
Abstract
Purpose of Review
Childhood obesity is increasing substantially in many Pacific island countries and poses an urgent and serious challenge. The Sustainable Development Goals set by the United Nations and the NCD Roadmap created at the request of the Pacific Finance and Economic Ministers identify prevention and control of noncommunicable diseases as core priorities. Among the various risk factors responsible for the development of noncommunicable diseases (NCDs), overweight and obesity are particularly of concern with the potential to negate many of the health benefits that have contributed to increased life expectancy. With the increase in childhood obesity across the region, it has become apparent that surveillance data remains a challenge; however, it is essential to inform the development of effective policies and strategies to tackle the challenge of childhood obesity in the Pacific region.
Recent Findings
The paper highlights the paucity of childhood obesity surveillance data available in the Pacific region and how the absence of a standardised tool to collect this data makes it difficult to do comparative analysis between countries.
Summary
Drawing on a global protocol and identifying the gaps that currently exist in the region, the paper aims to highlight opportunities via which childhood obesity surveillance data can be improved to monitor better childhood obesity across the Pacific region.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is an increasing prevalence of overweight and obese children globally with monitored trends from 2010 to 2016 indicating that the rate has been very alarming in the Western Pacific region [1]. If the trend continues, there will be more obese than underweight children in 2022. The Western Pacific region is home to one-quarter of the world’s population covering 37 countries in the Pacific, Oceania and parts of Asia. These countries comprise high-income to low-income ones, some with exploding populations and others that are rapidly ageing. It includes China with the largest number of people with diabetes globally as well as Pacific island countries and territories (PICTs) in Oceania with the highest prevalence rates [2]. The top 10 countries with the highest prevalence of adult obesity globally can also be found in Oceania [3].
In light of the increase in global childhood obesity rates, the Commission on Ending Childhood Obesity developed a report [4] that was welcomed by the sixty-ninth World Health Assembly and asked the World Health Organization (WHO) to develop an implementation plan. Numerous discussions took place on ways to improve data collection on body mass index (BMI) for age of children—including for ages not currently monitored—and to set national targets for childhood obesity. In many countries, growth monitoring is commonly done through child health clinics, for those under 5 years of age [5]. For primary school-aged children, surveillance can include national and/or local surveys, or the measurement of all eligible children at screening or health examinations [5].
Characterising the current burden of obesity in PICTs is challenging based on a paucity of data as well as inconsistent measurement methodologies across nationally implemented health surveillance programmes and surveys [6]. In a similar vein, the availability of childhood obesity data and data collection methods vary across the region especially by body mass index (BMI) cut-off points. BMI cut-off points refer to the use of different international references to assess a child’s anthropometric status and whether they are underweight, normal, overweight or obese. These international references include the WHO growth standards [7], the International Obesity Task Force (IOTF) 2000 and 2012 references [8, 9], the French classification system and the Centers for Disease Control and Prevention (CDC) 2000 reference [10]. While the WHO 2006 standards are widely accepted as ideal for assessing anthropometric status among children aged 0–5 years across the region, there is no single, universal reference or standard for children of older ages, particularly those in the 6 to 12 age groups. Data for primary school children in the 6 to 12 age group vary considerably as BMI monitoring programmes for primary schools are routinely conducted in a small number of countries, and these are often not analysed and reported nationally due to limited capacity. Further to this, BMI cut-off references used by countries have, in many instances, been largely dependent on who is analysing the data and which funding agencies have been involved in the surveillance programmes. The cut-offs used, the inconsistent measurement methodologies and the limited analysis capacity, could lead to underestimation or overestimation of childhood overweight and obesity.
In response, there is a need to establish a standardised and systematic method of data collection to improve understanding of the progression of childhood overweight and obesity in the Pacific region. Additionally, there is a need to understand the trend and how the ongoing challenges countries are having with the NCD crisis affects the changes over time. Childhood obesity data is critical in helping countries to target interventions and to monitor impacts of activities. This paper will present an overview of the gaps in current surveillance systems in the region, highlight a childhood obesity surveillance initiative in Europe that can be adapted for the Pacific region and then discuss two key Pacific-wide platforms that have been established to address and monitor the growing childhood obesity prevalence across the Pacific region.
Childhood Obesity Surveillance in Pacific Island Countries and Territories
The prevalence of infant, childhood and adolescent obesity is increasing around the world [4]. While rates are plateauing in some settings, the Pacific region has some of the highest rates of obesity, and the increasing burden of childhood obesity has become more evident. Despite this, progress in tackling childhood obesity has been slow and inconsistent, and monitoring this growing epidemic in children has been negligent. There is a paucity of information on childhood obesity (ages 6–12) in the 22 PICTs given that most of the data in this category is either not collected or, where they are collected, are not reported nationally and the BMI cut-offs applied to child BMI national surveys across the region vary.
PICTs have undertaken a number of nationally implemented health surveillance programmes and surveys across different age categories. The WHO STEPwise approach to surveillance (STEPS) surveys used to describe overweight/obesity and diabetes in the adult population has been defined largely by age 15–64 years. Out of the 15 PICTs that have completed the survey [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25], 10 of these PICTs have sampled their adult population by the ages 15–64. Children included in the 15–17 age group have been captured in these surveys with reported BMIs applying the WHO reference standard. For the WHO Global School Based Health Surveys (GSHS) which measure and assess the behavioural risk factors and protective factors in 10 key areas among adolescents defined by the ages 13–17, the 13 PICTs that have completed this also applied the WHO standard [26,27,28,29,30,31,32,33,34,35,36,37,38]. For the Asian Development Bank (ADB) and Secretariat of the Pacific Community (SPC) supported Demographic Health Surveys (DHSs) defined by the ages of children under 5 years and adults 15 years and over, of the nine countries for which reports are available [39,40,41,42,43,44,45,46,47], 7 of these countries have applied the WHO growth reference standards, 1 applied the CDC reference standard, and 1 applied both the CDC and WHO standards in their BMI calculations and reporting. The DHSs collects information on population, health and nutrition. For the Republic of Marshall Islands Integrated Child Health and Nutrition Survey supported by UNICEF [48] and defined by the age of children under 5 years, the WHO growth reference standard was applied. In the Maternal Child and Health Program undertaken in all PICTs monitoring the growth of all children under 5 years, the BMI cut-offs applied differ. For the six US-Affiliated Pacific Islands (American Samoa, Northern Marianas, Federated States of Micronesia, Guam, Marshall Islands and Palau), the CDC standard is used. In the 3 French territories (French Polynesia, New Caledonia and Wallis and Futuna), the French classification system and the IOTF standard is used and for the remaining 13 PICTs, the WHO standard is used. For the Health Behaviour and Lifestyle of Pacific Youth Surveys (HBLPY) of adolescents’ and defined by the ages 11–17 years, 3 PICTs (Tonga, FSM and Vanuatu) undertook this and the reported BMIs applied the WHO standard [49]. In some US-Affiliated Pacific Islands, the Youth Risk Behavioural Survey (YRBS) defined by the ages 13–18 applies the CDC cut-off to measure the prevalence of overweight and obesity. The YRBS monitors six categories of health-related behaviours among adolescents including tobacco use, unhealthy dietary behaviours and physical activity. In the Children’s Healthy Living Program monitoring the prevalence of overweight and obesity in the US-Affiliated Pacific region and defined by the ages 2–8 years, the CDC cut-off was applied [50]. In all these surveys, most of the data collected and analysed have largely been for the 5 years and under and 13–17 years age categories with studies completed between 3 and 12 years ago. Most of the countries participating in these surveys have only undertaken the respective surveys once. Except for the Children’s Healthy Living Program, none of these surveys target children in the 6–12 age groups, and this remains a significant gap for the region.
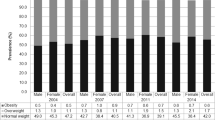
Drawing on the WHO Global School Based Health Surveys, overweight and obesity are significant problems in adolescents. The graph in Fig. 1 shows the prevalence of overweight and obesity in some PICTs. High prevalence is found in Wallis and Futuna, Tonga, Cook Islands, Tuvalu, Niue and Samoa. The Youth Risk Behavioural Survey also indicated high rates of obesity among adolescents, with about 40% in American Samoa (2011), and about 25% in Guam (2015) and the Marshall Islands (2007). For the Children’s Healthy Living Program, Novotny et al. reported an estimated prevalence of overweight and obesity for children aged 2–8 years and this increased with age [50]. At age 2 years, the estimated prevalence of OWOB years was reported at 21% and 39% at 8 years of age, increasing significantly at the age of 5 years. The proportion of obese increased from 10 at age 2 years to 23% at age 8 years, with the highest prevalence in American Samoa and Guam.

Percentage of overweight and obese 13–15 years in PICTs
WHO/Europe’s Childhood Obesity Surveillance Initiative
To undertake regular surveillance of OWOB in children, the WHO Regional Office for Europe developed the Childhood Obesity Surveillance Initiative (COSI) in 2007 [51]. With its intent to serve all countries in Europe, COSI has developed a standardised, harmonised and systematic nationally representative sampling method used by all participating countries to effectively monitor the childhood OWOB epidemic, develop targeted action and evaluate interventional effectiveness [52]. The aim of COSI is to routinely measure trends in OWOB children aged 6.0–9.9 years in primary schools to monitor the epidemic and enable inter-country comparisons via standardised measurements [53]. Rather than replacing any existing surveillance systems that countries are already using, COSI is integrated into national contexts with existing surveillance systems for health, anthropometric and dietary data. Since the implementation of COSI in 2007, WHO Europe regularly releases reports from each round of data collection [53,54,55]. WHO Europe is conducting the fifth round of COSI during the 2018–2019 school year with the participation of more than 40 out of its total 53 member states.
Current COSI Protocol
Each member state participating in COSI holds a responsibility to conduct and fund national data collection in addition to identifying an institute responsible for national coordination, while WHO Europe is responsible for preparing protocols, coordinating COSI among participating countries, analysing data at the macro-level and organising meetings for investigators. WHO Europe provides technical support for COSI implementation, training and assistance for sampling, equipment usage, and data interpretation, presentation, and usage to participating countries [53]. A scientific development group advises WHO Europe in improving survey methods and tools. Using the COSI protocol [53], there are core items that are mandatory for participating countries and optional activities which they may take up in addition to the core activities. In terms of study design, a semi-longitudinal design with repeated cross-sectional samples is expected for each data collection round at defined intervals. This will be conducted in primary schools, and each round of data collection will involve a new sample of schools. A nationally representative sample of primary schools will be selected, and these schools may remain national sentinel sites giving an overall picture of the population to be surveyed. The target population will involve primary school-aged children, and countries can collect data for different age groups in one or more of the following categories: 6.0–6.9, 7.0–7.9, 8.0–8.9 or 9.0–9.9. Cluster sampling should be used, although countries may opt for simple random sampling of primary school classes. A sample size of about 2300 children per age group should be selected. At each data collection round, the core objective is to undertake anthropometric measurements by collecting data on weight, height and body mass index (BMI) with the prevalence of underweight, normal weight, overweight and obesity calculated as well as the median and mean BMI.
Changes over time in the prevalence of overweight and obesity and mean BMI relative to the previous cohort of children of the same age range are also calculated, with some characteristics of school nutrition and physical activity environment also assessed. Other variables that need to be recorded include the child identification number, date of birth or age, sex, urbanisation grade of residence, indication of whether breakfast was eaten and date and time of measurement. Countries can also opt to measure and collect data on children’s waist and hip circumference, associated comorbid conditions, dietary intake patterns, physical activity and inactivity patterns, as well as details on the parents and the school being sampled.
COSI’s standardised and systematic sampling method should be explored as a surveillance approach for primary school children aged 6 to 12 in PICTs. The advantage of COSI is that it can be integrated into national contexts with existing surveillance systems as demonstrated for Europe. PICTs should consider developing a similar approach with the Pacific Ending Childhood Obesity Network’s priority area 4 on childhood obesity surveillance. Using COSI as a reference approach, PICTs can also consider applying a standardised alternative BMI cut-off [56] which still allows for CDC, IOTF, the French classification system and WHO cut-offs to be compared directly.
Pacific Ending Childhood Obesity Network
The Pacific Ending Childhood Obesity (ECHO) Network was established at a Regional Committee Meeting event held in October 2017 by Pacific Health Leaders in Brisbane, Australia, and endorsed at the Pacific Heads of Health Meeting in April 2018. The Network aims to provide a platform for collective advocacy and provide mutual support in implementing actions to remedy obesogenic environments and promote physical activity and obesity prevention across the region. A working group comprising of country representatives, technical agencies and a few universities in the region acted on this endorsement and met in December 2017. At this meeting, the establishment of the network was discussed further, the governance structure was explored, and three proposals for initial priorities for Pacific ECHO in the areas of physical activity, fiscal policies and restriction of marketing of unhealthy food and non-alcoholic beverages to children were considered. Childhood obesity surveillance was added as a fourth priority area in 2019.
At the inaugural member-ECHO Network meeting in February 2019 in Fiji, country representatives drafted Pacific-level action plans in the first three priority areas and agreed to implement these to complement individual country efforts. It was also anticipated that countries, with support from partner agencies, would lead the Network and allocate budgetary resources to progress these collective actions. Despite commitments made by member countries at the regional level, challenges remain in maintaining and sustaining the Pacific ECHO Network.
The Network recognises that no single intervention can halt the rise of the growing obesity epidemic. Like the NCD epidemic, addressing childhood obesity requires a whole of government approach with closer, more coordinated, multi-sectoral action and engagement between government sectors, implementing agencies and teams, civil society groups, the private sector, development partners, academic institutions, media organisations and communities. It is anticipated for the coordinated efforts to (i) coordinate policy development that are health promoting and tackle childhood obesity, including, sectors such as education, food and agriculture, commerce and industry, development, sport and recreation, communication and trade among others; (ii) implement interventions remedying obesogenic environments and promoting obesity prevention; and (iii) monitor and evaluate interventions to tackle childhood obesity. The need to strengthen government and joint action has been recognised in the WHO Commission on Ending Childhood Obesity (ECHO) [4], the Global NCD Action Plan [57] and the Decade of Action on Nutrition. These documents have outlined key proven population-based measures to address the increasing burden of childhood obesity and associated NCDs and move towards achieving the Healthy Islands vision for the Pacific which has as its first component “places where children are nurtured in body and mind”. These documents constantly emphasise the need for bolder, intensified action to halt the rise in childhood obesity, reduce mortality from NCDs significantly and end hunger and eradicate all forms of malnutrition worldwide. The recommendations in these documents call for all countries and stakeholders to align activities and programmes of intervention, monitoring and evaluation around a shared framework and timeline, and to increase the visibility, coordination and effectiveness of nutrition actions worldwide. They also ask for stronger commitment from a wide range of stakeholders including policy-makers and governments, implementing agencies and teams, civil society groups, research institutions, businesses and communities and acknowledge that such commitment does not come easily: it must be created, sustained and strengthened over time.
Pacific Monitoring Alliance for NCD Action
NCDs are the leading cause of death in most PICTs [58], accounting for approximately 70% of mortality [59] and creating an epidemic hindering the achievement of the Healthy Island Vision [60] and Sustainable Development Goals [61]. Recognising this, at the Joint Forum Economic and Health Ministers Meeting in 2014, Pacific ministers endorsed the Pacific NCD Roadmap [59] and committed to take action at both regional and national high political level. The Roadmap specifies policy and legislation measures aimed at preventing NCD and includes a listing of over 30 other multi-sectoral interventions suited to PICTs. To monitor progress against the Roadmap, the Pacific Monitoring Alliance for NCD Action (MANA) was formed, and a mutual accountability mechanism using the MANA dashboard was developed [62]. The dashboard is used to assess the status of NCD policy and legislation in PICTs. The MANA dashboard has 31 NCD indicators covering four broad categories [62]. These include areas on leadership and governance; preventive policies concerning the regulation of tobacco, alcohol, food environments and physical activity; health system response programmes including the access to NCD treatment and drugs, tobacco cessation programmes and maternal and infant nutrition interventions; and routine monitoring processes focusing on adult and adolescent risk factor surveys, child growth monitoring and NCD-related mortality. The dashboard uses a “traffic light” rating scheme to track progress where the colour red indicates no policy/action present, amber indicates policy/action under development, and green indicates policy/action in place [62].
In terms of child growth monitoring (ages 3–12) in the MANA dashboard, the “traffic light” rating scheme tracks PICT progress where the colour red indicates no growth data is collected for children of any age up to 13 years, amber indicating some childhood growth data are collected but not reported and green for childhood growth data that are collected and reported. To achieve a star rating in addition to the green colour, 2 of the items listed in the following must be met by countries: (i) data collected for more than one age/grade; (ii) dataset is available to within-country stakeholders (e.g. other ministries) for analysis; (iii) data reported at least every 2 years; (iv) training/standardisation of height and weight measurement and (v) extra risk factor data are collected (e.g. about nutrition or physical activity). To achieve a 2-star rating in addition to the green colour, 3 of the items listed must be met, and a 3-star rating is achieved when 4 of these requirements are met. Drawing on the Pacific MANA baseline assessment undertaken in 2018 [63], the 14 PICTs for which data was collected show that in 8 of these 14 PICTs, there is some childhood growth data collected but not reported, while 6 other PICTs collect and report on childhood growth data with some variations to star ratings (see Fig. 2). The majority of surveys undertaken across these 14 PICTs largely involve annual health school checks for all primary school children aged 6 to 14 years, and these include BMI data collection and monitoring programmes in schools.

Status of NCD policy and legislation in Pacific island countries and territories, 2018
In terms of child growth monitoring for PICTs, Fig. 2 highlights that only 6 out of the 14 countries that completed the 2018 baseline assessment collect and report on childhood growth data for the years 3–12. The remaining 8 countries collect some of the data, but these are not reported. In many of these countries, there are school health programmes that include the nutrition assessment of primary school students. BMI measurements are collected through these programmes; however, these are not analysed nor reported nationally and as a result are not monitored properly. Although Pacific MANA does not do any surveillance of OWOB children like COSI, it helps countries to firstly establish whether there are existing national surveys and/or surveillance programmes that are currently reporting and monitoring the growth of children. For those countries achieving the green star ratings, the child growth indicator also helps them to identify the data collected and the age/grades for which data is collected, ascertain if these datasets are available to within-country stakeholders for analysis, monitor how regularly data is reported and whether this is done at least every 2 years, identify needs for training/standardisation of height and weight measurement and ascertain whether extra risk factor data are collected (e.g. about nutrition or physical activity). For all PICTs, these five criteria act as a guide in assisting countries with monitoring their childhood growth through the development of appropriate surveys.
Conclusion
Childhood obesity monitoring and inter-country comparisons remain significant challenges for the Pacific region given the absence of a standardised and harmonised system of monitoring. The establishment of Pacific ECHO and Pacific MANA are timely platforms to actively monitor childhood obesity systematically in the region. With Pacific ECHO’s focus on obesity surveillance under its fourth strategic priority area and Pacific MANA’s focus on childhood growth monitoring under its 30th indicator, there are opportunities to tailor making COSI to suit PICTs national context. Through Pacific ECHO, PICTs should focus on developing a protocol like COSI that they can use or refer to for regular surveillance of overweight and obesity in children, particularly targeting the primary school age group as a starting point. This tool should be made available for countries to use if they do not have any current system of their own and are interested in developing a national approach. As in the case of COSI, countries that already have existing surveillance systems can integrate this new surveillance tool with their existing systems for health, anthropometric and dietary data. A robust monitoring system would not only provide more accurate trends of childhood OWOB over time, but it would also assist countries to target interventions and to monitor the impact of these activities better.
References
NCD-RisC. NCD Risk Factor Collaboration. [cited 2020 3 February]; Available from: http://www.ncdrisc.org/.
Chan JC, et al. Diabetes in the Western Pacific region--past, present and future. Diabetes Res Clin Pract. 2014;103(2):244–55.
NCD-RisC. NCD Risk Factor Collaboration. [cited 2020 24 August]; Available from: http://www.ncdrisc.org/obesity-prevalence-ranking.html.
World Health Organization, Report of the commission on ending childhood obesity. 2016, WHO: Geneva, Switzerland p 68.
World Health Organization, Overweight and obesity in the Western Pacific region: an equity perspective. 2017, World Health Organization Regional Office for the Western Pacific: Manila, Phillippines.
Hawley NL, McGarvey ST. Obesity and diabetes in Pacific islanders: the current burden and the need for urgent action. Current Diabetes Reports. 2015;15(5):1–10.
World Health Organization and United Nations Children's Fund, WHO child growth standards and the identification of severe actue malnutrition in infants and children: a joint statement. 2009, World Health Organization p 11.
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240–3.
Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ: British Medical Journal. 2007;335(7612):194–7.
Kuczmarski RJ, et al. CDC growth charts for the United States: methods and development. Vital Health Stat 11. 2000;2002(246):1–190.
World Health Organization. FSM (Chuuk) STEPS survey 2006. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2006_Micronesia_FactSheet.pdf.
World Health Organization. Kiribati STEPS survey 2015-2016. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2015-2016_Kiribati_Fact_Sheet.pdf?ua=1.
World Health Organization. Marshall Islands STEPS survey. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2002_MarshallIslands_FactSheet.pdf.
World Health Organization. Nauru STEPS survey. Fact Sheet. . Available from: https://www.who.int/ncds/surveillance/steps/2004_Nauru_FactSheet.pdf.
World Health Organization. Papua New Guinea STEPS survey 2007–2008. Fact Sheet. . [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/PapuaNewGuinea_2007-08_STEPS_FactSheet.pdf.
World Health Organization. Solomon Islands STEPS survey 2006. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2006_SolomonIslands_FactSheet.pdf.
World Health Organization. Vanuatu NCD Risk Factors STEPS report. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/Vanuatu_Fact_Sheet_2011.pdf.
World Health Organization. American Samoa STEPS survey. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2004_AmericanSamoa_FactSheet.pdf.
World Health Organization. Cook Islands NCD STEPS survey. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2004_CookIslands_FactSheet.pdf.
World Health Organization. Polynésie française enquête STEPS 2010. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2010_STEPS_Report_FP.pdf.
World Health Organization. Niue NCD Risk Factors STEPS report. . [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/Niue_STEPS_Report_2011.pdf.
World Health Organization. Samoa STEPS survey. Fact Sheet. . [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2002_Samoa_FactSheet.pdf.
World Health Organization. Tokelau STEPS survey 2005. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2005_Tokelau_FactSheet.pdf.
World Health Organization. Tonga STEPS survey 2004. Fact Sheet. [cited 2020 January 10]; Available from: https://www.who.int/ncds/surveillance/steps/2004_TongaFactSheet.pdf.
World Health Organization. Fiji Non-Communicable Diseases (NCD) STEPS survey 2002. [cited 2020 January 2010]; Available from: https://www.who.int/ncds/surveillance/steps/FijiSTEPSReport.pdf.
World Health Organization. Cook Islands Global School-based Health Survey 2015. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/2011_GSHS_FS_Cook_Islands.pdf.
World Health Organization. Fiji Global School-based Student Health Survey 2016. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/gshs_fs_fiji_2016.pdf.
World Health Organization. French Polynesia Global School-based Student Health Survey 2015. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/gshs_fs_french_polynesia_2015.pdf.
World Health Organization. Kiribati Global School-based Student Health Survey 2011. Fact Scheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/2011_GSHS_FS_Kiribati.pdf.
World Health Organization. Nauru Global School-based Student Health Survey 2011. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/Nauru_GSHS_FS_2011.pdf.
World Health Organization. Niue Global School-based Student Health Survey 2010. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/Niue_GSHS_FS_2010.pdf.
World Health Organization. Solomon Islands Global School-based Student Health Survey 2011. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/2011_GSHS_FS_Solomon_Islands.pdf.
World Health Organization. Samoa Global School-based Student Health Survey 2017. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/2017WSH_Fact_Sheet.pdf?ua=1.
World Health Organization. Tonga Global School-based Student Health Survey 2017. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/TOH2017_fact_sheet.pdf.
World Health Organization. Tuvalu Global School-based Student Health Survey 2013. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/2013_Tuvalu_Fact_Sheet.pdf.
World Health Organization. Vanuatu Global School-based Student Health Survey 2016. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/Vanuatu_2016_GSHS_FS.pdf?ua=1.
World Health Organization. Wallis and Futuna Global School-based Student Health Survey 2015. Fact Sheet. [cited 2020 January 12]; Available from: https://www.who.int/ncds/surveillance/gshs/2015_WallisFutuna_GSHS_Fact_Sheet.pdf.
World Health Organization. Tokelau Global School-based Student Health Survey 2014. Fact Sheet. [cited 2020 January 2012]; Available from: https://www.who.int/ncds/surveillance/gshs/2014-GSHS-Tokelau-fact-sheet.pdf.
Kiribati National Statistics Office, Kiribati Social Development Indicator Survey 2018–2019, Snapshot of Key Findings. 2019, National Statistics Office: South Tarawa, Kiribati.
National Statistics Office (NSO) [Papua New Guinea], ICF, Papua New Guinea Demographic and Health Survey. 2019, NSO and ICF: Port Moresby, Papua New Guinea and Rockville. USA: Maryland; 2016-2018.
Solomon Islands National Statistical Office (SINSO), Solomon Islands Ministry of Health and Medical Services (SIMoHMS), and Pacific Community (SPC), Solomon Islands Demographic and Health Survey 2015, Final Report 2017, SPC: Noumea, New Caledonia.
Samoa Census-Surveys and Demography Division, Samoa Demographic and Health Survey 2014. 2014, Samoa Bureau of Statistics: Apia, Samoa.
VNSO (Vanuatu National Statistics Office) and SPC (Secretariat of the Pacific Community), Vanuatu Demographic and Health Survey 2013. Final Report. 2014: Noumea, New Caledonia.
Economic Policy Planning and Statistics Office (EPPSO), SPC (Secretariat of the Pacific Community), and Macro International Inc., Republic of the Marshall Islands Demographic and Healthy Survey 2007. 2007: Noumea, New Caledonia.
Nauru Bureau of Statistics, SPC (Secretariat of the Pacific Community), and Macro International Inc., Nauru 2007 Demographic and Health Survey. 2007: Noumea, New Caledonia.
Tonga Department of Statistics and Tonga Ministry of Health, SPC (Secretariat of the Pacific Community), and UNFPA, Tonga Demographic and Health Survey, 2012. 2013: Noumea, New Caledonia.
Central Statistics Division (TSCD), SPC (Secretariat of the Pacific Community), and Macro International Inc., Tuvalu Demographic and Health Survey. 2007: Noumea, New Caledonia.
Republic of the Marshall Islands Ministry of Health and Human Services, RMI Economic Policy Planning and Statistics Office, and UNICEF, Republic of the Marshall Islands Integrated Child Health and Nutrition Survey 2017 Final Report. 2017, Republic of the Marshall Islands Ministry of Health and Human Services, RMI Economic, Policy Planning and Statistics Office: Majuro, Republic of the Marshall Islands.
Phongsavan P, Olatunbosun-Alakija A, Havea D, Bauman A, Smith BJ, Galea G, et al. Health behaviour and lifestyle of Pacific youth surveys: a resource for capacity building. Health Promot Int. 2005;20(3):238–48.
Novotny R, Davis J, Butel J, Boushey CJ, Fialkowski MK, Nigg CR, et al. Effect of the children’s healthy living program on young child overweight, obesity, and Acanthosis Nigricans in the US-Affiliated Pacific region: a randomized clinical trial. JAMA Netw Open. 2018;1(6):e183896.
Health and Wellbeing, Childhood Obesity Surveillance Initiative. 2018. Accessed 15 December 2019. Retrieved from https://www.hse.ie/eng/about/who/healthwellbeing/our-priority-programmes/heal/childhood-obesity-surveillance-initiativecosi/, Health and Wellbeing Division: Ireland.
World Health Organization Europe, Childhood Obesity Surveillance in the WHO European Region. Retrieved from: http://www.euro.who.int/__data/assets/pdf_file/0020/123176/FactSheet_5.pdf
World Health Organization Europe, Childhood Obesity Surveillance Initiative (COSI) Protocol. 2016, WHO: Copenhagen, Denmark.
Wijnhoven, T., J. Raaij, and J. Breda, WHO European Childhood Obesity Surveillance Initiative Implementation of round 1 (2007/2008) and round 2 (2009/2010). 2014, WHO Europe: Copenhagen, Denmark.
World Health Organization Europe, WHO European Childhood Obesity Surveillance Initiative: overweight and obesity among 6–9-year-old children. Report of the third round of data collection 2012–2013. 2018, WHO: Copenhagen, Denmark.
Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatric Obesity. 2012;7(4):284–94.
World Health Organization, Global action plan for the prevention and control of non-communicable diseases, 2013–2020. 2013, World Helath Organisation: Geneva.
World Health Organization, Noncommunicable diseases progress monitor 2017. 2017, WHO: Switzerland.
World Bank, Non-communicable disease (NCD) roadmap report. 2014, World Bank Group: Washington, DC.
World Health Organization, Eleventh Pacific Health Ministers Meeting: 2015 Yanuca Island Declaration on health in Pacific island countries and territories. 2015, WHO, SPC, Ministry of Health and Medical Services Fiji.
United Nations. Sustainable Development Goals. [cited 2019 13th November]; Available from: https://www.un.org/sustainabledevelopment/sustainable-development-goals/.
Tolley H, Snowdon W, Wate J, Durand AM, Vivili P, McCool J, et al. Monitoring and accountability for the Pacific response to the non-communicable diseases crisis. BMC Public Health. 2016;16(1):958.
The Pacific Monitoring Alliance for NCD Action (MANA). Status of non-communicable diseases policy and legislation in Pacific Island countries and territories. 2018, Pacific Community (SPC): Noumea, New Caledonia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with humans or animals performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on The Obesity Epidemic: Causes and Consequences
Rights and permissions
About this article

Cite this article
Ravuvu, A., Waqa, G. Childhood Obesity in the Pacific: Challenges and Opportunities. Curr Obes Rep 9, 462–469 (2020). https://doi.org/10.1007/s13679-020-00404-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13679-020-00404-y