
Abstract
Pyoderma gangrenosum (PG) is a skin disease characterized by an unknown neutrophilic infiltration in dermis and a nonbacterial destructive ulcer. Post-operative PG is an extremely rare type that occurs around surgical sites during the immediate post-operative period. It is usually diagnosed as surgical site infection at the time of presentation. The condition rapidly worsens despite antibiotic treatment and debridement. We report on a case of post-operative PG in a 64-year-old man after radical prostatectomy. Following the operation, redness and pus from surgical site rapidly progress although repeated antibiotic therapy and debridement were performed. Although the patient received appropriate debridement and broad-spectrum antibiotic treatment, the ulcerative lesion spread surrounding drain region and the condition of the skin region deteriorated. The diagnosis of PG was made by a skin biopsy that presented only neutrophilic invasion in the dermis without vasculitis, tumor, or malignancy. Finally, the patient died of lesion progression in whole body and multiple organ dysfunction. Considering PG along with ulcers, wounds, and post-operative complications is critical for prompt diagnosis and proper treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pyoderma gangrenosum (PG) is frequently associated with systemic disease and is often confused with other skin pathergies [1, 2]. PG occurs in approximately three cases in a population of one million individuals, with over half of all cases associated with immune system disorders in an underlying systemic disease. The condition develops rapidly and forms deep ulcers. Post-operative PG is extremely rare and typically develops around surgical sites within the first 2 weeks post-operatively [3]. Therefore, it is often misdiagnosed as wound infection, and the pathergy may complicate wound debridement with rapid ulcer development [4]. This condition has clinical features analogous to infectious processes. The following report describes a case of post-operative PG in a 64-year-old man after retropubic radical prostatectomy.
Case report
A 64-year-old man with a history of hypertension was referred to our hospital with a high serum level of prostate-specific antigen (9.01 ng/ml). The patient had no medical history of immune disease such as inflammatory disease, arthritis or hematological disease. The result of a systemic prostate biopsy showed prostate cancer with a Gleason score of 7, and a clinical stage of cT2bN0M0. The patient underwent a retropubic radical prostatectomy. We treated the patient with ampicillin sulbactam for prevention of post-operative infection. The site of the surgical wound and drain insertion presented redness and produced pus in addition to prolonged fever for 4 days following surgery. Following the diagnosis of surgical site infection, antimicrobial therapy using meropenem that is a broad-spectrum antibacterial agent of the carbapenem family was initiated (Fig. 1a). Although the patient received appropriate debridement and broad-spectrum antibiotic treatment, the ulcerative lesion spread surrounding drain region and the condition of the skin region deteriorated 10 days following surgery. The patient presented kidney and liver dysfunction and was transferred to the Intensive Care Unit. Despite treatment with an additional antifungal agent and debridement, there was no improvement (Fig. 1b). Blood, urine, sputum and wound culture were negative for any pathogen. The diagnosis of PG was made by a skin biopsy that presented only neutrophilic invasion in the dermis without vasculitis, tumor, or malignancy 37 days following surgery (Fig. 2). Although treatment with 80 mg/day intravenous prednisolone was initiated, the patient died of multiple organic dysfunction due to liver, heart, and kidney dysfunction.

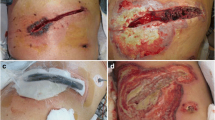
Post-operative pyoderma gangrenosum. Erythema occurred in the surgical site 4 days after radical prostatectomy (a). The skin inflammation change spread with deep erosion despite introduction of debridement. Inflammation continued to spread even 15 days following surgery (b)

Histological findings of the skin biopsy of post-operative pyoderma gangrenosum. Pathological features revealed that severe inflammatory cells, predominantly of neutrophils, infiltrated in the dermis. No bacterial components or tumor cells were observed. Hematoxylin–eosin stain ×4 (a), ×40 (b)
Discussion
Brunsting et al. [5] initially described PG as an uncommon inflammatory ulcerative skin disease. It typically occurs in the lower extremities at any age. Although approximately 50% of all cases are associated with autoimmune diseases such as inflammatory bowel disease, rheumatoid arthritis and hematological malignancy, PG is difficult to differentiate from similar etiologies, including infectious, vasculitic, drug-induced and other inflammatory dermatoses [6,7,8]. The pathophysiology of post-operative PG in particular has remained unknown, but the primary cause could be polymorphonuclear neutrophils chemotaxis following post-operative upregulation of cytokine release [9,10,11] Most cases of post-operative PG follow breast surgery or, occasionally, abdominal, gynecological or heart surgery [3]. To our knowledge, the present case was first report of post-operative PG after urological surgery.
In the present case, the other differential diagnosis we must considered was drug-induced PG [8]. The Naranjo score for determining the likelihood of whether an adverse drug reaction is actually due to the drug rather than the result of other factors. The score is one for indicating a possibility of adverse drug reaction was extremely low.
As diagnosis of PG is challenging due to the absence of laboratory findings and pathology, a definite diagnosis is determined by clinical course, ulcerative lesion, failed responsiveness to antibiotic treatment and debridement, and a skin biopsy ruling out other disease. Unfortunately, post-operative PG has often been misdiagnosed as severe surgical site infection due to similar clinical presentation. In fact, a retrospective study of 240 cases showed misdiagnosis in 95 cases [12]. Delayed diagnosis leads to deteriorating ulcerative lesions by repeated debridement and an increased mortality rate [13]. However, early intervention with steroids produces great improvement within 24 h and a reduced mortality rate that generally estimated up to 22.4% [13, 14].
Brown et al. suggested that PG was systemic disease and extracutaneous involvement might exist at the present of skin lesions [15]. 80% of the PG patients who died had an associated systemic disease, although we could not diagnose definite systematic diseases in our case. In addition, our case may have a possible correlation between infected PG wounds and poorer prognosis which has been reported in the literature [16].
As one of the main causes of pathergy was surgery, we need to consider if surgical site is worsening despite repeated debridement and broad antibiotic therapy. Although there are currently no uniformly accepted diagnostic criteria for PG, this disease is characterized by the appearance of a painful, irregular ulcer with a violaceous border. It is critical for clinicians to be aware and vigilant in diagnosing this complication as delayed diagnosis can potentially lead to poorer prognosis as our case.
References
Powell FC, Su WP, Perry HO (1996) Pyoderma gangrenosum: classification and management. J Am Acad Dermatol 34(3):395–409
Tolkachjov SN, Fahy AS, Wetter DA et al (2015) Postoperative pyoderma gangrenosum (PG): the Mayo Clinic experience of 20 years from 1994 through 2014. J Am Acad Dermatol 73(4):615–622
Zuo KJ, Fung E, Tredget EE et al (2015) A systematic review of post-surgical pyoderma gangrenosum: identification of risk factors and proposed management strategy. J Plast Reconstr Aesthet Surg 68:295–303
Tolkachjov SN, Fahy AS, Cerci FB et al (2016) Postoperative pyoderma gangrenosum: a clinical review of published cases. Mayo Clin Proc 91(9):1267–1279
Brunsting LA, Goeckerman WH, O’Leary PA (1930) Pyoderma (ecthyma) gangrenosum: clinical and experimental observations in five cases occurring in adults. Arch Derm Syphilol 22(4):655–680
Dolan OM, Burrows D, Walsh M (1997) Pyoderma gangrenosum of the breast treated with low-dose cyclosporine A. Clin Exp Dermatol 22(2):92–95
Davis MD, Alexander JL, Prawer SE (2006) Pyoderma gangrenosum of the breasts precipitated by breast surgery. J Am Acad Dermatol 55(2):317–320
Wang JY, French LE, Shear NH, Amiri A, Alavi A (2018) Drug-induced pyoderma gangrenosum: a review. Am J Clin Dermatol 19(1):67–77
Malech HL, Gallin JI (1987) Current concepts: immunology. Neutrophils in human diseases. N Engl J Med 317(11):687–694
Adachi Y, Kindzelskii AL, Cookingham G et al (1998) Aberrant neutrophil trafficking and metabolic oscillations in severe pyoderma gangrenosum. J Invest Dermatol 111(2):259–268
Oka M, Berking C, Nesbit M et al (2000) Interleukin-8 overexpression is present in pyoderma gangrenosum ulcers and leads to ulcer formation in human skin xenografts. Lab Invest 80(4):595–604
Binus AM, Qureshi AA, Li WW et al (2011) Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol 165(6):1244–1250
Langan SM, Groves RW, Card TR et al (2012) Incidence, mortality, and disease associations of pyoderma gangrenosum in the United Kingdom: a retrospective cohort study. J Invest Dermatol 132(9):2166–2170
Su WP, Davis MD, Roger H et al (2004) Pyoderma gangrenosum: clinicopathologic correlation and proposed diagnostic criteria. Int J Dermatol 43(11):790–800
Brown TS, Marshall GS, Callen JP (2000) Cavitating pulmonary infiltrate in an adolescent with pyoderma gangrenosum: a rarely recognized extracutaneous manifestation of a neutrophilic dermatosis. J Am Acad Dermatol 43(1):108–112
Ye MJ, Ye JM (2014) Pyoderma gangrenosum: a review of clinical features and outcomes of 23 cases requiring inpatient management. Dermatol Res Pract 2014:461–467
Acknowledgements
The authors wish to thank Ms. Keiko Yamamoto for her great assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Consent for publication
The case report approval was obtained from the Hospital Research Ethics Board (Approval Number: 1763).
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Osaka, A., Ide, H., Ban, S. et al. Pyoderma gangrenosum after radical prostatectomy: case report. Int Canc Conf J 7, 114–116 (2018). https://doi.org/10.1007/s13691-018-0332-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13691-018-0332-3