
Abstract
Purpose of Review
Alopecia areata (AA) and vitiligo are dermatological autoimmune diseases that, until recently, have had no specifically targeted therapies. Here, we review the future of therapies specifically targeted to the treatment of alopecia areata and vitiligo, both of which have JAK-STAT signaling implicated in their pathogenesis.
Recent Findings
With a greater understanding of disease mechanisms and pathogenesis, we are now able to target the immune dysfunction in autoimmune diseases with more precision than topical corticosteroids and calcineurin inhibitors. Inhibition of the JAK-STAT pathway has been shown to be effective in the treatment of AA, vitiligo, and in some patients with both diseases.
Summary
In this review, we summarize the current molecular and immunological understanding of AA and vitiligo, how JAK inhibition is increasingly positioned as a new therapy for autoimmune diseases, and the future of topical JAK inhibitors in the field of dermatology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Immune-mediated dermatological diseases encompass inflammatory conditions such as atopic dermatitis and psoriasis, as well as autoimmune disorders like alopecia areata (AA) and vitiligo. As a significant physical and immunological barrier between the body and the environment, the skin is the home of complex and intricate interactions between the epithelial and immune cells. Common first-line treatments for immune-mediated dermatological conditions include topical corticosteroids, which cause blanket immunosuppression and are replete with adverse effects. In this age of directed therapies and personalized medicine, we now have a more nuanced understanding of the various components of the immune system, along with the technology to disrupt them selectively. Thus, general therapies may soon be relegated to the archives, and research and development of directed therapies are now taking center stage. One such pathway that holds promise for therapeutic targeting in dermatology is the Janus Kinase (JAK)-Signal Transduction and Activators of Transcription (STAT) pathway.
JAK-STAT Signaling
JAK-STAT signaling is a ubiquitous and pleiotropic signaling pathway that is central to controlling multiple cellular processes. JAKs form non-covalent interactions with the cytoplasmic portion of cell surface receptors for over 50 growth factors and cytokines, most of which lack an intrinsic signaling apparatus, and ligand binding results in their dimerization and trans-phosphorylation (Fig. 1). Phosphorylated JAKs recruit cytoplasmic proteins known as STATs via their Src-homology (SH2) domains. Phosphorylation of STAT proteins on a conserved C-terminal tyrosine residue leads to activation and dimerization of the STATs, and translocation to the cell nucleus where they bind to DNA elements to direct gene expression. In most eukaryotic systems, there are four different JAKs (JAK1, JAK2, JAK3, Tyk2) and seven STATs (STAT1, STAT2, STAT3, STAT4, STAT5A, STAT5B, STAT6).

Schematic of JAK-STAT signaling pathway. Specific cellular context will determine the combination of JAKs and STATs activated upon ligand binding. Recruitment of JAKs to the cytoplasmic portion of the receptor leads to auto-phosphorylation and activation, which in turn recruits and phosphorylates STAT proteins. Phosphorylated STATs translocate into the nucleus and bind to promoter sequences to enhance or repress gene expression. JAKinibs commonly used (tofacitinib, ruxolitinib) inhibit the kinase domain of the JAKs, preventing STAT protein phosphorylation and activation
JAK-STAT signaling was initially discovered as the main downstream pathway for interferon (IFN) signaling [1]. Subsequently, many other receptors have been found to employ a combination of JAKs for signaling, each system having preferential specificity for STAT proteins. Signal transduction is thus a product of the specific combination of JAKs and STATs present, and is lineage and context dependent in different cell types, leading to diverse patterns of gene expression. Details of the JAK-STAT pathway have been reviewed extensively by other authors [2•, 3].
JAK-STAT signaling is well characterized in the differentiation, maintenance, and activation of the healthy innate and adaptive immune system. JAK-STAT signaling has also been placed downstream of growth factor receptors, thus mediating cellular processes such as survival, differentiation, and proliferation in almost all cell types. In pathogenic states, constitutive or aberrant activation of JAK-STAT signaling may result in oncogenesis or dysfunction of the immune and hematopoietic system. As such, a new class of small-molecule drugs known as JAK inhibitors (JAKinibs) has been designed and developed to target these pathways. Ruxolitinib, a JAK1/JAK2 inhibitor, was the first JAKinib to be FDA approved, showing efficacy in the treatment of high-risk primary myelofibrosis [4]. Tofacitinib, a pan-JAK inhibitor, was later approved for the treatment of rheumatoid arthritis (RA) and has shown efficacy in the treatment of other immune-mediated diseases such as psoriasis, psoriatic arthritis (PsA), inflammatory bowel disease, and transplant rejection [5,6,7].
Use of JAK Inhibitors in Dermatology
Compared to corticosteroids, JAKinibs provide a greater specificity to inhibit aberrant immune responses, while avoiding non-specific adverse effects associated with corticosteroids that may or may not be immune mediated (e.g., dermal atrophy, telangiectasia). Thus, as a class of drugs, JAKinibs have the potential to be applied to many dermatological conditions, due to their ability to inhibit many of the relevant signaling pathways.
Psoriasis
Because RA and PsA were hypothesized to share similar pathogenic Th1 cytokines with psoriasis, in particular those that signal via the common γ-chain (IL-2, IL-7, IL-9, IL-15, IL-21 and IFN-γ), JAKinibs were rationalized to be effective in psoriasis. Subsequent clinical trials have shown tofacitinib (as an oral medication) to be safe and effective in psoriasis and PsA [5, 8]. In a Phase 3 randomized non-inferiority trial of tofacitinib against etanercept and placebo for psoriasis, tofacitinib at a dose of 10 mg twice daily was as effective as etanercept twice weekly [9]. In contrast to biologics, small-molecule inhibitors like the JAKinibs can be orally administered, making them far more convenient and acceptable for the patient. Tofacitinib and ruxolitinib have also been topically formulated for psoriasis and have been shown to be effective in Phase 1–2 trials [8, 10, 11]. Topical JAKinibs will further improve on convenience and adherence to treatment, while reducing the risks of systemic exposure of the drug.
Atopic Dermatitis
Tofacitinib has been shown to have significant anti-pruritic effects on a mouse model of allergic contact dermatitis when given systemically, but had additional significant antagonistic effects on local pro-inflammatory cytokines and ear thickness when used topically [12]. Oclacitinib, a JAK-1/3 inhibitor, also effective in this model, was recently approved by the FDA for veterinary in canine atopic dermatitis [13]. JTE-052, a novel pan-JAK inhibitor developed for treatment of inflammatory arthritis [14], has also been used topically to ameliorate the inflammation in a mouse model of atopic dermatitis [15] and allergic contact dermatitis (without a similar effect on croton oil-induced irritant contact dermatitis). A pilot study with six patients with moderate to severe AD showed oral tofacitinib to be effective in reducing disease severity where other treatments had failed [16]. Future studies will delineate the efficacy of JAKinibs in human AD, informing the potential therapeutic application and scope of the JAKinibs.
Pathogenesis of Alopecia Areata and Vitiligo
One of the prevailing theories surrounding the pathogenesis of AA involves the breakdown of immune privilege of the hair follicle, whereby “danger signals” in the form of MHC Class I or ULBP3 molecules are erroneously upregulated on the hair follicle [17••]. ULBP3 was identified by extensive genome-wide association studies to be a significant factor in AA pathogenesis [18••, 19], and its aberrant expression results in an attack by pathogenic CD8+ cytotoxic effector T cells that also express NKG2D, the binding ligand of ULBP3 [17••]. This leads to destruction of the hair follicle, and a non-scarring hair loss that is initially noted to start in hairless patches, and may proceed to multifocal or universal involvement of the patient’s hair-bearing skin.
Vitiligo, on the other hand, is due to a direct autoimmune attack as a result of sensitization of T cells to melanocyte autoantigens [20]. Abnormal cellular stress in melanocytes precipitated by genetic and environmental factors is believed to be a leading cause of melanocyte dysfunction [21,22,23]. This dysfunction activates innate immune inflammation and dendritic cell presentation of melanocyte autoantigens such as MART-1, gp100, tyrosinase, and tyrosinase-related proteins (TRP1 and 2) to T cells, hence sensitizing the T cells to target melanocytes for destruction, leading to depigmentation (reviewed in [24]).
While the triggering events in AA and vitiligo are likely to be distinct, both processes result in the activation of the Th1 adaptive immune response, and the recruitment of CD8+ effector T cells into the skin [25]. In AA, IFN-γ induces the production of CXCL10, which is a central chemokine in the recruitment of the effector T cells to the skin to drive alopecia. IFN-γ has been shown to be significantly upregulated in circulating PBMCs and lesional skin of AA patients [26, 27]. Likewise, IFN-γ is also a critical component of vitiligo pathogenesis [28, 29], inducing CXCL10 in lesional vitiligo skin to promote autoreactive T cell recruitment and effector function [30••]. Serum CXCL10 has been shown to correlate with disease activity in vitiligo and may be useful as a clinical biomarker in this disease [31••, 32, 33]. In the case of AA, interleukin 15 (IL-15) has also been shown to be a supporting cytokine for the CD8+ NKG2D+ T cells [17••]. Both IFN-γ and IL-15 bind to cytokine receptors that employ the common γ-chain, which in turn signals via the JAK-STAT pathway.
Current Therapies for AA and Vitiligo
Despite their considerable clinical burden, both AA and vitiligo have no FDA-approved therapies that reverse or target the disease process. Randomized controlled trials (RCTs) are rare, and those that are published are often poorly designed (usually underpowered or insufficient follow-up), and rank low on the American College of Physicians (ACP) grading system for clinical trials [34].
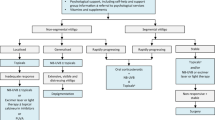
Topical corticosteroids, a mainstay of dermatological therapies, are normally first-line treatment for vitiligo. Intralesional injections of corticosteroids are generally preferred in AA, where the pathogenic immune infiltrate is deeper in the dermis [25]. Corticosteroids have a global suppressive effect on all immune cells, causing reduced cellular proliferation and attenuation of cytokine production and chemotaxis. Corticosteroids also have effects on other cell types in the skin, such as fibroblasts and keratinocytes, and their suppressive effects in these cell types lead to adverse side effects such as atrophy and skin fragility [35]. Other topical immunosuppressants include the calcineurin inhibitors (e.g., cyclosporin, tacrolimus, pimecrolimus), which disrupt the NFAT-calcineurin signaling pathway and interfere with the activation of T cells, decreasing production of IL-2. While adverse effects are less severe compared with corticosteroids, calcineurin inhibitors come with a US FDA Black Box warning for potential malignancies resulting from immunosuppression [36]. Thus, it is imperative that safer and more specific therapies are developed for dermatological conditions such as AA and vitiligo.
The era of directed therapies began with biologics, which revolutionized the treatment of immune-mediated diseases by targeting specific cytokine-receptor interactions. The most successful example is the treatment of psoriasis [37] with TNF-α (Tumor Necrosis Factor-α) inhibitors, and more recently with IL-12/23 inhibitors that target common or unique subunits (p40, and soon p19 [38]) of the cytokines produced by Th17 skewed T cells, and the upcoming biologic therapies to IL-17, the driving force for Th17 differentiation [39]. However, biologics, which are essentially proteins (either antibodies or modified receptor subunits), require parenteral administration and are potentially immunogenic with repeated exposure. While there was some genetic evidence that TNF-α might play a role in the pathogenesis of AA and vitiligo [40, 41], subsequent case reports and case studies revealed that TNF-α inhibitors were not effective in the treatment of either disease [42, 43] and, in many cases, they have been shown to precipitate disease [44,45,46]. The development of small-molecule inhibitors of multiple signaling pathways relevant to dermatological disease has undergone significant growth in the pharmaceutical industry.
Success Stories: Treatment of AA and Vitiligo with JAK Inhibitors
Recent studies on the immunopathogenesis of AA and vitiligo also uncovered a potential role for targeting the JAK-STAT pathway in these diseases. Following the work that identified the pathogenic CD8+ NKG2D+ T cells in AA, oral ruxolitinib given at a dose of 20 mg twice daily for 3 to 5 months resulted in full regrowth of hair in three patients who were previously treatment-resistant [17••]. Other JAKinibs, tofacitinib and baricitnib, were subsequently also found to be highly effective in patients with treatment-resistant AA [47, 48]. Serendipitously, one patient in a pilot study of ruxolitinib for the treatment of AA had concomitant vitiligo that also responded to treatment [31••]. This was supported by an additional case report describing the efficacy of systemic tofacitinib in the treatment of vitiligo [49•]. These findings have been confirmed in recent open-label trial of 12 patients with moderate-to-severe AA, where 75% of patients experienced at least 50% regrowth (compared to the expected rate of 12% spontaneous remission in a matched population) [50].
As a further corroboration on these findings, AA patients who had received systemic ruxolitinib for the treatment of other diseases like plaque psoriasis, essential thrombocythemia [51] and chronic mucocutaneous candidiasis [52] also were reported to have concomitant resolution of their alopecia. Further case reports confirming the efficacy of tofacitinib in the treatment of alopecia universalis also appeared in the literature [53, 54].
In a recent single-arm pilot study of tofacitinib for AA, it was noted that the starting dose of 5 mg BID was sufficient for effective hair regrowth in as soon as 4 weeks [55]. While there were no adverse events reported with the higher dose regimen in AA, topical formulations have been considered for delivery of higher concentrations of JAKinibs to the hair follicle microenvironment, so as to spare patients the potential side effects of prolonged systemic exposure, which may include immunosuppression.
The Future for Topical JAK Inhibitors in AA and Vitiligo
Targeting the JAK-STAT pathway with small-molecule inhibitors has many advantages over systemic biologic therapy. For skin diseases, higher local concentrations can be achieved with a topical formulation compared with systemic dosing so as to modulate local immune dysfunction. One of the earliest proof-of-concept studies used an intranasal topical inhibitory peptide to STAT6 to prevent Th2 differentiation in the airways in an experimental model of asthma, preventing development of allergic airway disease [56]. By avoiding systemic administration, the use of JAKinibs topically might avoid reported adverse effects such as increased risk of infections, hyperlipidemia, myelosuppression, and potential systemic malignancy.
Preclinical studies of topical ruxolitinib have shown it to be an effective modulator of the local immune response in an animal model of contact hypersensitivity [57] and have been shown to be effective for psoriasis in a small pilot study [11]. Topical 0.6% ruxolitinib cream was also recently shown to be effective in treating a case of alopecia universalis (complete loss of hair including scalp, eyebrows), and even though a larger surface of application was used in this case, there were no adverse effects on complete blood count, renal, or liver biomarkers [58]. This success has spurred several pharmaceutical companies to develop topical JAK inhibitors for AA, which are currently in Phase 1 and 2 clinical studies (please refer to www.clinicaltrials.gov for updates).
The safety profile of topical JAK inhibitors have thus been proven during these trials or other conditions. Topical tofacitinib has been shown to be efficacious and safe in both psoriasis and atopic dermatitis in Phase 2 clinical trials [10, 59]. Although there have not been any published data on the topical bioavailability of FDA-approved JAKinibs, preclinical studies on mouse skin have suggested that increased local concentrations have a more robust effect on hair regrowth in the mouse model of AA than systemic treatment [17••]. Further exploration into this effect has raised the possibility of a direct effect on hair follicle stem cells, promoting hair growth in normal mice [60]. Notably, in these studies in both AA and normal mice, topical treatment with JAKinibs only induced hair growth at the site of application, arguing against systemic absorption. In human patients using topical ruxolitinib for psoriasis, systemic JAK inhibition was ruled out by showing negligible inhibition of pSTAT3 in peripheral blood cells [61].
A recent study reported that chemokine production in the skin of a mouse model of vitiligo during disease progression predominantly originated from the keratinocytes [62•]. Selectively eliminating IFN-γ signaling only in keratinocytes abrogated disease, suggesting that specifically targeting this pathway only in the epidermis could be a highly effective treatment strategy. Thus, topical JAK inhibitors hold at least theoretical promise in the treatment of vitiligo as well. While AA and vitiligo may share certain pathogenic traits, the culprit inflammatory infiltrate is much deeper in the dermis for AA [25]. Thus, bioavailability and drug penetration may be a legitimate concern for AA to target the anatomical site of inflammation and will be addressed in preclinical and Phase 1 clinical trials.
Conclusion
Future studies of topical JAKinibs for AA and vitiligo will interrogate and open new avenues of treatment for these diseases. New formulations and subsequent generations of the JAKinibs for topical use will expand their use beyond these diseases and may also find their place in the treatment of other dermatological diseases like psoriasis, allergic and atopic skin diseases, and possibly some forms of cutaneous malignancies.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Darnell Jr JE. STATs and gene regulation. Science. 1997;277(5332):1630–5.
• O'Shea JJ, et al. The JAK-STAT pathway: impact on human disease and therapeutic intervention. Annu Rev Med. 2015;66:311–28. Excellent perspective on the JAK-STAT pathway in relation to disease pathogenesis, and summary of strategies to target this pathway therapeutically
O'Shea JJ, Plenge R. JAK and STAT signaling molecules in immunoregulation and immune-mediated disease. Immunity. 2012;36(4):542–50.
Clark JD, Flanagan ME, Telliez JB. Discovery and development of Janus kinase (JAK) inhibitors for inflammatory diseases. J Med Chem. 2014;57(12):5023–38.
Menter MA, et al. Efficacy of tofacitinib for the treatment of moderate-to-severe chronic plaque psoriasis in patient subgroups from two randomised Phase 3 trials. J Drugs Dermatol. 2016;15(5):568–80.
Sandborn WJ, et al. Tofacitinib, an oral Janus kinase inhibitor, in active ulcerative colitis. N Engl J Med. 2012;367(7):616–24.
Vincenti F, et al. Evaluation of the effect of tofacitinib exposure on outcomes in kidney transplant patients. Am J Transplant. 2015;15(6):1644–53.
Papp KA, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a Phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167(3):668–77.
Bachelez H, et al. Tofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a phase 3 randomised non-inferiority trial. Lancet. 2015;386(9993):552–61.
Ports WC, et al. A randomized phase 2a efficacy and safety trial of the topical Janus kinase inhibitor tofacitinib in the treatment of chronic plaque psoriasis. Br J Dermatol. 2013;169(1):137–45.
Punwani N, et al. Preliminary clinical activity of a topical JAK1/2 inhibitor in the treatment of psoriasis. J Am Acad Dermatol. 2012;67(4):658–64.
Fukuyama T, et al. Topically administered Janus-kinase inhibitors tofacitinib and oclacitinib display impressive antipruritic and anti-inflammatory responses in a model of allergic dermatitis. J Pharmacol Exp Ther. 2015;354(3):394–405.
Olivry T, et al. Treatment of canine atopic dermatitis: 2015 updated guidelines from the international committee on allergic diseases of animals (ICADA). BMC Vet Res. 2015;11:210.
Tanimoto A, et al. Pharmacological properties of JTE-052: a novel potent JAK inhibitor that suppresses various inflammatory responses in vitro and in vivo. Inflamm Res. 2015;64(1):41–51.
Amano W, et al. The Janus kinase inhibitor JTE-052 improves skin barrier function through suppressing signal transducer and activator of transcription 3 signaling. J Allergy Clin Immunol. 2015;136(3):667–77. e7
Levy LL, Urban J, King BA. Treatment of recalcitrant atopic dermatitis with the oral Janus kinase inhibitor tofacitinib citrate. J Am Acad Dermatol. 2015;73(3):395–9.
•• Xing L, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nat Med. 2014;20(9):1043–9. The first proof of a mechanism with information garnered from GWAS data, implicating the JAK-STAT pathway in the common effector pathways that drive CD8 NKG2D cells in AA
•• Petukhova L, et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature. 2010;466(7302):113–7. The pivotal GWAS that uncovered many possible genes associated with AA immunopathogenesis, including ULBP3 and CTLA-4
Betz RC, et al. Genome-wide meta-analysis in alopecia areata resolves HLA associations and reveals two new susceptibility loci. Nat Commun. 2015;6:5966.
Dell'Anna ML, E. K, Hamzavi I, Harris J, Parsad D, Taieb A, Picardo M. Vitiligo. Nature Reviews Disease Primers. 2015;1(1):1–16.
Kroll TM, et al. 4-Tertiary butyl phenol exposure sensitizes human melanocytes to dendritic cell-mediated killing: relevance to vitiligo. J Invest Dermatol. 2005;124(4):798–806.
van den Boorn JG, et al. Skin-depigmenting agent monobenzone induces potent T-cell autoimmunity toward pigmented cells by tyrosinase haptenation and melanosome autophagy. J Invest Dermatol. 2011;131(6):1240–51.
Toosi S, Orlow SJ, Manga P. Vitiligo-inducing phenols activate the unfolded protein response in melanocytes resulting in upregulation of IL6 and IL8. J Invest Dermatol. 2012;132(11):2601–9.
Harris JE. Cellular stress and innate inflammation in organ-specific autoimmunity: lessons learned from vitiligo. Immunol Rev. 2016;269(1):11–25.
Harris JE. Vitiligo and alopecia areata: apples and oranges? Exp Dermatol. 2013;22(12):785–9.
Sadeghi S, et al. Study of Th1/Th2 balance in peripheral blood mononuclear cells of patients with alopecia areata. Acta Microbiol Immunol Hung. 2015;62(3):275–85.
Suarez-Farinas M, et al. Alopecia areata profiling shows TH1, TH2, and IL-23 cytokine activation without parallel TH17/TH22 skewing. J Allergy Clin Immunol. 2015;136(5):1277–87.
Gregg RK, et al. Mechanisms of spatial and temporal development of autoimmune vitiligo in tyrosinase-specific TCR transgenic mice. J Immunol. 2010;184(4):1909–17.
Harris JE, et al. A mouse model of vitiligo with focused epidermal depigmentation requires IFN-gamma for autoreactive CD8(+) T-cell accumulation in the skin. J Invest Dermatol. 2012;132(7):1869–76.
•• Rashighi M, et al. CXCL10 is critical for the progression and maintenance of depigmentation in a mouse model of vitiligo. Sci Transl Med. 2014;6(223):223ra23. Study in human patients and a mouse model that implicated the IFNg-CXCL10 cytokine axis in vitligo pathogenesis and provided the rationale for targeting the JAK-STAT pathway as a treatment strategy for vitiligo
•• Harris JE, et al. Rapid skin repigmentation on oral ruxolitinib in a patient with coexistent vitiligo and alopecia areata (AA). J Am Acad Dermatol. 2016;74(2):370–1. The first striking case report that suggested a mechanistic link between AA and vitiligo, and proof of concept that JAK inhibitors will be effective for both diseases
Wang XX, et al. Increased expression of CXCR3 and its ligands in patients with vitiligo and CXCL10 as a potential clinical marker for vitiligo. Br J Dermatol. 2016;174(6):1318–26.
Rashighi M, Harris JE. Serum chemokines herald disease activity and treatment response in vitiligo patients. Br J Dermatol. 2016;174(6):1190–1.
Hordinsky M, Donati A. Alopecia areata: an evidence-based treatment update. Am J Clin Dermatol. 2014;15(3):231–46.
Oikarinen A, et al. The molecular basis of glucocorticoid-induced skin atrophy: topical glucocorticoid apparently decreases both collagen synthesis and the corresponding collagen mRNA level in human skin in vivo. Br J Dermatol. 1998;139(6):1106–10.
Ring J, Mohrenschlager M, Henkel V. The US FDA ‘black box’ warning for topical calcineurin inhibitors: an ongoing controversy. Drug Saf. 2008;31(3):185–98.
Sobell JM, Leonardi CL. Therapeutic development in psoriasis. Semin Cutan Med Surg. 2014;33(4 Suppl):S69–72.
Papp K, et al. Tildrakizumab (MK-3222), an anti-interleukin-23p19 monoclonal antibody, improves psoriasis in a phase IIb randomized placebo-controlled trial. Br J Dermatol. 2015;173(4):930–9.
Ritchlin CT, Krueger JG. New therapies for psoriasis and psoriatic arthritis. Curr Opin Rheumatol. 2016;28(3):204–10.
Redler S, et al. Investigation of selected cytokine genes suggests that IL2RA and the TNF/LTA locus are risk factors for severe alopecia areata. Br J Dermatol. 2012;167(6):1360–5.
Laddha NC, Dwivedi M, Begum R. Increased tumor necrosis factor (TNF)-alpha and its promoter polymorphisms correlate with disease progression and higher susceptibility towards vitiligo. PLoS One. 2012;7(12):e52298.
Alghamdi KM, et al. Treatment of generalized vitiligo with anti-TNF-alpha agents. J Drugs Dermatol. 2012;11(4):534–9.
Abramovits W, Losornio M. Failure of two TNF-alpha blockers to influence the course of alopecia areata. Skinmed. 2006;5(4):177–81.
Tauber M, et al. Alopecia areata occurring during anti-TNF therapy: a national multicenter prospective study. J Am Acad Dermatol. 2014;70(6):1146–9.
Maruthappu T, Leandro M, Morris SD. Deterioration of vitiligo and new onset of halo naevi observed in two patients receiving adalimumab. Dermatol Ther. 2013;26(4):370–2.
Mery-Bossard L, et al. New-onset vitiligo and progression of pre-existing vitiligo during treatment with biological agents in chronic inflammatory diseases. J Eur Acad Dermatol Venereol. 2016.
Jabbari A, et al. Reversal of alopecia areata following treatment with the JAK1/2 inhibitor baricitinib. EBioMedicine. 2015;2(4):351–5.
Jabbari A, et al. Treatment of an alopecia areata patient with tofacitinib results in regrowth of hair and changes in serum and skin biomarkers. Exp Dermatol. 2016.
• Craiglow BG, King BA. Tofacitinib citrate for the treatment of vitiligo: a pathogenesis-directed therapy. JAMA Dermatol. 2015;151(10):1110–2. First reported attempt to treat vitiligo with tofacitinib
Mackay-Wiggan J, et al. Oral ruxolitinib induces hair regrowth in patients with moderate-to-severe alopecia areata. JCI Insight. 2016;1(15):e89790. doi:10.1172/jci.insight.89790.
Pieri L, Guglielmelli P, Vannucchi AM. Ruxolitinib-induced reversal of alopecia universalis in a patient with essential thrombocythemia. Am J Hematol. 2015;90(1):82–3.
Higgins E, et al. Use of ruxolitinib to successfully treat chronic mucocutaneous candidiasis caused by gain-of-function signal transducer and activator of transcription 1 (STAT1) mutation. J Allergy Clin Immunol. 2015;135(2):551–3.
Gupta AK, Carviel JL, Abramovits W. Efficacy of tofacitinib in treatment of alopecia universalis in two patients. J Eur Acad Dermatol Venereol. 2016;30(8):1373–8.
Anzengruber F, et al. Transient efficacy of tofacitinib in alopecia areata universalis. Case Rep Dermatol. 2016;8(1):102–6.
Crispin MK, et al. Safety and efficacy of the JAK inhibitor tofacitinib citrate in patients with alopecia areata. JCI Insight. 2016;1(15):e89776. doi:10.1172/jci.insight.89776.
Wang Y, et al. Effective treatment of experimental ragweed-induced asthma with STAT-6-IP, a topically delivered cell-penetrating peptide. Clin Exp Allergy. 2011;41(11):1622–30.
Fridman JS, et al. Preclinical evaluation of local JAK1 and JAK2 inhibition in cutaneous inflammation. J Invest Dermatol. 2011;131(9):1838–44.
Craiglow BG, Tavares D, King BA. Topical ruxolitinib for the treatment of alopecia universalis. JAMA Dermatol. 2016;152(4):490–1.
Bissonnette R, et al. Topical tofacitinib for atopic dermatitis: a phase 2a randomised trial. Br J Dermatol. 2016.
Harel S, et al. Pharmacologic inhibition of JAK-STAT signaling promotes hair growth. Sci Adv. 2015;1(9):e1500973.
Punwani N, et al. Downmodulation of key inflammatory cell markers with a topical Janus kinase 1/2 inhibitor. Br J Dermatol. 2015;173(4):989–97.
• Richmond JM, et al. Keratinocyte-derived chemokines orchestrate T cell positioning in the epidermis during vitiligo and may serve as biomarkers of disease. J Invest Dermatol. 2016. Study that elegantly places the epidermal cells in the center of vitiligo pathogenesis, thus allowing it to be a suitable target for topical therapy.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of Interest
Etienne CE Wang declares no conflict of interest.
Dr. Christiano reports grants from National Institutes of Health, grants from Locks of Love Foundation, during the conduct of the study; personal fees from Aclaris Therapeutics, other from National Alopecia Areata Foundtion (NAAF), outside the submitted work. In addition, Dr. CHRISTIANO has a patent issued.
Dr. Harris reports grants and personal fees from Pfizer, grants and personal fees from Abbvie, Inc., grants and personal fees from Genzyme/Sanofi, personal fees from Concert Pharmaceuticals, grants from Stiefel/GSK, personal fees from Novartis, personal fees from Aclaris Therapeutics, Inc., grants from Celgene, outside the submitted work.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Cutaneous Drug Reactions
Rights and permissions
About this article

Cite this article
Wang, E.C.E., Harris, J.E. & Christiano, A.M. Topical JAK Inhibitors for the Treatment of Alopecia Areata and Vitiligo. Curr Derm Rep 6, 1–6 (2017). https://doi.org/10.1007/s13671-017-0163-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13671-017-0163-z