
Abstract
Prostate cancer (PCa) is the second most common cancer among the male population. Conventional therapies target androgen signalling, which drives tumour growth; however, they provide limited survival benefits for patients. It is essential, therefore, to develop a more specific biomarker than the current gold standard, PSA testing. The Wnt signalling pathway induces expression of target genes through cell surface receptors. A non-canonical member of this family, Wnt-11, is evolutionarily highly conserved and is normally expressed by various cells in the developing embryo, as well as in the heart, liver and skeletal muscle of adult humans. We comprehensively review several cell signalling pathways to explain how they interact with Wnt-11, demonstrating its use as a potential biomarker for PCa. Several studies have shown that the expression of Wnt-11 is associated with gastric, renal and colorectal adenocarcinomas and PCa. Moreover, Wnt-11 affects extracellular matrix composition and cytoskeletal rearrangement, and it is required for proliferation and/or survival during cell differentiation. It was found that PCa cell lines express high levels of Wnt-11, which allows differentiation of the epithelial prostate tumour cells to neuron-like (NE) cells. The NE cells produce additional factors that can cause regression after treatment. Accumulating evidence shows that Wnt-11 could be a potential biomarker in diagnosing PCa. Many studies have shown both non-canonical and canonical Wnts interact with several signalling cascades such as PKC, JNK, NF-κB, Rho, PKA and PI3K. In particular, evidence demonstrates Wnt-11 is involved in the progression of PCa, thus it could have the potential to become both a specific disease marker and an important therapeutic target.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer (PCa) remains a major health risk for men, especially over the age of 65, with the annual death rate in the western world reaching more than 100,000 cases [1] . Issues surrounding detection, management and prevention of PCa have driven debate among scientists worldwide. The main objective for current PCa researchers is to define treatment options that are successful for both localised and metastatic disease.
Legalisation of the prostate specific antigen (PSA) test within the UK still remains in question. According to the U.S. Food and Drug Administration, 4.0 ng/ml is described as the upper limit of PSA for PCa [2]. An increased PSA level can be indicative of PCa but can also be linked to benign prostatic hyperplasia, urinary tract infections and prostatitis. This leads to the assumption that the PSA test is more sensitive than specific. On the other hand, the PSA test can neglect PCa diagnosis and cannot distinguish between aggressive and the non-aggressive form [3]. In a modified approach, the PSA test includes monitoring the PSA levels over a period of time. This is defined as PSA velocity, which is the change in PSA levels per year (ng/ml/year) [4]. This highlights the need for more reliable biomarkers to generate more efficient and effective methods to screen and monitor the progression of PCa. An example of a biomarker that has been well characterised in PCa is a chromosomal rearrangement, namely the TMPRSS2-ERG gene fusion [5]. The TMPRSS2 gene is an androgen responsive promoter, which, when fused with the transcriptional factor from the ETS family, can drive tumour progression under androgen influences. This gene fusion was present in 79 % of 29 PCa cases. However, whilst this biomarker has shown a statistically significant correlation with PCa, the time at which it presents itself is still unclear [3] .
This review will focus on the role of Wnt signalling in the onset of PCa, its progression and its malignancy, in the hope that Wnt could be a candidate as a biomarker in PCa diagnosis. In particular, the focus will be on Wnt-11 and the mechanism of its downstream signal transduction cascades and their interactions with one another, and whether the inhibition of certain pathways will decrease cellular proliferation, migration and invasion of cancerous cells.
Wnt proteins and their functions
The Wnt signalling pathway was first described during a study on colon cancer and also in embryonic developmental studies of Drosophilia [6]. Embryogenesis and adult homeostasis are just two of many functions of the Wnt proteins [7]. However, when aberrant Wnt signalling occurs, tumourgenesis can arise such as PCa. Two Wnt signalling pathways have been identified: canonical and non-canonical pathways. A hallmark of the canonical pathway is the activation and stabilisation of a signalling pool of β-catenin that acts as a transcriptional factor for many cancer genes in the nucleus by binding to a number of transcriptional factors (Fig. 1) but is also involved in cadherin-medicated cell adhesion [8]. The regulation of β-catenin gene expression is mediated by interaction with both T cell specific transcriptional factor and lymphoid enhancing binding factor-1 (TCF/LEF-1), both members of the transcriptional factor family. In the absence of Wnt signalling, a low level of β-catenin in the cell is maintained by ubiquitination and degradation by the destruction complex. The destruction complex is comprised of adenomatous polyposis coli (APC) protein, glycogen synthase kinase 3 β (GSK3β), casein kinase 1 α and the axin proteins [7]. However, when initiation of Wnt signalling occurs, Wnt interacts with the frizzled receptor, and phosphorylation of the low-density lipoprotein receptor related protein (LRP) occurs simultaneously, allowing interaction with the destruction complex. Thus, accumulation of β-catenin occurs [7]. The non-canonical pathway involves initiation of other signalling cascades such as the planar cell polarity pathway and activation of Ca2+ (Fig. 2) [9]. In some cases, non-canonical pathways can antagonise the canonical pathway. The non-canonical pathway is less defined than its canonical counterpart; however, it has been said that the frizzled receptor (Fz) can activate enzymatic cascades such as c-Jun N-terminal kinase (JNK), p38 and protein kinase C (PKC) [10]. The more clearly defined non-canonical signalling pathway is that for Wnt/planar cell polarity signalling. Wnt-11 interaction with the frizzled receptor can activate dishevelled (Dvl), which is a cytoplasmic scaffold protein in the plasma membrane. This causes downstream signalling to occur, which activates different features of cytoskeletal reorganisation in cell movement and polarity. For example Daam1 and RhoA are activated, which can lead to the activation of JNK [9].

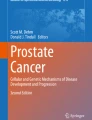
The Wnt canonical pathway. Wnt binding to the Fz receptor causing the dissociation of the destruction complex (axin, APC, Dsh, GSK3) causing an accumulation of β-catenin that is able to transport to the nucleus and transcribe for Wnt-associated genes. Image adapted from [52]

The non-canonical pathway can take two paths. a The planar cell polarity pathway causing actin cytoskeletal rearrangements. b The Wnt-Ca2+ pathway activating the calcium-sensitive protein PKC. Image adapted from [53]
Invasive behaviour of PCa cells is thought to be the cause of the Wnt/β-catenin signalling activation, which allows PCa cells to proliferate, differentiate and has an effect on the epithelial-mesenchymal transition. Usually, malignant PCa is androgen dependent and androgen ablation therapy can be successful until androgen independence occurs. The majority of androgen-independent tumours still express the androgen receptor and it is this abnormal androgen receptor signalling that allows tumour progression [11].
Wnt-11 and PCa
Wnt-11 is one of the 19 known Wnt proteins and belongs to the non-canonical signalling pathway. Previously, high Wnt-11 expression in androgen-independent PCa cells and in high-grade prostate tumours was identified [12] . Furthermore, inhibition of the androgen receptor and Wnt-11 signalling was found to be defective in the hormone independent PCa cell line PC-3. Numerous Wnt genes have been found to be expressed in both normal prostate and cancerous prostate cells indicating that these genes play a role in ‘house-keeping’ within the prostate [13]. However, it has been said that expression of Wnt-11 alone is not sufficient to progress PCa cells to androgen independence and therefore other aberrations accompanying Wnt-11 expression are needed for this phenomenon to occur. Numerous theories surround the fact that Wnt-11 expression is increased in androgen-depleted LNCaP cells. This could be owing to the possibility that Wnt-11 might take part in the termination of cell growth following androgen depletion resulting from a signal produced by Wnt-11 [13]. Another theory is that the increase in Wnt-11 expression in androgen depleted LNCaP cells is due to neuroendocrine differentiation (NED). Neuroendocrine cells constitute a population of cells found in the epithelial compartment of the prostate gland. They are able to secrete factors to stimulate the survival and metastatic potential of cancerous prostate cells, such as neurone specific enolase (NSE) [14, 15].
The function of Wnt-11 in the onset of NED has been shown to be restricted only to PCa cells [15] as the ectopic expression of Wnt-11 in the RWPE-1 cell line, which is non-tumorigenic, exhibits characteristics similar to prostate progenitor cells and did not induce any neuroendocrine differentiation. To summarise, Wnt-11 is involved in progression of PCa cells, migration into surrounding tissues and differentiation of these cells in neuroendocrine-like cells.
Wnt and protein kinase C (PKC) signalling pathways
The protein kinase C (PKC) family of isozymes plays a vital role in cellular functions by transducing signals resultant from the hydrolysis of phospholipids mediated through cell membrane receptors. Cell membranes provide the stage for PKC to carry out its function, allowing the phosphorylation of PKC and its activation by binding specific lipids. These are tightly controlled mechanisms that regulate the production of PKC signalling within the cell. Often, it is these mechanisms that are deregulated during the onset of cancer [16].
The interaction of PKC and Wnt has been well documented. When the Wnt ligand binds to the Fz receptor, there is a sudden increase in the concentration of intracellular signalling molecules such as inositol 1,4,5-triphosphate (IP3), 1,2 diacylglycerol (DAG), and Ca2+ [17]. Both IP3 and DAG result from the action of phospholipase C on the membrane bound phospholipid phosphatidyl inositol 4,5-bisphosphate. This in turn leads to the diffusion of IP3 through the cytosol towards the endoplasmic reticulum where calcium channels are found, causing a release of calcium ions. Both DAG and calcium ions activate two calcium sensitive proteins, PKC and calmodulin-dependent kinase II (CamKII), that then activate nuclear transcription factors such as NFAT, NF-κB and CREB that transcribe for downstream regulatory genes [17].
According to [18] PKCδ is essential for convergent extension through the function of dishevelled (Dvl) during the Wnt/JNK signalling pathway. Further, experiments have confirmed that over-expression of the Fz7 receptor in Xenopus embryos caused the activation of PKCδ by it moving to the plasma membrane. On the other hand, reduction in PKCδ stopped the activation of JNK downstream of the Wnt/JNK pathway.
PKC is one of the main components of the non-canonical pathway involved in Wnt/Ca2+ signalling and has been found to take part in promoting invasiveness and malignancy in human cancers [7]. Using small hairpin RNA to disorder individual PKC isozymes, both in vitro and in vivo experiments demonstrated that, depending on cell types and signalling pathways, PKC isozymes are either pro-apoptotic or anti-apoptotic. It is noted that tumour cells display an altered balance in PKC isozyme expression. For example PKCϵ has been seen to be elevated in high grade prostate tumours and is involved in the progression of the tumour and the transition from an androgen-dependent state to an androgen independent state in LNCaP cells [17]. Interestingly, activation of JNK downstream of TNFα was increased in PKCϵ depleted cells, whereas over-expression of PKCϵ decreased JNK activation, suggesting some interlinking of the two pathways. Therefore, pharmacological targeting of PKCϵ within prostate tumours, where PKCϵ is overexpressed, can be a potential treatment [ 18 ].
Although numerous findings have shown cross talk between PKC and Wnt, their molecular function in cancer progression still needs to be elucidated. Screening of PKC isoforms led to the identification of Xenopus PKCδ as a therapeutic target for the inhibition of cancer growth [18]. This introduces further complications as different isoforms of PKC can exert either overlapping or differing functions within the cell, causing issues in anti-cancer therapy. Therefore, it is of immense importance to address the different isoforms of PKC and their interactions with Wnt within mitogenesis, transformation and metastasis.
Wnt and c-Jun N-terminal kinases (JNKs)
c-jun N-terminal kinases (JNKs) are members of the mitogen-activated protein kinases (MAPKs) family. MAPKs can activate a variety of processes including cellular proliferation, tumourgenesis, differentiation and apoptosis [19]. JNK’s mode of action is to phosphorylate serine 63 and 73 at the N-terminal domain of c-jun. This in turn stimulates activator protein-1 (AP-1) that then carries out transcriptional activity (Fig. 3). c-jun is essential for the transition of the G1 phase to the remainder of the cell cycle [20]. It also carries out a protective role against UV-induced apoptosis. At present there are only three distinct spliced JNK genes, JNK1, JNK2 and JNK3 21. JNK3 is primarily expressed throughout the nervous system, as opposed to JNK1 and JNK2 that are ubiquitously expressed. JNKs become activated during cellular stress due to exposure to UV, hypoxia, osmotic pressure, and variation in cytokines and growth factors concentrations [20]. Moreover, JNKs are found to play a role in the inflammatory signalling network, therefore, not surprisingly, the hyper-activation of JNKs is associated with oncogenic transformation.

Activation of the MAPKs through UV or stress-related signals causing the transcription of JNK-related genes. Image adapted from [54]
Reports indicate that less than an hour of JNKs activation is linked to cell survival, whereas a more sustained activation of JNKs causes pro-apoptotic signalling. Moreover, JNK participates in mRNA stabilisation, cell migration, and integrity of the cell skeleton [20]. Members of the JNK family are robustly involved in the regulation of certain transcriptional factors such as ATF2, stat3, c-myc and members of the Bcl-2 family. There is gathering evidence to show that JNK is involved in carcinogenesis; also, blocking JNK signalling with small molecule, JNK inhibitors can be beneficial in the treatment of cancer. TGFβ-1 has been identified as a key activator of JNK1, which in turn phosphorylates p21, a cell cycle regulator, and up-regulates its stability through a SMAD independent mechanism [21].
In PCa, the administration of antisense oligonucleotide caused a defeat in PC3 PCa xenografts, highlighting that JNK is needed for PCa cell proliferation [22]. Moreover, the nuclear and total JNK expression is amplified in malignant human PCa as opposed to the normal epithelium. The current therapy for androgen-dependent PCa, androgen ablation, may provoke apoptosis through JNK signalling through the production of reactive oxidative species in PCa cells, highlighting JNK’s pro-apoptotic function. With regards to JNKs anti-apoptotic function, JNK can protect PCa cells from apoptosis. Moreover, there is evidence that JNK promotes PCa metastasis by controlling cell adhesion through increasing the expression of extracellular matrix degradation proteins such as matrix metalloproteinases 2 and 9 [23].
Wnt and NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) crosstalk
There is gathering evidence to suggest that NF-κB has a key function in tumour progression and chemotherapy resistance. Its function is to regulate numerous cytokines such as TNFα, IL-8 and IL-1, cell adhesion molecules such as VCAM, and cell cycle genes such as c-myc and p53 [24].
The association of Wnt with NF-κB has been shown in osteoclasts, where an accumulation of nuclear β-catenin regulates the DNA binding activity of NF-κB [25]. Moreover, according to [26], NF-κB is also a target of Wnt10B in U20S osteosarcoma cells. Interestingly, it has also been shown that NF-κB can regulate gene expression involved in cell motility and invasiveness, an example being MMP-9.
The activation of NF-κB can take two pathways: classical or alternative. The classical pathway is triggered by either viral or bacterial infections whereas the alternative is activated by the members of the tumour necrosis factor family, [27]. It has been reported that the isoform PKCϵ mediates the activation of NF-κB in PCa cell lines and there is an established correlation with the over-expression of PKCϵ and the constant activation of NF-κB within these PCa cells. A transgenic PCa mouse model of PKCϵ over-expression triggered pre-neoplastic lesions that exhibited noteworthy hyper-activation of NF-κB. With the use of interfering RNA (RNAi) targeting PKCϵ, the translocation of NF-κB to the nucleus was consequently depleted, impairing NF-κB transcription. Furthermore, PKCϵ aids the assembly of the tumour necrosis receptor -1 signalling complex, which in turn activates NF-κB. Studies carried out by [17] demonstrated a molecular link between NF-κB and PKCϵ which plays a pivotal role in PCa progression. On another note, the link between NF-κB expression and AP-1 in PCa cells may have something to do with the differences in sensitivity to TNF-induced apoptosis in PCa cell lines. To investigate, two cell lines were used: androgen-dependent LNCaP and androgen-independent DU145. Results indicated that Du145 cells always expressed the active form of NF-κB and AP-1 and thus were resistant to TNF-induced apoptosis. LNCaP cells were seen not to express NF-κB and therefore were susceptible to TNF-induced apoptosis, [17].
Wnt and protein kinase a (PKA)
Recent studies demonstrated that the progression from AR-dependent to the AR-independent form of prostate cancer is linked with increased NE expression [15]. NE cells are derived from non-NE PCa cells and secrete factors and peptides such as bombesin, vasoactive intestinal polypeptide, somatostatin, and neurotensin, which can stimulate AR independent growth and trigger invasion of PCa cells [14]. The cAMP (Cyclic adenosine monophosphate)-dependent protein kinase A (PKA) and its activator cyclic adenosine monophosphate (cAMP) are a classic example of a signal transduction pathway. The cAMP signalling pathway also interlinks with other intracellular signalling such as Ca2+ and Ras-mediated MAP kinase. During pathological conditions such as PCa, the composition of the PKA holoenzyme or its localisation within the cell may change, prompting abnormal effects. The inactive holoenzyme is composed of a regulatory subunit (R) dimer and two catalytic kinase subunits (C). The active site of the C subunit reversibly associates with the inhibitory domain of the R subunit. Cooperative binding of cAMP molecules to the four nucleotide binding sites on the R subunit dimer causes dissociation of the C subunits and, thus, activation of the enzyme [28]. In mammalian cells, full activation of PKA requires phosphorylation at Thr197 by phosphoinositide-dependent protein kinase 1 (PDK1). Two major isoforms of PKA have been identified (PKA-I and II), and it has been shown that they interact with identical C subunits but have different R subunits. Several studies have shown that changes in the PKA-I/PKA-II ratios play a role in important processes like cellular differentiation and cancer development [29]. PKA-I over-expression has been studied in various cancer cells including PCa [30]. Moreover, phase III randomised clinical trial studies examined PKA RIα, one of the four R subunit genes, as a biomarker to predict the outcome for men with locally advanced prostate cancer treated with either radiation therapy (RT) alone or in addition to short-term androgen deprivation therapy (STAD) [31]. As a result, PKA RIα over-expression was significantly related to poor patient outcome, and was observed in 80 of 456 eligible and analysable men (17.5 %). Another study of independent patients treated with RT and either STAD or long-term androgen deprivation therapy (LTAD) was performed [31]. Once again, high level of PKA RIα expression was found to be an independent predictor for both distant metastasis and biochemical failure. These studies confirmed that PKA can be a suitable marker for PCa and that there is a link between AR dependency and PKA signalling. Indeed, another study showed a novel mechanism for PKA and AR crosstalk and suggested that PKA activation can trigger AR-dependent transcription [32]. cAMP responsive element-binding protein (CREB) can cooperate with AR via CREB-binding protein (CBP) and p300. Several studies have demonstrated that increased levels of cAMP alone are sufficient to induce NE differentiation in both androgen-dependent and androgen-independent cells [33]. Moreover, the NE phenotype of PCa cells can be reversible depending on the tumour microenvironment [34]. We have previously shown that Wnt-11 is linked to NE differentiation of PCa and it is PKA dependent [15], and have also observed a link between high level of Wnt-11 expression and CREB activity by performing CREB luciferase assay (unpublished results). It has been found that the cAMP pathway is concurrent with Ras activation through a negative feedback loop involving phosphorylation of phosphodiesterases, which diminishes cAMP concentrations within cells [35]. Wnt/β-catenin signalling has also been identified in PKA-activated samples of kidney cells [36]. Taking these together, Wnt-11 plays a crucial role in NED of PCa by activating the cAMP/PKA pathway. Therefore, blocking both PKA and Wnt-11 can be a potential therapy for PCa.
Wnt and Rho family of GTPases
The family of Rho proteins regulate the transition between an active GTP bound and an inactive GDP bound conformations. Rho GTPase family members control cell adhesion and motility via actin cytoskeleton reorganisation and therefore influence a broad range of processes such as cell movement and cell polarity [37, 38]. Rho and Rac are the most studied members of this family with Rho regulating the assembly of actin and myosin filaments whilst Rac initiates actin polymerisation at the periphery of the cell [10]. Studies show that Rho GTPase expression levels are often significantly different in tumours and metastases and this correlates with a poor prognosis [39, 40]. RhoB is closely linked with both RhoA and C, and despite the high homology between their sequences, it has been demonstrated that RhoB regulates growth factor tyrosine kinase receptors’ cellular trafficking from endosomes to the cell membrane [41]. RhoB often acts as a tumour suppressor in cancer and regulates apoptosis [42]. Moreover, reduced expression of RhoB has been reported in several carcinomas including PCa [43]. Inhibition of RhoB expression resulted in a higher migration rate of PC cell line PC-3 and mouse macrophages [38, 44]. Another study demonstrated that RhoB is responsible for the maintenance of cell-cell junctions in epithelial PCa cell line DU145 in addition to controlling the N-cadherin levels of mesenchymal-like PC-3 cells [45]. Rho-GTPases are ideally positioned for non-canonical signalling such as the polarised reorganisation of the actin cytoskeleton leading to cell movement. One of the best models giving genetic evidence for Rho GTPase participation in non-canonical Wnt signalling is in the organisation of the Drosophila wing. In the wing, activation of the frizzled receptor results in localised Rho activation. In parallel to this, Rac activation by either frizzled or dishevelled causes JNK activation initiating gene expression [10].
Wnt and PI3K
The phosphoinositide 3-kinase (PI3K) pathway has a fundamental role in the initiation of numerous malignancies and their progression. The initial signalling is activated by either tyrosine kinase receptors’ or non-tyrosine kinase receptors’ interaction with a ligand, which then goes on to engage with PI3K. PI3K then proceeds to convert phosphatidylinositol (4,5)-bisphosphate, which is membrane bound, to phosphatidylinositol (3,5)-bisphosphate. This in turn activates and phosphorylates Akt and then the activated Akt translocates to the cytoplasm and nucleus, activating downstream targets [46]. Akt has a multi-functional purpose in promoting cell survival by regulating pathways that take part in the cell cycle, resistance to apoptosis and interaction with a host of proteins including GSK3 and mTOR. The latter is a serine threonine kinase that is involved in cellular proliferation and cell growth [47]. There are two known functional complexes of mTOR: mTOR1 and mTOR2. mTOR1 is rapamycin-sensitive whereas mTOR2 is not. PTEN (phosphatases and tensin homologue), a tumour suppressor gene, is an obligate negative regulator of the PI3K/AKT/mTOR signalling pathway and is a crucial therapeutic target for cancers where signalling cascades are out of control.
Deregulation of this pathway can arise through a series of events. These include loss of function of PTEN through mutation, gene deletion or epigenetic silencing or mutation of AKT/PKB [46]. It has been shown that PTEN null cells continuously express high level of AKT. PCa cell lines PC-3 and LNCaP have deletions and mutations of PTEN but they have high levels of phosphorylated AKT in both basal and activated forms [48]. AKT regulates cell growth and cell survival by inactivating its downstream factors such as GSK3. In 42 % of primary prostate tumours, mutation of the PI3K/AKT/mTOR signalling pathway, and its altered expression, has been reported [49]. Androgens have been reported to cause the accumulation of mammalian target for rapamycin complex 2 (mTORC2) complex components and stress activated protein kinase interacting protein-1 within the nucleus. This promotes the activation of AKT by TORC2 components. The loss of both AKT and PTEN is correlated with a poor clinical outcome for PCa patients, generating resistance to both chemotherapy and radiotherapy. Moreover, loss of PTEN is associated with raised AKT phosphorylation, and a higher Gleason grade. This can also promote castration-resistant growth and a shorter time for metastasis to occur. Furthermore, preclinical studies of the PI3K/AKT/mTOR pathway have highlighted its importance in maintaining the cancer stem cell population and promotion of the transition of PCa cells from the epithelium to the mesenchymal [49]. It was shown that blocking PI3K leads to inhibition of Wnt signalling via Wnt5a and Wnt3 in PCa [50]. One of the most important breakthroughs in PCa was the identification that ETS gene rearrangement has been reported in 50–70 % of PCa cases [50]. PTEN loss was associated with TMPRSS2-ERG activation as nearly 40 % of reported cases were linked [51]. PI3K pathway inhibitory complementary therapies are currently in use as ERG targeted therapies and this implies that PTEN loss and ETS gene rearrangements together may trigger downstream transcription targets to induce proliferation and cell survival. We believe Wnt-11 cross talks with PI3K to regulate those downstream targets as we found inhibition of PI3K and/or mTOR reduces Wnt11 dependent migration/invasion of PCa cell lines (unpublished results).
Conclusion
PCa is surrounded with dangers that implicate both patients and the healthcare system. Wnt-11 has been evidenced to play a role in the progression, differentiation and hormone independent characteristics associated with malignant PCa. The PI3K/AKT/mTOR pathway interacts with other signalling cascades such as androgen receptor signalling and RAS/RAF/MEK signalling. Human epidermal growth factor 2/3 kinases (HER2/3) inhibit androgen receptor signalling through the PI3K/AKT/mTOR pathway via a negative feedback system. Moreover, PTEN can enhance AR activity by supressing the transcription of c-jun and Egr1, which inhibits AR transcription [50]. These suggest that PCa cells can survive in androgen-deprived conditions due to PTEN loss or the activation of the PI3K/AKT/mTOR/Wnt pathways through targeted inhibition of the AR signalling. The rarity of possessing the aggressive form of PCa, and its inability to be successfully treated with androgen ablation, still remains a big problem. Therefore, the involvement of Wnt-11 and its interaction with various signalling pathways such as JNK, PKA and PI3K may propose innovative and novel research directions. This will open up new treatment options to improve prognosis and overall survival rate, especially for PCa.
References
Wilt TJ, Ahmed HU. Prostate cancer screening and the management of clinically localized disease. BMJ (Clinical research ed). 2013;346:f325.
Cary K, Cooperberg M. Biomarkers in prostate cancer surveillance and screening: past, present and future. Ther Adv Urol. 2013;5(6):318–29.
Makarov DV, Loeb S, Getzenberg RH, Partin AW. Biomarkers for prostate cancer. Annu Rev Med. 2009;60:139–51.
Bjurlin M, Loeb S. PSA velocity in risk stratification of prostate cancer. Rev Urol. 2013;15(4):204–6.
Hagglof C, Hammarsten P, Stromvall K, Egevad L, Josefsson A, Stattin P. TMPRSS2-ERG expression predicts prostate cancer survival and associated with stromal biomarkers. PLoS One. 2014;9(2):e86824.
Hausmann G, Banziger C, Basler K. Helping wingless take flight: how WNT proteins are secreted. Nat Rev Mol Cell Biol. 2007;8(4):331–6.
Komiya Y, Habas R. Wnt signal transduction pathways. Organogenesis. 2008;4(2):68–75.
Heuberger J, Birchmeier W. Interplay of cadherin-mediated cell adhesion and canonical Wnt signaling. Cold Spring Harb Perspect Biol. 2010;2(2):a002915.
Wang Y. Wnt/planar cell polarity signalling: a new paradigm for cance therapy. Mol Cancer Ther. 2009;8(8):2103–9.
Schlessinger K, Hall A, Tolwinski N. Wnt signalling pathways meet Rho GTPases. Genes Dev. 2009;23:265–77.
Kypta RM, Waxman J. Wnt/B-catenin signalling in prostate cancer. Nat Rev Urol. 2012;9:418–28.
Uysal-Onganer P, Kypta RM. Wnt11 in 2011—the regulation and function of a non-canonical Wnt. Acta Physiol. 2012;204(1):52–64.
Zhu H, Mazor M, Kawano Y. Analysis of Wnt gene expression in prostate cancer: mutual inhibition by WNT11 and the androgen receptor. Cancer Res. 2004;64(21):7918–26.
Sun Y, Niu J, Huang J. Neuroendocrine differentiation in prostate cancer. Am J Transl Res. 2009;1(2):148–62.
Uysal-Onganer P, Kawano Y, Caro M, Walker MM, Diez S, Darrington RS, et al. Wnt-11 promotes neuroendocrine-like differentiation, survival and migration of prostate cancer cells. Mol Cancer. 2010;9:55.
Newton A. Protein Kinase C: poised to signal. Am J Phsiol Endocrinol Metab. 2010;298(3).
Garg R, Blando J, Perez C, Wang H, Benavides F, Kazaniez M. Activation of nuclear factor kB (NF-kB) in prostate cancer is mediated by protein kinase C ε (PKCε). J Biol Chem. 2012;287(44):37570–82.
Luna-Ulloa L, Hernandez-Maqueda J, Castaneda-Patlan M, Robles-Flores M. Protein Kinase C in Wnt signalling: implications in cancer initiation and progression. IUBMB Life. 63(10):915–21.
Dhillon AS, Hagan S, Rath O, Kolch W. MAP kinase signalling pathways in cancer. Oncogene. 2007;26(22):3279–90.
Saadeddin A, Babaei-Jadidi R, Spencer-Dene B, Nateri A. The links between transcription, beta-catenin/JNK signalling, and carcinogenesis. Mol Cancer Res. 2009;7(8):1189–96.
Guo X, Wang XF. Signaling cross-talk between TGF-beta/BMP and other pathways. Cell Res. 2009;19(1):71–88.
Ma J, Zhang L, Han W, Shen T, Ma C, Liu Y, et al. Activation of JNK/c-Jun is required for the proliferation, survival, and angiogenesis induced by EET in pulmonary artery endothelial cells. J Lipid Res. 2012;53(6):1093–105.
Bode AM, Dong Z. The functional contrariety of JNK. Mol Carcinog. 2007;46(8):591–8.
Kunsch C, Rosen C. NF-kappa B subunit-specific regulation of the interleukin-8 promoter. Mol Cell Biol. 1993;13(10):6137–46.
Spencer G, Utting J, Etheridge S, Arnett T, Genever P. Wnt signalling in osteoblasts regulates expression of the receptor activator of NFKappaB ligand and inhibits osteoclastogenesis in vitro. J Cell Sci. 2006;119(9):1283–96.
Modder UI, Oursler MJ, Khosla S, Monroe DG. Wnt10b activates the Wnt, notch, and NFkappaB pathways in U2OS osteosarcoma cells. J Cell Biochem. 2011;112(5):1392–402.
Lawrence T. The nuclear factor NK-kB pathway in inflammation. Inflammation. 2009:1–10.
Taylor S, Beuchler J, Yonemoto W. cAMP-dependent protein kinase:framework for a diverse family of regulatory enzymes. Annu.Rev.Biochem. 1990;59:971–1005.
Pearce LR, Komander D, Alessi DR. The nuts and bolts of AGC protein kinases. Nat Rev Mol Cell Biol. 2010;11(1):9–22.
Sarwar M, Persson JL. The protein kinase A (PKA) intracellular pathway and androgen receptor: a novel mechanism underlying the castration-resistant and metastatic prostate cancer. J Cancer Sci & Ther. 2012;01(S5).
Khor L, Bae K, Paulus R. MDM2 and Ki-67 predict for distant metastasis and mortality in men treated with radiotherapy and androgen deprivation for prostate cancer. J Clin Oncol. 2009;27(19).
Kim C, Xuong N, Taylor S. Crystal structure of a complex. Sci Mag. 2005;307:690–6.
Sainz R, Mayo J, Tan D, Len J, Manchester L, Resiter R. Melatonin reduces prostate cancer cell growth leading to neuroendocrine differentiation via a receptor and PKA independent mechanism. Prostate. 2005;63(1):29–75.
Shen R, Dorai T, Olsson C, Buttyan R, Katz A, Szaboles M. Transdifferentiation of cultured human prostate cancer cells to a neuroendocrine cell phenotype in a hormone-depleted medium. Urol Oncol. 1997;3(2):67–75.
Caretta A, Caretta C. Protein kinase A in cancer. Cancer. 2011;3(1):913–26.
Gallegos TF, Kouznetsova V, Kudlicka K, Sweeney DE, Bush KT, Willert K, et al. A protein kinase A and Wnt-dependent network regulating an intermediate stage in epithelial tubulogenesis during kidney development. Dev Biol. 2012;364(1):11–21.
Ridley AJ. Rho GTPases and cell migration. J Cell Sci. 2001;114(15):2713–22.
Vega FM, Ridley AJ. Rho GTPases in cancer cell biology. FEBS Lett. 2008;582(14):2093–101.
Kusama T, Mukai M, Endo T, Ishikawa O, Tatsuta M, Nakamura H, et al. Inactivation of Rho GTPases by p190 RhoGAP reduces human pancreatic cancer cell invasion and metastasis. Cancer Sci. 2006;97(9):848–53.
Rathinam R, Berrier A, Alahari S. Role of Rho GTPases and their regulations in cancer progression. Front Biosci. 2011:2561–71.
Fernandez-Borja M, Janssen L, Verwoerd D, Horijk P, Neefjes J. RhoB regulates endosome transport by promoting actin assembly on endosomal membranes through Dia1. J Cell Sci. 2005;118(12):2661–70.
Huang M, Prendergast G. RhoB in cancer suppression. Histol Histopathol. 2006;21(1):213–8.
Lui M, Tang Q, Qui M, Lang N, Li M, Zheng Y, et al. miR-21 targets the tumor suppressor RhoB and regulates proliferation, invasion and apoptosis in colorectal cancer cells. FEBS Lett. 2011;585(19):2998–3005.
Wheeler AP, Ridley AJ. RhoB affects macrophage adhesion, integrin expression and migration. Exp Cell Res. 2007;313(16):3505–16.
Vega FM, Thomas M, Reymond N, Ridley AJ. The Rho GTPase RhoB regulates cadherin expression and epithelial cell-cell interaction. Cell Commun Signal. 2015;13:6.
Sarker D, Reid AH, Yap TA, de Bono JS. Targeting the PI3K/AKT pathway for the treatment of prostate cancer. Clin Cancer Res. 2009;5(15):4799–805.
Roccaro AM, Sacco A, Husu EN, Pitsillides C, Vesole S, Azab AK, et al. Dual targeting of the PI3K/Akt/mTOR pathway as an antitumor strategy in Waldenstrom macroglobulinemia. Blood. 2010;115(3):559–69.
Majumder P, Sllers W. AKt-regulated pathways in prostate cancer. Oncogene. 2005;24(50):7465–74.
Bitting RL, Armstrong AJ. Targeting the PI3K/Akt/mTOR pathway in castration-resistant prostate cancer. Endocr-Relat Cancer. 2013;20(3):R83–99.
Tomlins S, Rhodes D, Perner S, Dhanasekaran S, Mehra R, Sun X, et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science. 2005;310(5748):644–8.
Carver B, Tran J, Gopalan A, Chen Z, Shaikh S, Carracedo A, et al. Aberrant ERG expression cooperates with loss of PTEN to promote cancer progression in the prostate. Nat Genet. 2009;41(5):619–24.
Baron R, Kneissel M. WNT signaling in bone homeostasis and disease: from human mutations to treatments. Nat Med. 2013;19(2):179–92.
Staal FJT, Sen JM. The canonical Wnt signaling pathway plays an important role in lymphopoiesis and hematopoiesis. Eur J Immunol. 2008;38(7):1788–94.
Czaja MJ. JNK regulation of hepatic manifestations of the metabolic syndrome. Trends Endocrinol Metab. 2010;21(12):707–13.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Rights and permissions
About this article

Cite this article
Koushyar, S., Grant, G.H. & Uysal-Onganer, P. The interaction of Wnt-11 and signalling cascades in prostate cancer. Tumor Biol. 37, 13049–13057 (2016). https://doi.org/10.1007/s13277-016-5263-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-016-5263-z