
Abstract
Apolipoprotein E (ApoE) is a factor involved in Alzheimer’s disease, which recently attracted great attention as an important protein related to tumorigenesis and metastasis. However, serum ApoE levels and its diagnosis and prognosis value in non-small cell lung cancer (NSCLC) patients are still unknown. In 196 NSCLC patients and 203 healthy controls, serum ApoE was measured by turbidimetric immunoassay. The associations of serum ApoE levels with the clinicopathological characteristics and clinical outcomes of NSCLC patients were analyzed. Serum ApoE levels were obviously elevated in NSCLC patients compared with healthy controls (41.6 ± 11.63 vs. 33.8 ± 6.24 mg/L) and were associated with TNM stage, lymph node metastasis status, and distant metastasis status (all P < 0.0001). For NSCLC diagnosis, the area under the receiver operating characteristic (ROC) curve was 0.71 at a specificity of 0.90 and sensitivity of 0.47. For lymph node metastasis predicting, the area under the ROC curve was 0.68 at a specificity of 0.56 and sensitivity of 0.73. From ROC/area under curve (AUC) analysis, we used 41.25 mg/L as the serum ApoE cut-off value, to divide NSCLC patients into two groups, the median survival was 11.0 weeks (95 % CI = 8.7 to 13.3) for patients in high serum ApoE group and 20.0 weeks (95 % CI = 15.0 to 25.0) in low serum ApoE group. Serum ApoE levels elevated in NSCLC patients, which also associated with TNM stages, lymph node metastasis, distant metastasis, and poor prognosis, suggest that serum ApoE may act as a useful clinical serological biomarkers for evaluating the progress of NSCLC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung cancer remains the leading cause of cancer death worldwide, attribute to the fact that approximately 70 % of lung cancer patients were diagnosed at advanced stage with the presence of metastatic tumors, which were no longer suitable for surgical resection, regardless of the advancements of diagnostic methods [1]. Lung cancer is classified into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC), and NSCLC accounts for 85 % of lung cancer cases [2]. According to histological and immunophenotypic characteristics, NSCLC is divided into adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. NSCLC presents is extremely resistance to anticancer therapy, and the 5-year overall survival rate is merely close to 15 % [3]. The emergency of early diagnosis is based on the fact that the 5-year survival rate for early stage NSCLC is above 50 %, compared with less than 5 % in patients with metastasis [4]. Therefore, the screening of the novel biomarkers and diagnostic tools to detect early stage NSCLC has been act as the vital task thread on the majority of physicians and scientists. Currently, screening method including chest X-rays, sputum exfoliative cytologic examination, or computed tomography scans has display an effect on survival, even computed tomography can detect lung cancers with submillimeter range [5], but the diseases screening approaches need further development.
Apolipoprotein E (ApoE) is a glycoprotein-rich arginine, which is mainly synthesized and secreted by liver and macrophages [6], consisting of 299 amino acid, with molecular weight of 34.5 kDa. ApoE is a component of lipoproteins, mainly involved in the regulation of lipid metabolism, neurobiology, and neurodegenerative diseases through receptor-mediated endocytosis pathways [7]. In addition, ApoE involved in the regulation of a series of biological process, including cell growth, differentiation, immune stresses, and macular degeneration [8]. Recent studies have suggested that ApoE can function as either cancer metastasis-suppressive factor or a biomarker for cancer metastasis [8–10]. Pencheva et al. identified the cancer-secreted ApoE involved in melanoma metastasis inhibition and anti-angiogenesis through targeting melanoma cell LRP1 and endothelial cell LRP8 receptors, respectively [9]. Su et al. reported that the ApoE overexpression promotes cancer cells proliferation and migration and contributes to cisplatin resistance and can serve as a poor prognostic biomarker for patients with lung adenocarcinoma and malignant pleural effusions [11]. Rice et al. showed that elevated serum ApoE level is associated with smoking, and ApoE can serve as a predictive biomarker for early lung cancer [10]. Liu et al. demonstrated by proteomic and immunological methods that elevated serum ApoE is associated with lymph node metastasis in lung adenocarcinoma patients [8]. These three studies suggested that serum ApoE could be a potential early diagnostic and poor prognostic biomarker in lung cancer. Wang et al. also reported that ApoE levels were significantly increased in the pleural effusion of NSCLC patients, and increased levels could be a potential marker for the diagnosis of malignant pleural effusions in NSCLC [12]. However, the prognostic significance of serum ApoE in patients with NSCLC is still unknown.
In this study, we aim to investigate the utility of serum ApoE as a biomarker for NSCLC prognosis.
Materials and methods
Patient population and specimens
The study group comprised of 196 patients diagnosed with different subtypes of NSCLC at the First Affiliated Hospital of Sun Yat-sen University, from January 2010 to December 2011. Patients who had hyperlipidemia, liver disease, previous malignancy, a second primary cancer, received hormone replacement therapy of any drug known to affect lipid metabolism, or received preoperative adjuvant therapy were excluded. For NSCLC, diagnoses were confirmed by pathological examination of tissue from biopsy or resected specimens. The tumor histopathological classification was defined according to the WHO criteria, and stage classification was employed according to the 7th edition of UICC TNM staging system [13, 14]. The control group consisted of 203 age-matched healthy subjects who performed a routine health check-up at the Physical Health Examination Centre of the First Affiliated Hospital of Sun Yat-sen University. This study was approved by the ethics committee of the First Affiliated Hospital of Sun Yat-sen University according to the guidelines of Helsinki conventions. All participants enrolled in this study were Chinese and gave written informed consent at the first visit. All participants with NSCLC were followed-up at intervals of 1–2 months until June 2015, and follow-up time ranged from 1 to 60 months.
Data collection and laboratory tests
The patients’ clinical data were recorded, including their age, sex, treatment, histopathological findings, TNM stages, and medication history. To avoid the effects of diet on testing ApoE levels, subjects were overnight fast of at least 8 h, and blood was collected in the morning between 7:00 a.m. and 10:00 a.m. for serum tests before treatment. Blood samples were allowed to clot, centrifuged, and tested immediately in the clinical laboratory of the First Affiliated Hospital of Sun Yat-sen University. Hemolysis sample was excluded from the study. ApoE was determined by turbidimetric immunoassay (Sekisui Medical Co. Ltd., Tokyo, Japan) using a Beckman Coulter AU5800 Platform automated analyzer. All tests were performed according to the manufacturer’s instructions.
Statistical analyses
All variables with normal distributions were displayed as the mean ± standard deviation. T test and one-way ANOVA are performed to compare means between two groups and within several groups, respectively. To determine differences in serum ApoE levels between groups, we used the Mann–Whitney U test and Kruskal–Wallis test. The statistical power was analyzed by using the Power and Precision software (version 4). Receiver operating characteristic (ROC) curves were plotted to evaluate the sensitivity and specificity of the serum ApoE to stratify patients at a high risk of malignancy-related death. The diagnostic value of serum ApoE level was evaluated by sensitivity, specificity, and area under ROC curve. The cut-off value was calculated according to the score closest to the value with both maximum sensitivity and specificity. The survival rates were determined by Kaplan–Meier method, and significant differences of survival were conducted by using the log-rank test. COX regression analysis model was performed for multivariate analysis of prognostic factors. In all cases, P < 0.05 was considered statistically significant, and all P values were calculated by two-sided significance tests. All data analyses were performed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
Clinical characteristics
In this study, we collected 196 patients diagnosed with NSCLC and 203 healthy controls. The baseline characteristics of the study subjects are described in Table 1. There is no statistically significantly difference between patients and healthy controls on the age and gender. The mean age of the patients and healthy controls was 61.6 and 60.7 years, respectively. The proportion of male gender for patients and healthy controls was 65.8 and 57.6 %, respectively. The proportion of smoking status was higher in patients than in healthy controls (71.9 vs. 57.1 %, respectively). Most of the patients were in stage III or IV (70.4 %), and 63.3 % of the patients were lymph node metastases positive.
Association between serum ApoE levels with clinicopathologic characteristics
We used the turbidimetric immunoassay to investigate the serum ApoE levels in patients with NSCLC and healthy controls. Comparison of serum ApoE levels between NSCLC patients and healthy controls demonstrated that ApoE was obviously higher in patients than in healthy controls (41.6 ± 11.63 vs. 33.8 ± 6.24 mg/L, Fig. 1a). The statistical power was analyzed by using the Power and Precision where power value was 1.0 (>0.8 was accounted significant). We further analyzed the clinicopathologic significance of the serum ApoE expression. The relationship between the serum ApoE levels and the clinicopathologic characteristics in NSCLC patients is summarized in Table 2. Serum ApoE was higher in advanced TNM stage NSCLC patients (stage III/IV) than early stage patients (stage I/II; Table 2, Fig. 1b). Serum ApoE levels were significantly higher in NSCLC patients with lymph node metastases positive than those lymph node metastases negative (Table 2, Fig. 1c). We also analyzed the association between serum ApoE levels and distant metastases in NSCLC patients, NSCLC patients with distant metastases showed higher serum ApoE levels (Table 2, Fig. 1d). For other clinicopathologic characteristics, the serum ApoE levels were not obviously different (Table 2). Taken together, these data demonstrated that serum ApoE was elevated in NSCLC patients and associated with the progression and metastasis of NSCLC, which could be a potential indicator for prognosis of NSCLC patients.

Comparison of serum ApoE levels a between normal controls and NSCLC patients; b in NSCLC patients at different TNM stage; c in NSCLC patients with and without lymph node metastasis; d in NSCLC patients with and without distant metastasis
ROC analysis of serum ApoE levels in NSCLC patients
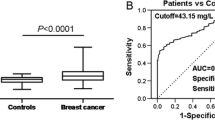
To further assess the indicating value of serum ApoE levels in NSCLC, we analyzed the receiver operating characteristic/area under curve (ROC/AUC) by plotting sensitivity against specificity. First, we evaluated the probability in discriminating NSCLC patients from healthy controls by serum ApoE levels, and ROC/AUC analysis showed an AUC 0.71 with a specificity of 0.90 at a sensitivity of 0.47 (the cut-off was 41.25 mg/L, Fig. 2a). Second, in distinguishing NSCLC patients without lymph node metastasis from healthy controls, the ROC/AUC analysis showed an AUC 0.58 with a specificity of 0.90 at a sensitivity of 0.32 (the cut-off was 41.25 mg/L, Fig. 2b). We continue to differentiate NSCLC patients with lymph node metastasis positive from healthy controls, the serum ApoE levels demonstrated an AUC 0.78 with a specificity of 0.90 at a sensitivity of 0.57 (the cut-off was 41.4 mg/L, Fig. 2c). Last, we compared the lymph node metastasis positive NSCLC patients with the lymph node negative patients, results showed an AUC 0.68 with a specificity of 0.56 at a sensitivity of 0.73, and the cut-off was 37.05 mg/L (Fig. 2d).

ROC analyses for serum ApoE to differentiate a NSCLC from healthy controls; b NSCLC patients with lymph node metastasis negative from healthy controls; c NSCLC patients with lymph node metastasis positive from healthy controls; d NSCLC patients with lymph node metastasis positive from lymph node metastasis negative. Nor normal controls, LYM-Neg lymph node metastasis, LYM-Pos lymph node metastasis positive
Serum ApoE levels are an independent prognostic indicator for overall survival of NSCLC patients
To explore the potential clinical meaning of the high serum ApoE levels in NSCLC, we assessed the prognostic power of serum ApoE levels on the overall survival in 196 NSCLC patients. We calculated the overall survival time from the sampling date to the date of death from cancer (cancer-specific survival). Deaths due to unknown cause, not cancer-related, and patients alive were censored. All patients received conventional adjuvant chemotherapy after surgery, follow-up time ranged from 1 to 60 months. Based on the cut-off value from ROC analysis, we used the serum ApoE level 41.25 mg/L as the threshold to partitioned the 196 NSCLC patients into two groups, high serum ApoE group (n = 93), and low serum ApoE group (n = 103). As determined by Kaplan–Meier method and log rank test, the high serum ApoE group was correlated with a shorter overall survival (P < 0.01, Fig. 3). The median survival was 11.0 weeks (95 % CI = 8.7 to 13.3) for patients in high serum ApoE group and 20.0 weeks (95 % CI = 15.0 to 25.0) in low serum ApoE group. Table 2 displayed multivariate Cox regression analyses of clinical that variables, and serum ApoE levels for their prognostic power on overall survival, TNM stage (HR = 3.37, 95 % CI = 1.82–8.47; Table 3), lymph node metastasis status (HR = 2.87, 95 % CI = 1.32–6.89; Table 3), distant metastasis status (HR = 4.52, 95 % CI = 1.97–7.85; Table 3), and serum ApoE levels (HR = 2.18, 95 % CI = 1.31–3.79; Table 3) were independent risk factors of prognosis of NSCLC patients.

Kaplan–Meier survival curves of NSCLC patients. Overall survival rate of NSCLC patients with high serum ApoE levels was obviously shorter than those with low ApoE levels
Discussion
In this study, we analyzed the serum ApoE levels in the NSCLC patients and revealed that serum ApoE levels significantly elevated in NSCLC patients compared to healthy controls. Serum ApoE levels were associated with TNM stages, lymph node metastasis status, and distant metastasis status of NSCLC patients. Elevated serum ApoE correlated with shorter survival period, which indicating serum ApoE to reflect poor prognosis in NSCLC patients, and Cox regression analysis revealed serum ApoE levels were an independent prognostic factor for NSCLC patients. ROC analysis showed that serum ApoE level had a good potential to distinguish lymph node metastasis NSCLC patients from lymph node metastasis negative patients with high sensitivity. Meanwhile, ApoE test can be easily performed by conventional clinical biochemistry lab with commercially available kit. Therefore, serum ApoE may serve as a general serum biomarker for the diagnosis of NSCLC.
The high mortality of lung cancer is mainly owing to lack of early diagnosis biomarker and the pale of clinical therapeutic methods. Because blood sample is easily accessible, and the test results are stable repeatable over time, serological biomarkers have shown to be beneficial in the diagnosis, treatment, and monitoring of lung cancer [15]. NSCLC as a common and poor prognostic lung cancer, whose diagnosis and treatment have troubled the scientists and physicians for decades. Early diagnosis and more comprehensive assessment of NSCLC by serological biomarkers are hence extremely necessary for the clinicians, which would assist the doctors to the delineation of tumor extent and surgical planning, and give efficient adjuvant therapy for NSCLC patients. By now, a series of biomarkers associated with diagnosis and prognosis of NSCLC have been discovered [2–4, 16–19]. In this study, we reported serum ApoE levels elevated in NSCLC patients compared with normal healthy controls, Moreover, serum ApoE levels also associated with TNM stages, lymph node metastasis, and distant metastasis status, which indicated serum ApoE might play a role in the tumorigenesis and progression of NSCLC.
ApoE is a class of apolipoprotein which is composed of chylomicrons and intermediate-density lipoprotein. Recently, ApoE has been proved to be related to tumorigenesis and cancer progression and makes it be concerned by the majority of scientists and clinicians. Accumulated evidence indicates that ApoE overexpressed in a series of human cancers, including bladder cancer [20], breast cancer [21], colorectal cancer [22], melanoma [9], ovarian cancer [23], gastric cancer [24], and lung cancer [8, 11]. ApoE is potentially important in regulating ovarian cancer cell proliferation and survival, knockdown ApoE expression led to cell cycle arrest and apoptosis in an ApoE-expressing cancer cell [25]. Studies on gastric cancer have demonstrated that an elevated level of ApoE is associated with advanced TNM stage and that ApoE lead to muscular invasion and is a biomarker of poor survival [24]. Su et al. reported ApoE overexpression in lung adenocarcinoma patients, and it could be concern with cancer cell proliferation, migration, and cisplatin in lung cancer cells [11]. All those studies imply that ApoE can make an important role in cancer progression and could be a predictive biomarker of poor prognosis.
More recently, ApoE has been identified as a factor related to metastasis and angiogenesis. As mention before, Pencheva et al. identified cancer-secreted ApoE involved in melanoma metastasis inhibition and anti-angiogenesis through targeting melanoma cell LRP1 and endothelial cell LRP8 receptors, and miR-1908, miR-199-5p, and miR-199a-3p convergent targeting of ApoE prompt melanoma metastasis and angiogenesis. Chen et al. reported that ApoE is highly expressed in pancreatic cancer, and the ApoE levels were associated with advanced stages and lymph node metastasis, reflecting ApoE concern with the development of pancreatic cancer, and could be as diagnostic biomarker of advanced pancreatic cancer [26]. However, ApoE in those two studies was based on the tumor tissue expression, detected by immunohistochemical (IHC) staining. ApoE levels were also reported highly elevated in NSCLC-associated malignant pleural effusion, which also has potential value in differentiating adenocarcinoma from other subtypes of NSCLC [12]. Very few studies concern the serum ApoE levels with metastasis. Liu et al. reported that combining proteomic and immunological analyses found serum ApoE as a potential biomarker for lung adenocarcinoma metastasis [8]. But, this study analyzed without prognosis data, and study samples size was limited. Large scale study needed to be perform, but serum ApoE measured by enzyme-linked immunosorbent assay was difficult to perform automate analysis. In this study, we used the conventional turbidimetric immunoassay kit to evaluate the serum ApoE as a diagnostic biomarker in NSCLC patients’ serum samples, which is suitable for screening test in primary hospital in developing country, such as in China. We also found serum ApoE levels to be associated with lymph node metastasis and distant metastasis in NSCLC patients, and elevated serum ApoE levels patients had poor prognosis. Meanwhile, from ROC/AUC analysis, we found ApoE levels at 41.25 mg/L could be the cut-off value for NSCLC, people with high ApoE levels will have more risk for NSCLC, and NSCLC patients with high serum ApoE levels get metastasis easier, which were consistent with Liu’s work (43.98 mg/L) [8].
There were several limitations in this study. First, it was a single institution study, a large multicenter, and multiracial study with large scale of NSCLC patients will be needed to evaluate the value of serum ApoE as diagnosis and evaluation biomarker of NSCLC. Second, CEA, SCC, and CYFRA 21–1 have no analysis in this study, we could not compare the usefulness of serum ApoE with existing markers.
Conclusions
In summary, we demonstrated that serum ApoE levels were elevated in the NSCLC patients compared to the healthy controls. We also found ApoE associated with TNM stages, lymph node metastasis, and distant metastasis, NSCLC patients with higher serum ApoE levels had poorer prognosis, suggest that serum ApoE may act as a useful clinical serological biomarkers for evaluating the metastasis of NSCLC.
References
Chen Z, Xu Z, Sun S, Yu Y, Lv D, Cao C, et al. Tgf-beta, 1, il–6, and tnf-alpha in bronchoalveolar lavage fluid: useful markers for lung cancer? Sci Rep. 2014;4:5595.
Spivey KA, Banyard J, Solis LM, Wistuba II, Barletta JA, Gandhi L, et al. Collagen xxiii: a potential biomarker for the detection of primary and recurrent non-small cell lung cancer. Cancer Epidemiol, Biomark Prev : Publ Am Assoc Cancer Res, Cosponsored Am Soc Prev Oncol. 2010;19:1362–72.
Farlow EC, Vercillo MS, Coon JS, Basu S, Kim AW, Faber LP, et al. A multi-analyte serum test for the detection of non-small cell lung cancer. Br J Cancer. 2010;103:1221–8.
Gumireddy K, Li A, Chang DH, Liu Q, Kossenkov AV, Yan J, et al. Akap4 is a circulating biomarker for non-small cell lung cancer. Oncotarget. 2015;6:17637–47.
Alberts WM. American College of Chest P: diagnosis and management of lung cancer executive summary: Accp evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132:1S–9.
Kraft HG, Menzel HJ, Hoppichler F, Vogel W, Utermann G. Changes of genetic apolipoprotein phenotypes caused by liver transplantation. Implications for apolipoprotein synthesis. J Clin Invest. 1989;83:137–42.
Huang Y, Mahley RW. Apolipoprotein e: structure and function in lipid metabolism, neurobiology, and alzheimer’s diseases. Neurobiol Dis. 2014;72:3–12.
Liu Z, Gao Y, Hao F, Lou X, Zhang X, Li Y, et al. Secretomes are a potential source of molecular targets for cancer therapies and indicate that apoe is a candidate biomarker for lung adenocarcinoma metastasis. Mol Biol Rep. 2014;41:7507–23.
Pencheva N, Tran H, Buss C, Huh D, Drobnjak M, Busam K, et al. Convergent multi-mirna targeting of apoe drives lrp1/lrp8-dependent melanoma metastasis and angiogenesis. Cell. 2012;151:1068–82.
Rice SJ, Liu X, Miller B, Joshi M, Zhu J, Caruso C, et al. Proteomic profiling of human plasma identifies apolipoprotein e as being associated with smoking and a marker for squamous metaplasia of the lung. Proteomics. 2015;15:3267–77.
Su WP, Chen YT, Lai WW, Lin CC, Yan JJ, Su WC. Apolipoprotein e expression promotes lung adenocarcinoma proliferation and migration and as a potential survival marker in lung cancer. Lung Cancer. 2011;71:28–33.
Wang Y, Chen Z, Chen J, Pan J, Zhang W, Pan Q, et al. The diagnostic value of apolipoprotein e in malignant pleural effusion associated with non-small cell lung cancer. Clinica Chimica Acta; Int J Clin Chem. 2013;421:230–5.
Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. International Association for the Study of Lung Cancer International Staging C, Participating I: the iaslc lung cancer staging project: proposals for the revision of the tnm stage groupings in the forthcoming (seventh) edition of the tnm classification of malignant tumours. J Thorac Oncol : Off Publ Int Assoc Study Lung Cancer. 2007;2:706–14.
Brambilla E, Travis WD, Colby TV, Corrin B, Shimosato Y. The new world health organization classification of lung tumours. Eur Respir J. 2001;18:1059–68.
Stieber P, Holdenrieder S. Lung cancer biomarkers—where we are and what we need. Cancer Biomarkers : Sect Dis Markers. 2010;6:221–4.
Wang DB, Lu XK, Zhang X, Li ZG, Li CX. Carbonic anhydrase 1 is a promising biomarker for early detection of non-small cell lung cancer. Tumour Biol J Int Soc Oncodevelopmental Biol Med 2015
Fan J, Yu H, Lv Y, Yin L. Diagnostic and prognostic value of serum thioredoxin and dj-1 in non-small cell lung carcinoma patients. Tumour Biol J Int Soc Oncodevelopmental Biol Med 2015
Wang T, Liang Y, Thakur A, Zhang S, Yang T, Chen T, et al. Diagnostic significance of s100a2 and s100a6 levels in sera of patients with non-small cell lung cancer. Tumour Biol J Int Soc Oncodevelopmental Biol Med 2015
Wikoff WR, Hanash S, DeFelice B, Miyamoto S, Barnett M, Zhao Y, et al. Diacetylspermine is a novel prediagnostic serum biomarker for non-small-cell lung cancer and has additive performance with pro-surfactant protein b. J Clin Oncol : Off J Am Soc Clin Oncol. 2015;33:3880–6.
Goodison S, Chang M, Dai Y, Urquidi V, Rosser CJ. A multi-analyte assay for the non-invasive detection of bladder cancer. PLoS One. 2012;7:e47469.
Cibeira GH, Giacomazzi J, Aguiar E, Schneider S, Ettrich B, CI DES, et al. Apolipoprotein e genetic polymorphism, serum lipoprotein levels and breast cancer risk: a case–control study. Mol Clin Oncol. 2014;2:1009–15.
Mrkonjic M, Chappell E, Pethe VV, Manno M, Daftary D, Greenwood CM, et al. Association of apolipoprotein e polymorphisms and dietary factors in colorectal cancer. Br J Cancer. 2009;100:1966–74.
Boylan KL, Andersen JD, Anderson LB, Higgins L, Skubitz AP. Quantitative proteomic analysis by itraq(r) for the identification of candidate biomarkers in ovarian cancer serum. Proteome Sci. 2010;8:31.
Oue N, Hamai Y, Mitani Y, Matsumura S, Oshimo Y, Aung PP, et al. Gene expression profile of gastric carcinoma: identification of genes and tags potentially involved in invasion, metastasis, and carcinogenesis by serial analysis of gene expression. Cancer Res. 2004;64:2397–405.
Chen YC, Pohl G, Wang TL, Morin PJ, Risberg B, Kristensen GB, et al. Apolipoprotein e is required for cell proliferation and survival in ovarian cancer. Cancer Res. 2005;65:331–7.
Chen J, Wu W, Zhen C, Zhou H, Yang R, Chen L, et al. Expression and clinical significance of complement c3, complement c4b1 and apolipoprotein e in pancreatic cancer. Oncol Lett. 2013;6:43–8.
Acknowledgments
The work was supported by grants from the Specialized Research Fund for the Doctoral Program of Higher Education of China (Grant No. 20130171120069 to LSL), and the Science and Technology Department of Guangdong Province (Grant No. 2014A020212477 to LSL, 2014A020212720 to JML), and the Natural Science Foundation of Guangdong Province, China (Grant No. 2015A030313035 to LSL), and the Science and Technology Department of Guangzhou City, China (Grant No. 201400000004–2 to ML). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authors’ contributions
LSL and ML designed the experiment, interpreted the data, and prepared the manuscript. JML, JLS, PNF, YHW, and WQL conducted the experiment, collected the data, and helped to prepare the manuscript. LSL and ML interpreted the data. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflicts interest
None
Additional information
Jinmei Luo and Junli Song contributed equally to this work.
Rights and permissions
About this article

Cite this article
Luo, J., Song, J., Feng, P. et al. Elevated serum apolipoprotein E is associated with metastasis and poor prognosis of non-small cell lung cancer. Tumor Biol. 37, 10715–10721 (2016). https://doi.org/10.1007/s13277-016-4975-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-016-4975-4