
Abstract
MicroRNA-96 (miR-96) is an oncomiR that facilitates the development of malignant tumors by promoting growth, proliferation, and survival of cancer cells. Previous studies using high-throughput techniques have shown that miR-96 is upregulated in colorectal cancer compared to adjacent normal colorectal tissue. The aim of this study was the investigation of the potential clinical value of miR-96 as a molecular prognostic biomarker in colorectal adenocarcinoma. For this purpose, total RNA was extracted from 108 primary colorectal adenocarcinoma samples and 54 paired non-cancerous colorectal tissue specimens. After polyadenylation and reverse transcription, miR-96 molecules were determined using an in-house developed real-time quantitative PCR based on SYBR Green chemistry. Calculations were carried out with the comparative CT method, using SNORD48 as endogenous reference gene. Finally, extensive biostatistical analysis was performed and showed that miR-96 is significantly upregulated in colorectal adenocarcinoma specimens compared to their non-cancerous counterparts (p < 0.001) as well as in tumors having invaded regional lymph nodes (p = 0.009) and those of advanced TNM stage (p = 0.008). miR-96 expression is an unfavorable prognostic marker in colorectal adenocarcinoma, predicting poor disease-free and overall survival (p = 0.041 and 0.028, respectively), independently of classical clinicopathological parameters. Most importantly, miR-96 expression stratifies patients without distant metastasis (M0) at the time of diagnosis into two groups with substantially different prognosis (p = 0.040). In conclusion, high tissue levels of miR-96 are associated with advanced stages of colorectal adenocarcinoma and predict an increased risk for disease recurrence and poor overall survival, especially in patients without distant metastasis at the time of diagnosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) has a yearly incidence of about 1.26 million patients all over the world, thus comprising around 9.4 % of all cancer cases, according to the WHO 2008 report [1]. CRC, the third most commonly diagnosed cancer in both men and women, is more frequent in the Western world. In Europe and the USA, CRC constitutes the second most frequent cancer-related cause of death. In 2008, 608 thousands of patients died of this malignancy [2]. More than 95 % of CRCs are carcinomas and about 95 % of these are adenocarcinomas [3]. Although heritability contributes to CRC risk, the vast majority of 75 % of CRC patients have sporadic disease [4]. A number of acquired molecular events are associated with the transition from normal colonic epithelium to adenoma and, finally, to adenocarcinoma [5].
CRC is highly curable as the pathological tissue can be surgically removed, provided that the disease is detected early enough. However, CRC is often diagnosed at an advanced stage, when the tumor burden has already spread, thus giving birth to distant metastasis. As a consequence, these patients have a rather poor prognosis. Moreover, currently available tumor markers are non-specific and have a low sensitivity for CRC detection [6]. Their role is limited, since they are used only for detection of relapse after surgery and monitoring patients’ response to treatment [7]. Hence, the discovery of novel, reliable biomarkers for the early diagnosis, accurate staging, and follow-up of CRC progression is an indispensable need.
MicroRNAs (miRNAs) were first discovered at Caenorhabditis elegans in 1993 [8]. They are endogenous, small (18–24 nucleotides), non-coding, single-stranded RNA molecules that function as post-translational regulators of gene expression by binding to partially complementary sequences which are usually located at the 3′-untranslated regions (3′-UTRs) of the targeted messenger RNAs (mRNAs). In most cases, the binding of miRNAs to mRNAs leads to downregulation of the targeted genes by translational repression and/or mRNA degradation [9]. A combination of bioinformatical analyses with functional studies uncovered the presence of more than 1000 miRNAs in the human genome. These essential regulators of gene expression control a wide gamut of cellular processes, such as cell proliferation, survival, apoptosis, differentiation, motility, invasiveness, epithelial-mesenchymal transition (EMT), and morphogenesis [10].
The expression of many miRNAs is deregulated in cancer. Alterations in miRNA expression can arise from deletions, duplications, point mutations, and changes at the methylation pattern of miRNA genes, which are often located in cancer-related genomic regions and/or fragile sites [10, 11]. Furthermore, changes in the transcription rate of miRNA genes and/or the two-step maturation of their primary transcripts account also for aberrant expression of these tiny regulators of gene expression [12, 13]. Apart from their tremendous biological significance, miRNAs may constitute very useful biomarkers in many diseases [14].
Extensive ongoing research tries to identify miRNAs with clinical relevance in CRC, particularly focusing on miRNAs as promising diagnostic and/or prognostic tumor biomarkers [15]. One such miRNAs is microRNA-96 (miR-96) [16], the expression of which is deregulated in several other human malignancies, such as prostate cancer [17], breast cancer [18], ovarian carcinoma [19], hepatocellular carcinoma [20], non-small-cell lung cancer [21], and pancreatic cancer [22]. The MIR96 gene is part of a miRNA gene cluster, miR-183-96-182, mapped at the 7q32.2 genomic regions, between the MET and BRAF oncogenes. miR-96 is considered to be an oncomiR regulating the expression of many cancer-related genes. Among them, the transcription factors FOXO1 and FOXO3A as well as the KRAS oncogene are perhaps the most important ones with regard to colorectal adenocarcinoma [18, 23]. Other validated targets of miR-96 include IRS1, HTR1B, ADCY6, MITF, AQP5, CELSR2, ODF2, MYRIP, and RYK, according to the miRecords database [24].
The aforementioned data prompted us to evaluate the prognostic potential of miR-96 expression and its putative clinical application in colorectal adenocarcinoma prognosis. For this purpose, we developed a highly sensitive real-time quantitative PCR (qPCR) methodology for the quantification of miR-96 levels in colorectal adenocarcinomas and in adjacent non-cancerous colorectal mucosae.
Materials and methods
Tissue samples
The tissue bank used in the current study included 108 colorectal adenocarcinomas and 54 paired non-cancerous colorectal tissue specimens from patients who underwent surgical treatment for primary colorectal adenocarcinoma at the University General Hospital “Attikon,” between 2000 and 2010. All specimens were histologically characterized by a pathologist and frozen in liquid nitrogen immediately after resection. The study was approved by the institutional Ethics Committee of the University General Hospital “Attikon” in accordance with the ethical standards of the Declaration of Helsinki and informed consent was obtained from the patients.
Clinicopathological variables taken into account in this study included the tumor size, histological grade, and disease stage as defined according to the TNM classification. The TNM staging system combines tumor invasion (T), regional lymph node status (N), and presence or absence of distant metastasis (M); it has been updated for the last time in May 2011 [25]. Clinical and biological characteristics of all patients are summarized in Table 1. Follow-up information included disease status (disease-free or recurrence) and survival status (alive or deceased), as well as the dates of the events and the cause of death. The median disease-free survival (DFS) was 26.0 months (range 3.0–120.0) and the median overall survival (OS) was 27.0 months (range 1.0–120.0). Patient age ranged from 37.0 to 93.0 years with a mean ± SE of 67.0 ± 1.1 (Table 2).
Human cancer cell line culture
The human prostate carcinoma DU 145 cell line, in which miR-96 is highly expressed, was chosen as calibrator for the normalization in real-time PCR, as described below. DU 145 cells were subcultured in Dulbecco’s modified Eagle’s medium (DMEM), adjusted to contain 10 % fetal bovine serum (FBS), 100 kU/L penicillin, 0.1 g/L streptomycin, and 2 mM l-glutamine. Cells were seeded at a concentration of 0.5 × 105 cells/mL and incubated for 48 h at 37 °C, in a humidified atmosphere containing 5 % CO2, before collecting them for further use.
Total RNA extraction, polyadenylation, and reverse transcription
Tissue specimens were homogenized and then dissolved in TRI Reagent® (Molecular Research Center, Inc. Cincinnati, OH). Following the manufacturer’s instructions, total RNA was extracted from pulverized tumors and trypsinized DU 145 cells, diluted in RNA Storage Solution (Life Technologies Ltd., Carlsbad, CA, USA), and stored at −80 oC until use. The concentration and purity of total RNA were assessed spectrophotometrically at 260 and 280 nm. Total RNA polyadenylation and reverse transcription into first-strand complementary DNA (cDNA) were then performed as described in Suppl. Materials and methods.
Real-time PCR
qPCR was carried out using the SYBR Green chemistry in a 7500 Fast Real Time PCR System (Applied Biosystems, Foster City, CA, USA). Taking into account the published sequences of mature miR-96 and SNORD48 (small nucleolar RNA, C/D box 48; also known as RNU48 or U48) with GenBank® accession numbers NR_029512.1 and NR_002745.1, respectively, two specific primers were designed and used along with a common reverse primer to generate two respective amplicons. Primer sequences, contents of the reaction mixture, cycling conditions, and melting curves are presented in Suppl. Materials and methods. Each real-time PCR reaction was performed in duplicate, so as to evaluate the reproducibility of data (Suppl. Fig. 1a, b).
Calculations and validation of the comparative CT (2−∆∆CT) method for miR-96 quantification
Calculations were made using the comparative CT (2−∆∆CT) method. SNOR48 was used as an endogenous control gene so as to normalize PCRs for the RNA amount added to the reverse transcription reactions, while the prostate adenocarcinoma cell line DU 145 was used as a calibrator in order to render PCRs from distinct runs comparable [26]. The prerequisites for the application of the comparative CT (2−∆∆CT) method [27] were checked in a validation experiment, in which CT values of miR-96 and SNORD48 were measured in a dilution series of DU 145 cDNA covering five orders of magnitude (1–10−4). The qPCR efficiency (E) for the amplification of each molecule (Suppl. Fig. 1c) was calculated using the following formula: E = −1 + 10(−1/α), where α is the slope of the respective amplification plot. The slopes of miR-96 and SNORD48 amplification plots are very similar (−3.488 and −3.422, respectively), which clearly indicates similar efficiencies for the corresponding amplicons (93.5 and 96.0 %, respectively).
The normalized miR-96 expression in each sample was calculated as the ratio of miR-96 copies to SNORD48 copies divided by the same ratio that had been previously calculated for the DU 145 cell line. The normalized (2−∆∆CT) miR-96 levels were then multiplied with the average ratio of miR-96 copies to SNORD48 copies of DU 145 cells (2−5.638), calculated based on the difference between the y-intercepts of the regression lines (Suppl. Fig. 1c), therefore resulting in comparable results which are independent of the miR-96 expression levels in DU 145 cells. Finally, normalized results were multiplied by 1000 and designated as relative quantification units (RQU), standing for miR-96 copies/1000 SNORD48 copies. Calculations are summarized in the following formula:
where “Sample_X” is a random tissue specimen, “CmiR-96” is the number of miR-96 copies, “C SNORD48 ” is the number of SNORD48 copies, and “Plate_i” is a random qPCR run.
Biostatistical analysis
As the distribution of the expression levels of miR-96 in our cohort of patients was not Gaussian, miR-96 levels between paired tissue specimens (colorectal adenocarcinomas vs. non-cancerous mucosae) were compared using the non-parametric Wilcoxon signed-rank test. Moreover, analysis of the differences among subgroups of patients—stratified according to each clinicopathological parameter—was performed with the Mann-Whitney U test or Kruskal-Wallis test, where appropriate. To examine the discriminatory value of miR-96 expression in colorectal adenocarcinoma, we constructed receiver operating characteristic (ROC) curves for miR-96 expression levels by plotting sensitivity versus (1-specificity); the areas under the ROC curves (AUC) were analyzed by Hanley and McNeil method. Moreover, we performed univariate logistic regression analysis, using miR-96 expression both as a continuous and as a dichotomous variable, after splitting the continuous variable at the optimal cutoff value, as explained below.
In order to determine the optimal cutoff point for categorization of patients into miR-96 positive and miR-96 negative as there are no established cutoff points, we used the X-tile software, an algorithm that facilitated the determination of an optimal cutoff point by correcting for the use of minimum p value statistics algorithm [28]. This cutoff point was 24.10 RQU, equal to the 64th percentile. According to this cutoff value, miR-96 expression in each specimen was categorized as negative or positive.
Relationships between miR-96 expression status and patients’ survival were assessed by Kaplan-Meier DFS and OS curves. The differences between the curves were evaluated by the log-rank (Mantel-Cox) test. We also developed Cox proportional hazard regression models to assess the association between the prognostic markers and the relative risks for relapse and death of patients. Multivariate Cox regression models were adjusted for the aforementioned established clinicopathological parameters. The level of statistical significance was defined at a probability value of less than 0.05 (p < 0.05).
Results
Overexpression of miR-96 in colorectal adenocarcinoma tissue specimens compared to paired non-cancerous colorectal mucosae
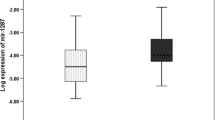
miR-96 expression was significantly higher in colorectal adenocarcinoma tissues than in non-cancerous mucosae, ranging from 0.50 to 99.74 RQU with a mean ± SE of 27.22 ± 2.55 in the former, while varying between 0.75 and 25.37 RQU with a mean ± SE of 5.85 ± 0.71 in the latter (Table 2 and Fig. 1a). Comparison of miR-96 levels among 54 pairs of colorectal tumors and their adjacent non-cancerous mucosae uncovered the profound overexpression of this molecule in the vast majority (83.3 %) of malignant colorectal tumors (p < 0.001; Fig. 1b).

Comparison of miR-96 levels between all colorectal adenocarcinoma samples and adjacent non-cancerous mucosae (a), as well as among pairs of colorectal adenocarcinoma tissues and their adjacent non-cancerous mucosae (b). miR-96 expression is significantly upregulated in colorectal adenocarcinoma specimens. Comparison of the distribution of miR-96 expression levels between colorectal adenocarcinoma specimens from node-negative (N0) and node-positive (N1 or N2) patients (c), as well as between early-stage (TNM stage I or II) and advanced-stage (TNM stage III or IV) colorectal tumors (d). High miR-96 expression was associated with positive regional lymph nodes and advanced TNM stages. The p value was calculated using the Mann-Whitney U test (a, c, and d) or the Wilcoxon signed-rank test (b). The line bars represent the median value (50th percentile) for each cohort, the bottom and top of each box indicate the 25th and 75th percentiles, respectively, the whiskers extend to 1.5 times the height of each box, and the circles outside boxes show outliers (a, c, and d)
Interestingly, miR-96 levels were elevated in colorectal adenocarcinomas of patients with positive regional lymph nodes, compared to tumors of those with negative nodal status (p = 0.009) (Fig. 1c). Moreover, colorectal adenocarcinomas classified at an advanced TNM stage showed stronger expression of miR-96 than early-stage tumors (p = 0.008) (Fig. 1d).
Discriminatory value of miR-96 expression in colorectal adenocarcinoma
So as to assess the ability of miR-96 expression to discriminate between colorectal adenocarcinoma and non-cancerous colorectal tissues, we performed ROC and logistic regression analyses. As illustrated by the ROC curve in Fig. 2, miR-96 expression was found to distinguish very efficiently colorectal adenocarcinoma from healthy colorectal mucosae (area under the curve (AUC) = 0.84, 95 % confidence interval (95 % CI) = 0.79–0.90, p < 0.001).

Receiver operating characteristic (ROC) curve for miR-96 expression. miR-96 expression was shown to efficiently distinguish colorectal adenocarcinoma from non-cancerous colorectal tissues
Univariate logistic regression analysis revealed that high miR-96 levels constitute a predictor of the presence of colorectal adenocarcinoma (crude odds ratio OR = 1.19, 95 % CI = 1.11–1.28, p < 0.001). Furthermore, analysis of miR-96 expression as a dichotomous variable showed that miR-96 positivity in colorectal mucosae predicts a 30-fold higher risk for adenocarcinoma (crude OR = 29.96, 95 % CI = 3.99–225.14, p < 0.001).
miR-96 expression predicts short-term relapse in colorectal adenocarcinoma patients, independently of other clinicopathological variables
miR-96 expression values were categorized into one of two groups (positive or negative), as described in the “Materials and methods” section; thus, 69 (63.9 %) cases were classified as miR-96 negative and 39 (36.1 %) as miR-96 positive. Furthermore, follow-up information was available for 106 patients; however, 13 patients were diagnosed with distant metastasis before or at the time of surgery and were excluded from DFS analysis. Out of the remaining 93 patients, 17 (18.3 %) relapsed during the respective follow-up periods.
In Cox univariate regression analysis (Table 3), a marginally significant 2.7-fold higher risk of recurrence was predicted for colorectal adenocarcinoma patients bearing tumors with positive miR-96 expression status (hazard ratio HR = 2.70, 95 % CI = 1.01–7.29, p = 0.049). We also performed Kaplan-Meier survival analysis to evaluate miR-96 expression in terms of predicting DFS. In agreement with the aforementioned results, Kaplan-Meier DFS curves illustrated that colorectal adenocarcinoma patients with miR-96-positive tumors had shorter DFS, compared to those who had a miR-96-negative colorectal adenocarcinoma (p = 0.041; Fig. 3a).

Kaplan-Meier survival curves for the disease-free survival (DFS) (a) and overall survival (OS) (b) of colorectal adenocarcinoma patients in total, as well as for the OS of metastasis-free patients (c). High miR-96 expression is an unfavorable prognostic biomarker in colorectal adenocarcinoma patients, particularly in those without distant metastasis (M0)
In the multivariate Cox regression analysis regarding DFS (Table 3), miR-96 expression predicted a significantly unfavorable prognostic outcome (HR = 3.10, 95 % CI = 1.06–9.02, p = 0.038), which was independent of tumor size, histological grade, tumor invasion, and regional lymph node status.
miR-96 expression is an independent prognosticator of poor OS in colorectal adenocarcinoma
Regarding OS, out of 106 colorectal adenocarcinoma patients for whom follow-up data were available, 24 patients (22.6 %) died during the accrual follow-up period. Cox univariate regression analysis (Table 3) demonstrated that patients with miR-96-positive colorectal adenocarcinoma were at higher risk of death (HR = 2.40, 95 % CI = 1.07–5.38, p = 0.033), compared to patients whose colorectal adenocarcinoma was miR-96 negative. Hence, enhanced miR-96 expression seems to constitute a strong unfavorable predictor of OS, as well. Histological grade of the tumor, tumor invasion, positive status of regional lymph nodes, and distant metastasis were also significant prognosticators of OS, as expected. In accordance with these results, Kaplan-Meier OS analysis revealed that patients with miR-96-positive colorectal adenocarcinoma were more likely to succumb to their disease earlier than patients with a miR-96-negative malignancy (p = 0.028; Fig. 3b).
In the multivariate Cox regression analysis (Table 3), miR-96 positivity remained a statistically significant indicator of poor OS in colorectal adenocarcinoma, independent of tumor size, histological grade, invasion, nodal status, and distant metastasis (HR = 2.48, 95 % CI = 1.04–5.96, p = 0.041). More importantly, Kaplan-Meier analysis in the subgroup of patients without distant metastasis (M0) demonstrated that positive miR-96 expression status predicts again a significantly unfavorable outcome (p = 0.040; Fig. 3c).
Discussion
Colorectal cancer is usually curable provided that it is detected early enough. The progression of the disease from normal mucosa to adenoma and, finally, to adenocarcinoma and metastasis to other tissues is a multistep process, involving mutations of tumor suppressors and oncogenes as well as altered expression of miRNAs and proteins, accompanied by impaired apoptosis. During the last decades, clinical researchers have focused their efforts on the discovery of novel molecular biomarkers that could be used in clinical practice for early diagnosis and/or reliable prognosis of CRC patients.
The emerging roles of miRNAs during carcinogenesis have been well highlighted in the recent past. miRNA functional studies in CRC have uncovered their implication in critical pathways involving EGFR [29], p53 [30], NFκB [31], Wnt, β-Catenin [32], and APC [33], as well as in the regulation of EMT [31] and cancer stem cell maintenance [31, 34]. Apparently, alterations of the expression pattern of specific miRNAs contribute significantly to colon carcinogenesis. Hence, their important functional roles in the initiation and progression of colorectal cancer as well as their stability and integrity even in formalin-fixed paraffin-embedded tissues render them potential first-class tumor biomarkers for this cancer type [35]. Their expression signatures are studied in tumor tissues [36], blood (plasma) [37, 38], and feces [39–41]. Thus, miRNA transcriptome constitutes a rich pool of novel, putative tumor biomarkers.
Focusing on miR-96, this one belongs to a miRNA family with high homogeneity and conservation among different species; all the members of this miRNA family have been shown to be deregulated in various human malignancies, including CRC, and are involved in critical cell processes, such as cellular differentiation, proliferation, apoptosis, and metabolism [18, 20, 23]. miR-96 expression is upregulated in a plethora of cancer types, including prostate, breast, bladder, lung, endometrial, and gastric cancer as well as hepatocellular and testis carcinoma [42, 43]. Our results regarding the remarkable upregulation of miR-96 expression in colorectal adenocarcinoma, compared to adjacent normal colorectal tissue, agree with those of previous studies [16, 43–45]. However, its potential diagnostic, prognostic, and/or predictive potential in colorectal adenocarcinoma have not been extensively studied, so far.
The role of deregulated miR-96 expression during colon carcinogenesis is critical, as this oncomiR facilitates the development of tumors by promoting growth, proliferation, and survival of cancer cells [46, 47]. According to our data, miR-96 levels are significantly higher in colorectal adenocarcinomas having invaded regional lymph nodes and in those of advanced TNM stage (III or IV). This finding along with the previously described association of miR-96 expression with liver metastasis [48] supports the notion that upregulation of miR-96 expression is related to the progression of colorectal adenocarcinoma. Similar conclusions have been drawn in non-small-cell lung cancer, as increased miR-96 expression in such malignant tumors of the lung was significantly associated with lymph node metastasis [49]. On the other hand, our results disagree with those of Ress et al. [46], who concluded that low miR-96 expression in primary colorectal tumors is associated with distant metastasis at the time of diagnosis. This could be attributed to the use of RNU6B (U6 snRNA) as a normalizer in that study, which constitutes a weakness due to the fact that RNU6B is an endogenous reference gene with the least stability in expression [50]. Another substantial difference between our study and the one of Ress et al. [46] is the cutoff value used for the dichotomization of miR-96 expression; in our study, we used an appropriate algorithm [28] to determine the optimal cutoff value for this purpose, whereas Ress et al. chose to split miR-96 expression at the median and hence create two cohorts of CRC patients [46].
In accordance with our aforementioned results, Cox univariate regression analysis showed that high miR-96 expression is a poor prognosticator in patients with colorectal adenocarcinoma, as it predicts an increased risk of relapse and/or death. Similarly, Kaplan-Meier survival analysis demonstrated significantly inferior DFS and OS rates for miR-96-positive patients. Again, our conclusions disagree with those drawn in the study of Ress et al. [46], according to which low miR-96 expression is likely to be associated with poor clinical outcome in CRC patients. The reasons for this apparent difference between the two studies are described in the previous paragraph. More interestingly, we hereby show that miR-96 positivity retained its unfavorable prognostic value in the subgroups of patients without distant metastasis at the time of diagnosis.
In summary, we examined the putative discriminatory and prognostic value of miR-96 expression in colorectal adenocarcinoma using a newly developed, in-house, low-cost, sensitive, and accurate SYBR Green-based qPCR technique for the quantification of the levels of this miRNA. The generation of an optimal cutoff and the subsequent dichotomization of miR-96 expression (positive vs. negative expression status) alleviates the need for utmost sensitivity that could be achieved by using a ready-to-use probe-based qPCR assay, rendering such assays much less cost-effective. Our study provides evidence that miR-96, an important oncomiR with anti-apoptotic behavior belonging to the miR-183-96-182 cluster, is able to distinguish colorectal adenocarcinoma tissues from non-malignant colorectal tissues. A novel finding of our study is that miR-96 expression is higher in primary colorectal adenocarcinoma of patients with metastasis in regional lymph nodes or advanced disease stage. In accordance with these results, strong miR-96 expression constitutes an unfavorable prognostic biomarker for this malignancy, predicting short DFS and OS time intervals. Most importantly, the prognostic value of miR-96 expression seems to be independent of classical clinicopathological parameters including tumor size, histological grade, tumor invasion, and regional lymph node status. In addition to these findings, we demonstrate that high miR-96 expression predicts poor OS even among patients with apparently similar OS probabilities, such as those without distant metastasis (M0), thus suggesting its putative future exploitation by multiparametric prognostic models comprising various molecular biomarkers with prognostic significance in colorectal adenocarcinoma.
In conclusion, the current study provides strong evidence that miR-96 expression constitutes a promising biomarker for colorectal adenocarcinoma. Under this perspective, trying to determine miR-96 levels in serum or plasma and to analyze its potential clinical value as a non-invasive molecular biomarker for colorectal adenocarcinoma would be particularly interesting. Our future efforts will focus on high-throughput small-RNA profiling in adenocarcinomas and adenomas as well as matched normal tissues of the colon and rectum by means of RNA-seq, in an attempt to identify miRNAs with high variations in their expression and study their combinatorial prognostic significance and ability to predict patient outcome.
References
Boyle P, Levin B. Colorectal cancer. In world cancer report. International Agency for Research on Cancer. 2008:374-8.
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: Globocan 2008. Int J Cancer. 2010;127:2893–917.
Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36:2251–70.
Schoen RE. Families at risk for colorectal cancer: risk assessment and genetic testing. J Clin Gastroenterol. 2000;31:114–20.
Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61:759–67.
Pokorny RM, Hunt L, Galandiuk S. What’s new with tumor markers for colorectal cancer? Dig Surg. 2000;17:209–15.
Duffy MJ, van Dalen A, Haglund C, et al. Clinical utility of biochemical markers in colorectal cancer: European group on tumour markers (egtm) guidelines. Eur J Cancer. 2003;39:718–27.
Lee RC, Feinbaum RL, Ambros V. The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell. 1993;75:843–54.
Ambros V, Lee RC, Lavanway A, Williams PT, Jewell D. Micrornas and other tiny endogenous rnas in C. elegans. Curr Biol. 2003;13:807–18.
Calin GA, Sevignani C, Dumitru CD, et al. Human microrna genes are frequently located at fragile sites and genomic regions involved in cancers. Proc Natl Acad Sci U S A. 2004;101:2999–3004.
Melo SA, Esteller M. Dysregulation of micrornas in cancer: playing with fire. FEBS Lett. 2011;585:2087–99.
Trabucchi M, Briata P, Filipowicz W, Rosenfeld MG, Ramos A, Gherzi R. How to control mirna maturation? RNA Biol. 2009;6:536–40.
Kontos CK, Scorilas A, Papavassiliou AG. The role of transcription factors in laboratory medicine. Clin Chem Labo Med : CCLM / FESCC. 2013;51:1563–71.
Lujambio A, Lowe SW. The microcosmos of cancer. Nature. 2012;482:347–55.
Schee K, Fodstad O, Flatmark K. MicroRNAs as biomarkers in colorectal cancer. Am J Pathol. 2010;177:1592–9.
Bandres E, Cubedo E, Agirre X, et al. Identification by real-time pcr of 13 mature micrornas differentially expressed in colorectal cancer and non-tumoral tissues. Mol Cancer. 2006;5:29.
Schaefer A, Jung M, Mollenkopf HJ, et al. Diagnostic and prognostic implications of microrna profiling in prostate carcinoma. Int J Cancer. 2010;126:1166–76.
Lin H, Dai T, Xiong H, et al. Unregulated mir-96 induces cell proliferation in human breast cancer by downregulating transcriptional factor foxo3a. PLoS One. 2010;5:e15797.
Wang L, Zhu MJ, Ren AM, et al. A ten-microRNA signature identified from a genome-wide microrna expression profiling in human epithelial ovarian cancer. PLoS One. 2014;9:e96472.
Leung WK, He M, Chan AW, Law PT, Wong N. Wnt/beta-catenin activates mir-183/96/182 expression in hepatocellular carcinoma that promotes cell invasion. Cancer Lett. 2015;362:97–105.
Ma L, Huang Y, Zhu W, et al. An integrated analysis of miRNA and mRNA expressions in non-small cell lung cancers. PLoS One. 2011;6:e26502.
Tanaka M, Suzuki HI, Shibahara J, et al. Evi1 oncogene promotes kras pathway through suppression of microRNA-96 in pancreatic carcinogenesis. Oncogene. 2014;33:2454–63.
Gao F, Wang W. MicroRNA-96 promotes the proliferation of colorectal cancer cells and targets tumor protein p53 inducible nuclear protein 1, forkhead box protein o1 (foxo1) and foxo3a. Mol Med Rep. 2015;11:1200–6.
Xiao F, Zuo Z, Cai G, Kang S, Gao X, Li T. Mirecords: an integrated resource for microRNA-target interactions. Nucleic Acids Res. 2009;37:D105–10.
Nagtegaal ID, Quirke P, Schmoll HJ. Has the new TNM classification for colorectal cancer improved care? Nat Rev Clin Oncol. 2012;9:119–23.
Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative pcr and the 2(-delta delta c(t)) method. Methods. 2001;25:402–8.
Schmittgen TD, Livak KJ. Analyzing real-time PCR data by the comparative c(t) method. Nat Protoc. 2008;3:1101–8.
Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10:7252–9.
Mlcochova J, Faltejskova P, Nemecek R, Svoboda M, Slaby O. MicroRNAs targeting EGFR signalling pathway in colorectal cancer. J Cancer Res Clin Oncol. 2013.
Ma Q, Wang X, Li Z, et al. MicroRNA-16 represses colorectal cancer cell growth in vitro by regulating the p53/survivin signaling pathway. Oncol Rep. 2013;29:1652–8.
Ma Y, Li W, Wang H. Roles of miRNA in the initiation and development of colorectal carcinoma. Curr Pharm Des. 2013;19:1253–61.
Yamada N, Noguchi S, Mori T, Naoe T, Maruo K, Akao Y. Tumor-suppressive microRNA-145 targets catenin delta-1 to regulate wnt/beta-catenin signaling in human colon cancer cells. Cancer Lett. 2013;335:332–42.
Nagel R, le Sage C, Diosdado B, et al. Regulation of the adenomatous polyposis coli gene by the mir-135 family in colorectal cancer. Cancer Res. 2008;68:5795–802.
Yu Y, Kanwar SS, Patel BB, et al. MicroRNA-21 induces stemness by downregulating transforming growth factor beta receptor 2 (TGFbetaR2) in colon cancer cells. Carcinogenesis. 2012;33:68–76.
Schetter AJ, Harris CC. Alterations of microRNAs contribute to colon carcinogenesis. Semin Oncol. 2011;38:734–42.
Menendez P, Villarejo P, Padilla D, Menendez JM, Rodriguez-Montes JA. Implications of the histological determination of microRNAs in the screening, diagnosis and prognosis of colorectal cancer. J Surg Oncol. 2013;108:70–3.
Madhavan D, Cuk K, Burwinkel B, Yang R. Cancer diagnosis and prognosis decoded by blood-based circulating microRNA signatures. Front Genet. 2013;4:116.
Bartley AN, Yao H, Barkoh BA, et al. Complex patterns of altered microrna expression during the adenoma-adenocarcinoma sequence for microsatellite-stable colorectal cancer. Clin Cancer Res. 2011;17:7283–93.
Wu CW, Ng SS, Dong YJ, et al. Detection of mir-92a and mir-21 in stool samples as potential screening biomarkers for colorectal cancer and polyps. Gut. 2012;61:739–45.
Xiao YF, Yong X, Fan YH, Lu MH, Yang SM, Hu CJ. MicroRNA detection in feces, sputum, pleural effusion and urine: novel tools for cancer screening (review). Oncol Rep. 2013;30:535–44.
Kalimutho M, Del Vecchio Blanco G, Di Cecilia S, et al. Differential expression of mir-144* as a novel fecal-based diagnostic marker for colorectal cancer. J Gastroenterol. 2011;46:1391–402.
Zhang QH, Sun HM, Zheng RZ, et al. Meta-analysis of microRNA-183 family expression in human cancer studies comparing cancer tissues with noncancerous tissues. Gene. 2013;527:26–32.
Navon R, Wang H, Steinfeld I, Tsalenko A, Ben-Dor A, Yakhini Z. Novel rank-based statistical methods reveal microRNAs with differential expression in multiple cancer types. PLoS One. 2009;4:e8003.
Kara M, Yumrutas O, Ozcan O, et al. Differential expressions of cancer-associated genes and their regulatory miRNAs in colorectal carcinoma. Gene. 2015;567:81–6.
Hamfjord J, Stangeland AM, Hughes T, et al. Differential expression of miRNAs in colorectal cancer: comparison of paired tumor tissue and adjacent normal mucosa using high-throughput sequencing. PLoS One. 2012;7:e34150.
Ress AL, Stiegelbauer V, Winter E. Mir-96-5p influences cellular growth and is associated with poor survival in colorectal cancer patients. Mol Carcinog. 2014.
Zhang Q, Ren W, Huang B, Yi L, Zhu H. MicroRNA-183/182/96 cooperatively regulates the proliferation of colon cancer cells. Mol Med Rep. 2015;12:668–74.
Xu XM, Qian JC, Deng ZL, et al. Expression of mir-21, mir-31, mir-96 and mir-135b is correlated with the clinical parameters of colorectal cancer. Oncol Lett. 2012;4:339–45.
Li J, Li P, Chen T, et al. Expression of microRNA-96 and its potential functions by targeting foxo3 in non-small cell lung cancer. Tumour Biol. 2015;36:685–92.
Peltier HJ, Latham GJ. Normalization of microRNA expression levels in quantitative RT-PCR assays: identification of suitable reference RNA targets in normal and cancerous human solid tissues. RNA. 2008;14:844–52.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the institutional Ethics Committee of the University General Hospital “Attikon” in accordance with the ethical standards of the Declaration of Helsinki and informed consent was obtained from the patients.
Conflicts of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Rapti, SM., Kontos, C.K., Papadopoulos, I.N. et al. High miR-96 levels in colorectal adenocarcinoma predict poor prognosis, particularly in patients without distant metastasis at the time of initial diagnosis. Tumor Biol. 37, 11815–11824 (2016). https://doi.org/10.1007/s13277-016-5023-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-016-5023-0