
Abstract
In 2006, St. Jude Children’s Research Hospital (Memphis, Tennessee) began developing a school-based outreach program known as the St. Jude Cancer Education for Children Program (SJCECP). The aim of this program is to teach Memphis-area children about cells, cancer, and healthy habits that can prevent the development of cancer in adulthood. Initial plans for delivery of the program was for St. Jude staff to present the program at local schools. This plan for disseminating instruction was not feasible due to the limited availability of St. Jude staff. As a next step, during the 2012–2014 academic years, we conducted a study entitled SJCECP2, utilizing the SJCECP curriculum, with the objective of evaluating the impact of the educational intervention on knowledge acquisition and retention among fourth-grade students participating in a modified, teacher-led version of the program. Eighteen teachers and 426 students from 10 local schools in the greater Memphis area participated in the program evaluation. This study used a single-group, pre-test/post-test design to determine the impact of the SJCECP intervention on changes in knowledge scores among fourth-grade students. Testing was on cells, cancer, and healthy living. The mean scores increased from 6.45 to 8.12, 5.99 to 7.65, and 5.92 to 7.96 on cell, cancer, and health behaviors units, respectively (all p values <.001). Preliminary evidence suggests that the SJCECP2 intervention is a useful tool for teachers to improve student knowledge of knowledge of cells, cancer, and healthy living concepts at the fourth-grade level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
From 1990 to 2010, communicable diseases decreased by 17 % worldwide and non-communicable diseases (NCDs) increased over 30 % [1, 2], with cancer being one of the leading causes of NCD deaths [3]. In the USA, 1 of 4 men and 1 of 5 women will develop cancer in their lifetime and ultimately die from the disease [3]. Despite current trends, many cancers are preventable by making healthy lifestyle choices such as maintaining a healthy weight, eating a nutrient-rich diet, getting regular exercise, and avoiding tobacco use [4–13]. Since lifestyle habits are often formed in childhood, health education for young children is essential to establishing healthy behaviors to reduce the overall risk of developing cancers into adulthood [14–17]. Schools provide excellent vehicles for delivering behavioral health programs, as many such institutions require health education to be included as part of the curriculum [18–23]. Objective EMC-4.3.1 of the US Government’s Healthy People 2020 initiative [7] aims to increase the proportion of schools that require cumulative instruction in health education meeting the US National Health Education Standards for elementary, middle, and high schools. This implies that health education should not only be taught in health classes but also be integrated throughout subject areas. While several school-based interventions targeting children for cancer education exist [23–32], rarely do interventions target young children at the primary school level with a multi-disciplinary, comprehensive cancer education that includes the science of cancer, cancer risk factors, and a wide range of cancer prevention topics (nutrition, avoiding smoking, exercise, and sun protection).
In 2006, St. Jude Children’s Research Hospital in Memphis, Tennessee, developed the St. Jude Cancer Education for Children Program (SJCECP), an educational health intervention designed to integrate cancer-related health topics in science classrooms [33–36]. Its specific goals are to educate schoolchildren about cancer, dispel common misconceptions, promote healthy lifestyle choices that can help them reduce their risk of cancer in adulthood, and inspire an interest in science and scientific careers. The program was designed for students at a third- to fifth-grade reading level as most schools in the Memphis area begin instruction on cells in the fourth grade. Therefore, the SJCECP curriculum, which is composed of three educational units addressing cells, cancer, and healthy living, is a logical fit. In particular, it addresses cancer preventative behaviors such as physical fitness, nutrition, smoking, and sun exposure as environmental factors that impact health at the cellular level. This also provides the opportunity to influence health behaviors in fourth graders before unhealthy behaviors become habitual in adulthood.
An evaluation of the original SJCECP intervention implemented by St. Jude staff members found that fourth graders, 3 months after participation in the program, still retained much of the information they had learned about cancer and healthy behaviors [35, 36]. The implication of these findings is that such knowledge may impact and reduce some behavior-related cancers in adulthood.
While the St. Jude-led delivery of the curriculum showed positive gains in student knowledge, a major drawback of this approach was the limited number of staff available to teach. To overcome this problem, we developed a teacher’s kit for the SJCECP curriculum in order to shift the role of program facilitator from a St. Jude staff member to the classroom teacher. This paper describes the findings of the teacher-led SJCECP study with regard to students’ gains in knowledge after participation in the program.
Methods
Study Design and Materials
This study utilized a single-group, pre-test/post-test design to determine the effect of the teacher-delivered SJCECP intervention on matched knowledge scores among fourth-grade students. The SJCECP intervention consists of three illustrated children’s books, video presentations, and hands-on activities. All of the educational materials were developed and reviewed by a multidisciplinary team composed of St. Jude faculty and staff and local educators. There are three educational modules: Cells (presented as the basic unit of life), Cancer (presented as a disease of unhealthy cells), and Healthy Living (health behaviors as a means of cancer prevention including proper nutrition, safe sun exposure, tobacco control, and appropriate physical activity). A more detailed report of the SJCECP intervention materials has been published previously [28].
Study Sample
Before student enrollment, we sent letters to the school principals through the Shelby County and Memphis City School boards inviting all affiliated public schools with classes in grade 4 to participate in the study. We also sent letters to the principals at private elementary schools in the area for recruitment purposes. Through 2012–2014, 18 teachers and 426 students from 10 local schools participated in the SJCECP intervention evaluation. Approximately 93 % of the students were from public schools, and this reflected the approximate distribution of public to private students in the region. Student participants in the study were fourth-grade boys and girls aged 8–11 years enrolled in traditional curriculum classrooms with the cognitive capacity to complete questionnaires (as determined by the teacher), whose teacher agreed to participate in the study and who attended a school in the Greater Memphis Area (Shelby and surrounding counties). All classroom teachers gave their written informed consent prior to their inclusion in the study. In addition, all parents of students were given an informed consent document providing them the opportunity to opt-out of participation. The demographic data of participating schools, when adjusted for number of student participants, reflect that of the Shelby County population (Table 1).
Teacher Training
Standardized teacher training was required for participating teachers from each school for consistent program implementation. Training took place at each participating school to provide easier access for teachers and to increase participation. Teacher training focused on the goals of the study, a detailed overview of the teacher’s kit, and a demonstration of individual lessons and activities. The teacher’s kit contained a frequently asked questions section for each chapter to help teachers develop comfort with the subject matter as well as detailed instructions for implementing each lesson. Teachers could also consult the St. Jude staff members who developed the program; they provided advice on content and efficiency of course delivery.
Intervention
Each student participated in three lessons delivered by their regular classroom teacher on cells, cancer, and healthy living. Teachers were allowed flexibility in their delivery timeline as long as the entire intervention was completed within a 2-week period. Each lesson was administered during the typical class period and lasted approximately 45–60 min depending on the school schedule. Successful completion of the program required that teachers deliver at least two activities, which could include reading the textbook, viewing the video, and at least one of the in-class activities. In addition, the teachers received a $100 gift card to a local office supply store upon completion of the program. All teachers enrolled in the SJCECP intervention completed the delivery of the program.
Instruments
To assess student knowledge, a questionnaire of 32 multiple-choice items was designed with 10 questions about cells, 10 questions about cancer, and 12 questions about healthy living (tobacco, ultraviolet rays, nutrition, and physical activity). The wording of the multiple choice questions was modified from the questionnaire used in the previous program evaluation based on teacher feedback to make each of the multiple-choice answer options more plausible [36]. An additional survey was added to measure attitudes that students had about healthy lifestyles and self-perceived health status. These data are not included as part of this manuscript.
Data Collection and Analysis
Teachers administered the pre-questionnaire 6 to 8 days before initiating the educational intervention (T0) and before students receive copies of the printed material. The post-questionnaire was administered within 6 to 8 days after the final day of intervention delivery (T1). Differences in the knowledge scores from pre- to post-assessment were utilized in subsequent analyses. Questionnaire completion had no time limit—the amount of time allowed was at the discretion of the teacher. Participants who did not complete both the pre- and post-tests were excluded from data analysis, as were participants who could not be verified as the same person based on self-reported age and birthdate. In total, 426 student pre- and post-tests were analyzed.
We used the one-sample signed rank test to evaluate the pre/post differences in knowledge scores. This difference was calculated within each school and then a stratified analysis was used to assess the overall effectiveness of the intervention. Alternatively, we obtained the p values (Pi) based on the one-sample signed rank test for each of the 10 schools and then combined these independent p values using Fisher combination statistic ΨF = −2Σlog Pi, which follows a chi-square distribution with 28 degrees of freedom, to obtain a p value as an overall measure of the impact that the intervention had on student knowledge.
Results
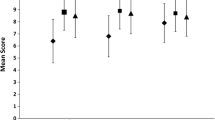
The cells and cancer module quizzes had a maximum score of 10, and the healthy living quiz had a maximum score of 12. The mean score for the cell quiz increased from 6.45 (T1) (2.18 SD) to 8.12 (T2) (2.10 SD). The mean score for the cancer quiz increased from 5.99 (T1) (1.91 SD) to 7.65 (T2) (2.26 SD). The mean score for the healthy living quiz increased from 5.92 (T1) (2.34 SD) to 7.96 (T2) (2.79 SD). Figure 1 shows a comparison of the mean score of the T1 and T2 tests on all modules.

Comparison of the pre- and post-test mean scores for cells, cancer, and healthy living modules
Analysis showed a significant increase in student knowledge in the content areas of cells, cancer, and healthy living from before the program to the week after the program (p < 0.001; Table 2).
Discussion
The results of this study suggest that classroom teachers were successful in promoting knowledge gains among students at the fourth-grade level specific to the topics of cells, cancer, and healthy living to an extent that is comparable to the St. Jude staff-led intervention [35]. In total, these results support the idea of building a sustainable program by shifting the role of program facilitator from St. Jude staff to classroom teacher. By utilizing classroom teachers as the deliverers of the program, dissemination of the program can be expanded beyond the Memphis area and ultimately impact a larger cohort of students.
All content provided for this study was aligned with the local school curriculums and standards. This was a prerequisite for the content to be considered by local school administrators. Expansion of the content nationally will also require alignment with local, state, and national curriculums and standards. This could potentially be a very time-consuming process since the standards are in constant change. Cooperation among national health education organizations would be useful to make it easier for health content developers to align their content with state and national standards. To promote behavior change beyond the initial delivery of the program, new content and community engagement strategies will be needed. The cost of updating the content, alignment with both state and national standards, and coordination with community and health organizations is unclear.
It should be emphasized that knowledge acquisition is only one possible predictor of behavior change. Health behavior changes are often influenced by multiple variables, including socio-demographic factors such as race, gender, and economic status [37]. Factors such as attitudes, beliefs, perceptions of vulnerability, intentions, and self-reported health behaviors can provide a more complete picture of the program’s impact on behavior change [37]. Also, without active ways to engage children and parents with the educational material beyond the initial delivery of the program, health behavior changes are often not achieved or sustained. A 2010 study of the CATCH intervention demonstrated that coupling the school-based intervention with a community component improved the reduction of obesity in disadvantaged students [38]. For the purpose of this article, a univariate approach was utilized to examine non-adjusted change scores in student knowledge across the three specified areas of a teacher-led version of the program; however, future considerations for program modification should include potential community partnerships to enhance the effectiveness of the program at inciting health-related behavioral changes in children.
The strengths of this study are the demonstration that teachers can effectively deliver health and cancer education and that cancer educational material can be presented and understood by young children in the classroom setting. Another strength of the study was its use of a diverse study population that was representative of the larger demographics of the region. Indeed, great care was taken to ensure that the study population represented the demographics of the city of Memphis and its surrounding areas (Table 1). Thus, the program was effective across a broad demographic spectrum and beyond the fourth grade classroom. For example, some students took their health and cancer booklets and educational materials home and discussed what they were learning with their parents. This illustrates an opportunity for reverse mentoring on health education, promoting discussion of health topics at home such as the risks of smoking or poor nutrition. This aspect of the learning experience was not formally evaluated but was reported by some teachers. Future studies could examine the implications of the education at home with parents and siblings.
Limitations of this study include the single-group versus cohort design and the lack of a control group. The study was also limited to one region, and it is not clear how much the effect of the St. Jude Children’s Hospital’s brand affected the positive response of the program. More teachers and students were possibly receptive to the program because of the high regard in which St. Jude is held in the community. Communities that do not have a highly visible health organization might find health education programs more difficult to integrate into the school curriculums. Without a control or comparison group, we cannot definitively conclude that the SJCECP program caused the gains in knowledge observed in this study. Other cancer education may have been available to study participants via Internet, TV, or other media.
Despite these limitations, comparison of the knowledge gains achieved in this study to those published in the St. Jude staff-led study suggests that the SJCECP curriculum is a useful tool for teachers to improve students’ knowledge of cells, cancer, and healthy living [35]. This, however, is no guarantee that teachers will choose to adopt the program into their classroom curriculum. Further research related to teachers’ perceptions of the program and its usefulness in the classroom is needed to determine the feasibility and sustainability of a teacher-led version of the program. Further research is also needed to determine whether this educational intervention positively affects student attitudes, how to create strategies for promoting sustained health behavior changes, and what organizations outside the school and sponsoring hospital could be involved in scaling the program.
Conclusions
Preliminary evidence suggests that the SJCECP intervention is a useful tool for teachers to improve student knowledge of knowledge of cells, cancer, and healthy living concepts at the fourth-grade level. Teachers were able to successfully deliver cancer education, and students in the program were able to improve their knowledge of cancer-related concepts.
References
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, et.al. (2013) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. 330: 2095–2128
Reardon SA (2011) World of chronic disease. Science 333:558–9
American Cancer Society (2014) Lifetime risk of developing cancer. American Cancer Society, Atlanta, http://www.cancer.org/cancer/cancerbasics/lifetime-probability-of-developing-or-dying-from-cancer. Accessed 05 Jan 2016
American Cancer Society (2015) ACS guidelines on nutrition and physical activity for cancer prevention. http://www.cancer.org/acs/groups/cid/documents/webcontent/002577-pdf.pdf. Accessed 07 Dec 2015
National Institute of Health (2015) Cancer prevention. http://www.cancer.gov/research/areas/prevention. Accessed 07 Dec 2015
Centers for Disease Control (2014) Cancer prevention among youth. http://www.cdc.gov/cancer/dcpc/prevention/youth.htm. Accessed 07 Dec 2015
U.S. Department of Health and Human Services. Healthy people 2020. http://www.healthypeople.gov/2020/topics-objectives/topic/cancer. Accessed 07 Dec 2015
World Health Organization (2015) Cancer prevention. http://www.who.int/cancer/prevention/en/. Accessed 07 Dec 2015
Danaei G, Ding E, Mozaffarian D et al (2009) The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med 6:e1000058
World Cancer Research Fund/American Institute for Cancer Research (2007) Food, nutrition, physical activity, and the prevention of cancer: a global perspective. http://www.aicr.org/assets/docs/pdf/reports/Second_Expert_Report.pdf. Accessed 07 Dec 2015
World Cancer Research Fund International. Continuous update project. http://wcrf.org/int/research-we-fund/continuous-update-project-cup. Accessed 07 Dec 2015
Norat T, Aune D, Chan D, Romaguera D (2014) Fruits and vegetables: updating the epidemiologic evidence for the WCRF/AICR lifestyle recommendations for cancer prevention. Cancer Treat Res 159:35–50
Boeing H, Bechthold A, Bub A, Ellinger S, Haller D, Kroke A, Leschik-Bonnet E, Müller MJ, Oberritter H, Schulze M, Stehle P, Watzl B (2012) Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr 51(6):637–63
White MC, Peipins LA, Watson M, Trivers KF, Holman D, Rodriguez JL (2013) Cancer prevention for the next generation. J Adolesc Health 52(5 Suppl):S1–7
Holman DM, Rodriguez J, Peipins L, Watson M, White MC (2013) Highlights from a workshop on opportunities for cancer prevention during preadolescence and adolescence. J Adolesc Health 52(5 Suppl):S8–14
Haverkos L (2010) Pediatric behavior and health promotion research program. National Institutes of Health, Washington, DC, http://www.nichd.nih.gov/about/org/crmc/cdb/prog_pbhp/index.cfm. Accessed 14 Oct 2014
Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC et al (2011) Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act 8:98
Nielsen SJ, Popkin BM (2003) Patterns and trends in food portion sizes, 1977–1998. JAMA 289:450–3
U.S. Department of Health & Human Services (2015) Adolescent and school health. Centers for disease control and prevention, division of adolescent and school health. National Center for HIV/AIDS, viral hepatitis, STD, and TB prevention. http://www.cdc.gov/healthyyouth/index.htm. Accessed 07 Dec 2015
U.S. Department of Health & Human Services (2014) School health policies and practices study 2014. Centers for disease control. Division of adolescent and school health, National Center for HIV/AIDS, viral hepatitis, STD, and TB Prevention. http://www.cdc.gov/healthyyouth/data/shpps/index.htm. Accessed 07 Dec 2015
Merlo C, Brener N, Kann L, McManus T, Harris D, Mugavero K (2015) School-level practices to increase availability of fruits, vegetables, and whole grains, and reduce sodium in school meals—United States, 2000, 2006, and 2014. http://www.cdc.gov/mmwr/pdf/wk/mm6433.pdf. Accessed 07 Dec 2015
Alliance for a Healthier Generation (2015) Program website. https://www.healthiergeneration.org/dev_home/. Accessed 07 Dec 2015
Bares CB, Gelman SA (2008) Knowledge of illness during childhood: making distinctions between cancer and colds. Int J Behav Dev 32:443–450
Rechis R, Neal C, McGoldrick D (2010) LIVESTRONG at school: changing classroom talk about cancer. J Cancer Educ 25(1):127–128
Stöver LA, Hinrichs B, Petzold U, Kuhlmei H, Baumgart J, Parpart C, Rademacher O, Stockfleth E (2012) Getting in early: primary skin cancer prevention at 55 German kindergartens. Br J Dermatol 167(Suppl 2):63–9
Shihab RA, Obeidat NA, Bader RK, Shtaiwi A, Ayub A, Hawari FI (2012) Cancer-related knowledge, attitudes, and risk perception among 6 grade students in Jordan. Stud Health Technol Inform 172:155–60
Rennie LJ, Bazillier-Bruneau C, Rouëssé J (2015) CaPSCA: evaluation of a brief cancer prevention education programme to promote balanced diet in French school children. J Cancer Educ 30(4):759–65
Kyle RG, Forbat L, Rauchhaus P, Hubbard G (2013) Increased cancer awareness among British adolescents after a school-based educational intervention: a controlled before-and-after study with 6-months follow-up. BMC Public Health 4(13):190
Kyle RG, Macmillan I, Rauchhaus P, O’Carroll R, Neal RD, Forbat L, Haw S, Hubbard G (2013) Adolescent Cancer Education (ACE) to increase adolescent and parent cancer awareness and communication: study protocol for a cluster randomised controlled trial. Trials 8(14):286
Divakaran B, Muttapillymyalil J, Sreedharan J, Shalini K (2010) Lifestyle risk factors of noncommunicable diseases: awareness among school children. Indian J Cancer 47(Suppl 1):9–13
Stölzel F, Seide N, Uhmann S, Baumann M, Berth H, Hoyer J, Ehninger G (2014) Be smart against cancer! A school-based program covering cancer-related risk behavior. BMC Public Health 23(14):392
Heuckmann B, Asshoff R (2012) German high school students’ attitudes and interest in cancer and factors influencing proactive behaviour for cancer prevention. J Cancer Educ 29(3):497–505
Van Kirk Villalobos A, Quintana Y, Ribeiro RC (2012) Cure4Kids for Kids: school-based cancer education outreach. Stud Health Technol Inform 172:111–9
Quintana Y, Van Kirk Villalobos A, Li Z, Kumar Srivastava D, Ribeiro RC (2012) Cure4Kids for Kids: preliminary results on evaluating knowledge acquisition and knowledge retention. Stud Health Technol Inform 172:120–8
Ayers K, Villalobos A, Li Z, Krasin M (2014) The St. Jude Cancer Education for Children Program Pilot Study: determining the knowledge acquisition and retention of 4th-grade students. J Cancer Educ. doi:10.1007/s13187-014-0752-5
St. Jude Children’s Research Hospital (2015) Cure4Kids for kids website. http://www.cure4kids.org/kids. Accessed 05 Jan 2016
Glanz K, Rimer BK, Viswanath K (2008) Health behavior and health education: theory, research, and practice. Jossey-Bass, San Francisco, pp 465–82
Hoelscher DM, Springer AE, Ranjit N et al (2010) Reductions in child obesity among disadvantaged school children with community involvement: the Travis County CATCH Trial. Obesity 18(S1):S36–44
Acknowledgments
We thank the St. Jude Children’s Research Hospital International Outreach Program. This study was funded by the American Lebanese and Syrian Associated Charities (ALSAC) of St. Jude Children’s Research Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Human and Animal Rights
This study was reviewed and approved by the St. Jude Children’s Research Hospital Institutional Review Board for Human Subjects Research and therefore was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All classroom teachers and parents of students gave their informed consent prior to their inclusion in the study.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Ayers, K., Li, Z., Quintana, Y. et al. St. Jude Cancer Education for Children Program: The Impact of a Teacher-Led Intervention on Student Knowledge Gains. J Canc Educ 32, 808–813 (2017). https://doi.org/10.1007/s13187-016-1010-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13187-016-1010-9