
Abstract
Standard treatment of early recurrence of colorectal liver metastases (CLM) after liver resection (LR) is chemotherapy followed by loco-regional therapy. We reviewed the outcome of a different strategy (“test-of-time” approach): upfront percutaneous ablation without chemotherapy. Twenty-six consecutive patients with early solitary liver-only recurrence amenable to both resection and ablation (< 30 mm, distant from vessels) undergone “test-of-time” approach were analyzed. Early recurrence had a median size of 17 mm and occurred after a median interval from LR of 4 months. Primary efficacy rate of ablation was 100%. Five patients are alive and disease-free after a mean follow-up of 46 months. Five patients had local-only recurrence; all had repeat treatment (LR = 4; Ablation = 1) without chemotherapy. Local recurrence risk was associated with incomplete ablation of 1-cm thick peritumoral margin. The remaining 16 patients had non-local recurrence, 13 early after ablation. Overall, six (23%) patients had ablation as unique treatment and 13 (50%) avoided or postponed chemotherapy (mean chemotherapy-free interval 33.5 months). Ablation without chemotherapy of early liver-only recurrence is a reliable “test-of-time” approach. It minimized the invasiveness of treatment with good effectiveness and high salvageability in case of local failure, avoided worthless surgery, and saved chemotherapy for further disease progression.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Liver metastases (CLM) are one of the major causes of death in patients affected by colorectal cancer: up to one-fourth of patients have CLM at diagnosis and one-fourth will develop it during follow-up [1, 2]. Liver resection (LR) in combination with chemotherapy is their standard treatment, but 60–70% of patients will have recurrence [3,4,5,6]. The management of the recurrent disease is complex and specific guidelines are lacking. Repeat hepatectomy is beneficial but burdened by operative risks due to adhesions, altered liver anatomy, and reduced liver remnant [7, 8]. Tumor biology should drive the choice of the most appropriate treatment. Coherently, when recurrence occurs early after LR, the standard is chemotherapy followed by loco-regional treatment only if the disease does not progress at restaging [7, 9].
Thermal ablation of CLM has gained consensus, thanks to its appealing minimal invasiveness, negligible morbidity, low impact on chemotherapy schedule, high repeatability, and good effectiveness [10,11,12,13]. Radiofrequency and microwave ablations (RFA and MWA) became the standard for unresectable patients or patients unfit for surgery [11, 13, 14] and now are considered as a treatment option for selected patients with small resectable CLM or recurrent CLM when complex repeat LR would be needed [3, 15,16,17,18,19,20,21]. Two randomized trials are even testing ablation as an alternative to surgery in resectable patients [22, 23].
In 2003, Livraghi et al. advanced the proposal of a “test-of-time” approach in synchronous CLM: they scheduled upfront ablation of metastases to elucidate tumor biology and to select good candidates for surgery [24]. The present analysis explored the adoption of a “test-of-time” approach for the early recurrence of CLM after a first LR. Upfront ablation without associated chemotherapy could have several benefits: (1) to obtain an immediate and effective treatment of recurrence with minimal risks; (2) to avoid the early activation of a new chemotherapy line; (3) to assess tumor biology in a longer time adapting further treatment strategy accordingly.
Methods
All consecutive patients that underwent LR for CLM between 2004 and 2017 at the authors’ institution were retrospectively reviewed. Among patients with recurrence, those having the following characteristics were selected for the analysis: early recurrence after LR (≤ 8 months according to the Imai et al. definition [25]); single liver-only recurrence; disease amenable to both resection and ablation (< 30 mm, distant from major vessels and bile duct); adoption of a “test-of-time” approach, i.e. RFA or MWA of recurrence without peri-procedural chemotherapy. Exclusion criteria were: treatment of early recurrence combining chemotherapy with RFA/MWA; last pre-ablation imaging performed > 1 month before the procedure; and follow-up duration after RFA or MWA < 12 months. Data were retrospectively collected from a prospectively maintained database.
The “test-of-time” approach was evaluated in terms of post-ablation short-term outcome, i.e. mortality, morbidity and completeness of ablation, and long-term outcome, i.e. recurrence rate, both local and non-local, and survival. Further, we analyzed the “test-of-time” approach in comparison with the standard approach (chemotherapy followed by loco-regional treatment) in terms of: (1) modification of treatment strategy; (2) effectiveness, i.e. no need for further treatments; (3) salvageability, i.e. chance of repeat treatment in case of local recurrence; (4) chemotherapy saving, i.e. avoidance or postponement of chemotherapy.
Whenever imaging modalities before and after RFA or MWA were available, we used Ablation-fit™ software (R.A.W. Srl, Milano, Italy) to retrospectively evaluate the adequacy of the ablated area. Ablation-fit™ is a software that automatically segments liver and intrahepatic blood vessels and semi-automatically targets lesions in pre-interventional CT scans and necroses in post-interventional ones. The segmented pre- and post-interventional CT scans were automatically co-registered using a non-rigid registration tool. The software verified in a 3D model whether the ablation zone included entirely or partially the tumor and a pre-defined safety margin (10-mm thick). Further, it calculated the percentages of volume of both target tumor and safety margin that were not included in the ablation area [26].
The Institutional Review Board of our hospital approved this retrospective study and the requirement of informed consent was waived.
Patients’ management
Management of patients with CLM in the authors’ institution has been previously detailed [6, 27,28,29]. All patients with a diagnosis of recurrent disease were discussed at a hepato-biliary multidisciplinary team meeting attended by surgical oncologists, medical oncologists, radiation oncologists, hepatologists, and interventional radiologists. Since 2004 thermal ablation was considered as an alternative to resection in patients with recurrence size up to 20 mm. In selected patients undergone multiple chemotherapy lines, having an easy-to-ablate recurrence, and, conversely, needing eventually complex resection, the ablation limit was extended to 30 mm. A “test-of-time” approach was considered only for patients with solitary early recurrence. In presence of two or more recurrent metastases, we preferred to schedule a new chemotherapy line followed by a loco-regional treatment in case of disease response. All patients scheduled for a “test-of-time” approach had restaging before ablation with thoracoabdominal computed tomography (CT), hepatic magnetic resonance imaging (MRI), positron emission tomography-CT, and carcinoembryonic antigen (CEA) value. All patients undergoing ablation have the last imaging modality performed no longer than 30 days before treatment.
Before 2016, patients were treated by RFA. Later on, patients underwent RFA or MWA, at the discretion of the interventional radiologist, being MWA preferred in CLM > 20 mm. All procedures were performed under CT or ultrasound guidance using a percutaneous approach. For MWA (AMICA®, HS Hospital Service, Aprilia, Italy), one antenna is placed directly into the tumor and an electromagnetic microwave is emitted. Each generator is capable of producing different powers, for example 45–100 W at a frequency of 915 or 2450 MHz, depending on the device type. For RFA (Boston Scientific®, Natick, MA, USA), we used an impedance-guided ablation system consisting of a retractable curved electrode and an isolated 14-gauge outer needle that houses 10 solid retractable curved electrodes that when deployed assume the configuration of an umbrella. The generator connected to the needle is switched on and the energy is administered until a rapid rise in impedance occurs. The ablation algorithm is based on tissue impedance, rather than tissue temperature. All procedures were performed by expert interventional radiologists (DP, VP, LS). All patients underwent CT the day after ablation to check the primary efficacy rate of ablation and to exclude any post-procedure complication. Post-ablation follow-up included abdominal CT 1 month after the procedure, and then ultrasound, CT, or MRI every 3 months. In case of further recurrence, the multidisciplinary board renegotiated the management of every patient according to the disease status.
Definitions and statistical analyses
Minor hepatectomies were classified according to CLISCO classification [30, 31]. Major hepatectomy was defined as the resection of ≥ 3 contiguous liver segments [32]. Post-procedural complications were classified according to Clavien-Dindo classification [33]. Any recurrence after ablation was classified as follows: local, hepatic non-local, or extra-hepatic. Standard terminology of image-guided tumor ablation was used [34].
Summary statistics were constructed with the use of frequencies and proportions for categorical data, and means and ranges for continuous variables. The Kaplan–Meier method was used to estimate survival probabilities. Overall survival (OS) was calculated from the date of ablation to the date of death or last follow-up. Recurrence-free survival (RFS) was calculated from the date of ablation to the date of further recurrence or last follow-up. Follow-up data were updated until December 2019. The minimum follow-up was 12 months and no patient was lost to follow-up. Stata 15 software was used for all the analyses.
Results
During the study period (2004–2017), 579 patients underwent LR for CLM. Overall, 415 (72%) patients had a recurrence, including 210 (36%) with liver-only recurrence. Twenty-seven patients with early (≤ 8 months) solitary liver-only recurrence amenable to both resection and ablation were considered for a “test-of-time” approach. One patient received ablation in combination with chemotherapy (systemic therapy administered by the oncologists of another hospital) and was excluded. Finally, 26 patients undergoing a “test-of-time” approach were analyzed.
Table 1 summarizes patients’ characteristics. Sixteen (62%) patients were male; in the whole series mean age was 61 years (46–78). At first diagnosis, three-fourth of patients had CLM synchronous with the primary tumor. Nineteen (73%) patients had chemotherapy before LR, 18 with a partial response and one with stable disease. At LR, the mean number of CLM was 7 (1–28), and the mean diameter of the largest nodule was 30 mm (7–80). All patients but one had ultrasound-guided parenchyma-sparing minor hepatectomy, including nine (35%) that underwent complex limited resections. The remaining patient underwent a two-stage hepatectomy. After LR, the overall morbidity rate was 19%; no severe complication occurred.
Recurrence data
The mean time interval between LR and recurrence was 4 months (1–8). Recurrence was a single hepatic nodule in all patients with a mean size of 17 mm (8–26). Six patients had recurrence size larger than 20 mm. All 26 patients underwent a single-session thermal ablation, 18 (69%) with RFA and eight (31%) with MWA. None had associated chemotherapy. No post-procedure complication was registered. CT scan performed the day after the procedure demonstrated a primary efficacy rate of ablation of 100% in all patients.
Long-term outcome
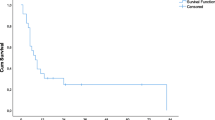
After a mean follow-up of 34 months, 1- and 3-year OS rates after ablation were 87.3 and 68.9%, respectively (Fig. 1). Overall, 21 out of 26 (81%) patients had recurrence after a mean interval of 5 months (1–16), leading to RFS rates at 1 and 3 years after ablation of 25.0 and 15.0%, respectively (Fig. 1).

Survival after ablation of recurrent liver disease: overall survival (blue curve); disease-free survival (green curve). OS overall survival, DFS disease-free survival, mo months (color figure online)
Results of the “test-of-time” approach can be summarized by four groups of patients (Fig. 2). First group: five patients (19%) did not develop any recurrence after ablation. All of them are alive and disease-free after a mean follow-up of 46 months (12–111). Second group: five patients (19%) had isolated local tumor recurrence at the ablation site (four after RFA and one after MWA; one out of six patients with recurrence size > 20 mm). All of them had repeat treatment, four LR and one repeat ablation. None had periprocedural chemotherapy. Of those, three (two LR and one repeat ablation) are alive and disease-free (mean follow-up 27 months), while two had non-local recurrence 18 and 24 months after repeat treatment, respectively. Third group: 13 (50%) patients had non-local recurrence early after the ablation (≤ 8 months). Recurrence was hepatic-only in six patients and hepatic + extrahepatic in seven. All patients had chemotherapy and four had repeat LR later on. Fourth group: three (12%) patients had non-local recurrence late after the ablation (> 8 months). Recurrence was hepatic in one patient and hepatic + extrahepatic in two. All had upfront chemotherapy; one had repeat LR and is alive and disease-free 12 months after ablation.

Outcomes of patients undergoing “test-of-time” approach with percutaneous ablation
The mutational status of CLM was not associated with outcome (Supplementary Table 1): early non-local recurrence risk was similar in RAS/BRAF mutated and wild-type patients (5/9, 56%, and 4/7, 57%, respectively). Of note, the patient with BRAF mutation had late non-local recurrence 16 months after ablation.
Impact of “test-of-time” approach
Overall, only four (15%) patients had LR of the initial recurrence site (patients with local-only recurrence), while six (23%) had effective ablation (repeat ablation in one) and did not develop further recurrences. The remaining 16 (62%) patients had recurrence in additional sites, early after ablation in most cases (n = 13).
Considering the salvageability of our approach, all five patients with local-only recurrence underwent repeat treatment without further local recurrence.
Chemotherapy was avoided in eight patients who did not have recurrence, either after ablation (n = 5) or after repeat treatment of local-only recurrence (n = 3). Further, chemotherapy was postponed in five patients with late recurrence, either after ablation (n = 3) or after repeat treatment of local-only recurrence (n = 2). Overall, chemotherapy was avoided or postponed in 13 (50%) patients (mean chemotherapy-free interval after ablation 33.5 months; mean chemotherapy-free interval in the whole population 18.1 months).
Evaluation of the ablation area by Ablation-fit™ software
Overall, in 11 patients pre- and post-ablation CT scans were evaluated with the Ablation-fit™ software. The co-registration of the two imaging modalities was successful in all patients. The tumor area was entirely included in the ablation zone in all patients. On the opposite, the ablation of the pre-defined peritumoral 10-mm safety margin was complete only in 3/11 patients (Fig. 3a). None of them had local tumor recurrence. In the remaining eight patients, residual unablated margin volume was documented, ranging from 17.1 to 65.5% of the complete volume, specifically below 25.4% in four patients and above 25.4% in the remaining four. In the first group no local tumor recurrence subsequently developed (Fig. 3b), while in the last four patients local tumor recurrences occurred, all located in the area where minimal or completely absent ablative margin had been documented by Ablation-fit™ software (Fig. 4).

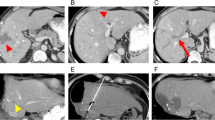
Perfectly co-registered (see the red line surrounding the liver) pre- and post-ablation CT scans of two patients. a Patient with metastasis at segment 3 (orange line) undergone MWA with a large volume of ablation zone (blue line). The 1-cm thick ablative margin (green line) is entirely included in the volume of the ablation zone. No local recurrence occurred in the follow-up. b Patient with metastasis at segment 7 (orange line) undergone RFA. The volume of the ablation zone (blue line) surrounds completely the metastasis and most of the 1-cm thick ablative margin (green line). Only a minor portion (18.4%) of the ablative margin, posteriorly located (colored in yellow) is not included in the volume of the ablation zone. No local recurrence occurred in the follow-up (color figure online)

Two patients with single metastases (orange lines) undergone RFA, respectively, located at segments 2 a and 5 c. In both cases, the volume of the ablation zone (blue line) entirely includes the metastases, but in a the ablative margin (green line) is absent along the lateral profile of the tumor (42.5% of the pre-defined margin) (area colored in yellow). The local recurrence b subsequently occurred exactly along the lateral margin of the metastasis. In the second patient c the ablative margin is widely (65.5%) untreated (yellow area). The location of the subsequent local recurrence corresponded with that of the original metastasis d (color figure online)
Discussion
In 2015, an international panel of experts recommended ablation in patients with limited liver disease that are technically unresectable or excluded from surgery because of comorbidities [11]. To date, thermal ablation is considered a suitable option in selected patients with resectable small nodules [3, 13, 19,20,21]. In comparison with open LR, RFA has fewer complications, shorter hospital stay, and high repeatability [12, 20, 35, 36]. Head-to-head comparisons between ablation and surgery are ongoing and will probably further expand the role of RFA and MWA in CLM treatment [22, 23]. In the setting of recurrent CLM, ablation has a wide application yet [15,16,17,18]. Even if repeat hepatectomy is the standard [7, 9], it is associated with some higher risks than the first LR because of adhesions, altered liver anatomy, and limited hepatic functional reserve [8, 37]. On the opposite, ablation maintains its benefits in terms of minimally-invasiveness, low morbidity, and adequate local disease control [15,16,17,18]. In the present series, no complications occurred after ablation, and all patients were discharged the day after the procedure.
When treating CLM, the assessment of tumor biology is crucial to define the most appropriate treatment strategy. In this sense, ablation could give a major contribution. In 2003, Livraghi et al. proposed to adopt RFA as a “test-of-time” approach for synchronous resectable CLM [24]. They performed upfront ablation of liver nodules to elucidate tumor biology and to select good candidates for surgery. LR was avoided in two-third of patients either because of a persistent complete response of CLM to ablation or because of the early appearance of additional unresectable CLM. We decided to apply the “test-of-time” approach to patients with early small solitary CLM recurrence. Their present standard treatment is the activation of a new chemotherapy line scheduling a repeat loco-regional therapy (ablation or LR) 2–3 months later in case of disease response or stabilization [3, 6, 7, 9]. This policy has some major limitations. It requires a new chemotherapy line that could be unnecessary if the recurrent nodule is just a residual disease and that could be saved for further progression. Short chemotherapy before loco-regional treatment (2–3 months) does not guarantee an adequate assessment of tumor biology, while a long one (6 months) may lead to tumor disappearance and chemotoxicity. We tried to overcome those limitations by scheduling upfront ablation without any associated chemotherapy: CLM is effectively treated with a minimally-invasive approach, while tumor biology is better analyzed in a longer time span. Our hypotheses were confirmed by the present results. First, ten patients (40%) showed favorable tumor biology and did not require chemotherapy. In detail, five patients did not have a further recurrence after ablation. Five additional patients had isolated local recurrence and all received a salvage treatment (one repeat ablation and four repeat LR) with excellent results and, again, without periprocedural chemotherapy. Second, three patients (10%) developed late non-local recurrence (> 8 months after ablation), benefitting from a postponement of chemotherapy. Finally, as expected, a high proportion of patients (50%) had an early non-local recurrence that required a prompt reactivation of chemotherapy and was associated with very poor outcome. Overall, only four patients had surgery for the initial disease (local-only recurrence), six had percutaneous effective treatment (repeated in one), and 13 avoided or postponed chemotherapy.
Thermal ablation is associated with two main concerns: the local disease control and the chance of repeat treatment when local recurrence occurs. The local failure rate of RFA is still higher than surgery, ranging from 10 to 20% [38]. Risk increases together with tumor size and proximity to intrahepatic vessels [39,40,41,42]. Insisted ablation once recurrence occurs should be cautiously evaluated because it could lead to complex salvage surgery in case of further local failure [43, 44]. Based on that background, since 2004 we considered amenable for ablation patients carrier of CLM single, distant from major intrahepatic vessels, and ≤ 20 mm in diameter. This peculiar limited size was borrowed from the experience with the HCC both with ablation [45], in absence of similar evidence for CLM. The extension up to 30 mm was reserved in selected patients undergoing multiple chemotherapy lines, having an easy-to-ablate recurrence, and, conversely, needing eventually complex resections. Despite this strict selection and the fact that every patient had a primary efficacy rate of ablation of 100% verified at CT the day after the procedure, we observed local recurrence in 20% of treated cases. That further sustains the need for caution in addressing this approach extensively. However, just one of the five cases with recurrence had a diameter above 20 mm. Ablation margins are crucial to obtain a high efficacy rate, even if their immediate check is not yet standard in practice [42, 46]. Further, some studies reported the need for larger margins in KRAS-mutated patients [47,48,49]. Possibly, as herein experienced, software enabling the real-time assessment of completeness of ablation including both tumor and peritumoral tissues could further improve the local effectiveness of interstitial treatments [26, 46]. It remains anyhow largely satisfactory the discussed policy which has been further implemented by preferring a prompt rescue surgical control in case of local relapse instead of insisted ablation. Indeed, four out of five patients with local-only recurrence received effective salvage surgery.
The present study is clinically relevant because it proposes a standardized approach to patients with early recurrence, for whom guidelines do not provide any recommendation. Some limitations could be argued. It is a retrospective analysis enroling a limited number of patients, but we adopted strict and homogeneous inclusion criteria. A large cohort of patients from a referral center was needed to collect present data. A prospective intention-to-treat analysis would give more conclusive data, but all patients undergoing a first LR for CLM at the authors’ institution were considered and all the enroled patients had an expert multidisciplinary team evaluation both at first diagnosis and at recurrence. We scheduled a “test-of-time” approach only for patients with solitary early recurrence. The possibility to extend the proposed approach to patients with two or three small lesions could be explored. Some gene mutations, such as RAS and BRAF mutations, have been associated with the tumor biology and outcome of thermal ablation [47,48,49]. The present series did not confirm such association, but few patients with genetic mutations were analyzed.
Conclusion
A “test-of-time” approach is recommended for all patients with solitary liver-only early recurrence of CLM. Upfront thermal ablation without chemotherapy allowed to adapt treatment strategy to tumor biology. It minimized the invasiveness of the initial treatment with good effectiveness and high salvageability in case of local failure, avoided worthless surgery, and saved chemotherapy for further disease progression.
References
Stangl R, Altendorf-Hofmann A, Charnley RM, Scheele J (1994) Factors influencing the natural history of colorectal liver metastases. Lancet (London, England) 343(8910):1405–1410
Manfredi S, Lepage C, Hatem C, Coatmeur O, Faivre J, Bouvier AM (2006) Epidemiology and management of liver metastases from colorectal cancer. Ann Surg 244(2):254–259
Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, Aguilar EA, Bardelli A, Benson A, Bodoky G, Ciardiello F, D’Hoore A, Diaz-Rubio E, Douillard JY, Ducreux M, Falcone A, Grothey A, Gruenberger T, Haustermans K, Heinemann V, Arnold D et al (2016) ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol 27(8):1386–1422. https://doi.org/10.1093/annonc/mdw235
Creasy JM, Sadot E, Koerkamp BG, Chou JF, Gonen M, Kemeny NE, Balachandran VP, Kingham TP, DeMatteo RP, Allen PJ, Blumgart LH, Jarnagin WR, D’Angelica MI (2018) Actual 10-year survival after hepatic resection of colorectal liver metastases: what factors preclude cure? Surgery 163(6):1238–1244. https://doi.org/10.1016/j.surg.2018.01.004
Viganò L, Ferrero A, Tesoriere RL, Capussotti L (2008) Liver surgery for colorectal metastases: results after 10 years of follow-up. Long-term survivors, late recurrences, and prognostic role of morbidity. Ann Surg Oncol 15(9):2458–2464. https://doi.org/10.1245/s10434-008-9935-9
Viganò L, Pedicini V, Comito T, Carnaghi C, Costa G, Poretti D, Franzese C, Personeni N, Del Fabbro D, Rimassa L, Scorsetti M, Santoro A, Solbiati L, Torzilli G (2018) Aggressive and multidisciplinary local approach to iterative recurrences of colorectal liver metastases. World J Surg 42(8):2651–2659
Wicherts DA, de Haas RJ, Salloum C, Andreani P, Pascal G, Sotirov D, Adam R, Castaing D, Azoulay D (2013) Repeat hepatectomy for recurrent colorectal metastases. Br J Surg 100(6):808–818
Fukami Y, Kaneoka Y, Maeda A, Takayama Y, Onoe S (2017) Postoperative complications following aggressive repeat hepatectomy for colorectal liver metastasis have adverse oncological outcomes. Surg Today 47(1):99–107
Viganò L, Capussotti L, Lapointe R, Barroso E, Hubert C, Giuliante F, Ijzermans JN, Mirza DF, Elias D, Adam R (2014) Early recurrence after liver resection for colorectal metastases: risk factors, prognosis, and treatment. A LiverMetSurvey-based study of 6025 patients. Ann Surg Oncol 21(4):1276–1286
Pathak S, Jones R, Tang JM, Parmar C, Fenwick S, Malik H, Poston G (2011) Ablative therapies for colorectal liver metastases: a systematic review. Colorectal Dis 13(9):e252–e265
Gillams A, Goldberg N, Ahmed M, Bale R, Breen D, Callstrom M, Chen MH, Choi BI, de Baere T, Dupuy D, Gangi A, Gervais D, Helmberger T, Jung EM, Lee F, Lencioni R, Liang P, Livraghi T, Lu D, Meloni F, Solbiati L (2015) Thermal ablation of colorectal liver metastases: a position paper by an international panel of ablation experts, the interventional oncology Sans Frontières meeting 2013. Eur Radiol 25(12):3438–3454
van Amerongen MJ, Jenniskens S, van den Boezem PB, Fütterer JJ, de Wilt J (2017) Radiofrequency ablation compared to surgical resection for curative treatment of patients with colorectal liver metastases—a meta-analysis. HPB (Oxford) 19(9):749–756
Solbiati L, Ahmed M, Cova L, Ierace T, Brioschi M, Goldberg SN (2012) Small liver colorectal metastases treated with percutaneous radiofrequency ablation: local response rate and long-term survival with up to 10-year follow-up. Radiology 265(3):958–968
Van Tilborg AA, Meijerink MR, Sietses C, Van Waesberghe JH, Mackintosh MO, Meijer S, Van Kuijk C, Van Den Tol P (2011) Long-term results of radiofrequency ablation for unresectable colorectal liver metastases: a potentially curative intervention. Br J Radiol 84(1002):556–565
Elias D, De Baere T, Smayra T, Ouellet JF, Roche A, Lasser P (2002) Percutaneous radiofrequency thermoablation as an alternative to surgery for treatment of liver tumour recurrence after hepatectomy. Br J Surg 89(6):752–756
Sofocleous CT, Petre EN, Gonen M, Brown KT, Solomon SB, Covey AM, Alago W, Brody LA, Thornton RH, D’Angelica M, Fong Y, Kemeny NE (2011) CT-guided radiofrequency ablation as a salvage treatment of colorectal cancer hepatic metastases developing after hepatectomy. J Vasc Interv Radiol 22(6):755–761
Dupré A, Jones RP, Diaz-Nieto R, Fenwick SW, Poston GJ, Malik HZ (2017) Curative-intent treatment of recurrent colorectal liver metastases: a comparison between ablation and resection. Eur J Surg Oncol 43(10):1901–1907
Valls C, Ramos E, Leiva D, Ruiz S, Martinez L, Rafecas A (2015) Safety and efficacy of ultrasound-guided radiofrequency ablation of recurrent colorectal cancer liver metastases after hepatectomy. Scand J Surg 104(3):169–175
Benson AB, Venook AP, Al-Hawary MM, Cederquist L, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Engstrom PF, Garrido-Laguna I, Grem JL, Grothey A, Hochster HS, Hoffe S, Hunt S, Kamel A, Kirilcuk N, Krishnamurthi S, Messersmith WA, Freedman-Cass DA et al (2018) NCCN guidelines insights: colon cancer, version 2.2018. J Natl Compr Canc Netw 16(4):359–369
Otto G, Düber C, Hoppe-Lotichius M, König J, Heise M, Pitton MB (2010) Radiofrequency ablation as first-line treatment in patients with early colorectal liver metastases amenable to surgery. Ann Surg 251(5):796–803
Meijerink MR, Puijk RS, van Tilborg A, Henningsen KH, Fernandez LG, Neyt M, Heymans J, Frankema JS, de Jong KP, Richel DJ, Prevoo W, Vlayen J (2018) Radiofrequency and microwave ablation compared to systemic chemotherapy and to partial hepatectomy in the treatment of colorectal liver metastases: a systematic review and meta-analysis. Cardiovasc Intervent Radiol 41(8):1189–1204
Gurusamy K, Corrigan N, Croft J, Twiddy M, Morris S, Woodward N, Bandula S, Hochhauser D, Napp V, Pullan A, Jakowiw N, Prasad R, Damink SO, van Laarhoven C, de Wilt J, Brown J, Davidson BR (2018) Liver resection surgery versus thermal ablation for colorectal LiVer MetAstases (LAVA): study protocol for a randomised controlled trial. Trials 19(1):105
Puijk RS, Ruarus AH, Vroomen L, van Tilborg A, Scheffer HJ, Nielsen K, de Jong MC, de Vries J, Zonderhuis BM, Eker HH, Kazemier G, Verheul H, van der Meijs BB, van Dam L, Sorgedrager N, Coupé V, van den Tol P, Meijerink MR, COLLISION Trial Group (2018) Colorectal liver metastases: surgery versus thermal ablation (COLLISION)—a phase III single-blind prospective randomized controlled trial. BMC Cancer 18(1):821
Livraghi T, Solbiati L, Meloni F, Ierace T, Goldberg SN, Gazelle GS (2003) Percutaneous radiofrequency ablation of liver metastases in potential candidates for resection: the “test-of-time approach.” Cancer 97(12):3027–3035
Imai K, Allard MA, Benitez CC, Vibert E, Cunha AS, Cherqui D, Castaing D, Bismuth H, Baba H, Adam R (2016) Early recurrence after hepatectomy for colorectal liver metastases: what optimal definition and what predictive factors? Oncologist 21(7):887–894
Solbiati M, Muglia R, Goldberg SN, Ierace T, Rotilio A, Passera KM, Marre I, Solbiati L (2019) A novel software platform for volumetric assessment of ablation completeness. Int J Hyperthermia 36(1):337–343
Torzilli G, Viganò L, Gatti A, Costa G, Cimino M, Procopio F, Donadon M, Del Fabbro D (2017) Twelve-year experience of “radical but conservative” liver surgery for colorectal metastases: impact on surgical practice and oncologic efficacy. HPB (Oxford) 19(9):775–784
Viganò L, Costa G, Cimino MM, Procopio F, Donadon M, Del Fabbro D, Belghiti J, Kokudo N, Makuuchi M, Vauthey JN, Torzilli G (2018) R1 resection for colorectal liver metastases: a survey questioning surgeons about its incidence, clinical impact, and management. J Gastrointest Surg 22(10):1752–1763
Vigano L, Darwish SS, Rimassa L, Cimino M, Carnaghi C, Donadon M, Procopio F, Personeni N, Del Fabbro D, Santoro A, Torzilli G (2018) Progression of colorectal liver metastases from the end of chemotherapy to resection: a new contraindication to surgery? Ann Surg Oncol 25(6):1676–1685
Viganò L, Torzilli G, Troisi R, Aldrighetti L, Ferrero A, Majno P, Toso C, Figueras J, Cherqui D, Adam R, Kokudo N, Hasegawa K, Guglielmi A, Krawczyk M, Giuliante F, Hilal MA, Costa-Maia J, Pinna AD, Cescon M, De Santibanes E, CLISCO Group et al (2019) Minor hepatectomies: focusing a blurred picture: analysis of the outcome of 4471 open resections in patients without cirrhosis. Ann Surg 270(5):842–851
Viganò L, Torzilli G, Aldrighetti L, Ferrero A, Troisi R, Figueras J, Cherqui D, Adam R, Kokudo N, Hasegawa K, Guglielmi A, Majno P, Toso C, Krawczyk M, Abu Hilal M, Pinna AD, Cescon M, Giuliante F, De Santibanes E, Costa-Maia J, CLISCO Group et al (2020) Stratification of major hepatectomies according to their outcome: analysis of 2212 consecutive open resections in patients without cirrhosis. Ann Surg 272(5):827–833
Pang YY (2002) The Brisbane 2000 terminology of liver anatomy and resections. HPB 2000; 2:333-39. HPB (Oxford) 4(2):99–100
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Ahmed M, Solbiati L, Brace CL, Breen DJ, Callstrom MR, Charboneau JW, Chen MH, Choi BI, de Baère T, Dodd GD 3rd, Dupuy DE, Gervais DA, Gianfelice D, Gillams AR, Lee FT Jr, Leen E, Lencioni R, Littrup PJ, Livraghi T, Lu DS, Standard of Practice Committee of the Cardiovascular and Interventional Radiological Society of Europe et al (2014) Image-guided tumor ablation: standardization of terminology and reporting criteria—a 10-year update. Radiology 273(1):241–260
Takahashi H, Berber E (2020) Role of thermal ablation in the management of colorectal liver metastasis. Hepatobiliary Surg Nutr 9(1):49–58
Mulier S, Ruers T, Jamart J, Michel L, Marchal G, Ni Y (2008) Radiofrequency ablation versus resection for resectable colorectal liver metastases: time for a randomized trial? An update. Dig Surg 25(6):445–460
Dupré A, Lefranc A, Buc E, Delpero JR, Quenet F, Passot G, Evrard S, Rivoire M (2013) Use of bioresorbable membranes to reduce abdominal and perihepatic adhesions in 2-stage hepatectomy of liver metastases from colorectal cancer: results of a prospective, randomized controlled phase II trial. Ann Surg 258(1):30–36
Kron P, Linecker M, Jones RP, Toogood GJ, Clavien PA, Lodge J (2019) Ablation or resection for colorectal liver metastases? A systematic review of the literature. Front Oncol 9:1052
van Duijnhoven FH, Jansen MC, Junggeburt JM, van Hillegersberg R, Rijken AM, van Coevorden F, van der Sijp JR, van Gulik TM, Slooter GD, Klaase JM, Putter H, Tollenaar RA (2006) Factors influencing the local failure rate of radiofrequency ablation of colorectal liver metastases. Ann Surg Oncol 13(5):651–658
Huo YR, Eslick GD (2015) Microwave ablation compared to radiofrequency ablation for hepatic lesions: a meta-analysis. J Vasc Interv Radiol 26(8):1139-1146.e2
Di Martino M, Rompianesi G, Mora-Guzmán I, Martín-Pérez E, Montalti R, Troisi RI (2020) Systematic review and meta-analysis of local ablative therapies for resectable colorectal liver metastases. Eur J Surg Oncol 46(5):772–781
Shady W, Petre EN, Do KG, Gonen M, Yarmohammadi H, Brown KT, Kemeny NE, D’Angelica M, Kingham PT, Solomon SB, Sofocleous CT (2018) Percutaneous microwave versus radiofrequency ablation of colorectal liver metastases: ablation with clear margins (A0) provides the best local tumor control. J Vasc Interv Radiol 29(2):268-275.e1
Torzilli G, Del Fabbro D, Palmisano A, Marconi M, Makuuchi M, Montorsi M (2007) Salvage hepatic resection after incomplete interstitial therapy for primary and secondary liver tumours. Br J Surg 94(2):208–213
Brouquet A, Vauthey JN, Badgwell BD, Loyer EM, Kaur H, Curley SA, Abdalla EK (2011) Hepatectomy for recurrent colorectal liver metastases after radiofrequency ablation. Br J Surg 98(7):1003–1009
Livraghi T, Meloni F, Di Stasi M, Rolle E, Solbiati L, Tinelli C, Rossi S (2008) Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice? Hepatology (Baltimore, MD) 47(1):82–89
Kaye EA, Cornelis FH, Petre EN, Tyagi N, Shady W, Shi W, Zhang Z, Solomon SB, Sofocleous CT, Durack JC (2019) Volumetric 3D assessment of ablation zones after thermal ablation of colorectal liver metastases to improve prediction of local tumor progression. Eur Radiol 29(5):2698–2705
Shady W, Petre EN, Vakiani E, Ziv E, Gonen M, Brown KT, Kemeny NE, Solomon SB, Solit DB, Sofocleous CT (2017) Kras mutation is a marker of worse oncologic outcomes after percutaneous radiofrequency ablation of colorectal liver metastases. Oncotarget 8(39):66117–66127
Calandri M, Yamashita S, Gazzera C, Fonio P, Veltri A, Bustreo S, Sheth RA, Yevich SM, Vauthey JN, Odisio BC (2018) Ablation of colorectal liver metastasis: interaction of ablation margins and RAS mutation profiling on local tumour progression-free survival. Eur Radiol 28(7):2727–2734
Odisio BC, Yamashita S, Huang SY, Harmoush S, Kopetz SE, Ahrar K, Chun YS, Conrad C, Aloia TA, Gupta S, Hicks ME, Vauthey JN (2017) Local tumour progression after percutaneous ablation of colorectal liver metastases according to RAS mutation status. Br J Surg 104(6):760–768
Acknowledgements
The authors thank Marco Solbiati (RAW-Endosight, Milan, Italy) for his contribution in imaging analysis with the Ablation-fitTM software.
Funding
The authors have no funding sources to declare.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Research involving human participants and/or animals
The present study complies with the guidelines for human studies. The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Informed consent
The Institutional Review Board of our hospital approved this retrospective study and the requirement of informed consent was waived.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Vigano, L., Galvanin, J., Poretti, D. et al. Percutaneous ablation of post-surgical solitary early recurrence of colorectal liver metastases is an effective “test-of-time” approach. Updates Surg 73, 1349–1358 (2021). https://doi.org/10.1007/s13304-021-01047-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-021-01047-x