
Abstract
TGF-β1 and oxidative stress are involved in cancer progression, but in melanoma, their role is still controversial. Our aim was to correlate plasma TGF-β1 levels and systemic oxidative stress biomarkers in patients with melanoma, with or without disease metastasis, to understand their participation in melanoma progression. Thirty patients were recruited for melanoma surveillance, together with 30 healthy volunteers. Patients were divided into two groups: Non-metastasis, comprising patients with tumor removal and no metastatic episode for 3 years; and Metastasis, comprising patients with a metastatic episode. The plasmatic cytokines TGF-β1, IL-1 β, and TNF-α were analyzed by ELISA. For oxidative stress, the following assays were performed: malondialdehyde (MDA), advanced oxidation protein products (AOPP) levels, total radical-trapping antioxidant parameter (TRAP) and thiol in plasma, and lipid peroxidation, SOD and catalase activity and GSH in erythrocytes. Patients with a metastatic episode had less circulating TGF-β1 and increased TRAP, thiol, AOPP and lipid peroxidation levels. MDA was increased in both melanoma groups, while catalase, GSH, and IL-1β was decreased in Non-metastasis patients. Significant negative correlations were observed between TGF-β1 levels and systemic MDA, and TGF-β1 levels and systemic AOPP, while a positive correlation was observed between TGF-β1 levels and erythrocyte GSH. Lower levels of TGF-β1 were related to increased oxidative stress in Metastasis patients, reinforcing new evidence that in melanoma TGF-β1 acts as a tumor suppressor, inhibiting tumor relapse. These findings provide new knowledge concerning this cancer pathophysiology, extending the possibilities of investigating new therapies based on this evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cutaneous melanoma is a highly aggressive malignancy with increasing incidence and limited therapeutic options in the metastatic stage of the disease. A primary cutaneous melanoma will not kill the patient, but its metastases will. The tumor suppression effects derived from epithelial, endothelial, myeloid and lymphoid cancer cell types are well understood, but in melanoma that arises from the transformation of neural crest-derived melanocytes, the suppressor, and prometastatic effects are still controversial [1–5]. Transforming growth factor beta 1 (TGF-β1) has been linked in several stages of cancer progression [6, 7], and has its role in the modulation of cell growth is still under investigation [1, 2, 8]. TGF-β1 can inhibit tumor growth and the migration of murine melanoma cells in vivo, and human melanoma cells in vitro, even though TGF-β1 is increased in the plasma of melanoma patients in all stages of the disease [2, 9–11]. Furthermore, in a recent study, Tas et al. [12] showed that TGF-β1 is a potential prognostic biomarker in patients with melanoma. Reactive oxygen species (ROS) has been related in many types of cancer, are important cellular messengers [13], and in melanoma, they are present in all stages of its development [14–16]. Systemic oxidative stress in melanoma patients is poorly investigated, but it is known that these patients present systemic and tumor redox deregulation [15–17]. The specific molecular targets of TGF-β1-stimulated ROS are unknown, but the TGF-β1 action in redox systems on different cells lineages regulates a number of physiological actions, such as growth-inhibitory effects, apoptosis and activation of latent TGF-β1 [18–21].
In human melanoma, TGF-β1 regulatory responses remain unclear and the characterization of circulation levels is controversial [9, 11, 12]. It is known that there is an important link between oxidative stress and this cytokine function; thus, in this study, we aimed to correlate plasma TGF-β1 levels and systemic oxidative stress biomarkers in patients with melanoma, with or without metastasis, to understand the role of TGF-β1 in systemic oxidative stress of human melanoma in two different conditions of the disease.
Materials and methods
Ethical approval
This study was approved by the National Research Ethics Committee, under protocol no. CAAE 5831.0.000.268.10. All the practices were approved by the institutional board, and all patients and controls signed a term of informed consent. All procedures in this study involving human participants were in accordance with the ethical standards of the local research committee and with the 1964 Helsinki Declaration and its later amendments of comparable ethical standards.
Sample collection and study design
A total of 30 patients between 28 and 67 years old were recruited for melanoma surveillance at the Londrina Cancer Hospital between April 2011 and November 2012. Sixteen patients had localized primary cutaneous melanoma stage I/II, with surgical tumor removal and no metastatic episode over a 3-year period (Non-metastasis group); and 14 patients had stage III/IV melanoma, with regional or distant metastasis (Metastasis group). In the latter group, six patients were submitted to surgical metastasis removal, and eight patients had metastasis at the time of blood collection (see Table 1). None of the patients were submitted to chemotherapy or immunotherapy treatment. The control group comprised 30 healthy women and men volunteers. Patients and controls were non-smoking or in antioxidant therapy treatment, were not obese and did not present hepatic, cardiac, or renal dysfunction. In addition, the control volunteers had no previous history of any type of cancer. Since people with fair skin are known to present a greater incidence of melanoma, the skin type of all the participants was classified using the self-rated Fitzpatrick skin phototype classification (FSPC) in order to ensure a similar pattern between the groups [22]. Venous blood was collected with heparin and centrifuged at 1100×g. Separated plasma were immediately frozen at −80 °C until oxidative stress or enzyme immunoassay (ELISA) analysis, while the erythrocytes were used fresh to evaluate lipid peroxidation in cell membrane.
Reagents
All the chemical reagents were purchased from Sigma Aldrich (St; Louis, MO, USA).
Sample-size calculation
The 2012 estimated melanoma incidence in the area of this study was 4.43/100,000 inhabitants [23]. To determine the minimal sample size required to estimate the proportion with the desired level of precision, we used the formula n = (Z 1 2 −α/2 P(1 − P)) / d 2, where: n = number of melanoma patients; Z 1 2-α = Constant valor for 95 % confidence level (1.96); P = Population proportion (0.0043 %); d = Level of significance α (α = 0.05) [24]. According to this formula, the minimum melanoma patient sample size was 7.
Plasma enzyme immunoassay analysis
Human/mouse TGF-β1 levels, human plasma TNF-α and human interleukin 1-beta (IL-1β) were determined by a sandwich enzyme-linked immunosorbent assay (ELISA), following the manufacturers’ instructions (eBioscience®), and analyzed with a microplate reader (Multiskan GO®, Thermo Fisher Scientific, Rockford, USA) at 450 nm. For TGF-β1 analysis, plasma samples were previously acidified to activate latent TGF-β1 to its immunoreactive form. Standard curves were constructed by a five-parameter regression formula and plotted as a linear curve (log-log). The results were calculated in pg mL−1.
Evaluation of oxidative stress in plasma
Plasma malondialdehyde (MDA) was measured by high-performance liquid chromatography (HPLC), as described by Victorino et al. [25]. Briefly, 160 μL of plasma sample was mixed with 100 μL of 0.5 M perchloric acid and incubated for 10 min on ice to precipitate the proteins, and then mixed with 100 μL of 1 % thiobarbituric acid. This reaction was incubated for 30 min in a boiling water bath and transferred to an ice bath to stop the reaction. A 100 μL volume of 1 M NaH2PO4, pH 7, was added to each sample to stabilize the sample pH. Samples were centrifuged for 10 min at 5000×g at 4 °C. The supernatants were filtered and injected into the LC-20AT® HPLC system (Shimadzu, Kyoto, Japan) in a mobile phase consisting of 65 % 50 mM KH2PO4 buffer and 35 % HPLC-grade methanol in a ShimPack® C18 reverse-phase column (Shimadzu, Kyoto, Japan). Acid hydrolyzed 1,1,3,3-tetraethoxypropane (TEP) was used as standard to obtain the linear regression equation and calculate the MDA concentration of the samples. Readings were obtained at 535 nm over 11 min at a flow rate of 0.8 mL/min at 35 °C, and the results were expressed as nM of MDA.
To evaluate oxidized protein formation by inflammatory response, the advanced oxidation protein products (AOPP) levels were measured. AOPP levels were measured as described by Descamps-Latscha et al. [26] in a microplate reader. Briefly, plasma was diluted 1:5 in phosphate-buffered saline (PBS). Supernatant samples or chloramine-T standard solutions (200 μL) were placed in the appropriate wells of a 96-well microtiter plate, 10 μL of 1.16 mol/L KI was added to each well and 20 μL of acetic acid was added 2 min later. The absorbance of the reaction mixture was immediately read at 340 nm against a blank containing 200 μL of PBS, 10 μL of KI, and 20 μL of acetic acid. AOPP levels were calculated using a chloramine-T calibration curve. Total protein was measured by the Lowry technique [27], modified by Miller [28], using bovine serum albumin (Sigma Aldrich®) as standard. The results were expressed in μM mg protein−1.
Total radical-trapping antioxidant parameter (TRAP) of plasma was determined as described by Repetto et al. [29]. The reaction medium contained 70 μL of plasma sample diluted 1:50 in glycine buffer (0.1 M, pH 8.6), 20 μM 2-azo-bis-(2-amidinopropane) and 200 μM luminol at 37 °C. Trolox, a soluble E vitamin analogue, was used as the reference antioxidant (1.75 μM in the reaction medium). Chemiluminescence curves were obtained in a GloMax® luminometer 20/20 (Promega, Madison, WI, USA), and the results were expressed in μM of Trolox.
Total thiols in plasma were measured by the method of Hu [30]. The final volume of 400 μL contained 40 μL of plasma and 320 μL of 0.25 M TRIS buffer containing 0.02 M EDTA, pH 8.2, followed by the addition of 40 μL of 0.01 M 2,2-dithiobisnitrobenzoic acid (DTNB) in absolute methanol. The tubes were capped and color was developed for 15 min at room temperature. The tubes were then centrifuged at 3,000×g for 15 min. Supernatant was collected and absorbance measured at 412 nm in a microplate reader. Total thiol groups were calculated using a calibration curve prepared by reduced glutathione (GSH).
Evaluation of oxidative stress in erythrocytes
Erythrocytes was obtained from heparinized blood and washed three times with 0.9 % saline solution at 4 °C. An aliquot of heparinized blood was used to determine hemoglobin (Coulter STKS®, Hialeah, FL, USA).
Erythrocyte lipoperoxidation was evaluated by chemiluminescence (CL) according to Panis et al. [31]. Briefly, 30 μL of packed erythrocytes were added to 3 mL of phosphate buffer, and 1 mL of this solution was diluted in 12.3 mL of the same buffer. The chemiluminescent reaction was initiated by the addition of tert-butyl (10 μl) at a final concentration of 3 mM in 1 mL of erythrocyte sample. Chemiluminescence curves were obtained in a GloMax® luminometer 20/20, and the results were expressed in relative light units (RLU) g hemoglobin−1. The curve obtained was used as a qualitative indicator of lipoperoxidation, and quantitative results were obtained following area under curve integration using GraphPad Prism® version 5.0 (GraphPad Software, San Diego, CA, USA).
Superoxide (SOD) activity was determined according to the method of Marklund and Marklund [32] using different contents of diluted erythrocytes at a ratio of 1:20 in deionized water. The samples were incubated in 1 M TRIS buffer and 0.15 mM pyrogallol, and autoxidation inhibition was measured at 420 nm in a UV-1650 PC® UV–vis spectrophotometer. The autoxidation of pyrogallol alone was used as a control. The amount of SOD that is able to inhibit 50 % of pyrogallol autoxidation is defined as the enzymatic activity unit (U). The final SOD results were expressed in U SOD g hemoglobin−1 103.
Catalase activity was determined as described by Aebi [33]. Washed erythrocytes were diluted 1:80 in deionized water, and 10 μL was incubated in a system containing 1 M TRIS buffer and 200 mM H2O2 solution. Absorbance disappearance kinetics was monitored in a UV-1650 PC® UV–vis spectrophotometer at 240 nm (Shimadzu, Kyoto, Japan). The results are expressed in absorbance decreased in 1 min (V abs/min) g hemoglobin−1 103.
Total (GT) and oxidized glutathione disulfide (GSSG) levels were determined with diluted erythrocytes at a ratio of 1:20 in deionized water incubated with 60 μM 5,5′-dithiobis (2-nitrobenzoic acid) in a 1 M TRIS buffer according to the method described by Tietze [34], after which the GSH value (GSH = Total glutathione − GSSG) was calculated. The kinetic curves were measured at 412 nm for 3 min using a UV-1650 PC® UV–vis spectrophotometer. The results were expressed in μM g Hb−1.
Statistical analysis
Comparisons were performed as follows: Control × Non-metastasis group and Control × Metastasis group. All data were expressed as arithmetic means and standard errors of means (SEM). The Shapiro–Wilk W test verified the normality of the data. For quantitative analysis, data with normal distribution were compared by the t test and data with non-normal distribution, by the Mann–Whitney test. CL curves were analyzed by the two-way ANOVA test. Spearman’s correlation test was used for TGF-β1 and OS parameters because the data analyzed showed non-normal distribution. Differences were considered statistically significant when p < 0.05. All the statistical analyses were performed using GraphPad Prism® version 5.0 (GraphPad Software).
Results
Characterization of the cohort and immunological parameters
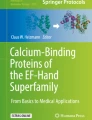
Table 1 presents the characterization of the individuals studied. TGF-β was decreased in the Metastasis group (Control 4902 ± 498.6 pg mL−1; Non-metastasis 4201 ± 862.0 pg mL−1, p = 0.1263; Metastasis 2985 ± 276.7 pg mL−1, p = 0.0272). Plasma IL-1β was increased in the Non-metastasis group (Control 6.533 ± 0.9448 pg mL−1; Non-metastasis 11.21 ± 2.120 pg mL−1, p = 0.0152; Metastasis 6.375 ± 1.048 pg mL−1, p = 0.8997) and plasma TNF-α showed no difference among groups (Control 11.92 ± 1.243 pg mL−1; Non-metastasis 17.12 ± 3.884 pg mL−1, p = 0.1817; Metastasis 9.641 ± 0.8492 pg mL−1, p = 0.6055) (Fig. 1a, b, c).

Systemic a TGF-β, b IL-1β, and c TNF-α levels in patients with cutaneous and metastatic melanoma. Non-metastasis group: localized primary cutaneous melanoma stage I/II with surgical tumor removal and no relapse episode in a 3-year period; Metastasis: melanoma and disease relapse (Stages III/IV), with or without surgical tumor removal. Melanoma groups were compared with control group by the Mann–Whitney test.*p < 0.05
Systemic oxidative stress evaluation
In the plasma samples, MDA levels were increased in both melanoma groups (Control 175.4 ± 22.55 nM; Non-metastasis 294.2 ± 24.53 nM, p = 0.0005; Metastasis 336.5 ± 38.78 nM, p = 0.0004) (Fig. 2a). AOPP, an oxidized protein generate by oxidative burst and inflammatory response, was increased only in the Metastasis group (Control 1.013 ± 0.04838 μM mg−1 protein; Non-metastasis 1.104 ± 0.065 μM mg−1 protein, p = 0.2662; Metastasis 1.235 ± 0.092 μM mg−1 protein, p = 0.0243) (Fig. 2b). Patients with melanoma metastasis had increased antioxidant parameters in the plasma. Figure 2c shows a rise in TRAP levels (Control 28.72 ± 3.098 μM Trolox; Non-metastasis 38.65 ± 5.356 μM Trolox, p = 0.1484; Metastasis 45.04 ± 7.204 μM Trolox, p = 0.0472), while Fig. 2d shows a rise in Thiol levels (Control 194.7 ± 5.733 μM; Non-metastasis 208.3 ± 7.610 μM, p = 0.1612; Metastasis 222.0 ± 9.751 μM, p = 0.0172).

Systemic antioxidant a MDA, b AOPP, c TRAP, and (d) Thiol levels in patients with cutaneous and metastatic melanoma. Non-metastasis group: localized primary cutaneous melanoma stage I/II with surgical tumor removal and no relapse episode in a 3-year period; Metastasis: melanoma and disease relapse (Stages III/IV), with or without surgical tumor removal. Melanoma groups were compared with control group by the Mann–Whitney test.*p < 0.05. MDA malondialdehyde; AOPP advanced oxidation protein products; TRAP total radical-trapping antioxidant parameter. *p < 0.05
In erythrocytes, all the CL curves were different by two-way ANOVA test (p < 0.0001) (Fig. 3a). Figure 3b shows increased AUC values in the Metastasis group (74.630 ± 8298; p = 0.0329) compared with the Control (60.440 ± 2365), while the Non-metastasis group was not significantly different (63.160 ± 3957; p = 0.5328) from the Control. No statistical differences were observed in SOD activity among the groups (Fig. 3c) (Control 8.185 ± 0.535 U SOD g Hb−1 103; Non-metastasis 8.787 ± 0.472 U SOD g Hb−1 103, p = 0.4721; Metastasis 7.758 ± 0.704 U SOD g Hb−1 103, p = 0.577). Figure 3d shows decreased catalase activity in the Non-metastasis group (Control 11.890 ± 0.714 V abs/min g Hb−1 103; Non-metastasis 9.352 ± 0.616 V abs/min g Hb−1 103, p = 0.050) but not in the Metastasis group, although the p value showed a trend toward decreased activity (Metastasis 9.757 ± 0.749 V abs/min g Hb−1 103, p = 0.051). GSH levels were decreased in the Non-metastasis group but not in the Metastasis group (Control 198.6 ± 38.66 μM g Hb−1; Non-metastasis 73.50 ± 4.194, p = 0.045; Metastasis 88.93 ± 10.56 66 μM g Hb−1) (Fig. 3e).

a Erythrocyte lipid peroxidation by CL, b erythrocyte lipid peroxidation analysis of the area under curve, c erythrocyte SOD levels, d erythrocyte catalase levels and e erythrocyte GSH levels in patients with cutaneous and metastatic melanoma. Non-metastasis group: localized primary cutaneous melanoma stage I/II with surgical tumor removal and no relapse episode in a 3-year period; Metastasis: melanoma and disease relapse (Stages III/IV), with or without surgical tumor removal. Melanoma groups were compared with control group by the Mann–Whitney test.*p < 0.05. CL: chemiluminescence; AUC area under curve; SOD superoxide dismutase; GSH reduced glutathione. *p < 0.05
Significant negative correlations were verified between TGF-β1 levels and systemic MDA, and TGF-β1 levels and systemic AOPP and a positive correlation was verified between TGF-β1 levels and erythrocyte GSH (see Table 2).
Discussion
The incidence of melanoma has increased, but this was not accompanied by the development of effective therapies for patients with advanced disease [35]. Despite specific and effective immunotherapy available in the last few years, many patients have developed pharmacological resistance to this treatment [36]. While very early-stage melanoma (localized, stages I and II) is >90 % curable by surgical excision, disseminated stage IV melanoma leads to a life expectancy of less than a year [3, 37]. For this reason, it is imperative to understand the progression of this disease and all the factors involved in it. The presence of TGF-β in human melanoma tissue is extensively reported and its expression is increased, particularly in metastatic tumors [11, 38, 39], together with its inflammatory status. In addition, oxidative stress has been related to cancer promotion, progression, and metastasis. However, the relationship between TGF-β and oxidative stress has not been reported in melanoma. There are few studies showing the interaction between TGF-β and oxidative stress in carcinogenesis and metastasis. Studies conducted on malignant keratinocytes, but not their pre-malignant counterparts, produce high levels of ROS, which, in turn, increase TGF-β expression and induce fibroblast activation and senescence [40]. An experimental study investigated the effect of curcumin treatment, a natural antioxidant, on 1,2-dimethylhydrazine-induced colon carcinogenesis in mice. This study concluded that the protective effect of curcumin on colon carcinogenesis was driven by the interplay between nitrosative and oxidative stress reduction and the upregulation of TGF-β1 expression signaling [41].
Here, we verified a decrease in circulating TGF-β1 in advanced disease, but not in non-metastatic melanoma. Recently, Humbert and Lebrun [2] showed a protective role of TGF-β1 in human melanoma cell migration and invasion in vitro. In a murine melanoma model, TGF-β1 also decreased the metastatic process [10]. Classically, TGF-β1 is an important anti-inflammatory mediator [42, 43]. As evidence that low levels of circulating TGF-β1 have a pro-inflammatory effect in cancer, patients with triple negative breast cancer and with metastasis show low levels of TGF-β1, which is related to poor prognosis [44]. Furthermore, in a recent study, Tas et al. [12] showed that patients with melanoma and elevated serum TGF-β1 concentrations had favorable overall survival compared with those with lower levels. IL-1β, another pro-inflammatory cytokine, was higher in the Non-metastasis group. No significant alterations were observed in TNF-α levels, despite a higher mean in relation to control levels in the Non-metastasis group.
To elicit biological activity, TGF-β must be released from a latent complex and the antioxidant system has been described as a protective mechanism against latent TGF-β activation in pathological processes, indicating that the increased circulating antioxidant levels may reflect TGF-β redox regulation [45]. Increased antioxidant response with increased pro-oxidant products can indicate a compensatory mechanism under sustained oxidative stress conditions [46]. Our findings support this, since even though TRAP and thiols were increased, patients with metastasis showed increased AOPP, MDA, and erythrocyte CL levels. AAOP is formed primarily by chlorinated oxidants (including hypochlorous acid and chloramines) that result from myeloperoxidase activity during a respiratory burst [47]. Since TGF-β1 also suppresses the expression of ROS intermediates and respiratory burst capacity by both resting blood monocytes and activated macrophages [48], it is reasonable to suppose that decreased TGF-β stimulates respiratory burst, which could explain the increased AOPP levels verified in the Metastasis group. Furthermore, increased AOPP levels have been observed in patients with several types of cancer and with advanced disease [49], but it has not been previously investigated in melanoma.
The increase in erythrocyte CL only in patients with metastasis indicates alterations in cell membrane properties, such as antioxidant composition, which modify the kinetics pattern by depleting the oxidizable species [50]. Erythrocyte levels of the antioxidant enzymes SOD and catalase and of the antioxidant peptide GSH are widely used to estimate the cell’s intracellular antioxidant system [46]. GSH is an important intracellular antioxidant, and since it acts as ROS scavenger, in situations of increased oxidative stress its levels usually decrease. Both melanoma groups showed decreased GSH and catalase levels, although this only showed statistical significance in the Non-metastasis group. There was no variation in SOD activity, but a significant reduction in catalase activity was observed in the non-metastatic group and a tendency toward reduction in the metastatic group. This scenario may support, in part, the oxidative stress observed in this study, since SOD generates hydrogen peroxide (H2O2), which when it accumulates, triggers damage and signals several pathways. The decrease in TGF-β verified in patients with stage III/IV melanoma was statistically significant and inversely correlated with the systemic pro-oxidant biomarkers MDA and AOPP, and positively correlated with the levels of the antioxidant GSH. Similar to our study, Panis et al. [44] showed a positive correlation between circulating TGF-β1 and erythrocyte GSH levels in patients with breast cancer. Based on this evidence, we suggest that in advanced melanoma, systemic low TGF-β1 has a pro-inflammatory role, stimulating pro-oxidative status and the metastatic process, since inflammation is closely associated with oxidative stress and metastasis [51].
Our findings reinforce recent evidence that patients with elevated levels of systemic TGF-β1 show favorable overall survival compared with those with lower levels [12] since this seem to prevent the disease from metastasizing. A limitation that should be highlighted is that numerous patients were tumor-free at the time of blood sample collection, even though it has previously been shown for our group that patients with melanoma present systemic pro-oxidant status post-surgery, demonstrating a role of oxidative stress in melanoma [52]. These limitations do not detract from the importance of the finding that patients with melanoma present significant changes in TGF-β1 levels and biomarkers of oxidative stress compared with healthy individuals. Our results indicate an interplay between oxidative stress and TGF-β1 in melanoma progression. Furthermore, our study contributes to the literature because is the first to show significant relationships between circulating TGF- β1 levels, systemic oxidative stress and metastatic episodes in patients with melanoma, providing a new perspective on the pathogenesis of melanoma and further insight in the search for new therapies.
References
Lebrun JJ. The dual role of TGF-beta in human cancer: from tumor suppression to cancer metastasis. ISRN Mol Biol. 2012. doi:10.5402/2012/381428.
Humbert L, Lebrun JJ. TGF-beta inhibits human cutaneous melanoma cell migration and invasion through regulation of the plasminogen activator system. Cell Signal. 2013. doi:10.1016/j.cellsig.2012.10.011.
Moustakas A. TGF-beta targets PAX3 to control melanocyte differentiation. Dev Cell. 2008. doi:10.1016/j.devcel.2008.11.009.
Schriek G, Oppitz M, Busch C, Just L, Drews U. Human SK-Mel 28 melanoma cells resume neural crest cell migration after transplantation into the chick embryo. Melanoma Res. 2005;15:225–34.
Perrot CY, Javelaud D, Mauviel A. Insights into the transforming growth factor-β signaling pathway in cutaneous melanoma. Ann Dermatol. 2013. doi:10.5021/ad.2013.25.2.135.
Lo RS, Witte ON. Transforming growth factor-beta activation promotes genetic context-dependent invasion of immortalized melanocytes. Cancer Res. 2008;68:4248–57.
Javelaud D, Alexaki VI, Mauviel A. Transforming growth factor-β in cutaneous melanoma. Pigment Cell Melanoma Res. 2008;21:123–32.
Krasagakis K, Garbe C, Schrier PI, Orfanos CE. Paracrine and autocrine regulation of human melanocyte and melanoma cell growth by transforming growth factor beta in vitro. Anticancer Res. 1994;14:2565–71.
Krasagakis K, Thölke D, Farthmann B, Eberle J, Mansmann U, Orfanos CE. Elevated plasma levels of transforming growth factor (TGF)-beta 1 and TGF-beta 2 in patients with disseminated malignant melanoma. Br J Cancer. 1998;77:1492–4.
Ramont SP, Hornebeck W, Maquart FX, Monboisse JC. Transforming growth factor-β1 inhibits tumor growth in a mouse melanoma model by down-regulating the plasminogen activation system. Exp Cell Res. 2003;291:1–10.
Malaponte G, Zacchia A, Bevelacqua Y, Marconi A, Perrotta R, Mazzarino MC, et al. Co-regulated expression of matrix metalloproteinase-2 and transforming growth factor-beta in melanoma development and progression. Oncol Rep. 2010;24:81–7.
Tas F, Karabulut S, Yasasever CT, Duranyildiz D. Serum transforming growth factor-beta 1 (TGF-β1) levels have diagnostic, predictive, and possible prognostic roles in patients with melanoma. Tumour Biol. 2014. doi:10.1007/s13277-014-1984-z.
Meyer M, Pahl HL, Baeuerle PA. Regulation of the transcription factors NF-κB and AP-1 by redox changes. Chem Biol Interact. 1994;91:91–100.
Meyskens Jr FL, McNulty SE, Buckmeier JA, Tohidian NB, Spillane TJ, Kahlon RS, et al. Aberrant redox regulation in human metastatic melanoma cells compared to normal melanocytes. Free Radic Biol Med. 2001;31:799–808.
Sander CS, Hamm F, Elsner P, Thiele JJ. Oxidative stress in malignant melanoma and non-melanoma skin cancer. Br J Dermatol. 2003;148:913–22.
Gadjeva V, Dimov A, Georgieva N. Influence of therapy on the antioxidant status in patients with melanoma. J Clin Pharm Ther. 2008. doi:10.1111/j.1365-2710.2008.00909.x.
Picardo M, Grammatico P, Roccella F, Roccella M, Grandinetti M, Del Porto G, et al. Imbalance in the antioxidant pool in melanoma cells and normal melanocytes from patients with melanoma. J Investig Dermatol. 1996;107:322–6.
Barcellos-Hoff MH, Dix TA. Redox-mediated activation of latent transforming growth factor-beta 1. Mol Endocrinol. 1996;10:1077–83.
Bauer G. Elimination of transformed cells by normal cells: a novel concept for the control of carcinogenesis. Histol Histopathol. 1996;11:237–55.
Häufel T, Dormann S, Hanusch J, Schwieger A, Bauer G. Three distinct roles for TGF-beta during intercellular induction of apoptosis: a review. Anticancer Res. 1999;19:105–11.
De Bleser PJ, Xu G, Rombouts K, Rogiers V, Geerts A. Glutathione levels discriminate between oxidative stress and transforming growth factor-beta signaling in activated rat hepatic stellate cells. J Biol Chem. 1999;274:33881–7.
Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869–71.
(INCA), I. N. D. C. Estimativas da incidência e mortalidade por câncer no Brasil. Rio de Janeiro: Ministério da Saúde; 2014.
Lawanga SK, Lemeshow S. Sample size determination in health studies. World Health Organization – Geneva, 1991. ISBN 92 4 154405.
Victorino VJ, Panis C, Campos FC, Cayres RC, Colado-Simão AN, Oliveira SR, et al. Decreased oxidant profile and increased antioxidant capacity in naturally postmenopausal women. Age (Dordr). 2013;35:1411–21. doi:10.1007/s11357-012-9431-9.
Descamps-Latscha B, Witko-Sarsat V, Nguyen-Khoa T, Nguyen AT, Gausson V, Mothu N, et al. Early prediction of IgA nephropathy progression: proteinuria and AOPP are strong prognostic markers. Kidney Int. 2004;66:1606–12.
Lowry OH, Rosenbrough NJ, Farr AL, Randall RJ. Protein measurement with the folin phenol reagent. J Biol Chem. 1951;193:265–72.
Miller G. Protein determination of large numbers of samples. Anal Chem. 1959;31:964.
Repetto M, Reides C, Gomez Carretero ML, Costa M, Griemberg G, Llesuy S. Oxidative stress in blood of HIV infected patients. Clin Chim Acta. 1996;255:107–17.
Hu ML. Measurement of protein thiol groups and GSH in plasma. In: Sies H, Abelson J, Simon M, editors. Methods in enzymoly 233. San Diego: Academic; 2004. p. 380–5.
Panis C, Herrera AC, Victorino VJ, Campos FC, Freitas LF, De Rossi T, et al. Oxidative stress and hematological profiles of advanced breast cancer patients subjected to paclitaxel or doxorubicin chemotherapy. Breast Cancer Res Treat. 2012;133:89–97.
Marklund S, Marklund G. Involvement of the superoxide anion radical in the autoxidation of pyrogallol and a convenient assay for superoxide dismutase. Eur J Biochem. 1974;47:469–74.
Aebi H. Catalase in vitro. In: Sies H, Kaplan N, Colowick N, editors. Methods in enzymoly 105. San Diego: Academic; 1984. p. 121–1266.
Tietze F. Enzymic method for quantitative determination of nanogram amounts of total and oxidized glutathione: applications to mammalian blood and other tissues. Anal Biochem. 1969;27:502–22.
Flaherty KT, Puzanov I, Kim KB, Ribas A, McArthur GA, Sosman J, et al. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med. 2010;363:809–19.
Rizos H, Menzies AM, Pupo GM, Carlino MS, Fung C, Hyman J, et al. BRAF inhibitor resistance mechanisms in metastatic melanoma: spectrum and clinical impact. Clin Cancer Res. 2014;20:1965–77.
Kim CJ, Reintgen DS, Balch CM. The new melanoma staging system. Cancer Control. 2002;9:9–15.
Schmid P, Itin P, Rufli T. In situ analysis of transforming growth factor-beta s (TGF-beta 1, TGF-beta 2, TGF-beta 3), and TGF-beta type II receptor expression in malignant melanoma. Carcinogenesis. 1995;16:1499–503.
Van Belle P, Rodeck U, Nuamah I, Halpern AC, Elder DE. Melanoma-associated expression of transforming growth factor-beta isoforms. Am J Pathol. 1996;148:1887–94.
Hassona Y, Cirillo N, Lim KP, Herman A, Mellone M, Thomas GJ, et al. Progression of genotype-specific oral cancer leads to senescence of cancer-associated fibroblasts and is mediated by oxidative stress and TGF-β. Carcinogenesis. 2013;34(6):1286–95.
Bounaama A, Djerdjouri B, Laroche-Clary A, Le Morvan V, Robert J. Short curcumin treatment modulates oxidative stress, arginase activity, aberrant crypt foci, and TGF-β1 and HES-1 transcripts in 1,2-dimethylhydrazine-colon carcinogenesis in mice. Toxicology. 2012;302(2–3):308–17.
Munger JS, Huang X, Kawakatsu H, Griffiths MJ, Dalton SL, Wu J, et al. The integrin alpha v beta 6 binds and activates latent TGF beta 1: a mechanism for regulating pulmonary inflammation and fibrosis. Cell. 1999;96:319–28.
Shull MM, Ormsby I, Kier AB, Pawlowski S, Diebold RJ, Yin M, et al. Targeted disruption of the mouse transforming growth factor-beta 1 gene results in multifocal inflammatory disease. Nature. 1992;359:693–9.
Panis C, Herrera AC, Victorino VJ, Aranome AM, Cecchini R. Screening of circulating TGF-β levels and its clinicopathological significance in human breast cancer. Anticancer Res. 2013;33:737–42.
Cui Y, Robertson J, Maharaj S, Waldhauser L, Niu J, Wang J, et al. Oxidative stress contributes to the induction and persistence of TGF-β1 induced pulmonary fibrosis. Int J Biochem Cell Biol. 2011;43:1122–33.
Halliwel B, Gutteridge JMC. Free radicals in biology and medicine. 4th ed. Oxford: Oxford University Press; 2007.
Korkmaz GG, Altınoglu E, Civelek S, Sozer V, Erdenen F, Tabak O, et al. The association of oxidative stress markers with conventional risk factors in the metabolic syndrome. Metabolism. 2013;62:828–35.
Letterio JJ, Roberts AB. Regulation of immune responses by TGF-beta. Annu Rev Immunol. 1998;16:137–61.
Suzuki Y, Ohno S, Okuyama R, Aruga A, Yamamoto M, Miura S, et al. Determination of chronic inflammatory states in cancer patients using assay of reactive oxygen species production by neutrophils. Anticancer Res. 2012;32:565–70.
Azorin I, Bella MC, Iborra FJ, Fornas E, Renau-Piqueras J. Effect of tert-butyl hydroperoxide addition on spontaneous chemiluminescence in brain. Free Radic Biol Med. 1995;19:795–803.
Halliwell B. Oxidative stress and cancer: have we moved forward? Biochem J. 2007;401:1–11.
Bernardes SS, Souza-Neto FP, Ramalho LN, Derossi DR, Guarnier FA, Silva CF, et al. Systemic oxidative profile after tumor removal and the tumor microenvironment in melanoma patients. Cancer Lett. 2015. doi:10.1016/j.canlet.2015.03.007.
Acknowledgments
The authors are grateful to J.A. Vargas and P. S. R. D. Filho for their excellent technical assistance and E. C. B. Carmelo of the Department of Clinical Research of the Londrina Cancer Hospital for her important assistance in patient recruitment and interview. The authors would also like to thank physicians M. A. Buges and C. Z. Campos for allowing their patients to participate in the study. The authors also thank the Araucária Foundation for providing financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Santos Bernardes, S., de Souza-Neto, F.P., Pasqual Melo, G. et al. Correlation of TGF-β1 and oxidative stress in the blood of patients with melanoma: a clue to understanding melanoma progression?. Tumor Biol. 37, 10753–10761 (2016). https://doi.org/10.1007/s13277-016-4967-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-016-4967-4