
Abstract
Background
Carcinoma in the cervix is the most common malignancy and the fourth most common cause of death in females worldwide. It is the most common malignancy in India, the increasing incidence of cancer is escalating burden over radiation. This is a prospective randomized study comparing NACT followed by definitive chemoradiation versus chemoradiation.
Materials and Methods
This prospective randomized study analyzed 80 cervical cancer patients who were treated at our center during March 2017 and July 2018. Patients were divided into two arms: one received NACT and definitive CT/T and the other received definitive CT/RT. Statistical analysis was done using SPSS V.20 software.
Results
Overall response rate in our study was found to be 96.2%. In the study group, it was 97.5%, whereas in the control group, it was 95%. Majority of patients were in the age group 41–50 years, mainly stage IIb and IIIb. Tumor response in both the arms was similar and statistically significant (Chi2 = 0.348; p > 0.05). The hematologic toxicities ( p > 0.05) were more in the NACT group than in the CCRT group, while gastrointestinal toxicities were slightly higher in the control (statistically insignificant).
Conclusion
NACT with taxane/platin followed by definitive CT/RT is as effective as the standard care in the treatment of locally advanced cervical cancer. It has even shown better results (p value > .005) and is also helpful in reducing systemic micrometastasis and bulk of the disease. It can be used as an alternative to the standard care at the places of long waiting time for the definitive treatment, without compromising the outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cervical cancer is the fourth most commonly diagnosed cancer. Worldwide, cervical cancer remains the most common gynecologic cancer and the third most common malignancy in women, with over 500,000 women globally developing this tumor and 233,000 dying of the disease every year [1].
Carcinoma of uterine cervix is the most common malignancy seen in Indian females with the peak age 45–54 years [1]. Indian women face a 2.5% cumulative lifetime risk and 1.4% cumulative death risk from cervical cancer [2, 3].
Carcinoma cervix accounted for approximately 30% of all cases in our rural-based medical college hospital, with monthly registration of new cases of cancer cervix on an average of 50 in numbers; about 80% suffer from carcinoma cervix with locally advanced disease (FIGO stages IIB, III and IV) in which surgery has higher morbidity [4, 5].
Currently, the two main modalities of radiation are external beam radiotherapy and brachytherapy [6, 7].
Due to long waiting period for availibility radiotherapy machines, giving neoadjuvant chemotherapy is the only available option [8].
With the intent to arrest the disease progression, to increase radiosensitivity complete response, to prevent the distal metastasis and to improve disease-free survival (DFS), we advocate neoadjuvant chemotherapy with paclitaxel and cisplatin immediately after histopathological confirmation and base-line investigation. Paclitaxel in combination with cisplatin showed remarkable activity against cervical cancer, use of neoadjuvant chemotherapy was not only associated with better tumor response but also less number of systemic relapses [9, 10].
In this study, we evaluated the response of neoadjuvant chemotherapy (NACT) in locally advanced cervical cancer in terms of complete response of disease, arrest the disease progression, improve the disease-free interval and prevention of micrometastasis.
Aims and Objective
-
To evaluate effects and side effects of NACT in locally advanced carcinoma of the cervix in Indian patients.
-
To evaluate the effects and side effects of chemoradiotherapy in locally advanced carcinoma of the cervix in Indian patients.
-
To clinically evaluate tumor response and locoregional control weekly during treatment and subsequent follow-up till 6 months.
Materials and Methods
After taking permission from institutional ethical committee 80 histopathologically confirmed newly diagnosed cases of squamous cell carcinoma cervix stage IIA to IIIB were included. These cases were registered, for treatment in the Department of Radiotherapy at N.S.C.B.M.C., from March 2017 to July 2018. Informed consent was obtained, and patients were randomized into two arms. All statistical calculations were done with SPSS Statistics version 20.0.
Inclusion criteria were as follows: (1) measurable disease; (2) age 18–69 years; (3) Karnofsky performance status of at least 70; (4) ECOG performance status 0–1–2; (5) normal hematological, renal and hepatic function as follows: hematological, Hb ≥ 10 g/l (however, patients could be transfused before any treatment to reach this level of hemoglobin); leukocytes > 4000/mm3; platelets > 100,000/mm3; total bilirubin; and transaminases < 1.5 × upper limit of normal and normal creatinine; (6) a normal chest X-ray; and (7) informed consent.
Exclusion criteria were as follows: (1) hypersensitivity to cisplatin or paclitaxel; (2) stages IA, IB1 and IV; (3) distant metastasis; (4) prior radiotherapy; (5) prior chemotherapy; (6) pregnant or nursing women; (7) mental illness; and (8) previous or concomitant malignancy.
Consort diagram


Neoadjuvant Chemotherapy
Newly diagnosed biopsy-proven cases of stage II/III cervical cancers were randomized into two arms (case and control).
Case arm received two cycles of neoadjuvant chemotherapy with each cycle three weeks apart, consisting of the injection paclitaxel in a dose of 175 mg/m2 i/v and injection cisplatin 75 mg/m2 i/v followed by definitive chemoradiotherapy after checking complete blood count, liver function test, renal function test.
Neoadjuvant chemotherapy was not administered in control arm.
Common Protocol for Both the (Case/Control) Arms
Protocol for definitive CT/RT—both arms received definitive CT/RT 50 Gy/25# 2 Gy per fraction, 5 days a week with concurrent cisplatin. Followed by ICRT 3, fraction of weekly ICRT was given at the dose of 700 cGy × 3 # at point A by using HDR brachytherapy. Total duration of completion of treatment with EBRT and ICRT was 56 days.
The result of the study group was analyzed and compared with the control group in terms of various aspects like side effects, drug toxicity profile, tumor response, and local disease status.
Statistical Methodology
Data thus collected was fed into the computers and after its proper validation, checked for error, coding and decoding compiled and analyzed with the help of SPSS 20 software for windows. Appropriate univariate, bivariate analysis and ANOVA for comparing more than two means were carried out, and use of Student’s t test and Chi-square test for categorical data was applied to check the hypothesis according to the type of data, i.e., continuous and categorical. The VAS scores in two groups were analyzed using a nonparametric test, namely Mann–Whitney U test.
All means are expressed as mean ± standard deviation and the proportion as in percentage (%). The critical value for the significance of the results was considered at 0.05 level.
Sample Size
Assuming a 30% difference in the proportion of patients with the presence of complications as clinically important in studied groups, we calculated that 30 patients would be required in each group to achieve 80% power at the 5% significance level to detect a true difference among the groups. The sample size was calculated using statistical software Epi info 2000 (CDC Atlanta, USA). Data was presented as mean ± SD, medians and ranges, or numbers and percentages of patients.
Forty patients in each arm were able to qualify the required norm.
Design of Study
This is a prospective randomized case control trial study.
Evaluation After Completion of Treatment and Follow-Up
Patients were evaluated at the end of treatment and 1-, 3- and 6-month follow-up, by clinical examination and pathological and radiological investigation. Response was evaluated in terms of stable disease (SD), partial response (PR), progressive disease (PD) or complete response (CR).
Observation and Results
A total of 40 patients in NACT arm (case) and 40 patients in CRT arm (control) were analyzed. The clinico-pathological characteristics were well balanced, and there were no major differences in age distributions, body weight, body surface area (BSA), body mass index (BMI), performance status, hemoglobin level, serum creatinine, serum urea and treatment duration. Patients of well-differentiated carcinomas were equal in percentage in both arms while percentages of poorly differentiated carcinomas were more in the study arm (Table 1).
At the end of treatment, 34 patients (85.0%) of the study group and 33 patients (82.5%) of the control group had complete response. Five patients (12.5%) in the study group as well as control had partial response. One patient (2.5%) in the study group and 2 patients (5%) in the control had stable disease as shown in Table 2 Weekly response assessment is summarized in Table 3. One case in the study group and 2 cases in the control group show stable disease, and they could not complete the brachytherapy course due to vaginal stenosis and involvement of the parametrium [1, 11, 12].
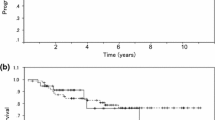
However, this difference was not found statistically significant. χ2 = 0.348; p > 0.05. During 1-month, 2-month and 3-month follow-up period, none of the patient in the study and control group developed metastasis.
Non-Hematological Toxicity
Nineteen patients (47.5%) in the study group and 21 patients (52.5%) in the control group had grade 1 skin reactions. Fourteen patients (35%) in the study group and 14 (35%) patients in control had grade 2 skin reaction. Five patients (12.5%) in the control group and 3 (7.5%) patients in the study group had grade 3 nausea. Four patients (10%) had grade 3 vomiting in the control group, and 3 patients (7.5%) in the study group had grade 3 vomiting. Grade 3 diarrhea was seen in 1 (2.5%) and 3 (7.5%) patients in the case and control, respectively. Grade 4 toxicity was seen in 1 (2.5%) patient in control groups (Table 4).
Hematological Toxicity
Grade 3 anemia was seen in 5 patients (12.5%) in the study group; no incidence of grade 3/4 anemia was seen in the control group (Table 4). The study group had more patients with grade 2 leucopenia 11 (27.5%) as compared to the control group (5%). Grade 3 toxicity was seen in 5 patients (12.5%) in the study group only. The study group had more patients with grade 1 and grade 2 neutropenia 11 (27.5%) and 15 (37.5%) as compared to the control group 15 (3.5%) and 5 (12.5%). Grade 3/4 toxicity was not seen in any patients in the study and control group.
Discussion
Concurrent chemoradiation is “standard of care” for women with locally advanced carcinoma cervix. This was in response to a National Cancer Institute Alert based on results of five randomized trials stating “strong consideration should be given to the incorporation of chemotherapy and radiotherapy for the treatment of cervical cancer” [1]. Our institute and almost all institutes are overburdened with cases of cervical cancer, and most patients report at advanced stages. Due to long waiting period for the availability of radiotherapy machines, often giving prior chemotherapy is the only available option [5].
Most of the patients belong to rural background and suffer from locally advanced cervical cancer. The rationales for the use of neoadjuvant chemotherapy (NACT) are multiple [13]. In this study, we compared toxicity, compliance and response of neoadjuvant chemotherapy followed by definitive chemotherapy versus definitive chemoradiotherapy. In our study, the mean age of cases in the study arm was 46.85 ± 8.45 years, and in the control arm, the mean age was 47.13 ± 10.28 years. The ECOG performance status of the patients (75%) in the studied population was 1. It was seen in our study that 58.8% of cases registered in either of the arms belonged to lower socioeconomic status [4, 11]. Almost 68.8% of the cases enrolled in the study were from rural area. This might be due to the fact that there is increased incidence of cervical cancer in lower strata of the society due to unhygienic health conditions and possible HPV infections or other sexually transmitted diseases which might possibly act as an etiological agent.
A study conducted by Cho et al. [14] found 94% ORR after giving neoadjuvant chemotherapy. We also found ORR 97.5% and 95%, in study and control arm, respectively.
At the end of the completion of treatment, 85% patients in the study group and 82.5% patients in the control group were found to have complete response to the treatment (χ2 = 0.348, p value > 0.05); 12.5% were found to have partial response in both the study and control group (p value is insignificant). Same results were found in the study conducted by Fotedar et al. [15] consisting of 113 patients which had 3-year follow-up. Clinical CR and PR were seen in 64% and 15% in study arm, respectively, and 66% and 14% in control arm, respectively; p value was insignificant. This study had more patients than our study and had 3-year follow-up, and this strengthens the fact that NACT followed by CT/RT has similar results to CT/RT alone. In fact, results are slightly more beneficial though statistically insignificant.
McCormack et al. investigated the feasibility of NACT with taxane/platin before radical chemoradiation (CRT) and assessed the response rate. They also concluded that treatment regimen is feasible as evidenced by the acceptable toxicity of NACT and by the high compliance to radiotherapy [16].
Saha et al. [13] reviewed available studies, and with the help of 3-year experience, they concluded that NACT is feasible and produces impressive responses in cervical carcinoma.
Katke et al. performed a prospective analytical study of 95 patients with locally advanced carcinoma of cervix in a tertiary care setup in India. Study has demonstrated a good response rate to NACT followed by CRT in patients with locally advanced carcinoma of the cervix with regard to tumor response, overall response and disease-free survival [17].
In this study there was no statistically significant toxicity between the study group and control group for acute skin reaction (χ2 = 0.433, p value > 0.05). The statistically significant toxicity was found in control group for nausea (χ2 = 8.612, p value 0.01). Vomiting (χ2 = 3.344, p value > 0.05), Diarrhea (χ2 = 3.329, p value > 0.05), and Nephrotoxicity (χ2 = 5.292, p value > 0.05), were seen slightly higher but not statistically significant in control group whereas haematological toxicity was seen slightly higher in study group, result was not statistically significant. Same result were also seen in study conducted by Duenas-Gonzalez et al, Mori et al. [18, 19].
Conclusion
We finally conclude that in developing countries like us facing escalating burden of malignancy, where resources are less and institute providing radiation treatment is limited, considering the sufferings of rural cancer patients and impact of delay in the initiation of radiation therapy in the course of the disease, we suggest trying NACT in all locally advanced cases of cancer cervix to arrest the progress of disease for quite a reasonable period without additive toxicity and compromising the outcome.
Larger prospective studies with longer follow-up are required to establish it as standard of care.
Abbreviations
- NACT:
-
Neoadjuvant chemotherapy
- LACCx:
-
Locally advanced cancer cervix
- T/P:
-
Taxane/platin
- DFS:
-
Disease-free survival
References
Vishwanathan A, Halperin EC, Wazer DE, et al. Principles and practice of radiation oncology. In: Halperin EC, editor. Perez and Brady’s Principles and practice of radiation oncology. 6th ed. Philadelphia: Wolters Kluwer Health; 1934.
Pecorelli S, Zigliani L, Odicino F. Revised FIGO staging for carcinoma of the cervix. Int J Gynecol Obstet. 2009;145:129–35.
Human Papillomavirus (HPV) Vaccines: Q & A. Fact sheets: risk factors and possible causes. National Cancer Institute (NCI). 2009. pp. 10–22. Retrieved 2009-11-11.
Bruni L, Barrionuevo-Rosas L, Albero G, et al. ICO Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in [Botswana]. Summary Report. 2014.
Narayan S, Sharma N, Kapoor A, et al. Pros and cons of adding of neoadjuvant chemotherapy to standard concurrent chemoradiotherapy in cervical cancer: a regional cancer center experience. J Obstet Gynecol India. 2016;66:385–90.
Eifel PJ, Morris M, Taylor Wharton J, et al. The influence of tumor size and morphology on the outcome of patients with figo stage IB squamous cell carcinoma of the uterine cervix. Int J Radiat Oncol. 1994;29:9–16.
Rotman M, Pajak TF, Choi K, et al. Prophylactic extended-field irradiation of para-aortic lymph nodes in stages IIB and bulky IB and IIA cervical carcinomas. Ten-year treatment results of RTOG 79-20. JAMA. 1995;274:387–893.
Woo YJ, Byun JM, Jeong D. Prognosis of stage IIb cervical cancer among treatment regimens: radical hysterectomy versus neoadjuvant chemotherapy followed by radical hysterectomy versus concurrent chemoradiotherapy. KJOG. 2012;55:913–9.
Dastidar G, Gupta P, Basu B, et al. Is neo-adjuvant chemotherapy a better option for management of cervical cancer patients of rural India? Indian J Cancer. 2016;53:56.
Tattersall MH, Ramirez C, Coppleson M. A randomized trial of adjuvant chemotherapy after radical hysterectomy in stage Ib-IIa cervical cancer patients with pelvic lymph node metastases. Gynecol Oncol. 1992;46:176–81.
Rath GK, Mohanti BK, editors. Textbook of radiation oncology: principles and practice. New Delhi: BI Churchill Livingstone, 2000 (ISBN 81-7042-166-7); Elsevier, 2003 (Reprint).
Erickson B, Eifel P, Moughan J, et al. Patterns of brachytherapy practice for patients with carcinoma of the cervix (1996–1999): a patterns of care study. Int J Radiat Oncol Biol Phys. 2005;63:1083–92.
Saha A, Mukherjee A. Role of neoadjuvant chemotherapy in cancer cervix: a brief review. Clin Cancer Investig J. 2013;2:281.
Cho YH, Kim DY, Kim JH, et al. Comparative study of neoadjuvant chemotherapy before radical hysterectomy and radical surgery alone in stage IB2-IIA bulky cervical cancer. J Gynecol Oncol. 2009;20:22–7.
Fotedar V, Seam RK, Gupta MK, et al. Neoadjuvant chemotherapy followed by radiotherapy versus radiotherapy alone in locally advanced carcinoma cervix: a prospective randomized study. IOSR J Dent Med Sci. 2013;4(6):58–63.
McCormack M, Kadalayil L, Hackshaw A, et al. A phase II study of weekly neoadjuvant chemotherapy followed by radical chemoradiation for locally advanced cervical cancer. Br J Cancer. 2013;108:2464–9.
Katke RD, Shivhar RM, Pagare P. Role of neoadjuvant chemotherapy and radiotherapy in locally advanced carcinoma of the cervix. Clin Cancer Investig J. 2016;5:365.
Mori T, Hosokawa K, Sawada M, et al. Neoadjuvant weekly carboplatin and paclitaxel followed by radical hysterectomy for locally advanced cervical cancer long-term results. Int J Gynecol Cancer. 2010;20:611–6.
Duenas-Gonzalez A. A phase II study of multimodality treatment for locally advanced cervical cancer: neoadjuvant carboplatin and paclitaxel followed by radical hysterectomy and adjuvant cisplatin chemoradiation. Ann Oncol. 2003;14:1278–84.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Statement
The author and coauthors declare that this is an original article and has none of the following ethical issues. The manuscript has not been submitted to more than one journal for simultaneous consideration. The manuscript has not been published previously (partly or in full), unless the new work concerns an expansion of previous work. A single study is not split up into several parts to increase the quantity of submissions and submitted to various journals or to one journal over time (e.g., “salami-publishing”). No data have been fabricated or manipulated (including images) to support our conclusions. No data, text, or theories by others are presented as if they were the author’s own (“plagiarism”). Consent to submit has been received explicitly from all coauthors, as well as from the responsible authorities—tacitly or explicitly—at the institute/organization where the work has been carried out, before the work is submitted. Authors have contributed sufficiently to the scientific work and therefore share collective responsibility and accountability for the results.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dr. Aradhna Tripathi, PG 3rd year, MD (radiation oncology), at Govt. Cancer Hospital, NSCBMC Jabalpur (Madhya Paradesh). Dr. Shyamji Rawat MD (radiotherapy) is a Professor in the Department of Radiotherapy and Oncology at Govt. Cancer Hospital NSCBMC Jabalpur (Madhya Pradesh).
Rights and permissions
About this article

Cite this article
Tripathi, A., Rawat, S. Comparative Study of Neoadjuvant Chemotherapy Followed by Definitive Chemoradiotherapy Versus Definitive Chemoradiotherapy Alone in Locally Advanced Carcinoma of Cervix. J Obstet Gynecol India 69, 546–552 (2019). https://doi.org/10.1007/s13224-019-01236-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-019-01236-0