading to control of growth rates of drug-resistant Mtb [28]. Inhibition of the latter is a main mechanism by which Mtb survives within macrophages [35].

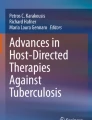
Metformin effects in mitochondria and mycobacteria. a Electron transport chain in a eukaryotic cell mitochondria. Metformin exerts its primary effect at the molecular level as a reversible inhibitor of NADH dehydrogenase activity of the respiratory chain, resulting in the suppression of ATP production. I complex I (NADH dehydrogenase), II complex II (succinate dehydrogenase), Q ubiquinone, III complex III (cytochrome bc1 complex), Cyt C cytochrome c, IV complex IV (cytochrome c oxidase). Orange arrows indicate electron flow. bM. tuberculosis cell membrane, including the electron transport chain. NDH1 complex I (NADH dehydrogenase), NADH nicotinamide adenine dinucleotide (reduced), NDH1 NADH dehydrogenase 1, SDH succinate dehydrogenase, MK menaquinone, Cyt C cytochrome c. Orange arrows indicate electron flow
Metformin in the immune response to Mtb
DM may increase the susceptibility for pulmonary TB via multiple mechanisms. Those directly related to hyperglycemia and cellular insulinopenia and the indirect effect on macrophages and lymphocytes function, lead to diminished ability to contain Mtb [36]. Monocytes and macrophages play an important role in TB immunopathogenesis [37]. DM is known to affect chemotaxis, phagocytosis, activation and antigen presentation by phagocytes in response to TB [38].
MTF increases human peripheral mononuclear cell PBMC phagocytosis of zymosan particles, with decreased cytokine production upon stimulation of Mtb lysates in vitro [39]. Despite lowering the production of inflammatory cytokines, TNF-α, IFN-γ, and IL-1β ex vivo, MTF enhances innate host defense pathways in human leukocytes, such as ROS generation [39]. AKT and mTOR are central metabolic regulators, known to influence cytokine production. MTF regulates the AKT–mTOR pathway in PBMCs in healthy volunteers [39]. In humans, MTF also downregulates type I IFN pathways [39], which are known to be associated with active TB [40]. Type I IFNs interfere with IFN-γ-mediated activation of macrophages [41, 42]. IFN-γ is in fact an indicator of successful anti-TB treatment. MTF administered along with insulin in DM patients with TB for 2 months increased their IFN-γ levels [21].
It was suggested that MTF has anti-inflammatory effects that are independent of its glucose-lowering effect [43]. Soluble(s) forms of CD14 and CD163 are inflammatory markers in monocytes [44, 45] and for macrophage polarization, and they show a positive relationship with HbA1c levels [46]. These two markers, along with inflammatory C-reactive protein, decrease in TB-DM patients with MTF-containing treatment regimens [46].
Matrix metalloproteinases (MMPs) are key mediators in the pathology of TB [47]. Systemic levels of MMP-1, -2, -3, -7, -10, and -12 are significantly higher in TB-DM patients compared to TB alone or healthy controls, with the levels of MMP-1, - 2, - 3 and - 8 showing a positive relationship with bacterial burden and HbA1c levels at baseline [48]. Standard anti-TB therapy is associated with a significant reduction in the levels of MMP-1, -2, -3, -8 and -13 post-treatment [48]. Patients known to be diabetic before incident TB on MTF treatment exhibited significantly lower levels of MMP-1, -2, -3, -7, - 9 and -12 at baseline and of MMP-7 post-treatment [48]. These results suggest a protective effect of metformin in TB-DM with possible implications for its use in TB without DBM.
Conclusions
For more than half a century, MTF has proven itself as the first defense against insulin-resistant morbidities. MTF can modify the function of different biological pathways, improving the outcome of anti-TB therapy in Mtb-infected DM patients. Increasing evidences suggest that MTF participates with beneficial effects on cellular metabolic mechanisms, immune functions that are part of the innate responses to M. tuberculosis and gene transcription in Mtb itself (Fig. 2). Further research is needed to have a more complete understanding of the role of MTF in patients with DM and active TB infection. Studies should also evaluate any beneficial effect of incorporating MTF as adjunct anti-TB therapy in non-diabetic individuals [33], as well as in targeting drug-tolerant Mtb infection [30, 34].

The multiple actions of metformin in tuberculosis. Diagram showing the effects of metformin on hyperglycemia, type I interferon (IFN) downregulation, Mtb phagosomal persistence, oxidative chains, inflammatory matrix metalloproteinases (MMPs), in phago-lysosome (PL) fusion
References
Houben RM, Dodd PJ. The global burden of latent tuberculosis infection: a re-estimation using mathematical modelling. PLoS Med. 2016;13:e1002152.
World Health Organization W. Global tuberculosis report. 2018. ISBN 978-92-4-156564-6
Ruslami R, Aarnoutse RE, Alisjahbana B, van der Ven AJ, van Crevel R. Implications of the global increase of diabetes for tuberculosis control and patient care. Trop Med Int Health TM & IH. 2010;15:1289–99.
Jeon CY, Harries AD, Baker MA, Hart JE, Kapur A, Lonnroth K, et al. Bi-directional screening for tuberculosis and diabetes: a systematic review. Trop Med Int Health TM & IH. 2010;15:1300–14.
Baker MA, Harries AD, Jeon CY, Hart JE, Kapur A, Lonnroth K, et al. The impact of diabetes on tuberculosis treatment outcomes: a systematic review. BMC Med. 2011;9:81.
Jeon CY, Murray M. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. 2008;5(7):e152.
Chiang CY, Lee JJ, Chien ST, Enarson DA, Chang YC, Chen YT, et al. Glycemic control and radiographic manifestations of tuberculosis in diabetic patients. PLoS One. 2014;9:e93397.
Skowronski M, Zozulinska-Ziolkiewicz D, Barinow-Wojewodzki A. Tuberculosis and diabetes mellitus—an underappreciated association. Arch Med Sci AMS. 2014;10:1019–27.
Kang YA. Tuberculosis treatment in patients with comorbidities. Tuberc Respir Dis. 2014;76:257–60.
Leow MK, Dalan R, Chee CB, Earnest A, Chew DE, Tan AW, et al. Latent tuberculosis in patients with diabetes mellitus: prevalence, progression and public health implications. Exp Clin Endocrinol Diabetes Off J Ger Soc Endocrinol Germ Diabetes Assoc. 2014;122(9):528–32.
Viollet B, Guigas B, Sanz Garcia N, Leclerc J, Foretz M, Andreelli F. Cellular and molecular mechanisms of metformin: an overview. Clin Sci. 2012;122:253–70.
El-Mir MY, Nogueira V, Fontaine E, Averet N, Rigoulet M, Leverve X. Dimethylbiguanide inhibits cell respiration via an indirect effect targeted on the respiratory chain complex I. J Biol Chem. 2000;275:223–8.
Owen MR, Doran E, Halestrap AP. Evidence that metformin exerts its anti-diabetic effects through inhibition of complex 1 of the mitochondrial respiratory chain. Biochem J. 2000;348:607–14.
Zhou G, Myers R, Li Y, Chen Y, Shen X, Fenyk-Melody J, et al. Role of AMP-activated protein kinase in mechanism of metformin action. J Clin Investig. 2001;108:1167–74.
van Crevel R, Koesoemadinata R, Hill PC, Harries AD. Clinical management of combined tuberculosis and diabetes. Int J Tuberc Lung Dis Off J Int Union Against Tuberc Lung Dis. 2018;22:1404–10.
Lee MC, Chiang CY, Lee CH, Ho CM, Chang CH, Wang JY, et al. Metformin use is associated with a low risk of tuberculosis among newly diagnosed diabetes mellitus patients with normal renal function: a nationwide cohort study with validated diagnostic criteria. PLoS One. 2018;13:e0205807.
Tseng CH. Metformin decreases risk of tuberculosis infection in type 2 diabetes patients. J Clin Med. 2018;7(9):264.
Lin SY, Tu HP, Lu PL, Chen TC, Wang WH, Chong IW, et al. Metformin is associated with a lower risk of active tuberculosis in patients with type 2 diabetes. Respirology. 2018;23:1063–73.
Marupuru S, Senapati P, Pathadka S, Miraj SS, Unnikrishnan MK, Manu MK. Protective effect of metformin against tuberculosis infections in diabetic patients: an observational study of south Indian tertiary healthcare facility. Braz J Infect Dis Off Publ Braz Soc Infect Dis. 2017;21:312–6.
Ma Y, Pang Y, Shu W, Liu YH, Ge QP, Du J, et al. Metformin reduces the relapse rate of tuberculosis patients with diabetes mellitus: experiences from 3-year follow-up. Eur J Clin Microbiol Infect Dis Off Publ Eur Soc Clin Microbiol. 2018;37:1259–63.
Novita BD, Soediono EI, Nugraha J. Metformin associated inflammation levels regulation in type 2 diabetes mellitus-tuberculosis coinfection patients—a case report. Indian J Tuberc. 2018;65:345–9.
Novita BD, Ali M, Pranoto A, Soediono EI, Mertaniasih NM. Metformin induced autophagy in diabetes mellitus–tuberculosis co-infection patients: a case study. Indian J Tuberc. 2019;66:64–9.
Lee YJ, Han SK, Park JH, Lee JK, Kim DK, Chung HS, et al. The effect of metformin on culture conversion in tuberculosis patients with diabetes mellitus. Korean J Intern Med. 2018;33:933–40.
Degner NR, Wang JY, Golub JE, Karakousis PC. Metformin use reverses the increased mortality associated with diabetes mellitus during tuberculosis treatment. Clin Infect Dis Off Publ Infect Dis Soc Am. 2018;66:198–205.
Cho SK, Yoon JS, Lee MG, Lee DH, Lim LA, Park K, et al. Rifampin enhances the glucose-lowering effect of metformin and increases OCT1 mRNA levels in healthy participants. Clin Pharmacol Ther. 2011;89:416–21.
Te Brake LHM, Yunivita V, Livia R, Soetedjo N, van Ewijk-Beneken Kolmer E, Koenderink JB, et al. Rifampicin alters metformin plasma exposure but not blood glucose levels in diabetic tuberculosis patients. Clin Pharmacol Ther. 2018;105(3):730–7.
World Health Organization W. Drug-resistant TB: global situation. 2019. https://www.who.int/tb/areas-of-work/drug-resistant-tb/global-situation/en/
Singhal A, Jie L, Kumar P, Hong GS, Leow MK, Paleja B, et al. Metformin as adjunct antituberculosis therapy. Sci Transl Med. 2014;6(263):263ra159.
Wheaton WW, Weinberg SE, Hamanaka RB, Soberanes S, Sullivan LB, Anso E, et al. Metformin inhibits mitochondrial complex I of cancer cells to reduce tumorigenesis. eLife. 2014;3:e02242.
Vashisht R, Brahmachari SK. Metformin as a potential combination therapy with existing front-line antibiotics for tuberculosis. J Transl Med. 2015;13:83.
Balaban NQ, Merrin J, Chait R, Kowalik L, Leibler S. Bacterial persistence as a phenotypic switch. Science. 2004;305:1622–5.
Leung CC. Repurposing metformin to prevent and treat tuberculosis. Respirology. 2018;23:974–5.
Restrepo BI. Metformin: candidate host-directed therapy for tuberculosis in diabetes and non-diabetes patients. Tuberculosis. 2016;101S:S69–72.
Rayasam GV, Balganesh TS. Exploring the potential of adjunct therapy in tuberculosis. Trends Pharmacol Sci. 2015;36:506–13.
Carranza C, Chavez-Galan L. Several routes to the same destination: inhibition of phagosome-lysosome fusion by Mycobacterium tuberculosis. Am J Med Sci. 2019;357:184–94.
Koziel H, Koziel MJ. Pulmonary complications of diabetes mellitus. Pneumonia. Infect Dis Clin N Am. 1995;9:65–96.
Guirado E, Schlesinger LS, Kaplan G. Macrophages in tuberculosis: friend or foe. Semin Immunopathol. 2013;35:563–83.
Kumari P, Meena LS. Factors affecting susceptibility to Mycobacterium tuberculosis: a close view of immunological defence mechanism. Appl Biochem Biotechnol. 2014;174:2663–73.
Lachmandas E, Eckold C, Bohme J, Koeken V, Marzuki MB, Blok B, et al. Metformin alters human host responses to Mycobacterium tuberculosis in healthy subjects. J Infect Dis. 2019. https://doi.org/10.1093/infdis/jiz064.
Berry MP, Graham CM, McNab FW, Xu Z, Bloch SA, Oni T, et al. An interferon-inducible neutrophil-driven blood transcriptional signature in human tuberculosis. Nature. 2010;466:973–7.
Lienard J, Movert E, Valfridsson C, Sturegard E, Carlsson F. ESX-1 exploits type I IFN-signalling to promote a regulatory macrophage phenotype refractory to IFNgamma-mediated autophagy and growth restriction of intracellular mycobacteria. Cell Microbiol. 2016;18:1471–85.
Teles RM, Graeber TG, Krutzik SR, Montoya D, Schenk M, Lee DJ, et al. Type I interferon suppresses type II interferon-triggered human anti-mycobacterial responses. Science. 2013;339:1448–53.
Foretz M, Guigas B, Bertrand L, Pollak M, Viollet B. Metformin: from mechanisms of action to therapies. Cell Metab. 2014;20:953–66.
Moller HJ, Aerts H, Gronbaek H, Peterslund NA, Hyltoft Petersen P, Hornung N, et al. Soluble CD163: a marker molecule for monocyte/macrophage activity in disease. Scand J Clin Lab Investig Suppl. 2002;237:29–33.
Su GL, Simmons RL, Wang SC. Lipopolysaccharide binding protein participation in cellular activation by LPS. Crit Rev Immunol. 1995;15:201–14.
Kumar NP, Moideen K, Bhootra Y, Nancy A, Viswanathan V, Shruthi BS, et al. Elevated circulating levels of monocyte activation markers among tuberculosis patients with diabetes co-morbidity. Immunology. 2018;156(3):249–58.
Xu Y, Wang L, Zimmerman MD, Chen KY, Huang L, Fu DJ, et al. Matrix metalloproteinase inhibitors enhance the efficacy of frontline drugs against Mycobacterium tuberculosis. PLoS Pathog. 2018;14:e1006974.
Kumar NP, Moideen K, Viswanathan V, Shruthi BS, Sivakumar S, Menon PA, et al. Elevated levels of matrix metalloproteinases reflect severity and extent of disease in tuberculosis-diabetes co-morbidity and are predominantly reversed following standard anti-tuberculosis or metformin treatment. BMC Infect Dis. 2018;18:345.
Funding
No funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
The authors adhered to the ethical standards described in Instructions for Authors of the journal. The manuscript has not been sent for simultaneous consideration, nor has been published elsewhere.
Rights and permissions
About this article

Cite this article
Oglesby, W., Kara, A.M., Granados, H. et al. Metformin in tuberculosis: beyond control of hyperglycemia. Infection 47, 697–702 (2019). https://doi.org/10.1007/s15010-019-01322-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-019-01322-5