
Abstract
This study is the first to investigate whether and, if so, why Hispanics and non-Hispanic whites in the United States differ in the variability of their lifespans. Although Hispanics enjoy higher life expectancy than whites, very little is known about how lifespan variability—and thus uncertainty about length of life—differs by race/ethnicity. We use 2010 U.S. National Vital Statistics System data to calculate lifespan variance at ages 10+ for Hispanics and whites, and then decompose the Hispanic-white variance difference into cause-specific spread, allocation, and timing effects. In addition to their higher life expectancy relative to whites, Hispanics also exhibit 7 % lower lifespan variability, with a larger gap among women than men. Differences in cause-specific incidence (allocation effects) explain nearly two-thirds of Hispanics’ lower lifespan variability, mainly because of the higher mortality from suicide, accidental poisoning, and lung cancer among whites. Most of the remaining Hispanic-white variance difference is due to greater age dispersion (spread effects) in mortality from heart disease and residual causes among whites than Hispanics. Thus, the Hispanic paradox—that a socioeconomically disadvantaged population (Hispanics) enjoys a mortality advantage over a socioeconomically advantaged population (whites)—pertains to lifespan variability as well as to life expectancy. Efforts to reduce U.S. lifespan variability and simultaneously increase life expectancy, especially for whites, should target premature, young adult causes of death—in particular, suicide, accidental poisoning, and homicide. We conclude by discussing how the analysis of Hispanic-white differences in lifespan variability contributes to our understanding of the Hispanic paradox.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
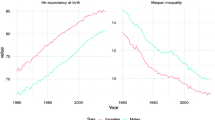
Racial and ethnic differences in mortality in the United States are wide and well established. In the 2010 U.S. life tables, Hispanic life expectancy at birth was estimated at 81.4 years; in comparison, life expectancy for non-Hispanic whites (hereafter, whites) was 2.6 years lower and life expectancy for non-Hispanic blacks (hereafter, blacks) was 6.7 years lower (Arias 2014). Hispanics exhibit higher life expectancy relative to whites despite their substantially lower socioeconomic status (SES). This pattern of higher life expectancy for Hispanics than for whites in the context of lower SES is known as the “Hispanic paradox” (Markides and Eschbach 2011) because it contests the fundamental importance of SES as a determinant of mortality differences (Baker et al. 2011; Elo 2009; Hummer and Lariscy 2011; Link and Phelan 1995). However, considering only group differences in life expectancy misses an important aspect of health inequality: group differences in lifespan variability. Life expectancy captures the central moment—the average—of the distribution of lifespans in a population and is a common summary indicator of between-group mortality disparities. Lifespan variability, on the other hand, measures the dispersion—the second moment of the distribution of lifespans—and captures within-group disparities. Comparing across population groups, higher lifespan variability reflects greater inter-individual inequality and uncertainty in length of life (Edwards and Tuljapurkar 2005; Shkolnikov et al. 2003; Wilmoth and Horiuchi 1999). Elevated lifespan variability in one population group versus another also indicates potential for public health interventions to reduce mortality inequality by averting premature mortality and presents challenges for individuals and institutions to allocate funds for retirement programs and later-life health expenses (Edwards 2013; Peltzman 2009; van Raalte et al. 2011).
If Hispanics’ higher life expectancy is accompanied by less individual variation in age at death relative to other groups, they exhibit particularly favorable longevity. Not only would Hispanics live longer, on average, but they would also do so more homogeneously across group members. Although variability in age at death has been inversely associated with life expectancy historically, research indicates that rising life expectancy does not necessarily compress variability in individual lifespans in contemporary societies. Two populations with similar mean age at death can exhibit very different dispersion around that mean (Smits and Monden 2009); and in the United States, the variability of adult lifespans is about the same now as it was in 1960, despite today’s significantly higher life expectancy (Edwards and Tuljapurkar 2005). Such findings challenge the idea that the distribution of age at death is automatically compressed by rising life expectancy so that, with respect to health disparities, the study of group differences in lifespan variability is now as strategic and important as the study of group differences in life expectancy.
This study uses 2010 U.S. National Vital Statistics System data to examine the magnitude of Hispanic-white differences in lifespan variability and their cause-specific underpinnings. We decompose the Hispanic-white difference in lifespan variance at ages 10+ into the contributions of (1) cause-specific variability in age at death (spread effect), (2) the number of deaths attributable to each cause (allocation effect), and (3) variability in cause-specific mean age at death (timing effect) (Nau and Firebaugh 2012). By integrating demographic research on lifespan variability and racial/ethnic health disparities, we aim to identify which cause and age patterns of death help explain the Hispanic paradox—one of the most persistent substantive puzzles in the field of demography.
Background
Elevated lifespan variability is consistently demonstrated among disadvantaged populations relative to their more-advantaged counterparts. For instance, researchers have shown socioeconomic differences in lifespan variability in a number of countries with SES measured with a variety of indicators, including educational attainment (Brown et al. 2012; Edwards and Tuljapurkar 2005; Shkolnikov et al. 2003; van Raalte et al. 2011, 2012), occupational class (van Raalte et al. 2014, 2015), and income (Edwards and Tuljapurkar 2005). The unequal distribution of health-enhancing socioeconomic resources across U.S. racial/ethnic groups may differentiate lifespan variability among disadvantaged minority groups relative to more socioeconomically advantaged whites. For instance, one-quarter of U.S. Hispanics and 28 % of blacks live in poverty compared with just 11 % of whites (Brown and Patten 2014). At the same time, the SES-mortality gradient is less pronounced among Hispanics than among whites (Turra and Goldman 2007). Although lifespan variability tends to be more dispersed among low-SES groups, the association may be weaker or nonexistent among Hispanics, as the Hispanic paradox would predict.
Although studies have examined racial/ethnic inequalities in mortality rates and life expectancy, examination of racial/ethnic inequalities in lifespan variability is limited. Brown et al. (2012) found that nonwhites exhibit greater variability above the modal age at death relative to whites. Similarly, Nau and Firebaugh (2012:1224) examined greater lifespan variability among Americans compared with Swedes and, among Americans, identified “nontrivial differences between whites and nonwhites in the spread, allocation, and timing effects for some specific causes.” Neither of these studies, however, examined particular nonwhite subgroups of the U.S. population.
Only a few studies to date have considered racial/ethnic differences in lifespan variability in the United States, and most of them have focused on black-white differences. Edwards and Tuljapurkar (2005) compared black-white lifespan variability (measured as the standard deviation in age at death conditional on survival to age 10, S10) using National Longitudinal Mortality Study (NLMS) data and found greater variability among blacks (S10 = 16.7 years) than among whites (S10 = 14.9 years). Lynch et al. (2003) showed that from 1972 to 1990, the greater lifespan variability among blacks became more compressed. In contrast, variability remained stagnant among whites. Most recently, Firebaugh et al. (2014) examined why lifespan variance is greater among blacks than among whites in the United States. They found that much of the variance difference between the two groups is due to greater within-cause variance among blacks relative to whites.
Despite 30 years of research on Hispanic mortality outcomes (see Markides and Eschbach 2005, 2011 for reviews), only one study to date has considered lifespan variability among Hispanics (Go et al. 1995), although the findings of this study are difficult to integrate with what is known about Hispanic-white health disparities. Using California vital statistics and census data for years 1970, 1980, and 1990, Go and colleagues examined the rectangularization of survival curves and compression of age-at-death distributions by race/ethnicity over time. Their results suggest that Hispanics in California had the lowest life expectancy as well as the largest standard deviation in age at death, and whites were characterized by much higher life expectancy and lower lifespan variability. This study serves as a benchmark for our estimates of Hispanic lifespan variability using current national-level data. One reason to be skeptical of the results of Go et al. is their finding of a substantial Hispanic disadvantage in life expectancy at birth relative to whites. For 1990, they reported a nearly 20-year life expectancy gap among males (67.1 years for white males and a mere 48.2 years among Hispanic males) and a 16-year gap among females (75.4 years among white females and 59.3 years among Hispanic females). These Hispanic life expectancy estimates are extremely low given that other studies examining Hispanic mortality in California and other southwestern states around that time found evidence of a longevity advantage of Hispanics over whites (Markides and Coreil 1986). The Hispanic-white difference in variability warrants specific focus because of persistent questions about the observed Hispanic paradox in adult mortality and because Hispanics now represent the largest U.S. minority group. Additionally, in contrast to the analysis here, Go et al. considered all-cause mortality without examining specific causes of death. Examination of racial/ethnic disparities in adult mortality by cause of death and age group is likely to provide additional insight about why lifespan variability differs for Hispanics and whites.
Although Hispanics exhibit lower age-adjusted all-cause mortality rates relative to whites,Footnote 1 patterns vary by age and cause of death. A Hispanic mortality advantage is not evident at all ages; adolescent and young adult Hispanics exhibit higher mortality risk relative to whites (Eschbach et al. 2007; Hayes-Bautista et al. 2002; Murphy et al. 2013), which (all else being equal) would produce greater variability in the lifespans of Hispanics compared with whites. Hayes-Bautista and colleagues (2002) identified the Latino adolescent male mortality peak (LAMMP) as an anomaly of the Hispanic paradox among Hispanic males in California, finding that it was limited to ages 15–24 and was primarily the result of elevated risk of homicide among Hispanics relative to whites. Eschbach and colleagues (2007) reexamined mortality risk of Hispanic young adults in California and Texas and confirmed the homicide disadvantage among both foreign-born and U.S.-born Hispanic males as well as U.S.-born Hispanic females. Mortality rates of U.S.-born Hispanics also exceeded those of whites among males for deaths attributed to alcohol use, substance use, sexually transmitted diseases, and infectious/parasitic diseases and among females for sexually transmitted disease and infectious/parasitic disease deaths. Both the Hayes-Bautista et al. (2002) and Eschbach et al. (2007) studies found significantly lower suicide mortality among Hispanics relative to whites. Recent research notes that in addition to suicide, young Hispanics have lower death rates from the emerging epidemic in accidental poisoning deaths, such as overdose from prescription or illicit drugs (Chen et al. 2014).
Beyond age 50, a Hispanic mortality advantage relative to whites clearly emerges as chronic and degenerative causes of death replace external causes as the leading underlying causes. Studies have found lower rates of cardiovascular disease and all-site cancer mortality among Hispanics compared with whites, the two causes that account for more than one-half of all U.S. deaths (Borrell and Crawford 2009; Hummer et al. 2000; Singh and Hiatt 2006; Sorlie et al. 1993). Several recent studies have identified differential smoking patterns as a critical factor shaping the Hispanic paradox. Lung cancer and respiratory disease mortality, both very strongly linked to life course patterns of tobacco use, are much lower among Hispanics than whites (Lariscy et al. 2015; Singh and Siahpush 2001). Blue and Fenelon (2011) found that Hispanics’ lower smoking prevalence accounts for about 75 % of their life expectancy advantage relative to whites beyond age 50. As among Hispanic young adults, Hispanic older adults are not advantaged for all causes of death. Hispanic older adults exhibit higher mortality rates from diabetes and cirrhosis relative to whites (Singh and Hoyert 2000), partly because of elevated levels of obesity and heavy alcohol consumption (Hummer et al. 1999). However, deaths from these underlying causes account for only a small proportion of total deaths.
In sum, Hispanics exhibit an adult mortality advantage relative to whites, although patterns vary extensively by age and cause of death. How might these differences in age and cause-of-death patterns influence Hispanic-white differences in lifespan variability? Although lower mortality at any age increases life expectancy, the sensitivity of lifespan variability to lower mortality rates depends on the age groups experiencing them. Lower mortality at younger ages decreases lifespan variability, whereas lower mortality at older ages increases variability. Separating young adult deaths from older adult deaths is a threshold age, which lies just below life expectancy in high-income, low mortality countries (Gillespie et al. 2014; van Raalte and Caswell 2013; Zhang and Vaupel 2009). The higher mortality among Hispanics relative to whites in adolescent and young adult ages (below the threshold age) could contribute to higher lifespan variability among Hispanics. At the same time, the lower mortality rate among Hispanics above the threshold age would also elevate Hispanics’ variability, all else being equal. These age patterns may increase Hispanics’ lifespan variability relative to whites, but it is currently unclear whether the patterns are substantial enough to elevate lifespan variability among Hispanics above that of whites. The Nau-Firebaugh decomposition approach provides an analytic tool for determining how cause-of-death patterns unfold throughout the adult lifespan to contribute to Hispanic-white differences in lifespan variability.
Methods
Data
We use 2010 U.S. National Vital Statistics System data. Death count data come from the 2010 U.S. Multiple Cause of Death file available from the National Center for Health Statistics (NCHS) and include all U.S. deaths during the year 2010 (NCHS 2013a). Midyear population estimates for individuals ages 0–85+ come from 2010 postcensal, bridged-race U.S. population estimate data released by the U.S. Census Bureau (NCHS 2013b). Population estimates for individuals ages 85–100+ years were provided as an NCHS special request file. A particular strength of our data is that we use 2010 postcensal data rather than intercensal data, the latter of which extrapolate population change since the most recent decennial census and tend to underestimate the Hispanic population (Passel and Cohn 2011). These data were selected because they are current, cover the entire U.S. population, include age in single years from 0 to 100+, and include detailed information regarding race/ethnicity and underlying cause of death. After dropping cases that do not meet our inclusion criteria (described in the upcoming Measures section), the final analytic data set includes 40,842,604 Hispanics and 178,263,151 whites ages 10+ in the denominators of death rates, with 139,046 Hispanic deaths and 1,956,916 white deaths in the numerators.
Measures
Race/Ethnicity
We compare lifespan variability among the two largest racial/ethnic groups in the United States: Hispanics and non-Hispanic whites. In the U.S. Census and vital statistics records, ethnicity (Hispanic or non-Hispanic) and race are separate items (OMB 1997). In our study, Hispanics can be of any race. Non-Hispanic whites are identified as non-Hispanic on the ethnicity item and white on the race item. One concern when estimating Hispanic death rates with vital statistics data is that they may be too low as a result of ethnic misclassification (Hispanics reported as non-Hispanic) on death certificates. This issue could reduce the death count in the numerator of Hispanic death rate calculations and thus bias Hispanic death rates downward and life expectancy upward. However, Arias and colleagues (2008:1) found that Hispanic ethnicity reporting on death certificates is of sufficient quality and that “adjustment for death certificate misclassification did not significantly affect minority-majority mortality differentials.” In the 2010 U.S. Hispanic life tables, Arias (2014) applied classification ratios derived from the NLMS to correct for ethnic misclassification on death certificates; results showed that Hispanics still exhibit a higher life expectancy at birth than whites. We do not adjust the data using Arias’ approach because those adjustments are for all-cause mortality and thus are not applicable for our analysis of specific causes of death. However, sensitivity analyses showed that our estimates of lifespan variability among Hispanics and whites are similar to estimates adjusted for ethnic misclassification, giving us greater confidence that our estimate of Hispanic lifespan variability is robust to ethnic misclassification.Footnote 2
Causes of Death
Underlying cause of death is classified according to the 10th revision of the International Statistical Classification of Diseases, Injuries, and Causes of Death (ICD-10). A very small number of deaths (n = 411, 0.02 % of total deaths) with missing information on underlying cause of death are excluded from the analysis. We examine the leading causes of death in the United States in 2010 as well as some less prevalent causes with notable racial/ethnic mortality differences. The 18 cause-of-death categories are heart disease, malignant neoplasms (cancer) other than of the lung, lung cancer, cerebrovascular disease, chronic lower respiratory disease, chronic liver disease and cirrhosis, homicide, suicide, accidental poisoning, other external causes, influenza/pneumonia, sexually transmitted or needle-transmitted diseases (STDs/NTDs), septicemia, other infectious diseases, diabetes, nephritis, Alzheimer’s disease, and a residual category of causes of death not elsewhere classified (N.E.C.) (see Table 3 in the appendix for ICD-10 codes).
Variance in Age at Death at Ages 10+
We measure lifespan variability as variance in life table age at death at ages 10+ years (σ 210 ). Several inequality indicators other than variance have been used to measure lifespan variability (e.g., interquartile range, Gini coefficient, life disparity index, and Theil’s index). Conclusions may depend on the indicator used due to their sensitivity to variability at different ages (Shkolnikov et al. 2003), but in most instances, these variability measures are very highly correlated (van Raalte and Caswell 2013; Wilmoth and Horiuchi 1999). Compared with the other indicators, variance is particularly well suited for additive decomposition into spread, allocation, and timing effects. Other studies of within-population variability in age at death rely on modal age at death as the central tendency indicator and the standard deviation above the modal age as the variability indicator (Brown et al. 2012; Cheung et al. 2009; Kannisto 2000). Although the modal approach is less sensitive to the age at left-truncation (Robine 2001), it primarily measures variability in mortality due to biological aging (i.e., senescence) without capturing group differences in early-life mortality, which have strong potential for influencing racial/ethnic differences in lifespan variability.
We limit the data to individuals aged 10+ years given that small differences in infant and child mortality affect variance disproportionally. Although racial/ethnic mortality differences exist in infancy and childhood (Hummer et al. 2007; Mathews and MacDorman 2013), relatively few deaths occur at these young ages, and the Hispanic-white difference is quite small. The number of life table survivors at age 10 (l 10) in our data among Hispanics (99,363) is only slightly greater than l 10 for whites (99,314). The age-at-death distribution in modern, high-income societies has a bimodal functional form, with a relatively high number of deaths in the first year of life, few deaths throughout much of childhood and early adolescence, and a gradual increase throughout adulthood to an old-age mode. Including infant and child mortality in the decomposition could inflate differences in lifespan variance through small mortality differences at very young ages (Edwards and Tuljapurkar 2005). Truncation past infant ages is therefore necessary to analyze variability in adult lifespans.
Analytic Approach
We apply the Nau-Firebaugh decomposition approach to examine differences in lifespan variability between Hispanics and whites. The decomposition process is developed and described in detail elsewhere (Nau and Firebaugh 2012; see also Firebaugh et al. 2014). Briefly, this methodology decomposes differences in lifespan variance between two populations into the contributions of differences in (1) cause-specific variability in age at death (spread effect), (2) number of deaths attributable to each cause (allocation effect), and (3) variability in cause-specific mean age at death (timing effect). To generate the necessary input for decomposition and minimize the influence of racial/ethnic differences in age structure, we construct multidecrement period life tables for Hispanic and white women and men ages 10+ years. These period-based life tables describe the mortality schedule for a synthetic cohort in which individuals experience the age- and cause-specific mortality rates of 2010.
Lifespan variance at ages 10+ is calculated as follows:
where d(x) denotes the number of life table deaths at age x; l 10 denotes the number of survivors to age 10; e 210 equals life expectancy at age 10 squared; and ω is the maximum age in our data, the open-ended 100+ age group.Footnote 3 We also calculate life expectancy at age 10 for Hispanics and whites:
The Hispanic-white difference in lifespan variance (σ 2 H − σ 2 W ) can be decomposed into four additive cause-specific terms (spread, allocation, timing, and joint effects), described and expressed mathematically as follows.
Spread Effect
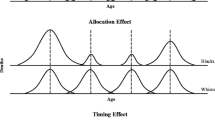
A pure spread effect would arise if two populations die from each cause at the same incidence and with the same mean age at death from each cause, but the two populations exhibit different variability in age of death for some or all causes. For instance, if deaths are more dispersed around the mean for some causes among whites than among Hispanics, then Hispanics would have lower lifespan variability due entirely to spread effects. Mathematically, using whites as the reference population, spread effects for cause c are expressed as
where σ 2 cH and σ 2 cW equal lifespan variance for cause c among Hispanics and whites, respectively; n cW equals the number of life table deaths from cause c among whites; and N equals the total number of life table deaths for each racial/ethnic group (i.e., 100,000). The formula for spread effect and all other effects are divided by N(σ 2 H − σ 2 W ) in order to express each effect as a proportion of the overall Hispanic-white difference in lifespan variability.
Allocation Effect
If Hispanics and whites experience the same cause-specific variance and mean age at death, their overall variances can still differ if one group experiences more life table deaths from causes that occur at particularly young or old ages. For example, suicide deaths tend to occur at young adult ages and are more common among whites than Hispanics. This elevated incidence of suicide deaths among whites far below the mean age at death would increase the overall variance among whites relative to Hispanics. Allocation effects for cause c are expressed as follows:
where \( \Delta {\overline{x}}_{cW}^2 \) equals the squared difference of the mean age at death from cause c for whites and the mean age at death from all causes among whites.
Timing Effect
Timing effects consist of group differences in the variability across cause-specific mean age at death. If Hispanics experience similar cause-specific incidence and variability to whites, they can still have less overall variability if their mean age at death from each cause is clustered closely together, and the mean age at death from each cause among whites diverges farther apart. Timing effects for cause c are expressed as
Joint Effect
To completely decompose the Hispanic-white difference in lifespan variability, we must include joint effects that represent allocation-spread and allocation-timing interaction terms. In our analysis, joint effects are minimal; thus, the Hispanic-white difference in lifespan variability is cleanly decomposed into spread, allocation, and timing components. Joint effects for cause c are expressed as
Results for all spread, allocation, and timing effects are multiplied by 100 so that they are expressed as percentages of the overall Hispanic-white difference in lifespan variability. Values less than 0 % and greater than 100 % are possible given that sizable negative values can offset values that exceed 100 % to constrain the total difference between lifespan variances to 100 %. In addition to presenting total cause-specific spread, allocation, timing, and joint effects, we also present effects separately by sex. Edwards and Tuljapurkar (2005) and Nau and Firebaugh (2012) found similar variability patterns for women and men, whereas Firebaugh et al. (2014) found that effects (particularly for spread) are larger for women than for men.
Results
Hispanic-White Differences in Lifespan Mean and Variability
Figure 1 plots the life table distributions of age at death (sex-combined and sex-stratified) and shows lifespan variance at ages 10+ (σ 210 ) and life expectancy at age 10 (e 10) for Hispanics and whites. Hispanics exhibit lower lifespan variance (σ 210 = 205.6) compared with whites (σ 210 = 221.5) in addition to higher life expectancy (e 10 = 72.7 years among Hispanics, and e 10 = 69.4 years among whites). In fact, the Hispanic-white disparity in lifespan variability of 7 % exceeds the 5 % disparity in life expectancy between the two groups. Visual inspection of the lifespan distributions suggests that throughout young adulthood, the number of deaths from all causes does not differ markedly between Hispanics and whites. From about age 40 onward, the Hispanic d(x) curve falls below that of whites, and then peaks at a higher modal age and at a higher number of life table deaths. Thus, the age-at-death distribution among Hispanics is more compressed than among whites.

Life table deaths from all causes among Hispanics and whites
Two important findings are observed in the sex-specific distributions (Fig. 1). First, the Hispanic-white difference in lifespan variability is larger among women than among men. Although lifespan variability is 7 % lower among Hispanics relative to whites overall, the gap is 15 % among women and 4 % among men. Second, among both Hispanics and whites, lifespan variability is lower for women relative to men. Thus, of the four racial-/ethnic-by-sex groups, Hispanic women exhibit the lowest lifespan variance, and white men exhibit the highest variance. We now turn to the decomposition results to identify the causes of death that distinguish Hispanics and whites and to determine whether spread, allocation, or timing effects are responsible for the Hispanic advantage in adult lifespan variability.
Causes of Death and Their Contribution to Lifespan Variability
The first two columns in Table 1 list the percentages of Hispanic and white deaths by cause in order of incidence among Hispanics, with the most common causes (heart disease, causes not elsewhere classified, and cancers other than lung cancer) at the top and the least common causes of death at the bottom. Total and sex-specific gross effects (presented in columns 3–5) are the sum of spread, allocation, timing, and joint effects and represent the percentage of the racial/ethnic difference in variance explained by each cause of death. The frequency of causes of death does not necessarily match their contribution to racial/ethnic group differences in lifespan variability. That is, some causes explain disproportionately more of the Hispanic-white variance difference than would be expected given their share of total deaths and are overcontributors. Other causes explain less of the difference in variance and are undercontributors.
Among cause-specific contributions to the Hispanic-white difference in variance, accidental poisoning and suicide are major overcontributors, accounting for 53.9 % and 48.2 %, respectively, of the Hispanic-white difference in lifespan variability but only 0.9 % of Hispanic deaths and 2.2 % of white deaths. Other notable overcontributors include lung cancer, lower respiratory disease, and other external causes. Note that negative gross values offset the substantial positive values for accidental poisoning, suicide, and other overcontributing causes to constrain the total of gross effects to 100 %. Four causes of death—diabetes, liver disease and cirrhosis, STDs/NTDs, and homicide—have nonnegligible negative effects on the Hispanic-white difference in lifespan variance, indicating that lifespan variance would be greater for Hispanics—not whites—if Hispanics and whites differed only with respect to those four causes. In that sense, these causes contribute negatively to (i.e., they reduce) the Hispanic advantage in lifespan variance.
The percentage of deaths from the two leading causes (heart disease and causes not elsewhere classified) roughly matches their gross contribution; these causes neither undercontribute nor overcontribute. The third and fourth most common causes of death among Hispanics—cancers (other than lung cancer) and cerebrovascular disease—undercontribute, together accounting for 21.6 % of Hispanic deaths and –12.7 % of the Hispanic-white difference in lifespan variance. Consistent with the larger lifespan variability difference among women shown in Fig. 1, the sex-specific gross contributions for all causes indicate that 69.4 % of the Hispanic-white difference in lifespan variance occurs among women. In other words, if lifespan variance did not differ between Hispanic and white men, 69.4 % of the Hispanic-white difference in lifespan variability would remain because of the higher variability among white women relative to Hispanic women.
Nau-Firebaugh Decomposition
We now examine why Hispanics exhibit lower lifespan variability relative to whites by decomposing the Hispanic-white difference in lifespan variability along both the cause-of-death and spread-allocation-timing axes. Table 2 presents cause-specific spread, allocation, and timing effects, with all-cause effect totals shown in the final row. Each value represents the percentage of the Hispanic-white difference in lifespan variability that would remain if the two groups were equalized for all other cause-specific effects except that one. Positive values indicate the percentage of the Hispanic advantage in lifespan variability that is due to a particular cause-specific spread, allocation, or timing effect. Conversely, negative values indicate cause-specific spread, allocation, or timing effects that reduce the Hispanic advantage by increasing the variance among Hispanics relative to whites.
When we decompose Hispanic-white differences in lifespan variance into spread, allocation, and timing effects, we find that the allocation effect (differences in number of deaths attributable to each cause) explains 64.4 % of the difference in variance. This allocation effect is mainly because of the greater incidence of suicide, accidental poisoning, other external causes, and lung cancer among whites. The greater incidence of suicide (Fig. 2) and accidental poisoning (Fig. 3) among whites relative to Hispanics accounts for 54.8 % and 50.9 %, respectively, of the Hispanic-white difference in lifespan variability.Footnote 4 Even though suicide and accidental poisoning deaths account for a small proportion of all deaths, their concentration in young adult ages and substantially elevated levels among whites greatly increases lifespan variability among whites vis-à-vis Hispanics. Lung cancer and chronic lower respiratory disease, causes linked to cigarette smoking, operate entirely through allocation, with no discernible spread or timing effects (Table 2). That is, Hispanics and whites exhibit similar variability in lung cancer and respiratory disease mortality (no spread effect) and roughly the same mean age at death for smoking-related causes (no timing effect), but many more whites than Hispanics die from lung cancer and respiratory disease (positive allocation effect). Together, lung cancer and chronic lower respiratory disease allocation effects account for 43 % of the Hispanic adult advantage in lifespan variability. Not all cause-specific allocation effects favor Hispanics; diabetes, homicide, heart disease, liver disease and cirrhosis, and STD/NTD mortality have sizable, negative allocation effects, indicating that the Hispanic-white difference in lifespan variability would be even greater were it not for the high incidence of mortality from these conditions among Hispanics.

Life table deaths from suicide among Hispanics and whites, by sex

Life table deaths from accidental poisoning among Hispanics and whites, by sex
After allocation effects, spread effects (cause-specific variability) are the second largest component, accounting for 26.1 % of the Hispanic advantage in adult lifespan variability. This means that cause-specific distributions tend to be more age-dispersed among whites than among Hispanics. When examining cause-specific spread effects, we find that most of the spread effect is due to deaths from heart disease (32.0 %) and causes not elsewhere classified (17.3 %), as shown in Table 2, with no other causes contributing to Hispanic-white differences in spread in a meaningful way. As with allocation effects, spread effects for some causes are negative (e.g., other cancers, cerebrovascular disease, suicide, and accidental poisoning) and therefore compress the racial/ethnic difference in lifespan variability, but they are generally small in magnitude.
In addition to presenting sex-combined cause-specific spread, allocation, and timing effects, we also present effects separately for men and women. We find some substantial sex differences in lifespan variability by race/ethnicity. As mentioned earlier, all-cause gross effects (the sum of spread, allocation, timing, and joint effects) are much larger among women than men. Figure 4 displays spread, allocation, timing and joint effects by sex. The allocation effect, which accounts for two-thirds of the overall difference in lifespan variability, operates almost exclusively among men. It’s particularly noteworthy that the seemingly negligible total timing effect (–0.1 %) conceals substantial but counterbalancing timing effects by sex. Sex-specific timing effects are 20.2 % for women and –20.3 % for men; thus, if Hispanic and white cause-specific means were equalized, the Hispanic-white difference in lifespan variability among females would close somewhat, but the Hispanic-white variability gap for men would expand.

Percentage of Hispanic-white difference in lifespan variability attributable to variance components, by sex
Figure 5 provides a visual representation of cause-specific allocation effects by sex to determine why allocation is so much more substantial among men. We focus on the allocation component because it accounts for two-thirds of the Hispanic-white difference in lifespan variability. We organize the 18 causes into four larger cause categories: chronic diseases, infectious diseases, external causes, and residual causes. Several external causes of death stand out as having important sex differences, which comes as no surprise given that men have elevated external cause mortality rates compared with women (Rogers et al. 2010; Waldron et al. 2005). For instance, we observe a large negative homicide allocation effect for men only. The male allocation effect for homicide is –22.2 %, indicating a greater incidence of homicide mortality among Hispanic men than white men, particularly through the age range of 10–40 years (Fig. 6). Homicide mortality for females is much lower than among males, and no racial/ethnic difference is apparent. Allocation effects for suicide also vary substantially by sex, with men exhibiting a larger effect (42.0 %) and women exhibiting a smaller but still noteworthy influence on Hispanic-white differences in lifespan variability (12.8 %; Fig. 2). Although not as large as the sex differences for homicide and suicide, the allocation effect for accidental poisoning is also larger for men than for women (31.8 % and 19.1 %, respectively). The all-cause female allocation effect is negligible because the large negative effects for heart disease (–23.2 %) and diabetes (–14.9 %) offset the positive effects from external causes.

Cause-specific allocation effects, by sex

Life table deaths from homicide among Hispanics and whites, by sex
Sensitivity Analysis
The sensitivity of lifespan variability to group differences in mortality rates depends on whether those differences exist above or below a threshold age. Lower death rates below the threshold age decrease lifespan variability, but lower death rates above the threshold increase variability. Our analyses have shown that the Hispanic advantage in lifespan variability is largely attributable to lower mortality rates from predominantly young adult causes. As an alternative analytic approach, we increase the index age from 10 years to 75 years to observe how our results change with a higher index age. An index age of 75 removes the influence of young adult deaths on the racial/ethnic difference in lifespan variability so that only old age deaths influence variability among Hispanics and whites.Footnote 5
When considering only older adult deaths, Hispanics continue to exhibit higher life expectancy but now have higher lifespan variability relative to whites. Life expectancy at age 75 is 14.0 and 12.1 years among Hispanics and whites, respectively, and lifespan variability above age 75 is 49.3 and 43.6 among Hispanics and whites, respectively. Here, as in other studies, higher life expectancy does not automatically mean lower lifespan variability. After we remove the influence of early adult deaths and thus exclude the higher allocation effect at early adult deaths, spread effects account for the entirety of the higher variability among older Hispanics relative to older whites (see Table S1 in Online Supplement 1). Although Hispanics exhibit higher variability than whites at older ages because of lower mortality rates above the threshold age,Footnote 6 this is more than offset by lower mortality rates among Hispanics below the threshold age to produce lower variability in adult lifespans among Hispanics relative to whites.
Discussion
Population health researchers have documented racial/ethnic disparities in life expectancy, but less attention has focused on racial/ethnic disparities in variability around that mean. Our results show that the mortality profile of U.S. Hispanics is characterized by lower lifespan variability relative to whites as well as higher life expectancy. To our knowledge, our study is the first to document a Hispanic advantage in lifespan variability among U.S. adults. The observation of less lifespan variability among Hispanics relative to whites despite Hispanics’ lower SES represents an extension of the Hispanic paradox. That is, Hispanics are socioeconomically disadvantaged relative to whites and lifespan variability is generally lower among groups with higher levels of SES compared with their socioeconomically disadvantaged counterparts (Brown et al. 2012; Edwards and Tuljapurkar 2005; van Raalte et al. 2011, 2014); yet, Hispanic adults exhibit an advantage in lifespan variability relative to white adults. We also confirm that the overall U.S. age-at-death distribution is an aggregate of different distributions for each racial/ethnic group. Hispanics exhibit a more compressed distribution than whites (as we demonstrate), and blacks exhibit the most dispersed distribution (Edwards and Tuljapurkar 2005; Firebaugh et al. 2014; Lynch et al. 2003). Thus, future reduction of U.S. lifespan variability will particularly depend upon reducing lifespan variability for blacks and whites.
Our analysis of Hispanic-white differences in lifespan variance, as opposed to conventional measures of mortality disparities such as life expectancy or mortality rates/ratios, offers numerous insights into the nature of the Hispanic adult mortality advantage. We identify the age groups and causes of death that either contribute to or detract from the Hispanic adult lifespan variability advantage. Causes with strong behavioral components that disproportionately occur at young adult ages clearly stand out. For instance, suicide and accidental poisoning contribute to Hispanics’ lower lifespan variability, whereas homicide reduces the Hispanic advantage. Although earlier research has pointed to differential smoking patterns as a key factor shaping Hispanics’ life expectancy and mortality rate advantage relative to whites (Blue and Fenelon 2011; Fenelon 2013; Lariscy et al. 2015), the current study is the first to show that Hispanics’ lower smoking prevalence also results in their favorable pattern of lower lifespan variability. The lower mortality from lung cancer and chronic lower respiratory disease among Hispanics accounts for 39 % of their lifespan variability advantage over whites.
Our emphasis on cause-specific mortality is also important because although Hispanics are advantaged on some population health dimensions (life expectancy and lifespan variability), they are disadvantaged in terms of mortality from particular causes (e.g., diabetes, cirrhosis, homicide, and sexually and needle-transmitted diseases). We find evidence consistent with the LAMMP in the homicide allocation effect (Eschbach et al. 2007; Hayes-Bautista et al. 2002). Despite elevated homicide incidence among young Hispanic men at ages far below the mean age at death, the relatively small number of homicide deaths and elevated risk of mortality among whites compared with Hispanics from several other young adult causes of death, such as suicide and accidental poisoning, more than outweigh these Hispanic young adult homicide deaths. Although Hispanics have overall lower lifespan variability relative to whites, Hispanic lifespan variability has the potential to be reduced further through a lowering of the incidence of mortality from homicide, diabetes, cirrhosis, and sexually and needle-transmitted diseases to the levels observed among whites.
Comparison With Prior Research
Our findings strongly contrast with those reported by Go et al. (1995), the only previous study to date that measured lifespan variability among U.S. Hispanics. Go and colleagues concluded that Hispanics exhibit the worst mortality profile of all the racial/ethnic groups they examined, with Hispanics exhibiting higher lifespan variability and much lower life expectancy relative to whites, blacks, and Asians/others. In contrast, our study documents a Hispanic advantage in lifespan variability relative to whites. This finding is compatible with much of the previous research demonstrating a Hispanic adult mortality advantage in more conventional population health summary indicators, such as life expectancy and mortality rates.
How does the magnitude of the Hispanic-white difference in lifespan variability compare with differences between other population subgroups? For the sake of comparison, we take the square root of our measure lifespan variance at ages 10+ to convert it to lifespan standard deviation at ages 10+, S10, the indicator that is more often reported (Edwards and Tuljapurkar 2005). The Hispanic-white S10 difference of 0.6 years \( \left(\sqrt{\upsigma_W^2}-\sqrt{\upsigma_H^2}=\sqrt{221.5}-\sqrt{205.6}=14.9-14.3\right) \) is somewhat modest relative to the 1.5-year black-white difference observed by Firebaugh et al. (2014). This is noteworthy because U.S. Hispanics and blacks are comparable in terms of socioeconomic disadvantage yet differ by more than two years in S10. Despite the favorable lifespan variability among Hispanics relative to whites in the United States, the difference between U.S. Hispanics and the country with the smallest S10 is still substantial; S10 for Sweden in 2010 was 12.5 years (authors’ calculation using Human Mortality Database data), nearly two years less than S10 for Hispanics. Even if lifespan variability of all Americans conformed to the variability of Hispanics, the United States would still rank well behind other high-income, low-mortality countries. In other words, the highly differentiated mortality patterns among U.S. racial/ethnic groups are not responsible for the elevated lifespan variability of the United States as a whole.
In their development and original application of the spread-allocation-timing decomposition method, Nau and Firebaugh (2012) found that spread effects (within-cause variability) accounted for about two-thirds of the greater lifespan variability in the United States relative to Sweden, with allocation effects (group differences in cause-specific incidence) accounting for roughly the remaining one-third. In a later application of the decomposition method to the U.S. black-white difference in lifespan variability, Firebaugh and colleagues (2014) also found that spread effects explained the majority of the greater length-of-life inequality among blacks compared with whites. The current study is the first to find that allocation effects are the primary driver of subgroup differences in lifespan variability, explaining 64 % of the Hispanic-white difference in lifespan variability. Spread effects account for 26 % of the difference, less than one-half the contribution of allocation effects. It will be interesting to see which variance components (spread, allocation, and/or timing) emerge as the main factors in further applications of the Nau-Firebaugh decomposition approach. To date, no study has found that timing effects matter very much. However, future research may identify a context in which timing effects explain lifespan variability differences between populations defined by SES, birth cohort, country, temporal period, or health behavior.
Limitations
A number of limitations must be considered when interpreting our findings. The 18 causes of death we examine in our decomposition analysis do not operate independently but rather compete against one another. Individuals who die from causes most prevalent at young adult ages are removed from the population at risk of dying from chronic and degenerative causes that occur at older adult ages. One indication of competing risks would be a correspondence between positive allocation effects for early-life causes with negative allocation effects for later-life causes (Nau and Firebaugh 2012), which is what we observe. Classification of underlying cause of death for older adults can be unreliable given that they may experience multiple contributing factors (Rosenberg 1999). Relatedly, the full mortality burden of diseases that are generally regarded as contributing factors rather than the underlying cause of death (particularly diabetes) may be understated.
Accurate documentation of Hispanic mortality patterns remains difficult given data and methodological issues (i.e., racial/ethnic misclassification, selective in- and out-migration, age misreporting, and census undercount) that potentially bias mortality estimates for U.S. minority populations (Arias 2010; Elo et al. 2004; Markides and Eschbach 2005; Palloni and Arias 2004). Hispanic life expectancy estimates using vital statistics data may be too high as a result of ethnic misclassification on death certificates (Hispanics reported as non-Hispanic) and salmon bias (Hispanic immigrants may die after returning to their country of origin and not have a U.S. death certificate). These issues reduce the death count in the numerator of Hispanic death rates and bias rates downward and life expectancy upward. We do not adjust the data using Arias’ (2010) approach because those adjustments cannot be applied to cause-specific mortality. The Hispanic mortality advantage in life expectancy and lifespan variability continues to be observed even when vital statistics data are adjusted for these issues (Arias 2014), but readers should be aware of these data quality concerns when interpreting our results.
Although we examine key age and cause-of-death patterns that influence Hispanics’ lifespan variability, other sources of heterogeneity among Hispanics cannot be observed with our data. The U.S. Hispanic population is diverse on a number of dimensions—including nativity, country or origin, duration in the United States, English language proficiency, and legal status/citizenship—and these factors differentiate the mortality experience of Hispanic subgroups (Markides and Eschbach 2011; Riosmena et al. 2014). Nativity information is not available in the public-use vital statistics data. Also, pooling foreign-born and U.S.-born Hispanics ensures a sufficient number of deaths from each cause to produce stable results from our multidecrement life table functions. Although we are unable to test for nativity differences in Hispanic lifespan variability, we speculate that lifespan variability is lower among Hispanic immigrants than among U.S.-born Hispanics given that the Hispanic mortality advantage is much more pronounced among immigrants (Lariscy et al. 2015; Markides and Eschbach 2011).
Conclusion
Lifespan variability differs by race/ethnicity among U.S. adults, with Hispanics exhibiting lower variability in addition to higher life expectancy relative to whites. Decomposition of racial/ethnic variance differences along both cause-of-death and spread-allocation-timing axes identified the sources of the Hispanic paradox in adult mortality and reveals strategies that could reduce lifespan variability for both groups. Our results suggest that this will not be a simple task and will require a multifaceted approach that addresses multiple sources of racial/ethnic mortality differences. For instance, two of the primary contributors to Hispanics’ lower dispersion relative to whites are lower incidence (allocation effects) of lung cancer, suicide, accidental poisoning, and other external causes and less variability (spread effects) in heart disease deaths. Not only do these causes have very different etiologies and age patterns, but they also contribute to overall variance through different components. In order to diminish the health inequality represented by lifespan variability among all U.S. racial/ethnic groups and, ultimately, to close the lifespan variability gap between the United States and other high-income countries, policies should focus in particular on averting premature, young adult deaths. This strategy would simultaneously increase life expectancy and decrease lifespan variability, whereas strategies aimed at extending length of life among the oldest-old increases a population’s life expectancy but at the expense of increasing lifespan variability (Gillespie et al. 2014; Kannisto 2001).
Despite Hispanics’ success in achieving higher life expectancy and lower lifespan variability relative to whites, they remain a socioeconomically disadvantaged group. Lifespan variability serves as an indicator of certainty regarding when individuals will die, which can facilitate how individuals and institutions set aside sufficient savings for retirement and later-life health expenses (Edwards 2013; Peltzman 2009). Although Hispanics have lower lifespan variability compared with whites, leading to greater certainty in when they will die, they have fewer financial resources. For instance, Hispanics earn lower wages than whites on average throughout their working lifetimes and hold less than 10 cents of wealth for every dollar of wealth held by whites (Kochar and Fry 2014). Furthermore, Hispanics live longer, on average, than whites and thus are required to stretch their much smaller level of assets over a longer period of old age. In sum, Hispanics exhibit longer lives and more certainty in how long they will live, but they possess fewer resources to sustain themselves for a longer period of old-age dependence. Research and policy attention must address closing socioeconomic disparities between Hispanics and whites so that future cohorts of Hispanics achieve long and healthy lives.
Notes
In 2010, the age-adjusted mortality rate among Hispanics (558.6 per 100,000) was 26 % lower than among whites (755.0 per 100,000) (Murphy et al. 2013).
Hispanics exhibit lower lifespan variability relative to whites by roughly the same margin regardless of whether 2010 data are adjusted for ethnic misclassification. With unadjusted data (reported in this article), variability estimates for Hispanics and whites are 205.6 and 221.5, respectively. With adjusted data (Arias 2014), variability estimates for Hispanics and whites are 201.6 and 215.3, respectively.
We include individuals in the open-ended age group 100+ in our variance estimates and assign them a value of 100.5 years. Our calculations may slightly underestimate the true variation of the mortality distribution by top-coding age at 100, although very small proportions of Hispanics and whites survive past age 100.
We present figures plotting cause-specific age-at-death distributions for the causes of death that most substantially contribute to the Hispanic-white difference in lifespan variability. Cause-specific figures for all 18 causes of death are available in Fig. S1 of Online Supplement 1.
Using the approximation of the threshold age derived by Gillespie et al. (2014), the threshold ages at age 10 are about 68 years among Hispanics and about 65 years among whites.
Age-standardized mortality rates for Hispanics and whites ages 75+ are 5,582.8 and 7,357.6 per 100,000, respectively (authors’ calculation).
References
Arias, E. (2010). United States life tables by Hispanic origin (Vital and Health Statistics Reports, Series 2, No. 152). Washington, DC: National Center for Health Statistics.
Arias, E. (2014). United States life tables, 2010 (National Vital Statistics Reports, Vol. 63, No. 7). Hyattsville, MD: National Center for Health Statistics.
Arias, E., Schauman, W. S., Eschbach, K., Sorlie, P. D., & Backlund, E. L. (2008). The validity of race and Hispanic origin reporting on death certificates in the United States (Vital and Health Statistics Reports, Series 2, No. 148). Washington, DC: National Center for Health Statistics.
Baker, D. P., Leon, J., Smith Greenaway, E. G., Collins, J., & Movit, M. (2011). The education effect on population health: A reassessment. Population and Development Review, 37, 307–332.
Blue, L., & Fenelon, A. (2011). Explaining low mortality among U.S. immigrants relative to native-born Americans: The role of smoking. International Journal of Epidemiology, 40, 786–793.
Borrell, L. N., & Crawford, N. D. (2009). All-cause mortality among Hispanics in the United States: Exploring heterogeneity by nativity status, country of origin, and race in the National Health Interview Survey-linked mortality files. Annals of Epidemiology, 19, 336–343.
Brown, A., & Patten, E. (2014). Statistical portrait of Hispanics in the United States, 2012 (Pew Research Center: Hispanic Trends report). Washington, DC: Pew Research Center. Retrieved from http://www.pewhispanic.org/2014/04/29/statistical-portrait-of-hispanics-in-the-united-states-2012/
Brown, D. C., Hayward, M. D., Montez, J. K., Hummer, R. A., Chiu, C. T., & Hidajat, M. M. (2012). The significance of education for mortality compression in the United States. Demography, 49, 819–840.
Chen, L. H., Hedegaard, H., & Warner, M. (2014). Drug-poisoning deaths involving opioid analgesics: United States, 1999–2011 (NCHS Data Brief, No. 166). Hyattsville, MD: National Center for Health Statistics.
Cheung, S. L. K., Robine, J. M., Paccaud, F., & Marazzi, A. (2009). Dissecting the compression of mortality in Switzerland, 1876–2005. Demographic Research, 21(article 19), 569–598. doi:10.4054/DemRes.2009.21.19
Edwards, R. D. (2013). The cost of uncertain life span. Journal of Population Economics, 26, 1485–1522.
Edwards, R. D., & Tuljapurkar, S. (2005). Inequality in life spans and a new perspective on mortality convergence across industrialized countries. Population and Development Review, 31, 645–674.
Elo, I. T. (2009). Social class differentials in health and mortality: Patterns and explanations in comparative perspective. Annual Review of Sociology, 35, 553–572.
Elo, I. T., Turra, C. M., Kestenbaum, B., & Ferguson, B. R. (2004). Mortality among elderly Hispanics in the United States: Past evidence and new results. Demography, 41, 109–128.
Eschbach, K., Stimpson, J. P., Kuo, Y. F., & Goodwin, J. S. (2007). Mortality of foreign-born and U.S.-born Hispanic adults at younger ages: A reexamination of recent patterns. American Journal of Public Health, 97, 1297–1304.
Fenelon, A. (2013). Revisiting the Hispanic mortality advantage in the United States: The role of smoking. Social Science & Medicine, 82, 1–9.
Firebaugh, G., Acciai, F., Noah, A. J., Prather, C., & Nau, C. (2014). Why lifespans are more variable among blacks than among whites in the United States. Demography, 51, 2025–2045.
Gillespie, D. O. S., Trotter, M. V., & Tuljapurkar, S. D. (2014). Divergence in age patterns of mortality change drives international divergence in lifespan inequality. Demography, 51, 1003–1017.
Go, C. G., Brustrom, J. E., Lynch, M. F., & Aldwin, C. M. (1995). Ethnic trends in survival curves and mortality. Gerontologist, 35, 318–326.
Hayes-Bautista, D. E., Hsu, P., Hayes-Bautista, M., Iniguez, D., Chamberlin, C. L., Rico, C., & Solorio, R. (2002). An anomaly within the Latino epidemiological paradox: The Latino adolescent male mortality peak. Archives of Pediatrics and Adolescent Medicine, 156, 480–484.
Hummer, R. A., & Lariscy, J. T. (2011). Educational attainment and adult mortality. In R. G. Rogers & E. M. Crimmins (Eds.), International handbook of adult mortality (pp. 241–262). Dordrecht, The Netherlands: Springer.
Hummer, R. A., Powers, D. A., Pullum, S. G., Gossman, G. L., & Frisbie, W. P. (2007). Paradox found (again): Infant mortality among the Mexican-origin population in the United States. Demography, 44, 441–457.
Hummer, R. A., Rogers, R. G., Amir, S. H., Forbes, D., & Frisbie, W. P. (2000). Adult mortality differentials among Hispanic subgroups and non-Hispanic whites. Social Science Quarterly, 81, 459–476.
Hummer, R. A., Rogers, R. G., Nam, C. B., & LeClere, F. B. (1999). Race/ethnicity, nativity, and U.S. adult mortality. Social Science Quarterly, 80, 136–153.
Kannisto, V. (2000). Measuring the compression of mortality. Demographic Research, 3(article 6), 1–24. doi:10.4054/DemRes.2000.3.6
Kannisto, V. (2001). Mode and dispersion of the length of life. Population: An English Selection, 13, 159–172.
Kochar, R., & Fry, R. (2014). Wealth inequality has widened along racial, ethnic lines since end of Great Recession (Pew Research Center Fact Tank report). Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2014/12/12/racial-wealth-gaps-great-recession/
Lariscy, J. T., Hummer, R. A., & Hayward, M. D. (2015). Hispanic older adult mortality in the United States: New estimates and an assessment of factors shaping the Hispanic paradox. Demography, 52, 1–14.
Link, B. G., & Phelan, J. (1995). Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 36, 80–94.
Lynch, S. M., Brown, J. S., & Harmsen, K. G. (2003). Black-white differences in mortality compression and deceleration and the mortality crossover reconsidered. Research on Aging, 25, 456–483.
Markides, K. S., & Coreil, J. (1986). The health of Hispanics in the southwestern United States: An epidemiologic paradox. Public Health Reports, 101, 253–265.
Markides, K. S., & Eschbach, K. (2005). Aging, migration, and mortality: Current status of research on the Hispanic paradox. Journals of Gerontology: Series B, 60, 68–75.
Markides, K. S., & Eschbach, K. (2011). Hispanic paradox in adult mortality in the United States. In R. G. Rogers & E. M. Crimmins (Eds.), International handbook of adult mortality (pp. 227–240). Dordrecht, The Netherlands: Springer.
Mathews, T. J., & MacDorman, M. F. (2013). Infant mortality statistics from the 2010 period linked birth/infant death data set (National Vital Statistics Reports, Vol. 62 No. 8). Hyattsville, MD: National Center for Health Statistics.
Murphy, S. L., Xu, J., & Kochanek, K. D. (2013). Deaths: Final data for 2010 (National Vital Statistics Reports, Vol. 61 No. 4). Hyattsville, MD: National Center for Health Statistics.
National Center for Health Statistics. (2013a). Mortality multiple cause files [Data files]. Hyattsville, MD: National Vital Statistics System. Retrieved from http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm
National Center for Health Statistics. (2013b). Vintage 2011 bridged-race postcensal population estimates for year 2010 [Data files]. Hyattsville, MD: National Vital Statistics System. Retrieved from http://www.cdc.gov/nchs/nvss/bridged_race/data_documentation.htm#july2010
Nau, C., & Firebaugh, G. (2012). A new method for decomposing group differences in the variability of lifespans. Demography, 49, 1207–1230.
Office of Management and Budget. (1997). Revisions to the standards for the classification of federal data on race and ethnicity (Federal register notice). Retrieved from http://www.whitehouse.gov/omb/fedreg_1997standards
Palloni, A., & Arias, E. (2004). Paradox lost: Explaining the Hispanic adult mortality advantage. Demography, 41, 385–415.
Passel, J. S., & Cohn, D. (2011). How many Hispanics? Comparing new census count with the latest census estimates (Pew Research Center: Hispanic Trends report). Washington, DC: Pew Research Center. Retrieved from http://www.pewhispanic.org/files/reports/139.pdf
Peltzman, S. (2009). Mortality inequality. Journal of Economic Perspectives, 23, 175–190.
Riosmena, F., Everett, B. G., Rogers, R. G., & Dennis, J. A. (2014). Negative acculturation and nothing more? Cumulative disadvantage and mortality during the immigrant adaptation process among Latinos in the U.S. International Migration Review, 49, 443–478.
Robine, J. M. (2001). Redefining the stages of the epidemiological transition by a study of the dispersion of life spans: The case of France. Population: An English Selection, 13, 173–193.
Rogers, R. G., Everett, B. G., Saint Onge, J. M., & Krueger, P. M. (2010). Social, behavioral, and biological factors, and sex differences in mortality. Demography, 47, 555–578.
Rosenberg, H. M. (1999). Cause of death as a contemporary problem. Journal of the History of Medicine and Allied Sciences, 54, 133–153.
Shkolnikov, V. M., Andreev, E. E., & Begun, A. Z. (2003). Gini coefficient as a life table function: Computation from discrete data, decomposition of differences and empirical examples. Demographic Research, 8(article 11), 305–358. doi:10.4054/DemRes.2003.8.11
Singh, G. K., & Hiatt, R. A. (2006). Trends and disparities in socioeconomic and behavioural characteristics, life expectancy, and cause-specific mortality of native-born and foreign-born populations in the United States, 1979–2003. International Journal of Epidemiology, 35, 903–919.
Singh, G. K., & Hoyert, D. L. (2000). Social epidemiology of chronic liver disease and cirrhosis mortality in the United States: Trends and differentials by ethnicity, socioeconomic status, and alcohol consumption. Human Biology, 72, 801–820.
Singh, G. K., & Siahpush, M. (2001). All-cause and cause-specific mortality of immigrants and native born in the United States. American Journal of Public Health, 91, 392–399.
Smits, J., & Monden, C. (2009). Length of life inequality around the globe. Social Science & Medicine, 68, 1114–1123.
Sorlie, P. D., Backlund, E. L., Johnson, N. J., & Rogot, E. (1993). Mortality by Hispanic status in the United States. Journal of the American Medical Association, 270, 2464–2468.
Turra, C. M., & Goldman, N. (2007). Socioeconomic differences in mortality among U.S. adults: Insights into the Hispanic paradox. Journals of Gerontology: Series B, 62, S184–S192.
van Raalte, A. A., & Caswell, H. (2013). Perturbation analysis of indices of lifespan variability. Demography, 50, 1615–1640.
van Raalte, A. A., Kunst, A. E., Deboosere, P., Leinsalu, M., Lundberg, O., Martikainen, P., . . . Mackenbach, J. P. (2011). More variation in lifespan in lower education groups: Evidence from 10 European countries. International Journal of Epidemiology, 40, 1703–1714.
van Raalte, A. A., Kunst, A. E., Lundberg, O., Leinsalu, M., Martikainen, P., Artnik, B., . . . Mackenbach, J. P. (2012). The contribution of educational inequalities to lifespan variation. Population Health Metrics, 10, 1–10.
van Raalte, A. A., Martikainen, P., & Myrskylä, M. (2014). Lifespan variation by occupational class: Compression or stagnation over time? Demography, 51, 73–95.
van Raalte, A. A., Myrskylä, M., & Martikainen, P. (2015). The role of smoking on mortality compression: An analysis of Finnish occupational social classes, 1971–2007. Demographic Research, 32(article 20), 589–620. doi:10.4054/DemRes.2015.32.20
Waldron, I., McCloskey, C., & Earle, I. (2005). Trends in gender differences in accidents mortality: Relationships to changing gender roles and other societal trends. Demographic Research, 13(article 17), 415–454. doi:10.4054/DemRes.2005.13.17
Wilmoth, J. R., & Horiuchi, S. (1999). Rectangularization revisited: Variability of age at death within human populations. Demography, 36, 475–495.
Zhang, Z., & Vaupel, J. W. (2009). The age separating early deaths from late deaths. Demographic Research, 20(article 29), 721–730. doi:10.4054/DemRes.2009.20.29
Acknowledgments
An earlier draft of this article was presented at the 2013 Population Association of America meeting in New Orleans, LA. We would like to thank Vladimir Canudas-Romo for his thoughtful comments and the National Center for Health Statistics for providing a special request data file. Research for this article was supported by training grants from the National Institute of Child Health and Human Development (5 T32 HD007081) and the National Institute on Aging (5 T32 AG000139). We are grateful to the Carolina Population Center and its NIH center grant (2 P2C HD050924-11) for general support.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Lariscy, J.T., Nau, C., Firebaugh, G. et al. Hispanic-White Differences in Lifespan Variability in the United States. Demography 53, 215–239 (2016). https://doi.org/10.1007/s13524-015-0450-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13524-015-0450-x