
Abstract
In neurodegenerative diseases, changes in neuronal proteins in the cerebrospinal fluid and blood are viewed as potential biomarkers of the primary pathology in the central nervous system (CNS). Recent reports suggest, however, that level of neuronal proteins in fluids also alters in several types of epilepsy in various age groups, including children. With increasing evidence supporting clinical and sub-clinical seizures in Alzheimer’s disease, Lewy body dementia, Parkinson’s disease, and in other less common neurodegenerative conditions, these findings call into question the specificity of neuronal protein response to neurodegenerative process and urge analysis of the effects of concomitant epilepsy and other comorbidities. In this article, we revisit the evidence for alterations in neuronal proteins in the blood and cerebrospinal fluid associated with epilepsy with and without neurodegenerative diseases. We discuss shared and distinctive characteristics of changes in neuronal markers, review their neurobiological mechanisms, and consider the emerging opportunities and challenges for their future research and diagnostic use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Neurodegenerative diseases are characterized by progressive age-dependent death of neurons in the central nervous system (CNS) with related decline of specific brain functions. Two distinctive features make neurons particularly susceptible to degeneration: (1) incompetence for self-renewal and (2) deterioration in homeostatic mechanisms over lifetime [1, 2]. With aging as the main risk factor, neurodegenerative diseases, which include increasingly common Alzheimer’s disease (AD) and associated dementias, Parkinson’s disease (PD), Lewy body dementia (LBD), and several less known conditions, are on the rise, with no cure currently available [3–5]. The lack of therapies is partly due to the shortage of mechanistic data and effective means for early diagnosis, which, if attained, might facilitate medical interventions before the onset of neuronal damage and irreversible functional loss.
Post-mortem histopathological examination remains the gold standard for differential diagnosis of neurodegenerative diseases (Fig. 1). As the method is applied to brain autopsy, it is of no clinical or therapeutic value to patients. The commonly utilized brain imaging and neurophysiological recordings while highly instructive for revealing anatomical and functional changes are of limited sensitivity for detecting subtle alterations during the early stages of pathology [6–10]. Cortical thinning and atrophy of selected brain regions, for instance, which are taken as imaging biomarkers of brain pathology in AD and LBD, appear at more advanced disease stages, indicating a widespread degeneration of neurons [6, 11–15]. Likewise, changes in neuronal activity detected by electroencephalography (EEG) reflect large-scale impairments of brain connectivity and neural synchrony, inferring a breakdown of long-range connections with disruptions in subcortical modulator influence [16–18]. Over recent years, a rapidly expanding portfolio of molecular biomarkers has shown major promise for the detection of early neurodegenerative processes, which include alterations in a variety of neuronal proteins and their autoantibodies in the blood and cerebrospinal fluid (CSF) of patients [19–23]. These advances have transformed the basic tenets of diagnostics and clinical studies [20, 22, 24, 25], paving a way for new prognostic and treatment opportunities.

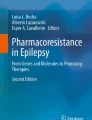
Biomarkers of epilepsy and neuronal proteins. a, d–f Examples of readouts used for diagnosis of epilepsy. a EEG and 18F-FDG PET are utilized commonly for detecting super-synchronous electrical activity (seizures) and mapping the location of the epileptic foci based on the level of glucose metabolism, respectively (top and bottom panels). In EEG, epileptic seizures are registered as widespread neuronal synchrony recorded by multiple electrodes (E1-5), while PET imaging shows a reduction in glucose metabolism in the affected brain region, exemplified as left temporal lobe hypometabolism (HMB). TLE—temporal lobe epilepsy. Reproduced with permission from [26]. d T1-weighted MRI images comparing cortical thinning in chronic epilepsy: annualized rate in people with epilepsy, with disease duration of more (top) or less (bottom) than 5 years after the onset of the first seizure. Reproduced with permission [27]. e NeuN-stained sections of hippocampi from patients with medial temporal lobe epilepsy with and without hippocampal sclerosis (left and right) without and with significant neuronal loss. Scale bars: 1 mm. Reproduced with permission from [28]. f Tau accumulation in TLE and hippocampal sclerosis: CA4 neurons labeled with neurofilament light-chain (NF-L) surrounded by pTau/AT8-positive synaptic-like processes in the cell body and axons, or dendritic marker MAP2. Reproduced with permission from [29]. b, c Schematic representation of physiological expression sites of neuronal proteins found in CSF and blood in epilepsy. NG neurogranin, APP amyloid precursor protein, NMDAR N-methyl-d-aspartate receptor, α-SYN α-synuclein, AP action potential, EPSP excitatory postsynaptic potential
Notwithstanding major advantages, molecular biomarkers of neurodegenerative diseases have considerable limitations, which include relative specificity and significant variability of the readouts, partly because of the overt and latent comorbidities [21, 23, 30]. Among the latter, epilepsy is of key interest, partly due to the growing recognition of the effects of seizures on profiles of neuronal proteins in blood and CSF. Given the increasing evidence for alterations in neuronal proteins in biological fluids associated with multiple types of seizures, there is a pressing need in elucidating their origin and interactions with established molecular biomarkers of epilepsy [31–33], as well as characterising their response to antiseizure medications (ASM) [34, 35]. In this study, we review changes in neuronal markers in CSF and blood in epilepsy with and without neurodegenerative diseases. We explore neurobiological mechanisms underlying alterations in molecular biomarkers and consider the emerging opportunities and challenges for their diagnostic and clinical use.
Molecular Biomarkers of Neurodegenerative Diseases: An Overview
In neurodegenerative diseases, an increase in the level of neuronal proteins and their fragments in CSF and blood are viewed as markers of injury and loss of nerve cells. Due to differential distribution in various neuronal compartments and the specific role played in pathobiology, some of the changes in neuronal proteins can provide additional clues about the type of pathology and the extent of the damage. Alterations in Aβ and tau, for instance, are explored primarily as indicators of amyloid and neurofibrillary tangle pathology and related neuronal loss, while the increase in α-synuclein, neurogranin, synaptic vesicle glycoprotein 2A and synaptosomal-associated protein 25 kD (SNAP-25) are viewed as markers of synaptic damage. The rise in neurofilament light chain (NF-L) level in fluids, on the other hand, is taken predominantly as a marker of axonal injury leading to a collapse of long-range connections [25] (Fig. 1).
In early preclinical and advanced stages of AD, most reports show a notable reduction in the level of Aβ1-42 in CSF and serum, with alternatively cleaved amyloid precursor protein (APP) fragments also reduced compared to age matched controls [36–38]. The level of tau protein increases in the blood and CSF in several neurodegenerative conditions (tauopathies), including AD, frontotemporal dementia (FTD), PD and LBD, amyotrophic lateral sclerosis, and prion disease [30, 39, 40]. In AD and related dementias, total tau and phosphorylated tau (t- and p-tau, respectively) in fluids are significantly higher compared with healthy controls, and correlate with the cognitive decline of patients, with very high levels of t-tau and p-tau in CSF predicting poor clinical outcomes [41–43]. An increase in α-synuclein is regarded mainly with synaptic loss and neuronal degeneration of PD and LBD, with a significant increase of this protein, also detected in biofluids [44, 45]. Like α-synuclein and tau protein, higher levels of NF-L were found in CSF and blood of multiple neurodegenerative diseases, which correlates with axonal breakdown [46–48]. In contrast to α-synuclein and some other proteins enriched in presynaptic terminals (i.e., BACE1 and SNAP-25), neurogranin is a post-synaptic protein of glutamatergic neurons, with its rise in blood and CSF taken as an indicator of damage and loss of dendritic spines [49, 50].
Despite important differences in their molecular pathology and clinical presentation, neurodegenerative diseases share important aspects of their pathobiology, leading to neuronal death. Some neurodegenerative diseases also share comorbidities, which can influence the molecular pathology and profiles of biomarkers. With aging and neurodegenerative disease-related increase in the odds of epilepsy, the impact of seizures on neuronal protein changes has become of major research and clinical interest. In AD, for instance, the risk of seizures can be as high as 35–50% [51–56]. High incidences of seizures were also reported in corticobasal degeneration, LBD, FTD, and PD [52, 54]. As detailed below, several types of epilepsy can alter levels of neuronal proteins in CSF and blood, which warrant comprehensive analysis to decide on their potential effects on profiles of molecular biomarkers of neurodegenerative diseases.
Aβ and Other APP Fragments in Biofluids of Epilepsy
It has long been known that AD and temporal lobe epilepsy share several histopathological features, including neuronal injury, gliosis, inflammation, and amyloid pathology [57, 58]. Senile plaques have been described in autopsies of patients with epilepsy before the first report of plaques in AD brain samples [59], with higher incidents of age-related amyloid pathology reported in patients with epilepsy than in age-matched controls without epilepsy [60]. Histopathological analysis of amyloid plaques in temporal lobectomy specimens showed both diffuse and neuritic plaques, which were stained with Bodian and Congo red but not with Gallyas methods [60, 61]. These findings implied that despite shared morphology and inclusion of Aβ, senile plaques of epilepsy are devoid of fibrillary tangles.
While the mechanisms for the convergence of histopathological features of AD and epilepsy brain samples remain elusive, growing data imply that neuronal hyperactivity associated with seizures can influence APP processing, as reflected in changes of Aβ isoforms and fragments of soluble APP in CSF [62]. Shahim and co-workers compared levels of Aβx-38, Aβx-40, Aβx-42, Aβ1-42, and sAPP fragments in CSF of patients with single and repetitive generalized tonic–clonic and partial seizures, and non-convulsive status epilepticus (SE) [62] (Table 1). There were no overt differences in Aβ1-42 or sAPP between epileptic patients and controls. However, in patients with repetitive partial seizures, the levels of Aβx-38 and Aβx-40 were higher compared to those with non-convulsive SE, single partial seizures, and controls, while the Aβx-42 was increased in both, patients with single and repetitive partial seizures relative to non-convulsive SE. These findings suggest that the described alterations in APP fragments might result from changes in its processing without neurodegenerative pathology. Interestingly, a comparative analysis of Aβ1-42 and several other neuronal markers in the CSF of AD patients with and without epilepsy showed lower levels of this peptide in AD patients with epilepsy [63]. In the same study, levels of p-tau and t-tau in CSF were enhanced by epileptic activity in AD patients [63]. To investigate if alterations in neuronal proteins of CSF can differentiate prodromal late-onset AD with and without seizures, their variations were quantified and compared [64]. Although the results of this analysis showed no difference, there was a significant correlation of the dynamics of Aβ1-42 and Aβ1-40 in CSF with interictal epileptiform discharges and EEG delta activity. Overall, it emerges that while epileptic seizures per se do not alter Aβ1-40 and Aβ1-42 in CSF, in AD patients with epileptic seizures, the level of CSF Aβ1-42 is lower as compared to those without seizures.
Tau in Biofluids of Epilepsy
Several reports have shown that the level of t-tau and p-tau is enhanced in the CSF and blood of patients with a single episode of self-limiting [65, 66] or reoccurring seizures [67, 69] (Table 2). Comparison of tau, glial fibrillary acidic protein (GFAP), ubiquitin C-terminal hydrolase-1 and NF-L in blood drawn at baseline, immediately or post 2, 6, and 24 h after a tonic–clonic seizure, demonstrated that all markers were increased postictally and returned to normal levels within hours, with tau changes being most prominent [66]. The authors concluded that both self-limited and reoccurring tonic–clonic seizures can lead to neuronal injury with release of tau protein. Another report addressed the level of tau protein in the blood after acute symptomatic seizures and in poststroke epilepsy (PSE) caused by thrombectomy [70]. No patient included in this study had epilepsy before the intervention, with some of the treated patients developing acute symptomatic seizures while others developed PSE. As the number of patients in this study was low, the results need independent verification in larger cohorts. Tau changes in serum and CSF were analyzed and compared also between patients with autoimmune epilepsy, genetic generalized epilepsy, and psychogenic non-epileptic seizures (PNES) to find if they could assist in differential diagnosis [71]. Neither serum nor CSF tau differed between these groups, implying that tau increments in other studies could involve additional effects associated with seizures.
Tau profile has been also analyzed in SE using a lumbar puncture, with patients stratified based on their response to ASM, disabilities, and epilepsy outcomes [68]. The levels of t-tau and p-tau were elevated in most of the SE patients, with fluid t-tau values higher in drug-refractory cases compared to those responsive to ASM [68]. In patients with especially high t-tau, the extent of tau increase correlated with the duration of SE. Analysis of the t-tau and p-tau variations and changes in their ratio in CSF collected 48 h after epileptic activity with tonic–clonic or secondary generalized seizures revealed that some patients with acute or remote symptomatic seizures showed altered t-tau levels with p-tau/t-tau ratio differing from controls [65]. As noted earlier, unlike Aβ1-42, the level of t-tau and p-tau in fluids was higher in AD cases with epilepsy [63]. It is interesting to note also that in patients with chronic temporal lobe epilepsy (TLE), the level of t-tau in CSF was lower compared to healthy individuals, while p-tau showed no difference [73]. Measurements of the p-tau/t-tau ratio, on the other hand, yielded higher values in TLE, with changes correlating with the extent of the brain white matter loss. A meta-analysis of children affected by eight different neurological conditions revealed that the concentration of t-tau was significantly increased in epilepsy, similar to that in infectious and inflammatory diseases of the CNS, and showed the highest predictive accuracy for epilepsy and progressive encephalopathy [72]. This report is of special interest as it excludes the effects of aging and related degenerative conditions on dynamics of neuronal and glial proteins in CSF and blood.
NF-L in Biofluids of Epilepsy
NF-L is another neuronal protein explored as a biomarker of neurodegenerative diseases, with single episodes and reoccurring seizures causing its increase in CSF and blood [74–76] (Table 3). Like studies of tau protein, in blood samples drawn at baseline, immediately after a tonic–clonic seizure and following 2, 6, and 24 h, NF-L was significantly increased after seizures and returned to normal level within several hours [66]. Giovannini and co-workers analyzed changes in NF-L in SE and drug-resistant epilepsy patients and compared them with healthy controls [75]. SE patients showed higher serum NF-L versus patients with refractory epilepsy and controls without epilepsy. Of note, in patients with SE, alterations in serum NF-L showed a stronger correlation with its changes in the CSF, as compared to t-tau protein. The increase in NF-L was more prominent in SE, extending beyond 24 h in refractory/super refractory SE, as well as in patients who died within 30 days, or who presented worsening clinical outcomes. It is worth stressing that NF-L dynamics correlated with ASM response, duration of treatment, and clinical outcomes, offering a potential readout for seizure-related neuronal damage and recovery [75]. An increase in NF-L has been also reported in a study comparing drug-resistant with well-controlled epilepsy and healthy cohort [76]. Analysis of blood samples drawn during the clinical interictal period showed significantly higher levels of NF-L in patients with refractory epilepsy.
A comparative analysis of several neuronal and glial proteins in adults with new-onset self-limiting seizures, chronic epilepsy, and PSE showed significant differences in NF-L between these conditions, with at least 2 years of follow-up demonstrating higher NF-L in PSE vs. self-limiting single seizure cases, and with overall levels of NF-L in patients with chronic epilepsy and PSE exceeding those in patients with single seizure episodes [74]. The same group assessed alterations in NF-L, tau, GFAP, S100, and neuron-specific enolase (NSE) in blood after incidents of symptomatic seizures in patients with a stroke leading to PSE [70]. No patient showed epilepsy before the ischemic stroke. The follow-up time (to death or last medical records review) of 0–4.5 years revealed a 2-year estimated PSE risk of 5.3%. The levels of neuronal and glial proteins in the blood in epileptic patients were above the cohort median. However, the number of PSE cases in this report was small, warranting additional studies. Analysis of neuronal proteins (tau, Aβ42, and NF-L) in CSF were also carried out in patients with anti-leucine-rich glioma-inactivated 1 encephalitis (anti-LGI-1), AD, Creutzfeldt-Jakob’s disease, and primary psychiatric disorders [77]. The concentration of NF-L in AD and anti-LGI-1 encephalitis was comparable and higher than that in psychiatric disorders, but lower than in Creutzfeldt-Jakob’s disease. In anti-LGI-1 encephalitis presenting epilepsy, levels of NF-L were enhanced further compared to cases without epilepsy [77]. Examination of NF-L in CSF of pediatric patients with epilepsy, brain tumor, infectious and inflammatory CNS disorders, static encephalopathy, movement disorders, miscellaneous disorders, and progressive encephalopathy groups with comparison to a control group showed that NF-L was higher in progressive encephalopathy, epilepsy, infectious and inflammatory disorders [72]. Importantly, t-tau, GFAP, and NF-L responded differently to these conditions.
It is interesting to note that in young children (6 months to 5 years), measurements of serum NF-L associated with febrile and epileptic seizures within a few hours after the convulsion revealed no difference as compared to age-matched controls [78]. In multivariable analysis, age was the most important predictor of the rise in serum NF-L, followed by gender and C reactive protein. Studies of the correlation between NF-L changes with the duration of seizures or the time elapsed from seizure onset to blood sampling have revealed no interactions [78]. A similar analysis of the phosphorylated NF-heavy chain (pNF-H) in children showed that prolonged febrile seizures cause a strong increase in serum pNF-H, while brief febrile seizures had no effects [79].
Other Neuronal Proteins in Biofluids of Epilepsy
Neurogranin and α-synuclein are other two neuronal proteins explored as biomarkers of neurodegenerative diseases. Regulation of calmodulin activity in dendritic spines of glutamatergic synapses makes neurogranin an important molecular switch of synaptic plasticity [80, 81]. Associated with neurodegenerative diseases increase in neurogranin concentration in CSF and blood has therefore been viewed as a specific marker of disruption of synaptic integrity and plasticity. A recent report has shown that neurogranin changes in biofluids can distinguish epileptic seizures from psychogenic non-epileptic seizures (PNES) in adults [82] (Table 4). This carefully conducted study excluded from analysis patients with infectious disease, dementia, stroke, Creutzfeldt-Jacobs’s disease, and brain abscess, as well as patients with a history of traumatic brain injury that could cause neuronal damage or compromise the integrity of the blood–brain barriers. The results of this analysis showed that neurogranin levels in patients with epileptic seizures (confirmed with EEG data) were significantly higher than in PNES and non-epileptic controls [82].
As opposed to neurogranin, α-synuclein is enriched in presynaptic terminals of axons, with evidence suggesting its upregulation in neurons of preclinical models of epilepsy [85]. Clinical data show that α-synuclein level is increased in serum and CSF in children and adults with a history of seizures, which does not respond to ASM [84, 83]. The results of comparative analysis of α-synuclein in serum and CSF of various subgroups of patients indicate that it is increased in cohorts with intractable epilepsy, whereas there was no difference in groups of patients with newly diagnosed or non-intractable epilepsy. These observations led the authors to conclude that the rise of α-synuclein in the serum and CSF may assist in the differential diagnosis of intractable epilepsy [83]. Choi and co-workers compared profiles of α-synuclein and cytokines in serum and exosomes in children with epilepsy and acquired demyelinating disorders of CNS, with readouts assessed against healthy age-matched children. It was found that like in adults, the concentration of α-synuclein and IL-1β were increased in serum and exosomes collected within 48 h after seizures or after relapse of neurological symptoms of autoimmune demyelinating disorders as compared to age-matched controls, and correlated with the severity of epilepsy [84]. Of note, the level of α-synuclein in exosomes is closely related to its level in serum, implying that α-synuclein in both serum and exosomes could help in predicting the severity of children’s epilepsy.
Release of Neuronal Proteins and Exchange Between CSF and Blood
Although the increase of neuronal proteins in biological fluids of patients with neurodegenerative diseases is viewed primarily in association with the breakdown of neurons and synaptic connections [25, 86], important questions remain over mechanisms underlying their changes related to seizures, given the lack of evidence for neurodegeneration in most types of epilepsy [87–92]. It is tempting to speculate that the bulk of neuronal proteins released during epileptic hyperactivity might go through physiological pathways mediating the secretion of neuropeptides, hormones, and trophic factors from nerve cells [86, 93–95]. Ample evidence also supports the potential involvement of intracellular endosomes in breaking out of proteins from neurons, via exosomes of endosomal origin as well as through budding and fission of the plasma membrane [96–98]. Like in neurodegenerative diseases, in chronic epilepsy, protein-containing endosomes can become abundant and associate with enhanced autophagy and protein secretion pathways [98, 99]. Importantly, the production and release of microvesicles can be promoted by a strong and persistent rise in intracellular Ca2+ as well as by cell stress response, which are key characteristics of the pathobiology of epilepsy [100–102]. The prolonged rise of intracellular free Ca2+ during intense neuronal activity, in fact, is required for induction of the physiological release of peptides, hormones, and trophic factors from neurons and other secretory cells [93–95, 103]. Finally, associated with epilepsy enhancement of protein degradation mechanisms with release of their fragments in the extracellular space [86, 99, 104] could also contribute to the kinetic and the extent of the variations of neuronal markers in CSF and blood.
It should be noted that in addition to the rate of release from hyperactive and damaged neurons, changes in neuronal proteins in CSF and peripheral circulation may be also influenced by the speed of their exchange between the two compartments, as well as by their degradation by extracellular proteases [105–107]. Along with widely accepted efflux routes of neuronal proteins from the CNS across compromised blood–brain barriers, in epilepsy, they may also escape along the walls of brain arteries and arterioles [106], basement membrane of capillaries [108, 109], as well as through glymphatic drainage routes [110, 111], which are subject to future research.
Summary and Future Directions
Epilepsy is among the most prevalent comorbidities of neurodegenerative diseases. Given the global aging population and neurodegenerative diseases on the rise, their intersection with epilepsy has become of major research and clinical interest. Recent data suggest that the incidents of epilepsy in older age and patients with neurodegenerative diseases are widely underrated, mainly due to poor screening and subclinical forms of epilepsy. The mounting clinical evidence implies a complex and dynamic relationship between these morbidities, with both sub-clinical and clinical seizures accelerating the progression and exacerbating outcomes of neurodegenerative diseases (Fig. 2).

Schematic representation of cause-consequence relation of neuronal injury proteins and epilepsy. In neurodegenerative diseases, several mechanisms contributing to epileptic activity have been described. These include (top, from left to right) activation of NMDAR and nAChR by soluble oligomers of amyloid-β, activation of NMDAR and mAChR by MAP tau protein, cleavage of NaV channel β-subunit by BACE1 protease with dysregulation of Na+ channel activity, impairments of Ca2+ signalling caused by C-terminal fragment (CTF), and FE65 domain of amyloid precursor protein (APP) released by γ-secretase cleavage, inhibition of Na/K+ ATPase, and activation of NMDAR-mediated drive by α-synuclein, and inhibition of glutamate clearance and Na/K+ ATPase dysregulation by huntingtin (mHtt) protein [112, 113]. Contributed to these changes epileptic activity leads to the excessive release of synaptic and ectopic glutamate and excitotoxicity [114, 115], which may contribute to neuronal hyperactivity and injury with the release of intracellular proteins. Neuronal proteins explored as biomarkers of neurodegenerative diseases are generally divided as (1) markers of amyloid pathology with neurodegeneration (top), (2) markers of axonal breakdown (i.e., neurofilament light chain, NLF-L), and (3) synaptic degeneration (NG, SV2, and SNAP-25). Amyloid-β, tau, and α-synuclein under pathological conditions can oligomerize and form non-selective cation pores facilitating Ca2+ influx with membrane depolarization, which can cause pathological activity in neurons
Throughout this study, we discussed reports of changes in neuronal proteins in CSF and blood associated with different types of epilepsy with and without neurodegenerative diseases. Based on the dynamics of neuronal markers in fluids and putative release mechanisms of peptides and proteins from neurons, as well as on the lack of evidence for neuronal degeneration in most types of epilepsy, it is reasonable to assume that the transient changes of neuronal markers in CSF and blood related with self-limiting and tonic-clinic seizures could reflect (1) increase in protein metabolism and release from hyperactive neurons, (2) vesicular (exosomal) discharge from stressed and hyperactive neurons, and (3) seizure-related changes in the rate of neuronal protein exchange between CSF and blood. In contrast, the strong and lasting increase of NF-L and tau in SE is likely indicate the extent of the cellular injury with degeneration and associated breakout of neuronal proteins.
With growing recognition of the prevalence of sub-clinical and clinical seizures in the most common neurodegenerative diseases and increasing use of neuronal protein changes as disease biomarkers, addressing the underlying mechanisms and clinical implications are well warranted. Combined with studies of the effects of ASM on dynamics of neuronal proteins and neurodegenerative process, the elucidation of the key mechanistic and translational aspects of neuronal biomarkers shared by epilepsy and neurodegenerative disease are likely to set us on a course to better diagnosis and therapies of these conditions.
Data Availability
This is a review article and does not contain original data. All questions related to the content of this study should be addressed to the corresponding author.
Abbreviations
- CNS:
-
Central nervous system
- AD:
-
Alzheimer’s disease
- PD:
-
Parkinson’s disease
- LBD:
-
Lewy body dementia
- NF-L:
-
Neurofilament light chain
- SV2:
-
Synaptic vesicle glycoprotein 2
- SNAP-25:
-
Synaptosomal-associated protein 25 kD
- CSF:
-
Cerebrospinal fluid
- APP:
-
Amyloid precursor protein
- FTD:
-
Front-temporal dementia
- t-tau:
-
Total tau
- BACE1:
-
β-Secretase amyloid cleaving enzyme
- sAPP:
-
Soluble amyloid precursor protein
- EEG:
-
Electroencephalography
- GFAP:
-
Glial fibrillary acidic protein
- PSE:
-
Poststroke epilepsy
- AME:
-
Autoimmune-mediated epilepsy
- PNES:
-
Psychogenic non-epileptic seizures
- ASM:
-
Antiseizure medication
- TLE:
-
Temporal lobe epilepsy
- NSE:
-
Neuron-specific enolase
- NF-H:
-
NF-heavy chain
- HS:
-
Hippocampal sclerosis
- MAP2:
-
Microtubule associate protein 2
- NG:
-
Neurogranin
- EPSP:
-
Excitatory postsynaptic potential
- AP:
-
Action potential
References
Mattson MP, Magnus T. Ageing and neuronal vulnerability. Nat Rev Neurosci. 2006;7:278–94.
Saxena S, Caroni P. Selective neuronal vulnerability in neurodegenerative diseases: from stressor thresholds to degeneration. Neuron. 2011;71:35–48.
Hou Y, Dan X, Babbar M, Wei Y, Hasselbalch SG, Croteau DL, Bohr VA. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol. 2019;15:565–81.
G.B.D.D.F. Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019, Lancet. Public Health. 2022;7:e105–25.
Wareham LK, Liddelow SA, Temple S, Benowitz LI, Di Polo A, Wellington C, Goldberg JL, He Z, Duan X, Bu G, Davis AA, Shekhar K, Torre A, Chan DC, Canto-Soler MV, Flanagan JG, Subramanian P, Rossi S, Brunner T, Bovenkamp DE, Calkins DJ. Solving neurodegeneration: common mechanisms and strategies for new treatments. Mol Neurodegener. 2022;17:23.
Young PNE, Estarellas M, Coomans E, Srikrishna M, Beaumont H, Maass A, Venkataraman AV, Lissaman R, Jimenez D, Betts MJ, McGlinchey E, Berron D, O’Connor A, Fox NC, Pereira JB, Jagust W, Carter SF, Paterson RW, Scholl M. Imaging biomarkers in neurodegeneration: current and future practices. Alzheimers Res Ther. 2020;12:49.
Ovsepian SV, Olefir I, Westmeyer G, Razansky D, Ntziachristos V. Pushing the boundaries of neuroimaging with optoacoustics. Neuron. 2017;96:966–88.
Chen JJ. Functional MRI of brain physiology in aging and neurodegenerative diseases. Neuroimage. 2019;187:209–25.
Hallett M, de Haan W, Deco G, Dengler R, Di Iorio R, Gallea C, Gerloff C, Grefkes C, Helmich RC, Kringelbach ML, Miraglia F, Rektor I, Strycek O, Vecchio F, Volz LJ, Wu T, Rossini PM. Human brain connectivity: clinical applications for clinical neurophysiology. Clin Neurophysiol. 2020;131:1621–51.
Koikkalainen J, Rhodius-Meester H, Tolonen A, Barkhof F, Tijms B, Lemstra AW, Tong T, Guerrero R, Schuh A, Ledig C, Rueckert D, Soininen H, Remes AM, Waldemar G, Hasselbalch S, Mecocci P, van der Flier W, Lotjonen J. Differential diagnosis of neurodegenerative diseases using structural MRI data. Neuroimage Clin. 2016;11:435–49.
Jack CR Jr, Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, Shaw LM, Vemuri P, Wiste HJ, Weigand SD, Lesnick TG, Pankratz VS, Donohue MC, Trojanowski JQ. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013;12:207–16.
Vemuri P, Jack CR Jr. Role of structural MRI in Alzheimer’s disease. Alzheimers Res Ther. 2010;2:23.
Jack CR Jr, Knopman DS, Jagust WJ, Shaw LM, Aisen PS, Weiner MW, Petersen RC, Trojanowski JQ. Hypothetical model of dynamic biomarkers of the Alzheimer’s pathological cascade. Lancet Neurol. 2010;9:119–28.
Whitwell JL, Jack CR Jr, Parisi JE, Knopman DS, Boeve BF, Petersen RC, Ferman TJ, Dickson DW, Josephs KA. Rates of cerebral atrophy differ in different degenerative pathologies. Brain. 2007;130:1148–58.
Mak E, Su L, Williams GB, O’Brien JT. Neuroimaging characteristics of dementia with Lewy bodies. Alzheimers Res Ther. 2014;6:18.
Babiloni C, Blinowska K, Bonanni L, Cichocki A, De Haan W, Del Percio C, Dubois B, Escudero J, Fernandez A, Frisoni G, Guntekin B, Hajos M, Hampel H, Ifeachor E, Kilborn K, Kumar S, Johnsen K, Johannsson M, Jeong J, LeBeau F, Lizio R, Lopes da Silva F, Maestu F, McGeown WJ, McKeith I, Moretti DV, Nobili F, Olichney J, Onofrj M, Palop JJ, Rowan M, Stocchi F, Struzik ZM, Tanila H, Teipel S, Taylor JP, Weiergraber M, Yener G, Young-Pearse T, Drinkenburg WH, Randall F. What electrophysiology tells us about Alzheimer’s disease: a window into the synchronization and connectivity of brain neurons. Neurobiol Aging. 2020;85:58–73.
Jeong J. EEG dynamics in patients with Alzheimer’s disease. Clin Neurophysiol. 2004;115:1490–505.
McMackin R, Muthuraman M, Groppa S, Babiloni C, Taylor JP, Kiernan MC, Nasseroleslami B, Hardiman O. Measuring network disruption in neurodegenerative diseases: new approaches using signal analysis. J Neurol Neurosurg Psychiatry. 2019;90:1011–20.
Solje E, Benussi A, Buratti E, Remes AM, Haapasalo A, Borroni B. State-of-the-art methods and emerging fluid biomarkers in the diagnostics of dementia—a short review and diagnostic algorithm. Diagnostics (Basel). 2021;11.
Zetterberg H, Blennow K. Moving fluid biomarkers for Alzheimer’s disease from research tools to routine clinical diagnostics. Mol Neurodegener. 2021;16:10.
Simren J, Ashton NJ, Blennow K, Zetterberg H. An update on fluid biomarkers for neurodegenerative diseases: recent success and challenges ahead. Curr Opin Neurobiol. 2020;61:29–39.
Kocurova G, Ricny J, Ovsepian SV. Autoantibodies targeting neuronal proteins as biomarkers for neurodegenerative diseases. Theranostics. 2022;12:3045–56.
Ovsepian SV, O’Leary VB. Adult neurogenesis in the gut, homeostatic autoimmunity and neurodegenerative disease biomarkers. Neuroscience. 2022. https://doi.org/10.1016/j.neuroscience.2022.09.019.
Barro C, Zetterberg H. The blood biomarkers puzzle—a review of protein biomarkers in neurodegenerative diseases. J Neurosci Methods. 2021;361:109281.
Hansson O. Biomarkers for neurodegenerative diseases. Nat Med. 2021;27:954–63.
Setoain X, Carreno M, Pavia J, Marti-Fuster B, Campos F, Lomena F. PET and SPECT in epilepsy. Rev Esp Med Nucl Imagen Mol. 2014;33:165–74.
Galovic M, van Dooren VQH, Postma TS, Vos SB, Caciagli L, Borzi G, Cueva Rosillo J, Vuong KA, de Tisi J, Nachev P, Duncan JS, Koepp MJ. Progressive cortical thinning in patients with focal epilepsy. JAMA Neurol. 2019;76:1230–9.
Jardim AP, Duarte JTC, Lancellotti CLP, Carrete H Jr, Centeno RS, Scorza CA, Cavalheiro EA, Guaranha MSB, Yacubian EMT. Granule cell dispersion is associated with hippocampal neuronal cell loss, initial precipitating injury, and other clinical features in mesial temporal lobe epilepsy and hippocampal sclerosis. Seizure. 2021 Aug;90:60-66. https://doi.org/10.1016/j.seizure.2021.05.024. Epub 2021 May 31. PMID: 34162493.
Thom M, Koepp M. Tau protein in drug-resistant epilepsy and cognitive decline. In: Janigro D, Nehlig A, Marchi A (Eds.) Inflammation and Epilepsy: New Vistas. Progress in Inflammation Research, Springer; 2021.
Obrocki P, Khatun A, Ness D, Senkevich K, Hanrieder J, Capraro F, Mattsson N, Andreasson U, Portelius E, Ashton NJ, Blennow K, Scholl M, Paterson RW, Schott JM, Zetterberg H. Perspectives in fluid biomarkers in neurodegeneration from the 2019 biomarkers in neurodegenerative diseases course—a joint PhD student course at University College London and University of Gothenburg. Alzheimers Res Ther. 2020;12:20.
Pitkanen A, Ndode-Ekane XE, Lapinlampi N, Puhakka N. Epilepsy biomarkers—toward etiology and pathology specificity. Neurobiol Dis. 2019;123:42–58.
Rana A, Musto AE. The role of inflammation in the development of epilepsy. J Neuroinflammation. 2018;15:144.
Hanin A, Lambrecq V, Denis JA, Imbert-Bismut F, Rucheton B, Lamari F, Bonnefont-Rousselot D, Demeret S, Navarro V. Cerebrospinal fluid and blood biomarkers of status epilepticus. Epilepsia. 2020;61:6–18.
Li Z, Cao W, Sun H, Wang X, Li S, Ran X, Zhang H. Potential clinical and biochemical markers for the prediction of drug-resistant epilepsy: a literature review. Neurobiol Dis. 2022;174:105872.
Zaitsev AV, Smolensky IV, Jorratt P, Ovsepian SV. Neurobiology, functions, and relevance of excitatory amino acid transporters (EAATs) to treatment of refractory epilepsy. CNS Drugs. 2020;34:1089–103.
Molinuevo JL, Ayton S, Batrla R, Bednar MM, Bittner T, Cummings J, Fagan AM, Hampel H, Mielke MM, Mikulskis A, O’Bryant S, Scheltens P, Sevigny J, Shaw LM, Soares HD, Tong G, Trojanowski JQ, Zetterberg H, Blennow K. Current state of Alzheimer’s fluid biomarkers. Acta Neuropathol. 2018;136:821–53.
Zou K, Abdullah M, Michikawa M. Current biomarkers for Alzheimer's disease: from CSF to blood. J Pers Med. 2020;10.
Janelidze S, Stomrud E, Palmqvist S, Zetterberg H, van Westen D, Jeromin A, Song L, Hanlon D, Tan Hehir CA, Baker D, Blennow K, Hansson O. Plasma beta-amyloid in Alzheimer’s disease and vascular disease. Sci Rep. 2016;6:26801.
Schraen-Maschke S, Sergeant N, Dhaenens CM, Bombois S, Deramecourt V, Caillet-Boudin ML, Pasquier F, Maurage CA, Sablonniere B, Vanmechelen E, Buee L. Tau as a biomarker of neurodegenerative diseases. Biomark Med. 2008;2:363–84.
Sergeant N, Delacourte A, Buee L. Tau protein as a differential biomarker of tauopathies. Biochim Biophys Acta. 2005;1739:179–97.
Stomrud E, Hansson O, Zetterberg H, Blennow K, Minthon L, Londos E. Correlation of longitudinal cerebrospinal fluid biomarkers with cognitive decline in healthy older adults. Arch Neurol. 2010;67:217–23.
Clark CM, Xie S, Chittams J, Ewbank D, Peskind E, Galasko D, Morris JC, McKeel DW Jr, Farlow M, Weitlauf SL, Quinn J, Kaye J, Knopman D, Arai H, Doody RS, DeCarli C, Leight S, Lee VM, Trojanowski JQ. Cerebrospinal fluid tau and beta-amyloid: how well do these biomarkers reflect autopsy-confirmed dementia diagnoses? Arch Neurol. 2003;60:1696–702.
Karikari TK, Pascoal TA, Ashton NJ, Janelidze S, Benedet AL, Rodriguez JL, Chamoun M, Savard M, Kang MS, Therriault J, Scholl M, Massarweh G, Soucy JP, Hoglund K, Brinkmalm G, Mattsson N, Palmqvist S, Gauthier S, Stomrud E, Zetterberg H, Hansson O, Rosa-Neto P, Blennow K. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: a diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol. 2020;19:422–33.
Magalhaes P, Lashuel HA. Opportunities and challenges of alpha-synuclein as a potential biomarker for Parkinson’s disease and other synucleinopathies. NPJ Parkinsons Dis. 2022;8:93.
Chang CW, Yang SY, Yang CC, Chang CW, Wu YR. Plasma and serum alpha-synuclein as a biomarker of diagnosis in patients with Parkinson’s disease. Front Neurol. 2019;10:1388.
Menke RA, Gray E, Lu CH, Kuhle J, Talbot K, Malaspina A, Turner MR. CSF neurofilament light chain reflects corticospinal tract degeneration in ALS. Ann Clin Transl Neurol. 2015;2:748–55.
Yuan A, Nixon RA. Neurofilament proteins as biomarkers to monitor neurological diseases and the efficacy of therapies. Front Neurosci. 2021;15:689938.
Gaetani L, Blennow K, Calabresi P, Di Filippo M, Parnetti L, Zetterberg H. Neurofilament light chain as a biomarker in neurological disorders. J Neurol Neurosurg Psychiatry. 2019;90:870–81.
Lista S, Hampel H. Synaptic degeneration and neurogranin in the pathophysiology of Alzheimer’s disease. Expert Rev Neurother. 2017;17:47–57.
Lista S, Toschi N, Baldacci F, Zetterberg H, Blennow K, Kilimann I, Teipel SJ, Cavedo E, Dos Santos AM, Epelbaum S, Lamari F, Dubois B, Nistico R, Floris R, Garaci F, Hampel H, Alzheimer Precision Medicine Initiative. Cerebrospinal fluid neurogranin as a biomarker of neurodegenerative diseases: a cross-sectional study. J Alzheimers Dis. 2017;59:1327–34.
Larner AJ. Epileptic seizures in AD patients. Neuromolecular Med. 2010;12:71–7.
Neri S, Mastroianni G, Gardella E, Aguglia U, Rubboli G. Epilepsy in neurodegenerative diseases. Epileptic Disord. 2022;24:249–73.
Xu Y, Lavrencic L, Radford K, Booth A, Yoshimura S, Anstey KJ, Anderson CS, Peters R. Systematic review of coexistent epileptic seizures and Alzheimer’s disease: Incidence and prevalence. J Am Geriatr Soc. 2021;69:2011–20.
Voglein J, Kostova I, Arzberger T, Noachtar S, Dieterich M, Herms J, Schmitz P, Ruf V, Windl O, Roeber S, Simons M, Hoglinger GU, Danek A, Giese A, Levin J. Seizure prevalence in neurodegenerative diseases-a study of autopsy proven cases. Eur J Neurol. 2022;29:12–8.
Vossel KA, Tartaglia MC, Nygaard HB, Zeman AZ, Miller BL. Epileptic activity in Alzheimer’s disease: causes and clinical relevance. Lancet Neurol. 2017;16:311–22.
Ovsepian SV, O’Leary VB. Neuronal activity and amyloid plaque pathology: an update. J Alzheimers Dis. 2016;49:13–9.
Yan XX, Cai Y, Shelton J, Deng SH, Luo XG, Oddo S, Laferla FM, Cai H, Rose GM, Patrylo PR. Chronic temporal lobe epilepsy is associated with enhanced Alzheimer-like neuropathology in 3xTg-AD mice. PLoS ONE. 2012;7:e48782.
Tombini M, Assenza G, Ricci L, Lanzone J, Boscarino M, Vico C, Magliozzi A, Di Lazzaro V. Temporal lobe epilepsy and Alzheimer’s disease: from preclinical to clinical evidence of a strong association. J Alzheimers Dis Rep. 2021;5:243–61.
Buda O, Arsene D, Ceausu M, Dermengiu D, Curca GC. Georges Marinesco and the early research in neuropathology. Neurology. 2009;72:88–91.
Mackenzie IR, Miller LA. Senile plaques in temporal lobe epilepsy. Acta Neuropathol. 1994;87:504–10.
Mackenzie IR, McLachlan RS, Kubu CS, Miller LA. Prospective neuropsychological assessment of nondemented patients with biopsy proven senile plaques. Neurology. 1996;46:425–9.
Shahim P, Rejdak R, Ksiazek P, Blennow K, Zetterberg H, Mattsson N, Rejdak K. Cerebrospinal fluid biomarkers of beta-amyloid metabolism and neuronal damage in epileptic seizures. Eur J Neurol. 2014;21:486–91.
Banote RK, Håkansson S, Zetterberg H, Zelano J. CSF biomarkers in patients with epilepsy in Alzheimer’s disease: a nation-wide study. Brain Commun. 2022;4(4).
Cretin B, Bousiges O, Hautecloque G, Philippi N, Blanc F, Dibitonto L, Martin-Hunyadi C, Sellal F. CSF in epileptic prodromal Alzheimer’s Disease: no diagnostic contribution but a pathophysiological one. Front Neurol. 2021;12:623777.
Palmio J, Suhonen J, Keranen T, Hulkkonen J, Peltola J, Pirttila T. Cerebrospinal fluid tau as a marker of neuronal damage after epileptic seizure. Seizure. 2009;18:474–7.
Nass RD, Akgun K, Elger C, Reichmann H, Wagner M, Surges R, Ziemssen T. Serum biomarkers of cerebral cellular stress after self-limiting tonic clonic seizures: an exploratory study. Seizure. 2021;85:1–5.
Costa C, Romoli M, Liguori C, Farotti L, Eusebi P, Bedetti C, Siliquini S, Cesarini EN, Romigi A, Mercuri NB, Parnetti L, Calabresi P. Alzheimer’s disease and late-onset epilepsy of unknown origin: two faces of beta amyloid pathology. Neurobiol Aging. 2019;73:61–7.
Monti G, Tondelli M, Giovannini G, Bedin R, Nichelli PF, Trenti T, Meletti S, Chiari A. Cerebrospinal fluid tau proteins in status epilepticus. Epilepsy Behav. 2015;49:150–4.
Tabuas-Pereira M, Duraes J, Lopes J, Sales F, Bento C, Duro D, Santiago B, Almeida MR, Leitao MJ, Baldeiras I, Santana I. Increased CSF tau is associated with a higher risk of seizures in patients with Alzheimer’s disease. Epilepsy Behav. 2019;98:207–9.
Eriksson H, Lowhagen Henden P, Rentzos A, Pujol-Calderon F, Karlsson JE, Hoglund K, Blennow K, Zetterberg H, Rosengren L, Zelano J. Acute symptomatic seizures and epilepsy after mechanical thrombectomy. Epilepsy Behav. 2020;104:106520.
Nass RD, Akgun K, Dague KO, Elger CE, Reichmann H, Ziemssen T, Surges R. CSF and serum biomarkers of cerebral damage in autoimmune epilepsy. Front Neurol. 2021;12:647428.
Shahim P, Darin N, Andreasson U, Blennow K, Jennions E, Lundgren J, Mansson JE, Naess K, Tornhage CJ, Zetterberg H, Mattsson N. Cerebrospinal fluid brain injury biomarkers in children: a multicenter study. Pediatr Neurol. 2013;49:31–9 e32.
Mo L, Ding X, Tan C, Liu X, Wei X, Wang H, Zhou W, Chen L. Association of cerebrospinal fluid zinc-alpha2-glycoprotein and tau protein with temporal lobe epilepsy and related white matter impairment. NeuroReport. 2019;30:586–91.
Eriksson H, Banote RK, Larsson D, Blennow K, Zetterberg H, Zelano J. Brain injury markers in new-onset seizures in adults: A pilot study. Seizure. 2021;92:62–7.
Giovannini G, Bedin R, Ferraro D, Vaudano AE, Mandrioli J, Meletti S. Serum neurofilament light as biomarker of seizure-related neuronal injury in status epilepticus. Epilepsia. 2022;63:e23–9.
Ouedraogo O, Rebillard RM, Jamann H, Mamane VH, Clenet ML, Daigneault A, Lahav B, Uphaus T, Steffen F, Bittner S, Zipp F, Berube A, Lapalme-Remis S, Cossette P, Nguyen DK, Arbour N, Keezer MR, Larochelle C. Increased frequency of proinflammatory CD4 T cells and pathological levels of serum neurofilament light chain in adult drug-resistant epilepsy. Epilepsia. 2021;62:176–89.
Lardeux P, Fourier A, Peter E, Dorey A, Muniz-Castrillo S, Vogrig A, Picard G, Rogemond V, Verdurand M, Formaglio M, Joubert B, Froment Tilikete C, Honnorat J, Quadrio I, Desestret V. Core cerebrospinal fluid biomarker profile in anti-LGI1 encephalitis. J Neurol. 2022;269:377–88.
Evers KS, Hugli M, Fouzas S, Kasser S, Pohl C, Stoecklin B, Bernasconi L, Kuhle J, Wellmann S. Serum Neurofilament Levels in Children With Febrile Seizures and in Controls. Front Neurosci. 2020;14:579958.
Matsushige T, Inoue H, Fukunaga S, Hasegawa S, Okuda M, Ichiyama T. Serum neurofilament concentrations in children with prolonged febrile seizures. J Neurol Sci. 2012;321:39–42.
Petersen A, Gerges NZ. Neurogranin regulates CaM dynamics at dendritic spines. Sci Rep. 2015;5:11135.
Pak JH, Huang FL, Li J, Balschun D, Reymann KG, Chiang C, Westphal H, Huang KP. Involvement of neurogranin in the modulation of calcium/calmodulin-dependent protein kinase II, synaptic plasticity, and spatial learning: a study with knockout mice. Proc Natl Acad Sci U S A. 2000;97:11232–7.
Kalkan A, Demirel A, Atis SE, Karaaslan EB, Ferhatlar ME, Senturk M. A new biomarker in the differential diagnosis of epileptic seizure: Neurogranin. Am J Emerg Med. 2022;54:147–50.
Rong H, Jin L, Wei W, Wang X, Xi Z. Alpha-synuclein is a potential biomarker in the serum and CSF of patients with intractable epilepsy. Seizure. 2015;27:6–9.
Choi J, Kim SY, Kim H, Lim BC, Hwang H, Chae JH, Kim KJ, Oh S, Kim EY, Shin JS. Serum alpha-synuclein and IL-1beta are increased and correlated with measures of disease severity in children with epilepsy: potential prognostic biomarkers? BMC Neurol. 2020;20:85.
Hussein AM, Eldosoky M, El-Shafey M, El-Mesery M, Ali AN, Abbas KM, Abulseoud OA. Effects of metformin on apoptosis and alpha-synuclein in a rat model of pentylenetetrazole-induced epilepsy. Can J Physiol Pharmacol. 2019;97:37–46.
Gafson AR, Barthelemy NR, Bomont P, Carare RO, Durham HD, Julien JP, Kuhle J, Leppert D, Nixon RA, Weller RO, Zetterberg H, Matthews PM. Neurofilaments: neurobiological foundations for biomarker applications. Brain. 2020;143:1975–98.
Eid T. Progressive neuronal loss in epilepsy—a long-standing conundrum finally resolved? Epilepsy Curr. 2021;21:366–8.
Rossini L, Garbelli R, Gnatkovsky V, Didato G, Villani F, Spreafico R, Deleo F, Lo Russo G, Tringali G, Gozzo F, Tassi L, de Curtis M. Seizure activity per se does not induce tissue damage markers in human neocortical focal epilepsy. Ann Neurol. 2017;82:331–41.
Thom M, Zhou J, Martinian L, Sisodiya S. Quantitative post-mortem study of the hippocampus in chronic epilepsy: seizures do not inevitably cause neuronal loss. Brain. 2005;128:1344–57.
Gorter JA, Goncalves Pereira PM, van Vliet EA, Aronica E, Lopes da Silva FH, Lucassen PJ. Neuronal cell death in a rat model for mesial temporal lobe epilepsy is induced by the initial status epilepticus and not by later repeated spontaneous seizures. Epilepsia. 2003;44:647–58.
Bertram EH 3rd, Lothman EW. Morphometric effects of intermittent kindled seizures and limbic status epilepticus in the dentate gyrus of the rat. Brain Res. 1993;603:25–31.
Mathern GW, Bertram EH III. Recurrent limbic seizures do not cause hippocampal neuronal loss: A prolonged laboratory study. Neurobiol Dis. 2021;148:105183.
Ovsepian SV, Dolly JO. Dendritic SNAREs add a new twist to the old neuron theory. Proc Natl Acad Sci U S A. 2011;108:19113–20.
Meng J, Ovsepian SV, Wang J, Pickering M, Sasse A, Aoki KR, Lawrence GW, Dolly JO. Activation of TRPV1 mediates calcitonin gene-related peptide release, which excites trigeminal sensory neurons and is attenuated by a retargeted botulinum toxin with anti-nociceptive potential. J Neurosci. 2009;29:4981–92.
van den Pol AN. Neuropeptide transmission in brain circuits. Neuron. 2012;76:98–115.
Kleijmeer M, Ramm G, Schuurhuis D, Griffith J, Rescigno M, Ricciardi-Castagnoli P, Rudensky AY, Ossendorp F, Melief CJ, Stoorvogel W, Geuze HJ. Reorganization of multivesicular bodies regulates MHC class II antigen presentation by dendritic cells. J Cell Biol. 2001;155:53–63.
Von Bartheld CS, Altick AL. Multivesicular bodies in neurons: distribution, protein content, and trafficking functions. Prog Neurobiol. 2011;93:313–40.
Nixon RA. The role of autophagy in neurodegenerative disease. Nat Med. 2013;19:983–97.
Fassio A, Falace A, Esposito A, Aprile D, Guerrini R, Benfenati F. Emerging role of the autophagy/lysosomal degradative pathway in neurodevelopmental disorders with epilepsy. Front Cell Neurosci. 2020;14:39.
Sproviero D, La Salvia S, Giannini M, Crippa V, Gagliardi S, Bernuzzi S, Diamanti L, Ceroni M, Pansarasa O, Poletti A, Cereda C. Pathological proteins are transported by extracellular vesicles of sporadic amyotrophic lateral sclerosis patients. Front Neurosci. 2018;12:487.
Tricarico C, Clancy J, D’Souza-Schorey C. Biology and biogenesis of shed microvesicles. Small GTPases. 2017;8:220–32.
Upadhya D, Shetty AK. Promise of extracellular vesicles for diagnosis and treatment of epilepsy. Epilepsy Behav. 2021;121:106499.
Ludwig M, Leng G. Dendritic peptide release and peptide-dependent behaviours. Nat Rev Neurosci. 2006;7:126–36.
Giorgi FS, Biagioni F, Lenzi P, Frati A, Fornai F. The role of autophagy in epileptogenesis and in epilepsy-induced neuronal alterations. J Neural Transm (Vienna). 2015;122:849–62.
Bakker EN, Bacskai BJ, Arbel-Ornath M, Aldea R, Bedussi B, Morris AW, Weller RO, Carare RO. Lymphatic clearance of the brain: perivascular, paravascular and significance for neurodegenerative diseases. Cell Mol Neurobiol. 2016;36:181–94.
Szentistvanyi I, Patlak CS, Ellis RA, Cserr HF. Drainage of interstitial fluid from different regions of rat brain. Am J Physiol. 1984;246:F835-844.
Ueno M, Chiba Y, Murakami R, Matsumoto K, Kawauchi M, Fujihara R. Blood-brain barrier and blood-cerebrospinal fluid barrier in normal and pathological conditions. Brain Tumor Pathol. 2016;33:89–96.
Albargothy NJ, Johnston DA, MacGregor-Sharp M, Weller RO, Verma A, Hawkes CA, Carare RO. Convective influx/glymphatic system: tracers injected into the CSF enter and leave the brain along separate periarterial basement membrane pathways. Acta Neuropathol. 2018;136:139–52.
Carare RO, Bernardes-Silva M, Newman TA, Page AM, Nicoll JA, Perry VH, Weller RO. Solutes, but not cells, drain from the brain parenchyma along basement membranes of capillaries and arteries: significance for cerebral amyloid angiopathy and neuroimmunology. Neuropathol Appl Neurobiol. 2008;34:131–44.
Hawkes CA, Hartig W, Kacza J, Schliebs R, Weller RO, Nicoll JA, Carare RO. Perivascular drainage of solutes is impaired in the ageing mouse brain and in the presence of cerebral amyloid angiopathy. Acta Neuropathol. 2011;121:431–43.
Iliff JJ, Wang M, Liao Y, Plogg BA, Peng W, Gundersen GA, Benveniste H, Vates GE, Deane R, Goldman SA, Nagelhus EA, Nedergaard M. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid beta. Sci Transl Med. 2012;4:147ra111.
Ovsepian SV, Horacek J, O’Leary VB, Hoschl C. The ups and downs of BACE1: walking a fine line between neurocognitive and other psychiatric symptoms of Alzheimer’s disease. Neuroscientist. 2021;27:222–34.
Ovsepian SV, O’Leary VB, Zaborszky L. Cholinergic mechanisms in the cerebral cortex: beyond synaptic transmission. Neuroscientist. 2016;22:238–51.
Ovsepian SV, O’Leary VB, Zaborszky L, Ntziachristos V, Dolly JO. Amyloid plaques of Alzheimer’s disease as hotspots of glutamatergic activity. Neuroscientist. 2019;25:288–97.
Ovsepian SV, Blazquez-Llorca L, Freitag SV, Rodrigues EF, Herms J. Ambient glutamate promotes paroxysmal hyperactivity in cortical pyramidal neurons at amyloid plaques via presynaptic mGluR1 receptors. Cereb Cortex. 2017;27:4733–49.
Acknowledgements
Innovation Fund Award 2022 from the University of Greenwich; Charles University, Third Faculty of Medicine Research Program COOPERATIO-207036; Medical Diagnostics and Basic Medical Sciences in ‘Medical Genetics’.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
This is a review manuscript and contains no experimental data involving humans or animals.
Conflict of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Negi, D., Granak, S., Shorter, S. et al. Molecular Biomarkers of Neuronal Injury in Epilepsy Shared with Neurodegenerative Diseases. Neurotherapeutics 20, 767–778 (2023). https://doi.org/10.1007/s13311-023-01355-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13311-023-01355-7