
Abstract
Malignant schwannoma, also called malignant peripheral nerve sheath tumor (MPNST), is a rare and aggressive tumor arising from the nerve sheath. We describe a rare case of endotracheal malignant peripheral nerve sheath tumor occurring in a middle-aged male who presented with asthma-like symptoms for 6 months with progressively increasing dyspnea. A computed tomogram (CT) scan of the thorax revealed near complete luminal obstruction of the trachea by a mass lesion at the level of the second and third tracheal rings. Microlaryngotracheoscopy revealed a fleshy pedunculated growth arising from the left side of the second and third tracheal rings and obliterating almost the entire tracheal lumen. Intraluminal complete excision of the mass was done. Later, he underwent excision of the 2nd and 3rd rings after the histopathology revealed MPNST. Patient after 28 months of follow-up is free of disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary malignancy tracheal tumors are rare. The most common primary malignant tracheal tumors are squamous cell carcinoma and adenoid cystic carcinoma [1]. Tracheal tumors present with airway obstruction. Malignant peripheral nerve sheath tumor (MPNST) is a malignant neoplasm arising from the peripheral nerve sheath and commonly seen in extremities. Surgery remains the primary modality of treatment for the MPNST. The present case is a very rare presentation of the malignant peripheral nerve sheath tumor arising primarily from the trachea. Primary MPNST of the trachea has not been described in literature but secondary tracheal involvement from MPNST arising from the thoracic vagus nerve has been reported [2].
Case Report
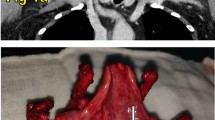
A 33-year-old male patient, non-smoker, presented with increasing breathlessness of 2 weeks duration. He was in stridor at presentation to the hospital. He gave his history of treatment for bronchial asthma for the last 6 months. To rule out any thoracic pathology, an emergency computed tomogram (CT) scan of the thorax was done which revealed near complete luminal obstruction of the trachea by a mass lesion at the level of the second and third tracheal rings (Fig. 1). The thoracic cage, lungs, other viscera, and neck were normal. Emergency tracheotomy was performed for acute airway obstruction and patient was stabilized. Microlaryngotracheoscopy was performed which revealed a fleshy pedunculated growth arising from the left side of the second and third tracheal rings and obliterating almost the entire tracheal lumen. Intraluminal complete excision of the mass was done with combination of laser and cold knife (Fig. 1). Patient was decannulated from tracheotomy after 2 days.

(1 and 2) Plain CT scan suggestive of near complete tracheal luminal obstruction by a mass lesion at the level of the second and third tracheal rings. (3) Microlaryngotracheoscopy showing a fleshy pedunculated growth. (4) Four weeks post operative bronchoscopy showing perfectly healed trachea
Microscopic examination revealed respiratory epithelium with foci of squamous metaplasia and underlying diffuse proliferation of spindle cells admixed with multiple ectatic prominent vascular channels. The cells were spindle shaped with elongated vesicular nuclei. Few cells showed wavy nuclei and exhibited pleomorphism. Mitoses and necrosis were noted. Tumor demonstrated positivity for S-100 and vimentin but was negative for pancytokeratin, SMA, CD34, calcitonin, and calponin (Fig. 2). Histopathology in correlation with immunohistochemistry studies was reported as spindle cell sarcoma with features suggestive of malignant peripheral nerve sheath tumor (MPNST).

(1) H&E × 40: Infiltrating spindle cell lesion arranged in bundles in the subepithelium. (2) H&E × 400: Spindle-shaped cells exhibiting marked pleomorphism. (3) Vimentin, IHC-Positive in tumor cells. (4) S100, IHC: Diffuse positivity in the tumor cells. (5) Pancytokeratin, IHC: Negative in tumor cells. (6) Calponin, IHC: Negative in tumor cells
A relook for neurofibromatosis was done. He did not have any stigmata of Von Recklinghausen’s disease. He denied any family history. Since the resected mass turned out to be MPNST, open sleeve tracheal re-resection of the second and third rings was done for wide margins and the resultant defect closed primarily. The re-resected specimen was free of tumor in the final histopathology report. The case was discussed in multidisciplinary tumor board meeting and was decided to keep under follow-up with regular bronchoscopy. Patient after 32 months of follow-up is free of disease.
Discussion
Tracheal neoplasms occur infrequently, accounting for less than 1% of all malignancies [3]. As per the Surveillance, Epidemiology and End Results (SEER) 1973–2004 database, primary carcinomas of the trachea occurred at a rate of 2.6 new cases per million people per year. Five hundred seventy-eight (578) cases of primary tracheal carcinomas were reported, of which 322 patients were men (55.7%) and 256 women (44.3%). Squamous cell carcinoma was the most common histology, constituting 259 tumors (44.8%). Adenoid cystic carcinoma (ACC) was the next common malignant histology (16.3%) [1]. A retrospective analysis of uncommon tracheal tumors among 360 primary tracheal tumors excluding adenoid cystic and squamous cell carcinoma presenting over 40 years was done by Gaissert et al. [4]. Ninety documented rare cases were reported. Thirty-four patients (38%) had benign tumors and 56 malignant. Eleven had carcinoid tumors, 14 mucoepidermoid carcinomas, 13 sarcomas, 15 nonsquamous bronchogenic carcinomas, 2 lymphomas, and 1 melanoma [4]. Three patients had a second tracheal malignancy. Nerve sheath tumors include neurofibroma, schwanomma, and malignant peripheral nerve sheath tumor. These tumors commonly occur in the mediastinum especially in the posterior compartment. They may cause a pressure effect on the mediastinal structures including the trachea. Neurofibroma and schwannoma present infrequently as endotracheal tumors [2].
Hakim et al. has described a rare case of endobronchial malignant peripheral nerve sheath tumor treated by pneumonectomy and tracheoplasty [5]. To the best of our knowledge, no cases of malignant peripheral nerve sheath tumor arising primarily in the trachea either solitary or as a part of Von Recklinghausen’s neurofibromatosis has been reported in literature till to date but secondary tracheal involvement by the tumor probably arising from the vagus nerve has been described [2, 6]. Our case is the first documented case of primary MPNST arising from the trachea occurring solitarily without any history of Von Recklinghausen’s disease.
In a series of 329 patients with primary tracheal malignancies, dyspnea was the most frequent symptom (71%), followed by cough (40%), hemoptysis (34%), asthma (19.5%), and stridor (17.5%) [7]. The first symptom may be shortness of breath after activity, which gradually worsens. Acute respiratory difficulty may not be present until the airway is almost completely occluded, which explains why it may be rapidly fatal. A persistent cough, wheezing, or stridor may be noted, as may recurrent attacks of respiratory obstruction caused by secretions [3].
The present case presented with asthma-like symptoms from 6 months with progressively increasing shortness of breath for 2 weeks and stridor on admission to hospital.
Surgical resection is the mode of treatment with the best hope for cure. Radiotherapy can be offered if the patient cannot tolerate surgical treatment. Chemotherapy can also be given after initial treatment with surgery, radiotherapy, or both. Laser removal of the intratracheal tumor is usually performed for palliation [3]. In the present case, we did intraluminal complete excision of the mass with combination of laser and cold knife and re-excision of the second and third tracheal rings after histopathology of resected tracheal lesion specimen revealed MPNST. The patient is kept on close observation with regular bronchoscopy after discussing in multidisciplinary tumor board meeting. Patient after 28 months of follow-up is free of disease. R0 excision is the most important prognostic factor in management of this malignancy which could not be achieved most of the times resulting in poor prognosis. .
Median survival for all patients after diagnosis of malignant tracheal tumors is 6 months, but varies widely, depending on the histology of the tumor [3]. In a series of 578 cases of primary tracheal carcinomas, localized, regional, and distant disease were found in 140 (24.2%), 212 (36.7%), and 108 (18.7%), respectively. General overall 5-year survival for all patients was 27.1%. Patients with localized disease had a better outcome with an overall 5-year survival of 46%. Squamous cell carcinoma tumors had worse outcomes than any other histologic type, with a 5-year overall survival of 12.6%. In contrast, a 5-year overall survival for adenoid cystic carcinomas was relatively good at 74.3% [1]. In this series, 34.3% did not undergo surgery and 29.1% did not receive any kind of radiation therapy contributing to poor prognosis [1]. In a series of 90 primary tracheal tumors (38 benign and 56 malignant cases) post resection, survival at 10 years was 94% for benign and 83% for carcinoid tumors, and at 5 years survival was 60% for bronchogenic carcinoma, 100% for mucoepidermoid tumors, and 78% for sarcomas [4]. Two-year and 5-year survival rates in intrathoracic MPNST were 35% and 16%, and median survival was 8.5 months [8]. The present case had only local tracheal disease.
References
Urdaneta AI, Yu JB, Wilson LD (2011) Population based cancer registry of primary tracheal carcinoma. Am J Clin Oncol 34(1):32–37
Javad B, Beheste J, Mark EJ (2004) Mesenchymal tumours of trachea In: Grillo HC (ed) Surgery of trachea and bronchi, 1st edn. BC Decker Inc., Ontario, p 86–97
Daley B (2015) Tracheal tumors: background, anatomy, pathophysiology. [online] Emedicine.medscape.com. Available at: https://emedicine.medscape.com/article/425904-overview. Accessed 10 Aug 2017
Gaissert HA, Grillo HC, Shadmehr MB, Wright CD, Gokhale M, Wain JC, Mathisen DJ (2006) Uncommon primary tracheal tumors. Ann Thorac Surg 82(1):268–272
Hakkim FA, Kirthana G, Krishnapriya SR, Muthurangan G (2015) A rare case of endobronchial malignant peripheral nerve sheath tumor. National Journal of Medical Research & Yoga Science (NJMEYS) 1(2):30–32
Fukai I, Masaoka A, Yamakawa Y, Niwa H, Eimoto T (1995) Mediastinal malignant epithelioid schwannoma. Chest. 108(2):574–575
Velez Jo ET, Morehead RS (1999) Hemoptysis and dyspnea in a 67-year-old man with a normal chest radiograph. Chest. 116(3):803–807
Kourea HP, Bilsky MH, Leung DH, Lewis JJ, Woodruff JM (1998) Subdiaphragmatic and intrathoracic paraspinal malignant peripheral nerve sheath tumors: a clinicopathologic study of 25 patients and 26 tumors. Cancer. 82(11):2191–2203
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nemade, H., Nusrath, S., Y, J. et al. Primary Malignant Peripheral Nerve Sheath Tumor of the Trachea: a Case Report with Brief Review of Literature. Indian J Surg Oncol 10, 392–395 (2019). https://doi.org/10.1007/s13193-019-00907-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-019-00907-8