
Abstract
Breast cancers (BC) are treated with surgery, radiotherapy, and chemotherapy. Neoadjuvant chemotherapy (NACT) is an emerging treatment option in many cancers and is given before primary therapy to shrink tumor size. The efficacy of NACT in varied settings of BC, such as inoperable tumors, borderline resectable tumors, and breast-conserving surgery, has been debated extensively in literature, and the results remain unclear and depended on a wide variety of factors such as cancer type, disease extent, and the specific combination of chemotherapy drugs. This study was performed to examine the efficacy, toxicity, and tolerability of pirarubicin (THP) and epirubicin (EPI) in combination with docetaxel and cyclophosphamide in a NACT setting for BC. A total of 48 patients with stage II or III breast cancers were randomly divided into two groups: THP group and EPI group. The patients in THP group received 2–4 cycles of neoadjuvant chemotherapy with DTC regimen (docetaxel, THP, cyclophosphamide), while patients in the EPI group received 2–4 cycles of DEC regimen (docetaxel, EPI, cyclophosphamide) before surgery. The incidence of adverse reactions and the efficacy of the treatment regimen were compared between the two groups. Prognostic evaluation indexes were estimated by Kaplan-Meier survival analysis, including the 5-year disease-free survival (DFS) and overall survival (OS). The overall response rate in THP group was 83.3 %, and the EPI group showed a response rate of 79.2 %, with no statistically significant difference in response rate between the two groups. The incidence of cardiac toxicity, myelosuppression, nausea, and vomiting in the THP group was significantly lower than the EPI group (all P < 0.05). The incidence of hepatic toxicity, alopecia, and diarrhea in the THP group was also lower than the EPI group, but these differences were not statistically significant. The 5-year DFS and OS in THP versus EPI groups were 80 versus 76 % (DFS) and 86 versus 81 % (OS), respectively. Our study found that NACTwith DTC regimen and DEC regimen were both very effective in treatment of BC. However, THP-based combination therapy was associated with significantly lower incidence of cardiac toxicity, myelosuppression, nausea, and vomiting.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer (BC) is the most common type of noncutaneous malignancy and is the second leading cause of cancer-related death in women globally [1, 2]. BC is not restricted to the females, and BC in males account for 1 % of total BC incidence [3]. More than one million women are diagnosed with BC annually, and approximately 41 % of the newly diagnosed cases are between the ages of 40–50 years. Women over the age of 65 are more likely to suffer from BC. Approximately, 0,000 women died from BC in 2013 in USA alone, and 22,000 of these women were over the age of 65 [4]. The morbidity and mortality rates of BC are considerably different across various countries, with the highest rates found in Europe and North America, and lowest rates in Asia [5]. A variety of risk factors are associated with the susceptibility to BC, including age at first birth, age at menarche, sex, age at menopause, parity, and genetic mutations [6, 7]. Environmental factors such as changes in reproductive patterns, physical inactivity, and obesity also play a major role in BC incidence [8, 9]. With an aim of improving patient prognosis and survival in BC, newer techniques have been introduced, including full-field digital mammography (FFDM), digital breast tomosynthesis, and computer-aided tomography [10, 11]. The management of BC also depends on various factors, such as tumor stage, menopausal status, histological features, and patient age [12]. BC patients are typically treated with surgery (primary therapy), followed by radiotherapy, or chemotherapy (adjuvant therapy), and this protocol significantly decreases recurrence and death. More recently, chemotherapy before primary therapy (neoadjuvant therapy), followed by the primary therapy, has gained popularity, and several previous studies have reported the efficacy of neoadjuvant chemotherapies in BC [13–15].
Neoadjuvant chemotherapy (NACT) is a systemic chemotherapy before partial operation or radiotherapy of malignant tumors [16, 17]. NACT is a standard treatment for patients with inflammatory and locally advanced BC because it can improve surgery outcomes by shrinking tumors first [18]. NACT may increase the chance for breast conservation to allow real-time evaluation of treatment efficacy in vivo for further therapeutic intervention in BC patients [19, 20]. Existing NACT protocols often include docetaxel, anthracycline, cyclophosphamide, and trastuzumab, which are effective in treatment of BC [21]. Notably, anthracyclines, such as pirarubicin (THP) and epirubicin (EPI), are standard combinations in NACT regimen in BC [22]. THP and EPI treatment correlates with significantly elevated disease-free and overall survival in BC [23]. THP has improved antitumor activity and lower acute cardiotoxicity, with a response rate of 23.2 % in advanced BC [24]. EPI is one of the most frequently used chemotherapy agents in BC treatment because of its fewer side effects, e.g., lower cardiac toxicity than doxorubicin or mitoxantrone [22]. The efficacy of combination therapy is generally better than single-agent chemotherapy in many aspects, including higher overall survival in BC patients [25]. To date, multiple studies have investigated the clinical response and efficacy of THP and EPI combination regimens as adjuvant therapy in BC patients [22, 24, 26]. Few studies focused on THP or EPI in combination with docetaxel and cyclophosphamide in NACT setting for breast cancer treatment. In view of this, the present study examined the efficacy, toxicity, and tolerability of THP or EPI in combination with docetaxel and cyclophosphamide in the treatment of BC.
Materials and methods
Ethics statement
This study was performed with the approval of the Institutional Review Board of the Shengjing Hospital of China Medical University. All procedures were conducted according to the Declaration of Helsinki. Each eligible patient signed the informed consent prior to the study.
Patient population
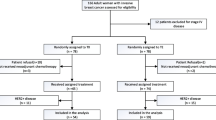
A total of 48 female patients, aged between 32 and 54 years (mean age: 46.2 years old), were recruited at the Breast Surgery Department in the Shengjing Hospital of China Medical University between January 2010 and December 2012. All patients included in this study met the following eligibility criteria: (1) patients were histological diagnosed as primary invasive breast cancer stage II–III via core needle biopsy before any treatment; (2) the absence of systemic disease measured by chest computed tomography scan, blood chemistry, abdominal ultrasound, and bone and computed tomography scans; (3) no previous treatment of chemotherapy or radiotherapy; (4) no history of other malignancies; (5) adequate hematologic function (hemoglobin >10 g/dL, neutrophil count >2.0 × 109/L and platelets >150 × 109/L); (6) adequate hepatic and renal function (serum total bilirubin, AST, and ALT levels of less than twice the normal upper limit, and a serum creatinine level less than 1.5 mg/dL); (7) normal ECG and adequate cardiac function with the left ventricular ejection fraction (LVEF) ≥60 %. Exclusion criteria were as follows: (1) older than 65 years old; (2) the maximum diameter of primary breast carcinoma less than 2 cm with axillary lymph node metastasis; or the maximum diameter of primary breast carcinoma over than 5 cm; (3) preoperative detection of chest wall and pectoral violations by chest ultrasonography; (4) obvious contraindication of chemotherapy; (5) previous history of breast operation, adjuvant chemotherapy, and radiotherapy. Clinical stage of the patients was based on the TNM staging classification of American Joint Committee on Cancer [27].
Treatment
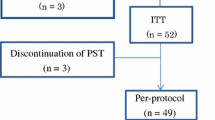
Forty-eight patients were randomized into two treatment groups with equal number of patients, THP group, and EPI group, and were given THP and EPI treatment, respectively. Baseline patient and tumor characteristics, including age, medical history, tumor stage and grade, nodal stage, estrogen receptor (ER), and progesterone receptor (PR) status, were not significantly different between the two groups. In the THP group (n = 24), patients received pirarubicin (50 mg/m2), docetaxel (75 mg/m2), and cyclophosphamide (500 mg/m2). In the EPI group (n = 24), patients received epirubicin (75 mg/m2), docetaxel (75 mg/m2), and cyclophosphamide (500 mg/m2). Both THP and EPI groups received 4 cycles by intravenous infusion every 21 days. Dexamethasone (8 mg) was given as routine premedication by intravenous push twice per day for 3 days prior to docetaxel administration. Prophylactic with granulocyte colony-stimulating factor (G-CSF) was required in case of febrile neutropenia (neutrophil count < 2.5 × 106/L). Patients were seen every two cycles during the treatment for physical examination, ultrasound, and assessment of status before surgery. Patients with complete remission or partial response after two cycles of chemotherapy received surgery. Patients were counseled to withdrawn from this study, change chemotherapy regimen, or undergo salvage surgery, if progressive disease was confirmed after two cycles or the disease was stable after four cycles of treatment.
Response and toxicity evaluation
Clinical and pathological response to neoadjuvant chemotherapy was assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST version 1.1) [28]. The response was assessed in 48 BC patients at the end of NACT for both THP and EPT. A clinical complete remission (CR) was judged when there was no evidence of residual tumor in the breast and axillary lymph nodes. A 30 % or greater reduction in tumor diameter was graded as a partial response (PR). An increase in tumor diameter of more than 20 % or appearance of new disease was considered as progressive disease (PD). Tumors that did not meet the criteria for objective PR or PD were considered as stable disease (SD). The absence of invasive tumor in the final histological breast and axillary lymph nodes specimens was defined as pathological CR (pCR). The patients with complete and partial pathological response (CR + PR) were considered as responders, while patients with static and progressive disease (SD and PD) were considered as nonresponders. The overall response rate (RR) of the THP and EPT combination therapies was defined as the total responders among the total patients in each group. Toxicity was assessed according to the National Cancer Institute Common Toxicity Criteria for Adverse Events version 4.0 (NCI-CTCAE) [29].
Follow-up
Kaplan-Meier estimates for prognosis of the study subjects were calculated based on the data obtained from the day of first hospitalization until death of the patient. Following the completion of the treatment regimen, patients were asked to return to the outpatient clinic for follow-ups. All patients were followed-up for survival every 3 months for 2 years, and thereafter, every 6 months until the death of the patient. Breast cancer risk was monitored each year of follow-up, using bilateral breast B ultrasound, breast X-ray, or MRI examination, liver B ultrasound, and chest CT examination. Prognostic evaluation indexes included5-year disease-free survival (DFS) and overall survival (OS).
Statistical analysis
Data were expressed as mean ± SD. Statistical analysis was performed using the SPSS software (version 18.0). Comparison of toxicity was calculated by using χ 2 test and Fisher’s exact test. Nonparametric Spearman's rank test was used to measure correlations. A P value of < 0.05 was adopted for significance.
Results
Efficacy
Clinical response to therapy was measured in all patients who finished the scheduled THP or EPI chemotherapy regimen for four cycles. In THP group, the RR was 83.3 % (20/24), with 4.2 % (1/24) showing complete response (CR), and 79.2 % (19/24) showing partial response (PR) (Table 1). In EPI group, the RR was 79.2 %, including CR and PR at 8.3 % (2/24) and 70.8 % (17/24), respectively. The results clearly showed that patients in THP group and EPI group displayed very similar clinical responses, and there was no statistically significant difference in the response rate between the two groups (all P > 0.05) (Table 1). Further, no statistically significant difference, in relation to pCR rate, was observed between the THP group and EPI group (both 4.2 %), which was postoperatively confirmed (all P > 0.05) (Table 1).
Safety
All 48 patients in THP or EPI groups were assessed for toxicity. Adverse events are summarized in Table 2. With respect to hematologic toxicity, 10 patients in THP group and 17 patients in EPI group developed grade I ~ II neutropenia, which was a statistically significant difference between the two groups (P = 0.042). In addition, grade III~IV neutropenia in THP group and EPI group were observed at 4 % (1/24) and 29 % (7/24), respectively (P = 0.048) (Table 2). Although nausea and vomiting (WHO grades III or IV) was more frequent with EPI therapy compared with THP therapy (75 versus 37.5 %; P = 0.009), grade I~II nausea and vomiting occurred more frequently in THP group compared to EPI group, at 62.5 % (15/24) and 25 % (6/24), respectively (P = 0.009) (Table 2). None of the patients experienced grade III~IV cardiac toxicity in both groups, however, grade I~II cardiac toxicity occurred at 4 % (1/24) in THP group and 29 % (7/24) in the EPI group (P = 0.048) (Table 2). In addition, none of the patients in both groups developed grade III~IV diarrhea and hepatic toxicity, with no significant differences in grade I~II diarrhea and hepatic toxicity between the two groups. The incidence of alopecia was also similar in both groups (P > 0.05).
Impact of THP and EPI chemotherapy on DFS and OS
All patients in both groups were followed-up until the death of the patient. The median follow-up of patients in THP group was 8.6 months, and the median time to progression (TTP) and median survival time (MST) were 8.3 months and 12.9 months, respectively. Further, EPI group patients were followed-up with a median follow-up of 9.5 months, and median TTP and MST were 9.5 months and 12.3 months, respectively. As shown in Fig. 1a-b, the 5-year DFS in THP and EPI groups were 80 % and 76 %, respectively. The 5-year OS was 86 % and 81 % in THP and EPI groups, respectively, and the OS was not significantly different between the two groups (all P > 0.05).

Impact of pirarubicin and epirubicin chemotherapy on the 5-year disease-free survival and overall survival. a The comparison of the 5-year disease-free survival rate between groups. b The comparison of the 5-year overall survival rate between groups
Discussion
NACT has been widely used in the clinical treatment of BC, especially for locally advanced breast cancer (LDBC) and inflammatory breast cancer (IBC) [30, 31]. NACT is also suitable for operable BC patients with larger sized tumors, axillary lymph node metastasis, or other recurrence and metastases [32]. NACT allows real-time assessment of early in vivo response to chemotherapy and provides the flexibility to choose the subsequent primary therapy in BC patients to improve therapy success [33]. In recent years, a variety of combination therapies have been introduced into clinics for BC treatment and have proven to be effective [34–36]. Previous clinical studies showed that anthracyclines, combined with paclitaxel chemotherapy drugs, displayed higher overall response rates compared with single-agent chemotherapy in BC treatment [37, 38]. Accordingly, docetaxel, combined with cyclophosphamide or anthracycline, is a first-line treatment in NACT. However, these combination therapies may also carry severe side effects [39, 40].
The primary objective of this current study was to assess the efficacy and safety of THP-based combination therapy and the EPI-based combination therapy in the treatment of BC patients. In our study, we found that the overall response rate in THP group was 83.3 %, and the overall response rate in EPI group was 79.2 %, with no significant differences between the two therapies. The results revealed that both THP-based combination therapy and EPI-based combination therapy were equally effective therapies for BC treatment, and both treatments relieved the symptom and improve the prognosis of BC in this patient cohort. THP is a derivate of doxorubicin (also known as Adriamycin, ADM), and THP shows higher antitumor activity in vivo and a significantly lower acute cardiac toxicity compared to ADM [41, 42]. On the other hand, EPI is an isomer of ADM, and its efficacy is similar to ADM in treating BC, but has lower cardiac toxicity compared to ADM [43, 44]. CPF regimen (THP, cyclophosphamide and 5-fluorouracil combination) and CEF regimen (EPI, cyclophosphamide and 5-fluorouracil combination) improved the prognosis in BC patients, and both are effective in adjuvant chemotherapy of BC [22]. Ying Li et al. showed that the 5-year survival rate of BC patients treated with FPC regimen (fluorouracil–pirarubicin-cyclophosphamide) was 88.7 %, and for BC patients treated with FEC regimen (fluorouracil–epirubicin–cyclophosphamide), the 5-year survival rate was 85.7 %. These result showed that THP and EPI are useful chemotherapy drugs for BC patients in various combinations [24]. Our results are consistent with previous studies and show that the overall response rates were excellent for both THP-based combination therapy and EPI-based combination therapy in treatment of BC and both chemotherapy regimens improved the outcomes in BC patients.
In this study, we found that the incidence of cardiac toxicity, myelosuppression, and nausea and vomiting in THP group were significantly lower than the EPI group. The incidence of nausea and vomiting in grades III or IV was more frequent in the EPI group compared to THP therapy, while the incidence of grade I~II nausea and vomiting occurred more frequently in the THP group compared to the EPI group. The observed grade I~II nausea and vomiting caused by the combination therapies were alleviated after completion of adjuvant therapy. Therefore, the results suggest that the toxicity of THP-based combination therapy is milder compared with EPI-based combination therapy. It is known that limiting or eliminating toxicity and side effects of chemotherapy drugs is crucial in cancer therapy [45–47], and a good tolerance to combination therapy is associated with better prognosis of BC patients [22, 34, 35]. BC patients treated with FPC and FEC regimens often suffer gastrointestinal toxicity and leucopenia, negatively influencing the prognosis of BC patients [24]. Zang MF et al., demonstrated that the incidence of gastrointestinal reactions in nausea and vomiting was significantly lower in the TAC group (pirarubicin in combination with docetaxel and cyclophosphamide) compared to TEC group (epirubicin in combination with docetaxel and cyclophosphamide) [48]. Thus, our results provide important information of drug combinations for NACT in BC, with the purpose of improving patient survival.
In summary, our results support the view that BC patients treated with the THP-based combination therapy or EPI-based combination therapy were associated with excellent overall response rates. Patients treated with THP-based combination therapy exhibited lower toxicity; therefore, the use of THP in chemotherapy drug combination is favorable based on our study results.
References
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300.
Assi HA, Khoury KE, Dbouk H, Khalil LE, Mouhieddine TH, et al. Epidemiology and prognosis of breast cancer in young women. J Thorac Dis. 2013;5:S2–8.
Germano S, O’Driscoll L. Breast cancer: understanding sensitivity and resistance to chemotherapy and targeted therapies to aid in personalised medicine. Curr Cancer Drug Targets. 2009;9(3):398–418.
Anders CK, Carey LA. Biology, metastatic patterns, and treatment of patients with triple-negative breast cancer. Clin Breast Cancer. 2009;9 Suppl 2:S73–81.
Tam C, Li Q, Friedenreich C, Martin LJ, Hislop G, Hanley AJ, et al. Lifetime physical activity in postmenopausal Caucasian and Chinese-Canadian women. Eur J Cancer Prev. 2014;23(2):90–5.
Nickels S, Truong T, Hein R, Stevens K, Buck K, et al. Evidence of gene-environment interactions between common breast cancer susceptibility loci and established environmental risk factors. PLoS Genet. 2013;9:e1003284.
Reeves GK, Pirie K, Green J, Bull D, Beral V, et al. Comparison of the effects of genetic and environmental risk factors on in situ and invasive ductal breast cancer. Int J Cancer. 2012;131:930–7.
Lee SA, Shu XO, Li H, Yang G, Cai H, et al. Adolescent and adult soy food intake and breast cancer risk: results from the Shanghai Women’s Health Study. Am J Clin Nutr. 2009;89:1920–6.
Lahart IM, Reichl C, Metsios GS, Nevill AM, Carmichael AR. Physical activity and awareness in breast screening attendees in Black Country, UK. Health Promot Int. 2014; doi:10.1093/heapro/dau053.
Waldherr C, Cerny P, Altermatt HJ, Berclaz G, Ciriolo M, et al. Value of one-view breast tomosynthesis versus two-view mammography in diagnostic workup of women with clinical signs and symptoms and in women recalled from screening. AJR Am J Roentgenol. 2013;200:226–31.
Azavedo E, Zackrisson S, Mejare I, Heibert Arnlind M. Is single reading with computer-aided detection (CAD) as good as double reading in mammography screening? A systematic review. BMC Med Imaging. 2012;12:22.
Campiglio M, Sandri M, Sasso M, Bianchi F, Balsari A, Menard S, et al. Prognostic role of tumor size in T1 HER2-positive breast cancers treated with adjuvant trastuzumab. Ann Oncol. 2014;25(5):1073–4.
Collins B, MacKenzie J, Tasca GA, Scherling C, Smith A. Cognitive effects of chemotherapy in breast cancer patients: a dose-response study. Psychooncology. 2013;22:1517–27.
Martin-Castillo B, Dorca J, Vazquez-Martin A, Oliveras-Ferraros C, Lopez-Bonet E, et al. Incorporating the antidiabetic drug metformin in HER2-positive breast cancer treated with neo-adjuvant chemotherapy and trastuzumab: an ongoing clinical-translational research experience at the Catalan Institute of Oncology. Ann Oncol. 2010;21:187–9.
Hurley J, Reis IM, Rodgers SE, Gomez-Fernandez C, Wright J, et al. The use of neoadjuvant platinum-based chemotherapy in locally advanced breast cancer that is triple negative: retrospective analysis of 144 patients. Breast Cancer Res Treat. 2013;138:783–94.
Byrski T, Gronwald J, Huzarski T, Grzybowska E, Budryk M, et al. Response to neo-adjuvant chemotherapy in women with BRCA1-positive breast cancers. Breast Cancer Res Treat. 2008;108:289–96.
Smith IC, Heys SD, Hutcheon AW, Miller ID, Payne S, et al. Neoadjuvant chemotherapy in breast cancer: significantly enhanced response with docetaxel. J Clin Oncol. 2002;20:1456–66.
Sanchez-Munoz A, Plata-Fernandez Y, Jaen A, Lomas M, Fernandez M, et al. Proliferation determined by ki67 marker and pCR in locally advanced breast cancer patients treated with neo-adjuvant chemotherapy. Breast J. 2013;19:685–6.
Guarneri V, Frassoldati A, Bottini A, Cagossi K, Bisagni G, et al. Preoperative chemotherapy plus trastuzumab, lapatinib, or both in human epidermal growth factor receptor 2-positive operable breast cancer: results of the randomized phase II CHER-LOB study. J Clin Oncol. 2012;30:1989–95.
Yamaguchi T, Mukai H. Ki-67 index guided selection of preoperative chemotherapy for HER2-positive breast cancer: a randomized phase II trial. Jpn J Clin Oncol. 2012;42:1211–4.
von Minckwitz G, Untch M, Nuesch E, Loibl S, Kaufmann M, et al. Impact of treatment characteristics on response of different breast cancer phenotypes: pooled analysis of the German neo-adjuvant chemotherapy trials. Breast Cancer Res Treat. 2011;125:145–56.
Li JJ, Di GH, Tang LC, Yu KD, Hu Z, et al. Adjuvant therapy of breast cancer with pirarubicin versus epirubicin in combination with cyclophosphamide and 5-fluorouracil. Breast J. 2011;17:657–60.
Gennari A, Sormani MP, Pronzato P, Puntoni M, Colozza M, et al. HER2 status and efficacy of adjuvant anthracyclines in early breast cancer: a pooled analysis of randomized trials. J Natl Cancer Inst. 2008;100:14–20.
Li Y, Tang JH, Huang XE, Li CG. Clinical comparison on the safety and efficacy of fluorouracil/pirarubicin/cyclophosphamide (FPC) with fluorouracil/epirubicin/cyclophosphamide (FEC) as postoperative adjuvant chemotherapy in breast cancer. Asian Pac J Cancer Prev. 2011;12:1795–8.
Chlebowski RT. Re: International guidelines for management of metastatic breast cancer: combination vs sequential single-agent chemotherapy. J Natl Cancer Inst. 2010;102:137.
Li JF, Ouyang T, Wang TF, Lin BY. Neoadjuvant chemotherapy for primary breast cancer. Chin J Oncol. 2004;26:493–5.
Singletary SE, Allred C, Ashley P, Bassett LW, Berry D, et al. Revision of the American joint committee on cancer staging system for breast cancer. J Clin Oncol. 2002;20:3628–36.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47.
Chen AP, Setser A, Anadkat MJ, Cotliar J, Olsen EA, et al. Grading dermatologic adverse events of cancer treatments: the common terminology criteria for adverse events version 4.0. J Am Acad Dermatol. 2012;67:1025–39.
Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13:25–32.
Gianni L, Eiermann W, Semiglazov V, Manikhas A, Lluch A, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010;375:377–84.
Rousseau C, Devillers A, Campone M, Campion L, Ferrer L, et al. FDG PET evaluation of early axillary lymph node response to neoadjuvant chemotherapy in stage II and III breast cancer patients. Eur J Nucl Med Mol Imaging. 2011;38:1029–36.
Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, et al. Preoperative chemotherapy: updates of national surgical adjuvant breast and bowel project protocols B-18 and B-27. J Clin Oncol. 2008;26:778–85.
Baselga J, Cortes J, Kim SB, Im SA, Hegg R, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med. 2012;366:109–19.
Swain SM, Ewer MS, Cortes J, Amadori D, Miles D, et al. Cardiac tolerability of pertuzumab plus trastuzumab plus docetaxel in patients with HER2-positive metastatic breast cancer in CLEOPATRA: a randomized, double-blind, placebo-controlled phase III study. Oncologist. 2013;18:257–64.
Mehta RS, Barlow WE, Albain KS, Vandenberg TA, Dakhil SR, et al. Combination anastrozole and fulvestrant in metastatic breast cancer. N Engl J Med. 2012;367:435–44.
Dear RF, McGeechan K, Jenkins MC, Barratt A, Tattersall MH, et al. Combination versus sequential single agent chemotherapy for metastatic breast cancer. Cochrane Database Syst Rev. 2013;12, CD008792.
Carrick S, Parker S, Thornton CE, Ghersi D, Simes J, et al. Single agent versus combination chemotherapy for metastatic breast cancer. Cochrane Database Syst Rev. 2009. CD003372.
Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, et al. Adjuvant capecitabine in combination with docetaxel and cyclophosphamide plus epirubicin for breast cancer: an open-label, randomised controlled trial. Lancet Oncol. 2009;10:1145–51.
Piccart-Gebhart MJ, Burzykowski T, Buyse M, Sledge G, Carmichael J, et al. Taxanes alone or in combination with anthracyclines as first-line therapy of patients with metastatic breast cancer. J Clin Oncol. 2008;26:1980–6.
Wang LZ, Ouyang T, Wang TF, Xie YT, Fan ZQ, et al. Efficacy analysis of THP-containing regimens as neoadjuvant and adjuvant chemotherapy for primary breast cancer. Chin J Oncol. 2012;34:143–6.
van Dalen EC, Michiels EM, Caron HN, Kremer LC. Different anthracycline derivates for reducing cardiotoxicity in cancer patients. Cochrane Database Syst Rev. 2010. CD005006.
Untch M, von Minckwitz G, Konecny GE, Conrad U, Fett W, et al. PREPARE trial: a randomized phase III trial comparing preoperative, dose-dense, dose-intensified chemotherapy with epirubicin, paclitaxel, and CMF versus a standard-dosed epirubicin-cyclophosphamide followed by paclitaxel with or without darbepoetin alfa in primary breast cancer-outcome on prognosi. Ann Oncol. 2011;22:1999–2006.
Joensuu H, Kellokumpu-Lehtinen PL, Huovinen R, Jukkola-Vuorinen A, Tanner M, et al. Adjuvant capecitabine, docetaxel, cyclophosphamide, and epirubicin for early breast cancer: final analysis of the randomized FinXX trial. J Clin Oncol. 2012;30:11–8.
Sioka C, Kyritsis AP. Central and peripheral nervous system toxicity of common chemotherapeutic agents. Cancer Chemother Pharmacol. 2009;63:761–7.
Hurria A, Togawa K, Mohile SG, Owusu C, Klepin HD, et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J Clin Oncol. 2011;29:3457–65.
Azim Jr HA, de Azambuja E, Colozza M, Bines J, Piccart MJ. Long-term toxic effects of adjuvant chemotherapy in breast cancer. Ann Oncol. 2011;22:1939–47.
Zang MF, Zhang YM, Zhi YH, Zhai Z, Zhang M, et al. Comparative study of chemosensitivity and efficacy between pirarubicin and epirubicin in breast cancer. Nat Med J China. 2011;91:1388–92.
Acknowledgments
This study was supported by the Science and Technology Research Project of Liaoning Province (No. 2012225016). We would like to acknowledge the reviewers for their helpful comments on this paper.
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Gu, X., Jia, S., Wei, W. et al. Neoadjuvant chemotherapy of breast cancer with pirarubicin versus epirubicin in combination with cyclophosphamide and docetaxel. Tumor Biol. 36, 5529–5535 (2015). https://doi.org/10.1007/s13277-015-3221-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-3221-9