
Abstract
Human immunodeficiency virus (HIV) genetic compartmentalization is defined as genetic differences in HIV in different tissue compartments or subcompartments that characterize viral quasispecies. This descriptive, longitudinal study assessed the dynamics of inflammation, humoral immune response, blood-brain barrier, blood-cerebrospinal fluid (CSF) barrier, as well as neuronal injury biomarkers in serially obtained CSF and serum samples from an antiretroviral (ARV) therapy-naïve patient with HIV-1 subtype C with CSF HIV genetic compartmentalization that resolved spontaneously without ARV treatment. The first CSF sample showed an increase in white blood cell (WBC) count (382 cells/mm3) and a marked increase in the levels of inflammatory cytokines and chemokines, including tumor necrosis factor (TNF)α, interleukin (IL)-10, IP-10, and regulated on activation, normal T cell expressed and secreted (RANTES), which raise the suspicion of dual infection. Serum sample analysis showed all cytokine levels to be normal, with only IP-10 slightly increased. These results corroborate the hypothesis that the CNS immunologic response in a patient with HIV infection was independent of the systemic immunologic response. The patient also had persistently elevated levels of sCD14, neopterin, and β2M, which were strongly suggestive of persistent CNS immunologic stimulation. This report describes a patient with HIV subtype C who developed a transient episode of asymptomatic HIV meningitis with compartmentalization of HIV in the CSF that resolved independently of ARV therapy. Extensive CSF studies were performed as part of an ongoing longitudinal study, which revealed CNS immune abnormalities. This case presents evidence of HIV-1 subtype C neurotropism and compartmentalization.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
HIV-1 infects the central nervous system (CNS) almost immediately after transmission and causes HIV-associated neurodegeneration (Spudich et al. 2011; Valcour et al. 2012). Previous studies have reported a subset of individuals presenting with cerebrospinal fluid (CSF) viral escape, regardless of sustained HIV suppression in the blood during antiretroviral (ARV) therapy (Lescure et al. 2013; Canestri et al. 2010). The discordance between HIV viral loads in the CSF and plasma is defined according to the detectable HIV RNA levels in the CSF, i.e., the viral load in the plasma is < 50 copies/mL and in the CSF is > 200 copies/mL or the HIV RNA viral load in the CSF is ≥ 1 log higher than that in the plasma (Canestri et al. 2010). Moreover, CNS HIV compartmentalization, presumed to be a late-stage event associated with prolonged HIV infection or HIV encephalitis, may be a dynamic event that can occur in the earliest stage of HIV infection (Schnell et al. 2010; Sturdevant et al. 2012, 2015).
Previous studies have performed extensive characterization of HIV-1 subtype B CNS infection. However, little is known about the dynamics of CNS infection of HIV-1 subtype C, which is the most prevalent subtype worldwide. Hence, this study aimed to evaluate the dynamics of several biomarkers related to inflammation, neuronal injury, immunoglobulin G (IgG) intrathecal synthesis, blood-brain barrier (BBB), and blood-CSF barrier (BCSFB) in serial CSF and serum samples from an asymptomatic individual from Southern Brazil who was infected with HIV-1 subtype C. To our knowledge, this was the first report of asymptomatic disagreement between HIV viral loads in CSF and plasma (CSF > plasma) that resolved spontaneously without ARV treatment.
Methods
This study was approved by the institutional review board (IRB) of Hospital de Clínicas–Universidade Federal do Paraná (UFPR) and the National IRB (CONEP) in Brazil.
Specimen collection and storage: HIV-positive CSF and serum samples
We evaluated CSF and blood samples sequentially collected from a 51-year-old heterosexual Caucasian man with 13 years of education who was employed as a motorcycle courier. The participant was tested for HIV because his wife had been diagnosed with AIDS and CNS toxoplasmosis in October 2008 (the wife’s nadir CD4 was 45 cells/mm3). She was a housewife and was infected by heterosexual transmission. The participant provided four longitudinal paired CSF and blood samples: (A) March 27, 2009, not on ARV, in which discordance in CSF and blood HIV RNA levels was identified; (B) November 29, 2013; (C) August 29, 2014, 6 months after starting ARV therapy; and (D) September 23, 2016. All CSF samples were collected by lumbar puncture in polypropylene tubes to avoid proteins adherence to the tube walls and were stored at − 80 °C, in HC-UFPR, Brazil.
HIV-negative control group (n = 19)
Although this was a descriptive study, we compared the levels of biomarkers found in this case report to those in an HIV-negative control group because the normal ranges of most of the biomarkers in this study were not defined. The HIV(−) group was described previously (de Almeida et al. 2016a, b).
Clinical laboratory parameters
CSF biochemistry and cytology were quantified by standard methods. The HIV RNA in the serum and CSF were quantified using a branched DNA assay (Siemens) with a nominal limit of detection of 50 copies/mL.
Sequence filtering, dual infection (DI) screening, and bioinformatics analysis
We amplified the HIV-1 env C2-V3 (HXB2 coordinates 6928–7344) region from RNA extracted from the CSF and HIV DNA from peripheral blood mononuclear cells (PBMC) by nested polymerase chain reaction (PCR) using specific primers. Sequencing was performed using an NGS 454 GS FLX Titanium system (454 Life Sciences, Roche, Branford, Connecticut, USA). Read (FASTA) and quality score files produced by the 454 instruments were further analyzed using a purpose-built bioinformatics pipeline used by our group in numerous published studies (Fisher et al. 2015; Carter et al. 2015; Wagner et al. 2014). The pipeline is available at https://github.com/veg/HIV-NGS . Viral compartmentalization was assessed by the F-statistics (Fst) (p < 0.01) (Hudson et al. 1992), which was used to measure the genetic distance between populations (Chen and Wang 2015). The statistical significance was derived via 1000 population-structure randomization/permutation test. Viral compartmentalization analysis via Fst statistics was repeated using representative haplotypes to guard against the possible skewing of allelic frequencies due to PCR amplification. Evidence of dual infection (DI) in gag and/or env was explored as previously described (Wagner et al. 2014, 2016). Briefly, representative haplotypes from the CSF, PBMC, and blood plasma for each coding region were assembled into separate phylogenies with (i) all GenBank HIV-1 subtype C sequences from Brazil and (ii) representative haplotypes from Curitiba’s local cohort from Brazil. Evidence of intermingled sequences between input haplotypes and background sequences suggested potential DI that could have been missed by focusing on intrasample diversity while well-segregated sequences argued against potential DI.
CSF and serum soluble biomarkers
All samples were assayed concurrently in duplicate according to the manufacturers’ instructions. We evaluated the levels of several soluble biomarkers in CSF and serum: Inflammation biomarkers, including tumor necrosis factor α (TNFα), interferon γ (IFNγ), interleukins (IL-1β, IL-2, IL-4, IL-6, IL-7, and IL-10), monocyte chemoattractant protein-1 (MCP-1), macrophage inflammatory protein-1α and β (MIP-1α and β), interferon gamma-induced protein-10 (IP-10), were quantified by multiplex bead suspension array immunoassays (EMD Millipore, Billerica, MA). Regulated during activation, normal T cell expressed and secreted (RANTES) and urokinase plasminogen activator receptors (uPARs) were quantified by high-sensitivity enzyme-linked immunosorbent assay (ELISA, R&D Systems, Minneapolis, MN). We also measured levels of BBB markers, including sE-Selectin, soluble cell adhesion molecules-1 (sVCAM-1), soluble intercellular adhesion molecule-1, and metalloproteinase-2, metalloproteinase-3, and metalloproteinase-9 (MMP-2, MMP-3, and MMP-9) using multiplex bead suspension array immunoassays (EMD Millipore, Billerica, MA). The tissue inhibitor metalloproteinase-1 and tissue inhibitor metalloproteinase-2 (TIMP-1 and TIMP-2) were measured by electrochemiluminescence assay (Meso Scale Discovery, Rockville, MD). The levels of neuronal injury markers, including phosphorylated tau-181 (pT-181, Thermo Fisher Scientific Inc., Waltham, MA, USA), were assayed by multiplex bead assays (FlexMAP 3D®, Luminex Corporation, Austin, TX, USA); total tau, amyloid β (Aβ 38, 40, and 42), and soluble amyloid precursor protein α and β (sAPPα and sAPPβ) were measured using electrochemiluminescence assay (Meso Scale Discovery, Rockville, MD). Neurofilament light (NFL-light) was quantified using high-sensitivity ELISA (Uman Diagnostic). Monocyte and macrophage activation: human β2 microglobulin (β2M) was quantified using the nephelometric method (Dade Behring BNII, Deerfield, IL) with N latex β2 microglobulin (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany). sCD-14 (R&D Systems, Minneapolis, MN) and neopterin (Thermo Fisher Scientific) were quantified by high-sensitivity ELISA. Microglia injury: ferritin (Architect, Abbott, Longford, Ireland). Demyelization: myelin basic protein (MBP, Ansh Labs) was quantified by high-sensitivity ELISA. BCSFB function: CSF and serum albumin were quantified using the nephelometric method (Dade Behring BNII, Deerfield, IL) with antiserum N human albumin (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) and VR 7.0–34 mg/dL (Breebaart et al. 1978). The functional integrity of the BCSFB was then assessed by calculating the CSF albumin/serum albumin quotient, QAlb = AlbCSF/Albserum. The upper limit of the reference range was age-dependent and was calculated for each sample using the following equation: QAlb ref. = (4 + age [y]/15) × 10−3 (Reiber and Peter 2001). IgG intrathecal synthesis was assayed using quantitative and qualitative methods. IgG in the CSF and serum were quantified using the nephelometric method (Dade Behring BNII, Deerfield, IL) with antiserum N human IgG (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) (Reiber et al. 2003). For the qualitative analysis of IgG intrathecal synthesis, the CSF and serum samples were assayed to detect oligoclonal bands by agarose gel isofocusing followed by IgG immunofixation (Hydragel CSF Isofocusing-Sebia, Norcross, GA). Quantitative analysis of IgG intrathecal synthesis and BCSFB function was analyzed by IgG hyperbolic function and Reibergram plot (Reiber 1995). The plots were generated using CSF Research software.
Results
This was a descriptive, longitudinal study of the dynamics of inflammation, humoral immune responses, BBB, and BCSFB, as well as neuronal injury biomarkers in serially obtained CSF and blood samples.
Patient clinical and laboratory parameters
The CSF cell and biochemistry measurements and clinical characteristics over time are shown in Table 1. At the time of the first CSF sample (A), the participant was classified as non-AIDS, with an initial CD4 count of 692 cells/mm3 (March 27, 2009) and negative for hepatitis B and C virus (HBV and HCV). He was asymptomatic, had no neurological complaints, had normal findings on neurological and neuropsychological evaluation, and was categorized as independent according to the Lawton Instrumental Activities of Daily Living scale. HIV-1 genotyping indicated subtype C. CSF samples were collected because the patient voluntarily agreed to participate in an HIV neurocognitive study. At time point A, the patient showed lymphocytic meningitis with a severe increase in CSF WBC (382 cells/mm3), but with normal lactate and glucose levels (Table 1). Standard microbiological methods were used to test for the presence of various infectious etiologic agents, including virus, bacteria, and fungus, but the results were negative and the patient’s CSF had negative Venereal Disease Research Laboratory (VDRL) test results. He was diagnosed with chronic HIV meningitis.
Five years later (February 19, 2014), the patient was categorized as A-2 based on the 1993 revised CDC classification system. ARV therapy was started with lamivudine (3TC), tenofovir (TDF), and lopinavir/ritonavir (LPV/r): Antiretroviral CNS penetration-effectiveness (CPE 2010) (2 + 1 + 3 + 1) = 7; after 2 months, LPV/r was substituted for efavirenz (EFZ) due to diarrhea in the ARV regimen: CPE 2010 (2 + 1 + 3) = 6. The patient demonstrated good treatment adherence and was responsive to ARV therapy. The HIV RNA was suppressed in both CSF and blood samples (Table 1).
Computed axial tomography (CAT) of the brain (12/07/2016) showed a discrete prominence of basal cisterns, brain, and cerebellar sulci. There was no pathological enhancement of the meninges after the administration of intravenous iodinated contrast injection. A brain CAT was not performed at the time of the first CSF sample collection.
Phylogenetic analyses of CNS compartmentalization and DI
We observed discordance in HIV RNA between the CSF and plasma samples (CSF > plasma) at time point A in which the viral load in the CSF sample was 2.6-log greater than that in the blood sample (Table 1). We amplified partial env and gag genes from the CSF and blood samples. The tree topology revealed evidence of compartmentalization in both env and gag regions between the blood (plasma or PBMC) and CSF, which were confirmed using the Fst approach (p < 0.01) (Hudson et al. 1992), but not (though nearly significant) between the plasma and PBMC (available for the gag region only) (Fig. 1).

Approximate maximum likelihood phylogenetic reconstruction of sequences generated from paired blood plasma and cerebrospinal fluid (CSF) HIV-1 RNA and peripheral blood mononuclear cells (PBMC) HIV DNA samples. HIV DNA and RNA haplotypes above a minimum frequency threshold of 0.01 were extracted from reads covering the env (a) and gag (b) regions for individual B0019 and were used to construct approximate maximum likelihood phylogenies using FastTree (Price et al. 2009). HIV DNA and RNA haplotypes are depicted in circles with sizes indicative of the haplotype frequencies. Colors denote the compartment of origin with blood plasma, CSF, and PBMC in red, blue, and green respectively. Scale bars are in substitutions/site. This analysis includes the sample collected when the HIV CSF escape was identified (sample A). There was evidence of compartmentalization in both the env and gag regions between the blood (plasma or PBMC) and CSF, as confirmed using the Fst approach (Hudson et al. 1992) (p = 0.01 and 0.009 respectively), but not (though nearly significant, p = 0.06) between plasma and PBMC, which was available for gag only. The phylogenetic distance is shown at the bottom of each tree for reference. a Paired blood plasma and CSF samples, partial env region. b Paired blood plasma, PBMC, and CSF samples, partial gag region (color figure online)
The CSF and plasma HIV RNA disagreement disappeared spontaneously 56 months after HIV diagnosis without ARV treatment (sample B); the HIV RNA were higher in the blood than those in the CSF and the WBC count and total protein levels in the CSF had decreased. It was not possible to amplify HIV RNA in CSF sample B, and HIV RNA was not detected in CSF samples C and D (Table 1).
We evaluated the potential for DI in the gag and/or env sequences from sample A by applying multiple approaches with GenBank and local cohort HIV-1 subtype C sequences for CSF, PBMC, and plasma. The results showed evidence of mono-infection. Although this conclusion is limited by the short region and single time point, we cannot reject the possibility of a DI (Fig. 2a–c).

Dual infection (DI) screening. a Approximate maximum likelihood phylogenies of CSF partial env and gag regions from our sampled patient (blue) and all representative CSF haplotypes from Curitiba’s local cohort from Brazil (black). b Phylogenies of blood partial env and gag regions from our sampled patient (red) and all representative blood haplotypes from Curitiba’s local cohort from Brazil (black). c Phylogenies of blood partial env and gag regions from our sampled patient (red) and GenBank HIV-1 subtype C sequences from Brazil (black). All phylogenies are suggestive of mono-infection, but the analyses are limited by the short region analyzed (partial env and gag) and the lack of longitudinal sampling; therefore, we cannot reject the potential for DI. The scale bar at the bottom represents the phylogenetic distance (substitutions/site). All phylogenies are rooted to HXB2 (color figure online)
Dynamics of CSF and serum biomarkers
Monocyte and macrophage activation biomarkers
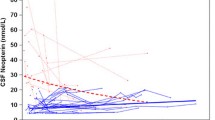
The CSF and serum values of the biomarkers of monocyte and macrophage activation are shown in Table 2. sCD14 levels in the CSF significantly were increased in time point A (6.5-fold higher compared to the median values in the control group) and decreased in sample C but was still higher than the median values in the control group. The CSF neopterin levels were increased in sample A (17-fold). It progressively decreased but persisted higher than the control group in sample C. The CSF Β2 microglobulin levels were increased in sample A (5-fold), while those in sample B were increased 3-fold. The increase in the levels of monocyte and macrophage activation biomarkers was more severe in the CSF than that in the serum (Table 2).
CSF and serum neuronal injury biomarkers
The NFL level was increased in all three CSF samples, although with a trend toward normalization (Table 2). The Aβ-40 levels also increased, while the Aβ-38 and Aβ-42 levels in the CSF sample A remained normal. All Aβ isoforms were normal in sample C. The level of myelin basic protein (MPB) was slightly increased, and the results were similar in all three samples (Table 2).
Humoral immune response (IgG intrathecal synthesis)
The dynamics of intrathecal IgG synthesis and BCSFB dysfunction are shown in Fig. 3. CSF sample A showed oligoclonal bands restricted to CSF, type 2 (Andersson et al. 1994). Oligoclonal bands were not analyzed in sequential samples.

Hyperbolic function (Reibergram plot) of blood-CSF barrier function and intrathecal IgG synthesis. The graph shows the dynamics of intrathecal IgG synthesis and blood-CSF barrier (BCSFB) dysfunction. Hyperbolic functions are a consequence of nonlinear interactions of molecular flux with the CSF flow rate, as derived from the laws of diffusion (Reiber 1995). BCSFB dysfunction is indicated on the graph in the area with vertical stripes; the age-corrected normal range for QAlb was 6 × 10−3. The plot was generated using CSF research software. Sample A was collected at the time when the CNS HIV compartmentalization was identified, before antiretroviral (ARV) initiation, showing BCSFB dysfunction; sample B was collected 56 months after the CNS HIV compartmentalization diagnosis, still without ARV, showing decrease of BCSFB dysfunction and 30% IgG intrathecal synthesis, in addition to CSF WBC and total protein improvement. The IgG values were estimated (open circle) in samples C and D; no BCSFB dysfunction was noted in these samples, but IgG intrathecal synthesis persisted despite the initiation of ARV (sample C) and normal CSF WBC values (sample D)
Cellular immune response (cytokines and chemokines)
The levels of CSF and serum cytokine and chemokine biomarkers in the sample with CNS HIV compartmentalization (sample A) compared to those in the HIV-negative control group are shown in Table 3. In sample A, the levels of all cytokines and chemokines quantified in the CSF, chiefly TNFα, IL-10, IFNy, IP-10, and RANTES were elevated. In the serum, the levels of all cytokines quantified were lower than those in the control group, except for IL-10. The IP-10 levels were increased while the levels of other chemokines remained normal. Analysis of the Th1/Th2 ratios revealed a predominance of antiinflammatory cytokines (Th2 response) in both the CSF and the serum. The CSF and serum values and the magnitude of the increase compared with those of the control group are shown in Table 3.
Blood-brain barrier biomarkers
In sample A, the sVCAM-1 and uPAR levels in the CSF were higher than those in the control group and the levels of MMP-9 (800-fold higher than the level in the control group) and its respective tissue inhibitor TIMP-1 was also increased. There was also an increase in the ratios of MMP-9/ TIMP-1 and MMP-2/TIMP-2. In the serum, a slight increase in sVCAM-1 and uPAR levels was observed. The ratios of MMP-9/TIMP-1 and MMP-2/TIMP-2 in the serum were normal. The levels of BBB biomarkers in the CSF and serum in the patient with CNS HIV compartmentalization (sample A) were compared to those in the HIV-negative control group (Table 3).
Discussion
We present a case of a patient infected with HIV-1 subtype C who was non-AIDS, ARV naïve, and with asymptomatic HIV meningitis. He showed discordance in the HIV RNA of CSF and plasma, which resolved spontaneously and independent of ARV therapy. This case presents evidence of HIV-1 subtype C neurotropism and CNS compartmentalization. Different from previous reports on HIV-1 subtypes B or C CNS compartmentalization (Canestri et al. 2010; van Lelyveld et al. 2010; Katlama et al. 2010; Bogoch et al. 2011; Bingham et al. 2011; Tamarit M del et al. 2012; Peluso et al. 2014; de Almeida et al. 2017), the present case did not meet the reported risk factors, such as low CD4+ T cell nadir and advanced immunosuppression, presence of HIV-associated dementia (HAD), and poor adherence to ART (Ritola et al. 2005; Harrington et al. 2009; Canestri et al. 2010; Schnell et al. 2010; Peluso et al. 2014).
The overall biomarker analysis showed that (1) concurrent with the increase in CSF WBC count (viral meningitis), the levels of most CSF neuroinflammation biomarkers, including all ß-chemokines, also increased. (2) This finding showed that ß-chemokines were successfully stimulated by HIV-1 subtype C, contrary to previous reports (Satishchandra et al. 2000; Ranga et al. 2004). (3) A severe increase in CSF biomarker levels in contrast with the patient’s asymptomatic presentation, including normal cognitive function. (4) Concurrent with HIV-1 subtype C CNS compartmentalization, there was a marked increase in the CSF WBC count and levels of CSF inflammatory, microglia, and neuronal injury biomarkers including NFL, with a slight impact on β-amyloid metabolism and no demyelination. (6) Persistent monocyte and macrophage activation and IgG intrathecal synthesis lasting more than 5 years were consistent with the persistence of CNS immunological stimulation, as HIV persisted in a latent state in microglia and astrocytes despite a controlled CSF HIV viral load. (7) The cellular immune response to HIV in the CSF was different from that in the serum. The response was stronger in the CNS than that in the peripheral blood, indicating that the CNS cellular immune response was compartmentalized (de Almeida et al. 2016a). (8) The levels of several biomarkers were higher in the CSF than those in the serum, strongly indicating intrathecal production. (9) The CSF HIV compartmentalization was accompanied by BCSFB dysfunction and BBB disruption with increased levels of cell adhesion molecules and metalloproteinases.
CNS escape has been described in association with and without symptoms. It was reported asymptomatic CSF escape in about 10% of a group of ART-treated patients with suppressed systemic HIV replication. The increased CSF HIV viral load (VL) was associated with intrathecal immune activation and appeared to be clinically benign (Eden et al. 2010; Ferretti et al. 2015). Although different from the present case, CSF pleocytosis was not observed in the previous cases.
The increases WBC count with lymphocyte and inflammatory biomarkers in sample A could be interpreted as HIV chronic meningitis exacerbated by HIV CNS compartmentalization. However, no other aspects in the patient’s history could have triggered meningitis. The severe increase in WBC count is not common in HIV chronic meningitis; however, the concomitant increase in all CSF cytokines and chemokines resembled acute HIV meningitis (Marshall et al. 1988). Although the patient had been diagnosed with HIV infection 4 months earlier, the duration of infection could have been longer due to the occurrence of his wife’s AIDS. This raises the possibility of dual infection (DI); however, specific phylogenetic analysis revealed mono-infection. In addition, the HIV viral load in the blood was consistent with chronic infection, arguing against the DI hypothesis.
DI results in the presence of two variants, each originating from an independent infection event. When the second infection occurs after seroconversion, it is called DI; when the second infection occurs nearly simultaneously with the first, or at least before seroconversion, the condition is generally considered co-infection (Waters and Smit 2012). The overall frequency of HIV DI varies between 0 and 20% (Hebberecht et al. 2018). However, the number of well-documented DI reports remains low, possibly because of difficulties in demonstrating this condition (Hebberecht et al. 2018).
HIV chronic meningitis occurs in 13 to 40% of HIV-positive individuals at any stage of infection (Marshall et al. 1988; Hollander et al. 1994) and approximately 59% are asymptomatic. The WBC count is less than that measured in the present case, with a median (IQR) count of 10 (8; 22) cells/mm3 (de Almeida et al. 2011). This is an exclusion diagnosis in which any other causes of chronic meningitis by opportunistic or co-infection must be ruled out (Marshall et al. 1988; Hollander et al. 1994).
The results of this study support the findings of a previous study from the same group, showing that HIV-1 subtype C is as neurotropic as subtype B and also able to develop CNS HIV genetic compartmentalization (de Almeida et al. 2017). Moreover, previous studies found similar frequencies of HIV-C and B neurological and psychiatric manifestations as well as similar stimulation of ß-chemokines and inflammatory biomarkers in the CSF (de Almeida et al. 2013, 2016a, b). These findings are contrary to a previous report that HIV-1 subtype C was less neuropathogenic than subtype B (Satishchandra et al. 2000).
These results should be interpreted with caution and should not be generalized to other HIV patients or groups. This study had several limitations. First, this was a descriptive study with a limited number of samples. There was no evidence of DI, but this observation was limited to a short sequence region and a single time point, which limited the possibility to reject the potential for DI. In addition, the phylogenic analysis could only be done for the first sample. In the following CSF samples, it was not possible to amplify HIV RNA or complementary DNA, making it difficult to determine the possibility of transient CNS HIV genetic compartmentalization. The loss of amplification might reflect a low HIV RNA copy number in the CSF, while the compartmentalization may still be present. However, the HIV viral load in the second CSF sample was lower than that of the plasma and there was a decrease in WBC count, suggesting that the HIV compartmentalization was resolved.
Despite the limitations of this study, we showed that independent and isolated HIV replication can occur in the CNS of patients infected with HIV-1 subtype C, which can lead to compartmentalization and development of quasispecies distinct from the peripheral plasma that are associated with strong cell and humoral immunological responses, BBB dysfunction, and brain injury.
From a pathophysiological standpoint, it is difficult to determine the clinical consequences of these episodes. Additional studies are necessary to establish if these events could lead to an increased risk of HAD or if they represent the natural history of HIV infection in CNS without clinical consequences. Previously reported cases of asymptomatic increases in CSF HIV VL reported no neurological progression (Eden et al. 2010).
These findings provide evidence for the future development of hypotheses and further investigation of CSF compartmentalization in asymptomatic HIV participants and provide support for HIV-1 subtype C neurotropism and neurovirulence studies. Future studies with larger sample sizes with adequate statistical analysis are necessary to validate these results.
References
de Almeida SM, Boritza K, Cogo LL et al (2011) Quantification of cerebrospinal fluid lactic acid in the differential diagnosis between HIV chronic meningitis and opportunistic meningitis. Clin Chem Lab Med 49:891–896
de Almeida SM, Ribeiro CE, de Pereira AP et al (2013) Neurocognitive impairment in HIV-1 subtype C versus B-infected individuals in Southern Brazil. J Neuro-Oncol 19:550–556
de Almeida SM, Rotta I, Ribeiro CE, Smith D, Wang R, Judicello J, Potter M, Vaida F, Letendre S, Ellis RJ (2016a) Blood-CSF barrier and compartmentalization of CNS cellular immune response in HIV infection. J Neuroimmunol 301:41–48
de Almeida SM, Rotta I, Jiang Y et al (2016b) Biomarkers of chemotaxis and inflammation in cerebrospinal fluid and serum in individuals with HIV-1 subtype C versus B. J Neuro-Oncol 22:715–724. https://doi.org/10.1007/s13365-016-0437-4
de Almeida SM, Rotta I, Ribeiro CE et al (2017) Dynamic of CSF and serum biomarkers in HIV-1 subtype C encephalitis with CNS genetic compartmentalization: case study. J Neuro-Oncol 23:460–473
Andersson MA, Cermeño J, Bernardi G et al (1994) Cerebrospinal fluid in the diagnosis of multiple sclerosis: a consensus report. J Neurol Neurosurg Psychiatry 57:897–902
Bingham R, Ahmed N, Rangi P, Johnson M, Tyrer M, Green J (2011) HIV encephalitis despite suppressed viraemia: a case of compartmentalized viral escape. Int J STD AIDS 22:608–609
Bogoch II, Davis BT, Venna N (2011) Reversible dementia in a patient with central nervous system escape of human immunodeficiency virus. J Inf Secur 63:236–239
Breebaart K, Becker H, Jongebloed FA (1978) Investigation of reference values of components of cerebrospinal fluid. J Clin Chem Clin Biochem 16:561–565
Canestri A, Lescure FX, Jaureguiberry S, Moulignier A, Amiel C, Marcelin AG, Peytavin G, Tubiana R, Pialoux G, Katlama C (2010) Discordance between cerebral spinal fluid and plasma HIV replication in patients with neurological symptoms who are receiving suppressive antiretroviral therapy. Clin Infect Dis 50:773–778
Carter CC, Wagner GA, Hightower GK, Caballero G, Phung P, Richman DD, Pond SLK, Smith DM (2015) HIV-1 neutralizing antibody response and viral genetic diversity characterized with next generation sequencing. Virology 474:34–40
Caudie C, Bancel J, Dupont M et al (2005) CSF levels and diagnostic utility of cerebrospinal fluid beta2-microglobulin. Ann Biol Clin 63:631–637
Centers for Disease Control and Prevention (CDC) (1993) Revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. JAMA 269:729–730
Chen W, Wang H (2015) Variance estimation for nucleotide substitution models. Mol Phylogenet Evol 90:97–103
Eden A, Fuchs D, Hagberg L et al (2010) HIV-1 viral escape in cerebrospinal fluid of subjects on suppressive antiretroviral treatment. J Infect Dis 202:1819–1825. https://doi.org/10.1086/657342
Ferretti F, Gisslen M, Cinque P, Price RW (2015) Cerebrospinal fluid HIV escape from antiretroviral therapy. Curr HIV/AIDS Rep 12:280–288
Fisher RG, Smith DM, Murrell B, Slabbert R, Kirby BM, Edson C, Cotton MF, Haubrich RH, Kosakovsky Pond SL, van Zyl GU (2015) Next generation sequencing improves detection of drug resistance mutations in infants after PMTCT failure. J Clin Virol 62:48–53
Greene DN, Schmidt RL, Wilson AR, Freedman MS, Grenache DG (2012) Cerebrospinal fluid myelin basic protein is frequently ordered but has little value: a test utilization study. Am J Clin Pathol 138:262–272
Harrington PR, Schnell G, Letendre SL, Ritola K, Robertson K, Hall C, Burch CL, Jabara CB, Moore DT, Ellis RJ, Price RW, Swanstrom R (2009) Cross-sectional characterization of HIV-1 env compartmentalization in cerebrospinal fluid over the full disease course. AIDS 23:907–915
Hebberecht L, Vancoillie L, Schauvliege M, Staelens D, Dauwe K, Mortier V, Verhofstede C (2018) Frequency of occurrence of HIV-1 dual infection in a Belgian MSM population. PLoS One 13:e0195679. https://doi.org/10.1371/journal.pone.0195679
Hollander H, McGuire D, Burack JH (1994) Diagnostic lumbar puncture in HIV-infected patients: analysis of 138 cases. Am J Med 96:223–228
Hudson RR, Slatkin M, Maddison WP (1992) Estimation of levels of gene flow from DNA sequence data. Genetics 132:583–589
Katlama C, Valantin MA, Algarte-Genin M et al (2010) Efficacy of darunavir/ritonavir maintenance monotherapy in patients with HIV-1 viral suppression: a randomized open-label, noninferiority trial, MONOI-ANRS 136. AIDS 24:2365–2374
van Lelyveld SF, Nijhuis M, Baatz F et al (2010) Therapy failure following selection of enfuvirtide resistant HIV-1 in cerebrospinal fluid. Clin Infect Dis 50:387–390
Lescure FX, Moulignier A, Savatovsky J, Amiel C, Carcelain G, Molina JM, Gallien S, Pacanovski J, Pialoux G, Adle-Biassette H, Gray F (2013) CD8 encephalitis in HIV-infected patients receiving cART: a treatable entity. Clin Infect Dis 57:101–108
Marshall DW, Brey RL, Cahill WT, Houk RW, Zajac RA, Boswell RN (1988) Spectrum of cerebrospinal fluid findings in various stages of human immunodeficiency virus infection. Arch Neurol 45:954–958 https://www.ncbi.nlm.nih.gov/pubmed/2970837
Peluso MJ, Ferretti F, Peterson J et al (2014) Cerebrospinal fluid hiv escape associated with progressive neurologic dysfunction in patients on antiretroviral therapy with well-controlled plasma viral load. AIDS 26:1765–1774
Petzold A, Eikelenboom MJ, Gveric D et al (2002) Markers for different glial cell responses in multiple sclerosis: clinical and pathological correlations. Brain 125:1462–1473
Price MN, Dehal PS, Arkin AP (2009) FastTree: computing large minimum evolution trees with profiles instead of a distance matrix. Mol Biol Evol 26:1641–1650
Ranga U, Shankarappa R, Siddapa NB et al (2004) Tat protein of human immunodeficiency virus type 1 subtype C strains is a defective chemokine. J Virol 78:2586–2590
Reiber H (1995) External quality assessment in clinical neurochemistry: survey of analysis for cerebrospinal fluid (CSF) proteins based on CSF/serum quotients. Clin Chem 41:256–263
Reiber H, Peter JB (2001) Cerebrospinal fluid analysis: disease-related data patterns and evaluation programs. J Neurol Sci 184:101–122
Reiber H, Thompson EJ, Grimsley G et al (2003) Assurance for cerebrospinal fluid protein analysis: international consensus by an internet-based group discussion. Clin Chem Lab Med 41:331–337
Ritola K, Robertson K, Fiscus SA, Hall C, Swanstrom R (2005) Increased human immunodeficiency virus type 1 (HIV-1) env compartmentalization in the presence of HIV-1-associated dementia. J Virol 79:10830–10834
Sacktor NC, Wong M, Nakasujja N et al (2005) The International HIV Dementia Scale: a new rapid screening test for HIV dementia. AIDS 19:1367–1374
Satishchandra P, Nalini A, Gourie-Devi M et al (2000) Profile of neurologic disorders associated with HIV/AIDS from Bangalore, South India (1989–1996). Indian J Med Res 111:14–23
Schnell G, Price RW, Swanstrom R, Spudich S (2010) Compartmentalization and clonal amplification of HIV-1 variants in the cerebrospinal fluid during primary infection. J Virol 84:2395–2407
Spudich S, Gisslen M, Hagberg L, Lee E, Liegler T, Brew B, Fuchs D, Tambussi G, Cinque P, Hecht FM, Price RW (2011) Central nervous system immune activation characterizes primary human immunodeficiency virus 1 infection even in participants with minimal cerebrospinal fluid viral burden. J Infect Dis 204:753–760
Sturdevant CB, Dow A, Jabara CB, Joseph SB, Schnell G, Takamune N, Mallewa M, Heyderman RS, van Rie A, Swanstrom R (2012) Central nervous system compartmentalization of HIV-1 subtype C variants early and late in infection in young children. PLoS Pathog 8:e1003094
Sturdevant CB, Joseph SB, Schnell G et al (2015) Compartmentalized replication of R5 T cell-tropic HIV-1 in the central nervous system early in the course of infection. PLoS Pathog 7:e1002286
Tamarit M del P, Quereda C, Gonzalez-Rozas M, Corral I et al (2012) HIV type 1 viral encephalitis after development of viral resistance to plasma suppressive antiretroviral therapy. AIDS Res Hum Retrovir 28:83–86
Valcour V, Chalermchai T, Sailasuta N, Marovich M, Lerdlum S, Suttichom D, Suwanwela NC, Jagodzinski L, Michael N, Spudich S, van Griensven F, de Souza M, Kim J, Ananworanich J (2012) Central nervous system viral invasion and inflammation during acute HIV infection. J Infect Dis 206:275–282
Wagner GA, Pacold ME, Kosakovsky Pond SL, Caballero G, Chaillon A, Rudolph AE, Morris SR, Little SJ, Richman DD, Smith DM (2014) Incidence and prevalence of intrasubtype HIV-1 dual infection in at-risk men in the United States. J Infect Dis 209:1032–1038
Wagner GA, Chaillon A, Liu S et al (2016) HIV-associated neurocognitive disorder is associated with HIV-1 dual infection. AIDS 13:2591–2597
Waters L, Smit E (2012) HIV-1 superinfection. Curr Opin Infect Dis 25:42–50
Acknowledgements
We thank Carlos Otávio Brandão, MD, PhD of Neurolife Laboratórios RJ, Brazil, for providing the CSF albumin measurements.
Funding
This work was supported by the following grants: National Institute of Health, NIH R21 MH76651 (Ellis, Ronald J; Almeida, Sergio M.), NIH R01 MH83552 (Smith, David M.), S10 RR31646 (Letendre, Scott), K24 MH097673 (Letendre, Scott); University of California, San Diego, Center for AIDS Research (CFAR), an NIH-funded program (P30 AI036214), which is supported by the following NIH Institutes and Centers: NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA, NIGMS, and NIDDK; Ministério da Ciência e Tecnologia/Conselho Nacional de Desenvolvimento Científico e Tecnológico, MCT/CNPq-Universal 014/2008, Brazil (Almeida, Sergio M.).
The HIV Neurobehavioral Research Center (HNRC) is supported by Center award P30MH062512 from NIMH. The San Diego HIV Neurobehavioral Research Center [HNRC] group is affiliated with the University of California, San Diego, the Naval Hospital, San Diego, and the Veterans Affairs San Diego Healthcare System and includes Director: Robert K. Heaton, Ph.D., Co-Director: Igor Grant, M.D.; Associate Directors: J. Hampton Atkinson, M.D., Ronald J. Ellis, M.D., Ph.D., and Scott Letendre, M.D.; Center Manager: Thomas D. Marcotte, Ph.D.; Jennifer Marquie-Beck, M.P.H.; Melanie Sherman; Neuromedical Component: Ronald J. Ellis, M.D., Ph.D. (P.I.), Scott Letendre, M.D., J. Allen McCutchan, M.D., Brookie Best, Pharm.D., Rachel Schrier, Ph.D., Debra Rosario, M.P.H.; Neurobehavioral Component: Robert K. Heaton, Ph.D. (P.I.), J. Hampton Atkinson, M.D., Steven Paul Woods, Psy.D., Thomas D. Marcotte, Ph.D., Mariana Cherner, Ph.D., David J. Moore, Ph.D., Matthew Dawson; Neuroimaging Component: Christine Fennema-Notestine, Ph.D. (P.I.), Monte S. Buchsbaum, M.D., John Hesselink, M.D., Sarah L. Archibald, M.A., Gregory Brown, Ph.D., Richard Buxton, Ph.D., Anders Dale, Ph.D., Thomas Liu, Ph.D.; Neurobiology Component: Eliezer Masliah, M.D. (P.I.), Cristian Achim, M.D., Ph.D.; Neurovirology Component: David M. Smith, M.D. (P.I.), Douglas Richman, M.D.; International Component: J. Allen McCutchan, M.D., (P.I.), Mariana Cherner, Ph.D.; Developmental Component: Cristian Achim, M.D., Ph.D.; (P.I.), Stuart Lipton, M.D., Ph.D.; Participant Accrual and Retention Unit: J. Hampton Atkinson, M.D. (P.I.), Jennifer Marquie-Beck, M.P.H.; Data Management and Information Systems Unit: Anthony C. Gamst, Ph.D. (P.I.), Clint Cushman; and Statistics Unit: Ian Abramson, Ph.D. (P.I.), Florin Vaida, Ph.D. (Co-PI), Bin Tang, Ph.D., Anya Umlauf, M.S.
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, nor the US Government.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the institutional review board (IRB) of Hospital de Clínicas–Universidade Federal do Paraná (UFPR) and the National IRB (CONEP) in Brazil.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
de Almeida, S.M., Oliveira, M.F., Chaillon, A. et al. Transient and asymptomatic meningitis in human immunodeficiency virus-1 subtype C: a case study of genetic compartmentalization and biomarker dynamics. J. Neurovirol. 24, 786–796 (2018). https://doi.org/10.1007/s13365-018-0672-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13365-018-0672-y