
Abstract
Objectives
To study the expression of CD14 + CD16 + monocytes and VEGF and the levels of serum adiponectin and MCP-1 in peripheral blood of patients with type 2 diabetes mellitus (T2DM) and diabetic macroangiopathy to understand the possible mechanism of inflammatory immune response in T2DM and diabetic macroangiopathy.
Methods
Peripheral blood CD14 + CD16 + monocytes were detected by flow cytometry in 50 T2DM patients, 50 patients with diabetic macroangiopathy, and 20 healthy controls or normal controls who participated in outpatient physical examination, and used the Ficoll-Hypaque density gradient centrifugation isolated PBMC and quantitative PCR technology comparison between groups research object in the peripheral blood PBMC VEGF mRNA expression level. Serum levels of adiponectin and MCP-1 were measured by ELISA.
Results
Compared with normal control group (NGT), the fluorescence intensity of proinflammatory CD14 + CD16 + monocytes in simple T2DM group and T2DM combined with macroangiopathy group were significantly increased (p < 0.05), and T2DM combined with macroangiopathy group was significantly higher than T2DM group, the difference was statistically significant (p < 0.01). Moreover, the expression of VEGF mRNA in peripheral blood PBMCs, T2DM combined with macroangiopathy> T2DM patients> healthy volunteers, the differences were significant (p < 0.05). Compared with NGT group, the levels of serum adiponectin in T2DM group and T2DM combined with macroangiopathy group were significantly lower than those in NGT group (p < 0.01), and the levels of serum adiponectin, simple T2DM Group were lower than T2DM combined with macroangiopathy group (p < 0.05). The level of MCP-1 in serum compared with simple T2DM group and NGT group, T2DM combined with macroangiopathy group had statistically significant difference (p < 0.05). The serum level of MCP-1 in T2DM group was also higher than that in NGT group (p < 0.05). At the same time, we also found that the increase of CD14 + CD16 + monocytes was positively correlated with serum MCP-1 levels.
Conclusions
T2DM patients and T2DM combined with macroangiopathy patients have increased expression of VEGF and MCP-1 concentration in peripheral blood mononuclear cells. The increase of MCP-1 may increase the number of CD14 + CD16 + monocytes, which is involved in the chronic inflammation in patients with T2DM and T2DM combined with macroangiopathy, resulting in the occurrence and development of T2DM and its complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
CD14 + CD16 + monocytes are considered to be a subset of proinflammatory monocytes. Our previous studies have found that in cytokine-mediated chronic low-grade inflammatory response in patients with type 2 diabetes mellitus (T2DM) and diabetic kidney disease (DKD), non-specific immune system activation participates in the occurrence and development of T2DM and its complications [1, 2]. In patients with diabetes mellitus and macrovascular disease, the expression of CD14 + CD16 + in chronic low-grade inflammation is rarely reported. Our purpose is to study the expression of CD14 + CD16 + monocytes and VEGF and the concentration of MCP-1 in peripheral blood in patients with T2DM and diabetic macroangiopathy to understand the possible mechanism of nonspecific inflammatory immune response in T2DM and diabetic macroangiopathy.
Subjects and methods
Research objects
From September 2012 to October 2014, all the newly diagnosed T2DM patients and normal glucose-regulated patients in the Affiliated Hospital of Zunyi Medical University of Guizhou Province received 75 g oral glucose tolerance test (OGTT). A total of 120 patients were enrolled, including 50 T2DM patients, 50 T2DM patients complicated with macrovascular disease, and 20 healthy controls or normal controls who participated in outpatient physical examination. T2DM diagnosis is in line with the 1999 World Health Organization (WHO) Diabetes Diagnostic and Classification Criteria and excludes the following: (1) a history of diabetes and hypoglycemic agents, (2) type 1 diabetes, gestational diabetes, and special types of diabetes, (3) acute complications of diabetes (e.g., diabetic ketoacidosis, hyperglycemia, and hyperosmolarity, and lactic acidosis), (4) severe infection, stress, (5) cerebrovascular accident, (6) heart, liver, and kidney dysfunction, (7) malignant tumor, connective tissue disease, coronary heart disease, stroke, and (8) take some drugs that affect the test (e.g., birth control pills, statins, etc.). All the selected persons were those of Chinese Han nationality who were not related to each other.
Main reagents
RPMI-1640 medium and fetal bovine serum were purchased from Gibco, and human lymphocyte separation solution 1.077 was purchased from Sigma. PE-labeled anti-human CD14 and FITC-labeled anti-human TLR4 antibodies were purchased from AbD Serotec, UK, and the ELISA test kit for MCP-1 was supplied by BioSource, USA. The adiponectin ELISA kit was supplied by Linco, USA.
Main methods
General data collection and grouping
-
(1)
Collection of medical history: Collect the age of the subject, past illness and medication history, smoking status, etc.
-
(2)
Body Mass Index (BMI) = weight/height2 (kg/m2) and height measurement: The subject is barefoot, standing in the “right position” on the bottom of the height gauge. The heel, the shin, and the two shoulders are placed against the height of the column, measuring the vertical distance from the top of the head to the heel, while recording the weight value.
-
(3)
Determination of biochemical indicators: Venous blood was taken on a fasting stomach, serum was separated, and serum MCP-1 concentration was determined by ELISA. HbA1c determination: using a high-pressure liquid phase method. Blood routine application XE-2100 automatic analyzer detection. Determination of fasting blood glucose, blood lipids, renal function, and hsCRP: Venous blood was taken on an empty stomach and detected by Olympus automatic biochemical analyzer.
-
(4)
Test group: Diagnostic criteria for diabetes according to the World Health Organization (WHO) Diabetes Diagnosis and Classification Standards in 1999; Divided according to the above diagnostic criteria: ①20 cases of normal glucose tolerance group (NGT) (male: female 12: 8),②50 cases of simple type 2 diabetes group (T2DM) (male: female 27:23), and ③50 cases of diabetic macroangiopathy group(male: female: 25:25). The HP-tip image color Doppler diagnostic device examines the lower extremity arteries (femoral artery, radial artery, anterior tibial artery, posterior tibial artery, and dorsal artery) and found arteriosclerotic plaques of the carotid artery and/or lower extremity arteries. Thrombosis or extensive irregular stenosis of the arteries; history of angina or myocardial infarction; diagnosis of coronary heart disease by dynamic electrocardiography and echocardiography or coronary angiography; history of cerebrovascular accident, ischemia of brain CT or MRI scan lesions; clinical manifestations of ischemic lesions of the lower extremities (intermittent breaks, ischemic pain).
A total of 20 healthy volunteers or normal controls who participated in the outpatient medical examination were selected. There were no significant differences in age, gender, blood routine, liver function, and renal function between the groups (p > 0.05). There were no significant differences in the incidence of hypertension, diabetic nephropathy, diabetic retinopathy, and smoking between the two groups (p > 0.05).
Collection of blood samples and isolation and culture of peripheral blood mononuclear cells (PBMC)
The subjects were collected for fasting venous blood in the morning, and the upper serum was taken and stored in a − 80 °C defreezer for use. At the same time, we sent the venous blood to the laboratory to test the blood routine, liver and kidney function, blood lipids, and other indicators. The remaining venous blood was placed in the heparin anticoagulation test tube for flow detection and PBMC separation. Peripheral blood PBMC was isolated by density gradient centrifugation of Ficoll lymphocyte separation solution, washed twice with serum-free medium, and added to complete RPM1–160 medium (containing 10% heat inactivated fetal bovine serum, penicillin, and streptomycin 1000 u /ml). To prepare a cell suspension, mix well and perform cell counting and trypan blue to identify cell viability (at least greater than 95%). The cell concentration was adjusted to 2 × 105 cells/ml and seeded into a 24-well plate, which was then placed in a 37 °C, 5% CO2 incubator for subsequent experiments.
VEGF-A qRT-PCR detection
TRIzol extracts total cellular RNA, determines RNA purity and content, and reverse transcribes into cDNA. The PCR primer sequence is as follows: VEGF-A forward primer 5'-CGAAGTGGTGAAGTTCATGG-3', reverse primer 5'-GTACT CGATCTCATCAGGGT-3', GAPDH forward primer 5'-CAATGACCCCTTCAT TGACC-’', reverse primer 5 '-GACAAGCTTCCCGTTCTCAG-3'. The relative content of VEGF-A mRNA is expressed by 2-ΔΔCt. Use GAPDH as an internal reference.
Flow cytometry to detect CD14 + CD16 + monocyte mean fluorescence intensity (MFI)
150 μl of EDTA anticoagulated peripheral whole blood was added to the bottom of the flow tube, and 1 tube was reserved as a blank control tube. No fluorescent antibody was added, and the other tubes were respectively added with corresponding antibodies (10 μl each of CD14-PE and CD16-FITC) and oscillated. After mixing, protect it from light, incubate for 30 min at room temperature, add 1 ml of red blood cell lysate to the above liquid, and mix for 10 min; then add l ml PBS + 1% BSA solution to each tube and place in a centrifuge to 1600 rpm/min, centrifugation for 5 min; the supernatant was discarded, and the cells were washed twice; the polyformaldehyde was added to each tube for 10 min; the MFI of CD14 + CD16 + was detected by flow cytometry. The use of an isotype control at the same time makes it possible to effectively ensure the specificity of the antibody.
Cytokine detection
The concentrations of serum MCP-1 and adiponectin were measured by ELISA. According to the instructions of the ELISA kit (purchased from Biosource and Linco, USA), the absorbance of each well was measured at 450 nm [A(450)]. The MCP-1 content calculation result is expressed in pg/ml, and the adiponectin content calculation result is expressed in mg/L. The intra-assay and inter-assay coefficients of variation of the reagents were all < 10%, and 5 replicate wells were set for all samples.
Statistical processing
Statistical analysis was performed using SPSS 13.0 software, and the measurement data was expressed by ± S. The t test was used to compare the measurement data between the two groups, and the one-way ANOVA was used for the three or more measurement data. Correlation analysis was performed using Pearson correlation analysis. p < 0.05 was considered statistically significant.
Results
Patient’s baseline characteristics
There were no significant differences in age, gender, DBP, liver function, renal function, peripheral blood leukocytes, and monocyte counts between the three groups (p > 0.05). The body mass index, HbA1c, fasting blood glucose, and SBP levels in the T2DM combined with macrovascular disease group were higher than those in the normal control group (p < 0.05; Table 1).
Flow analysis results of CD14 + CD16 + monocytes
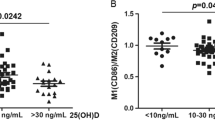
Compared with NGT, the peripheral blood proinflammatory CD14 + CD16 + monocyte fluorescence intensity values were increased in the T2DM group and the T2DM combined with macrovascular disease group (p < 0.05), and the T2DM combined with macrovascular disease group was higher than the T2DM group, the difference was statistically significant (p < 0.01;Fig. 1).

CD14 + CD16 + monocyte fluorescence intensity values NGT Normal glucose tolerance, T2DM Type 2 diabetes mellitus alone, T2DM-M Type 2 diabetes mellitus with macroangiopathy. υs NGT, *:p<0.05; υs T2DM, **:p<0.01
mRNA detection of VEGF-A in PBMC
Compared with NGT, the expression of VEGF-A mRNA in peripheral blood PBMC of patients with T2DM was significantly higher, and the T2DM combined with macrovascular disease group was higher than the T2DM group alone, and the difference was significant(p < 0.05;Fig. 2).

VEGF-A mRNA expression in peripheral blood PBMC NGT Normal glucose tolerance, T2DM Type 2 diabetes mellitus alone, T2DM-M Type 2 diabetes mellitus with macroangiopathy. υs NGT, *:p<0.05; υs T2DM, **:p<0.05
Serum MCP-1 and adiponectin levels
Serum MCP-1 levels in T2DM combined with macrovascular disease group were higher than those in T2DM group and NGT group, the difference was statistically significant (p < 0.05). The T2DM group was higher than the NGT group, and the difference was statistically significant (p < 0.05;Table 2). Compared with NGT group, the serum adiponectin level in T2DM group and T2DM combined with macrovascular disease group was higher than that in the NGT group, the difference was statistically significant (p < 0.05). However, compared with the latter two groups, serum adiponectin concentration in the T2DM group was higher than that in the T2DM with macrovascular disease group, and the difference was not statistically significant (p > 0.05;Table 2).
Correlation analysis
The mean fluorescence intensity of CD14 + CD16 + monocytes was positively correlated with serum MCP-1 level (r = 0.42, p < 0.05) and was not associated with adiponectin (p > 0.05).
Discussion
Diabetes has become the third most serious chronic disease that threatens human health after cancer and cardiovascular disease. Diabetes with vascular disease is one of the main complications of diabetes, and it is the main cause of death and disability. As a basic disease of diabetic macroangiopathy, atherosclerosis is a chronic inflammatory disease induced by various factors. The exact mechanism of vascular endothelial dysfunction and promotion of atherosclerosis and development has been a hot spot of research. Cells can secrete a variety of inflammatory factors, promote inflammatory reactions, trigger or aggravate the occurrence, and deterioration of atherosclerosis.
CD14 + CD16 + monocytes are considered to be a subset of proinflammatory monocytes. Our previous study found that abnormal expression of CD14 + CD16 + monocytes may be associated with the microinflammation state of type 2 diabetic mellitus (T2DM), and cytokine-mediated chronic low-grade inflammatory response in patients with T2DM and diabetic kidney disease (DKD), non-specific immune system activation participates in the occurrence and development of T2DM and its complications [1, 2]. This study found that the peripheral blood proinflammatory CD14 + CD16 + monocyte fluorescence intensity values were significantly higher in patients with T2DM alone and T2DM with macrovascular disease (p < 0.05), and T2DM with macrovascular disease group was higher than T2DM group (p < 0.01). Serum MCP-1 levels in patients with T2DM were significantly higher than those in normal controls, and T2DM with macrovascular disease group was significantly higher than T2DM alone (p < 0.05). Compared with NGT group, the serum adiponectin level in T2DM group and T2DM combined with macrovascular disease group was higher than that in the NGT group, the difference was statistically significant (p < 0.05). However, compared with the latter two groups, serum adiponectin concentration in the T2DM group was higher than that in the T2DM with macrovascular disease group, and the difference was not statistically significant (p > 0.05).
Adiponectin is one of the most abundant protein products expressed in adipose tissue and is abundantly present in the blood circulation. The study found that it has anti-inflammatory and anti-atherosclerotic effects [3]. The serum adiponectin concentration in patients with T2DM in this study was significantly lower than that in normal subjects. This is similar to Scherer [4] and Li et al [5] and others. Our study also found that serum adiponectin levels were further elevated in T2DM with macrovascular disease patients. Although the correlation analysis indicated the mean fluorescence intensity of CD14 + CD16 + monocytes and serum adiponectin p > 0.05, there is a negative correlation trend from the trend, but the number of samples is small, which may affect the results.
Vascular endothelial growth factor (VEGF) is a cytokine that acts specifically on vascular endothelial cells, which promote monocyte infiltration and increases skin cell proliferation and vascular permeability [6, 7]. Gurbuz et al and Carbajo-Pescador et al. found that VEGF expression is involved in the activation of the JAK/STAT pathway. STAT3 is a direct transcriptional activator of the VEGF gene [8, 9]. In the past, our research showed that the expression of VEGF and vascular endothelial growth factor receptor (VEGF-R) genes in atherosclerosis was significantly higher than that in the control group and consistent with the changes in JAK2/STAT3 levels [10]. This is consistent with the findings of the Gurbuz et al and Carbajo-Pescador et al. The study also found that compared with NGT, the expression of VEGF mRNA in peripheral blood PBMC of T2DM patients was significantly increased, and T2DM combined with macrovascular disease group was higher than T2DM alone group (p < 0.05), suggesting that VEGF may promote T2DM with large blood vessels. Monocytes infiltrate the diseased patients and participate in the pathogenesis.
In conclusion, this study showed that patients with T2DM and T2DM with macrovascular disease had increased VEGF expression and increased MCP-1 concentration in peripheral blood mononuclear cells, which may increase the number of CD14 + CD16 + monocytes due to increased MCP-1 concentration. It is involved in the chronic inflammatory response in patients with T2DM and T2DM with macrovascular disease, which leads to the development of T2DM and its complications. This may be one of the important reasons for diabetic patients suffering from atherosclerotic diseases such as coronary heart disease and diabetic lower extremity macrovascular disease. However, because the control group is not easy to obtain, resulting in a small sample size, this is a deficiency in the course of this experiment, which will be further studied in subsequent experiments, the sample size will be expanded, and the verification will be further repeated.
References
Yang M-X, Gan H, Shen Q, et al. Proportion of CD14+CD16+ monocyte s in peripheral blood from patients with type 2 diabetic mellitus and effect of LPS and IL-15 on expression of STAT5 in monocytes. Chin J Pathophysiol. 2012;28(1):136–41.
Yang M-X, Gan H, Shen Q, et al. Proinflammatory CD14+CD16+ monocytes are associated with microinflammation in patients with type 2 diabetes mellitus and diabetic nephropathy uremia. Inflammation. 2012;35(1):388–96.
Yuan G-Y, Chen M-D. Progress in adiponectin receptor and signal transduction. Sect Endocrinol For Med Sci. 2004;24(z1):3–6.
Scherer PE. Adipose tissue: from lipid storage compartment to endocrine organ. Diabetes. 2006;55(6):1537–45.
Li S, Shin HJ, Ding EL, van Dam RM. Adiponectin levels and risk of type 2 diabetes:a systematic review and meta-analysis. JAMA. 2009;302(2):179–88.
Tie J, Desai J. Antiangiogenic therapies targeting the vascular endothelia growth factor signaling system. Crit Rev Oncog. 2012;17(1):51–67.
Eichmann A, Simons M. VEGF signaling inside vascular endothelial cells and beyond. Curr Opin Cell Biol. 2012;24(2):188–93.
Gurbuz V, Konac E, Varol N, Yilmaz A, Gurocak S, Menevse S, et al. Effects of AG490 and S3I-201 on regulation of the JAK/STAT3 signaling pathway in relation to angiogenesis in TRAIL-resistant prostate cancer cells in vitro. Oncol Lett. 2014;7(3):755–63.
Carbajo-Pescador S, Ordoñez R, Benet M. Inhibition of VEGF expression through blockade of Hif1α and STAT3 signalling mediates the anti-angiogenic effect of melatonin in HepG2 liver cancer cells. Br J Cancer. 2013;109(1):83–91.
Li F-P, Li X-W, Yang M-X, et al. Expression of JAK2/STAT3 signaling pathway in human umbilical vein endothelial cells exposed to the serum of type 2 diabetic macroangiopathy patients. Acad J Second Mil Univ. 2016;37(4):452–6.
Funding
This study is funded by the National Natural Science Foundation of China (NO.81560147), The Science and Technology Support Program of Guizhou Province (Contract No. Qian Ke He Supporting Project [2017]2884]), The Key Science and Technology Program of Guizhou Province [Contract No. Qian Ke He SY (2012) 3116], and The Science and Technology Research Foundation of Guizhou Province, China [Contract No. Qian Ke He J LKZ (2013) 53].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the patient and by the Ethics Committee of Zunyi Medical University.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhou, X., Yang, MX., Xu, J. et al. Study on the expression of CD14 + CD16 + monocytes and VEGF in peripheral blood of patients with type 2 diabetes mellitus and diabetic macroangiopathy. Int J Diabetes Dev Ctries 40, 507–512 (2020). https://doi.org/10.1007/s13410-020-00809-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13410-020-00809-4