
Abstract
Hypertension, a major risk factor for cardiovascular diseases, is among the leading causes of morbidity and mortality worldwide. Genetic predisposition to the risk of developing hypertension due to angiotensin-converting enzyme (ACE) gene insertion(I)/deletion(D) polymorphism (through altered serum ACE activity) is well documented among various populations. The present study investigated the possible association between ACE (DD) genotype and hypertension using a nested case-control study design including 451 individuals (of either sex in the age group 30–65 years) from a rural North Indian population practicing agriculture and lacto-vegetarianism. Blood Pressure was classified using JNC-7 criterion. Age- and sex-matched individuals were selected from normotensive (N-122), pre-hypertensive (N-123), hypertensive not on medication (N-122), and hypertensive on medication (N-84) categories. Amplification of DNA and genotyping of PCR product was done using standard protocols. From the analysis, comparatively higher frequency of individuals with DD genotype in the hypertensive category was observed, indicating a possible relation between DD genotype and hypertension. The odds ratio analysis revealed 2.225 (1.13–4.37)-fold significant increased risk for hypertension among cases, validating the vulnerability of individuals with DD genotype towards hypertension. Thus, the present study highlights the increased risk for developing hypertension due to ACE DD genotype in the studied population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hypertension is one of the preventable risk factors for cardiovascular disorders, characterized by elevated blood pressure (systolic blood pressure, SBP ≥140 mmHg and/or a diastolic blood pressure, DBP ≥90 mmHg). It is a complex multi-factorial trait that may lead to complications like stroke, heart disease, kidney failure, blindness, and cognitive impairment. Hypertension is an important modifiable risk factor for premature deaths globally and is directly responsible for deaths due to stroke and coronary heart diseases, myocardial infarction, etc. Approximately 9.4 million deaths worldwide have been reported annually due to hypertension (Lim et al. 2013; WHO 2015). Hypertension is one of the predominant risk factors for cardiovascular diseases in developing countries such as India. Recent literary evidence has reported the prevalence of hypertension to be 29.8% among Indian population, with huge differences in prevalence between rural and urban regions (Anchala et al. 2014; Bhat et al. 2015).
Genetic predisposition also increases the susceptibility to various complex disorders and associated risk factors like elevated blood pressure (Erdmann et al. 2010; Qi et al. 2012). The genetic makeup of an individual could be an important risk factor for increased susceptibility to hypertension. Till date, a total number of 2129 genes have been associated with hypertension (CSELS, 2017). Angiotensin-converting enzyme (ACE) gene is one of the candidate genes involved in rennin angiotensin-aldosterone system (RAAS). ACE enzyme converts inactive angiotensin I into active angiotensin II and also degrades bradykinin to maintain homeostasis of blood pressure (Baudin 2002; Coates 2003; Fleming 2006). Therefore, an increase in serum ACE activity is implicated in elevated blood pressure or hypertension. The ACE insertion/deletion (I/D) gene polymorphism of a 287 Alu element is located in intron 16 on chromosome 17. In spite of its location in non-coding region, ACE I/D gene polymorphism appears to regulate the serum ACE activity. Several epidemiological studies have reported positive association of ACE gene I/D polymorphism with hypertension, specifically DD genotype being associated with elevated blood pressure among different populations (Tiret et al. 1992; Martinez et al. 2000; Choudhury et al. 2012; Singh et al. 2016; Krishnan et al. 2016; Paramasivam et al. 2016). Populations with rural agricultural background practicing lacto-vegetarian diet (Key et al. 1999) and high physical activity (Ekblom-Bak et al. 2014) are expected to be cardio-protected. Despite practicing lacto-vegetarianism and their engagement in high physical activity due to agricultural background, majority of the studied population was found to have elevated blood pressure in the form of hypertension and pre-hypertension (70%) (communicated elsewhere). Thus, the present study is an attempt to understand an association of ACE I/D polymorphism with elevated blood pressure in a Mendelian population with rural agricultural background and lacto-vegetarian diet.
Methods
The present study is a part of a major research project funded by Department of Biotechnology (DBT), Government of India. Under this project, 1634 individuals from either sex belonging to the age group 30–65 years were recruited from a Mendelian population from Palwal district, Haryana. Data on demographic (age and sex), physiological (blood pressure), somatometric [body mass index (BMI), waist circumference (WC), waist hip ratio (WHR)], biochemical (fasting glucose and lipid profile) and lifestyle (education, alcoholism, and smoking status) variables were collected from the recruited individuals unrelated upto first cousins. The categorization of subjects into different categories was done as per the JNC-7 criterion (hypertension, SBP ≥140 mmHg or DBP ≥90 mmHg; pre-hypertension, SBP 120–139 mmHg or DBP 80–89 mmHg; normal blood pressure, SBP <120 mmHg and DBP <80 mmHg). Of total 1634 individuals, 92 individuals were found to be clinically established hypertensive cases and were on medication for blood pressure control, of which comprehensive data on only 84 individuals was available. The selection of hypertensives not on medication (N-122), pre-hypertensives (N-123), and normotensives (N-122) was done matching them for age and sex with the established hypertensive cases on medication. A total of 451 individuals in four different categories were finally included in the study. Individuals with hypertension (both on medication and not on medication) were considered as hypertensive cases and pre-hypertensive and normotensive individuals were considered as controls. DNA samples of the individuals in studied groups were screened for ACE I/D gene polymorphism by using PCR followed by genotyping on 2% agarose gel (Rigat et al. 1990). Statistical analysis was performed using IBM SPSS statistics for Window 20, Version 20.0. (Armonk, NY: IBM Corp.). p value <0.05 was considered as statistically significant and p value 0.05–0.09 was considered suggestive.
Results
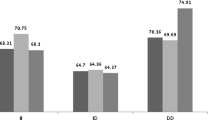
When the genotypic distribution among hypertensive cases and controls was compared, no statistically significant difference was observed. Further, normotensive category was compared independently with all the other four categories (hypertensives on medication, hypertensives not on medication, pre-hypertensives, and cases) with respect to ACE polymorphism (Table 1). From the distribution analysis, it was evident that individuals carrying DD genotype were significantly higher among all the case categories compared to normotensive category. Further, ACE D allele frequency was observed to be ≥0.6 among selected case categories, i.e., cases (0.61), hypertensive on medication (0.60), hypertensive not on medication (0.62), and pre-hypertensive (0.60).
As cases and controls were matched for sex and age, differences between the two with respect to lifestyle, somatometric, and biochemical variables were analyzed among the selected categories. Confounders for hypertension such as body mass index (BMI), waist circumference (WC), waist-hip ratio (WHR), fasting blood glucose, triglyceride (TG), very-low-density lipoprotein (VLDL), and smoking were found to be significantly higher among cases when compared to the normotensives (supplementary table 1). Crude odds ratio (OR) analysis indicated that DD genotype posed almost 2-fold significant increased risk (p value 0.024) whereas adjusted odds ratio analysis (for all the confounders) indicated more than 2-fold increased risk (p value 0.02) of hypertension among the cases (Table 2). Further, DD genotype appeared to pose more than 1-fold increased risk for hypertension (elevated blood pressure) in all the categories when odds ratio adjusted for confounders was calculated for pre-hypertension [1.49 (0.71–1.92)], hypertension on medication [1.73 (0.74–4.03)], and hypertension not on medication [2.59 (1.18–5.70)] independently, though the p value was significant for hypertension not on medication category only.
Discussion
In the present study, individuals with DD genotype were found to be significantly higher among all the four categories (individuals with hypertension and were on medication, hypertension were not on medication and pre-hypertension) compared to the normotensive individuals, indicating some sort of DD genotype or D allele association with elevated blood pressure. Whereas the cases when compared to controls with respect to ACE I/D gene polymorphism, no statistically significant difference was observed. This could possibly be due to inclusion of pre-hypertensive individuals with over-represented DD genotype in control group affecting the association of DD genotype with hypertension. Hypertension categorized as per JNC-7 criterion identifies individuals only with blood pressure SBP >140/DBP>90 as hypertensive cases and the rest as controls (JNC-7 2004). Therefore, many of the case-control studies reporting no association of DD genotype with hypertension (Ashavaid et al. 2000; Nair et al. 2003; Randhawa et al. 2006; Gupta et al. 2009; Badaruddoza 2012) could have been the case of inclusion of pre-hypertensive in control group. Further, the adjusted odds ratio analysis revealed more than 2-fold increased risk for hypertension among individuals with ACE DD genotype. The ACE D allele is implicated in the enhanced serum ACE activity in human body. The increased ACE level is responsible for the conversion of inactive angiotensin I to active angiotensin II which is a potent vasoconstrictor. Additionally, ACE D allele plays a role in metabolizing the bradykinin, a potent vasodilator. Therefore, in the present study as well, D allele in homozygous condition, i.e., DD genotype, is expected to make individuals with DD genotype more susceptible to hypertension (Sayed-Tabatabaei et al. 2006).
The positive association of DD genotype with hypertension as seen in the present study was found to be in concordance with the previous studies reporting positive associations (Choudhury et al. 2012; Zarouk et al. 2011; Paramasivam et al. 2016; Krishnan et al. 2016; Shanmuganathan et al. 2014). Thus, DD genotype appeared to be an important determinant of elevated blood pressure. Although, Gupta et al. has reported no association of ACE I/D polymorphism and hypertension among Haryana population (Gupta et al. 2009). The strength of the study was the selection of cases and controls from a single Mendelian population group wherein most of the confounders like geography, ethnicity, language, culture, food habits, and lifestyle are minimized or controlled to the maximum.
India is a country with high genetic diversity due to the presence of numerous Mendelian groups distinctly separated by geographical and cultural boundaries. A decreasing cline of ACE D allele observed from west to east (Rinaldi 2012) and north (Europeans) to south (Asians) (Fiuza-Luces et al. 2011) on globe has been reported. In Indian context, D allele frequency has been reported to be ranging from 0.26 to 0.78 among different population groups and more than 0.5 among majority of them (Gupta et al. 2009; Saraswathy et al. 2009; Zarouk et al. 2011; Krishnan et al. 2016). In the presently studied population group, high prevalence of hypertension (33%—communicated elsewhere) along with a relatively high frequency of D allele (0.6) was observed. Such co-existence of hypertension and D allele could pose a risk for future cardiovascular disorders, specifically in a population which is supposedly cardio-protected with its lacto-vegetarian diet and high physical activity through agricultural practices.
In addition to this, DD genotype has also been reported to be higher among older age group proposing its association with longevity (Schachter et al. 1994; Petranović et al. 2012; Garatachea et al. 2013). Despite DD genotype being associated with hypertension, a risk factor for cardiovascular complex disorders, it has been proposed to be protective among higher age groups (Fiuza-Luces et al. 2011; Petranović et al. 2012). This anticipated association could be explained through pleiotropic effect of a gene or an allele, leading to adversities at younger age and protection advancing age or an unspecified protective role, independent of cardiovascular system possibly through suggestive neuro-endocrinal activity in brain, immuno-modulating activity in cytotoxic T lymphocytes (Schachter et al. 1994), enhanced tissue repair (Garatachea et al. 2013) conservation of mass/strength (Woods et al. 2001), favoring the survival of individuals with DD genotype till such an age maturity. Alternately, this could also hint towards an association of II genotype with morbidity/mortality at younger age and thereby low frequency of II genotype among older population. However, the impression of DD genotype contributing to exceptional longevity could also be attributed to medical supervision under which hypertensive individuals with DD genotype had achieved improved health status enabling them to survive till such an age maturity.
In developing countries like India that are undergoing demographic transition, individuals with age ≥50 years are expected to form 31% of the total population by 2050; hypertension is not only a health concern but also an economic distress. As estimated by WHO’s EPIC model, India may suffer huge financial loss during 2012–2030 due to CVDs alone, attributed to reduced work force due to cardiovascular morbidities and/or reduction in investment of capital for CVDs’ treatment (Bloom et al. 2014).
Thus, such population specific associations need to be validated among various other population groups with bigger sample sizes to initiate health awareness and developmental programs specifically in light of the candidate gene polymorphisms like ACE insertion/deletion.
References
Anchala R et al (2014) Hypertension in India: a systematic review and meta-analysis of prevalence, awareness, and control of hypertension. J Hypertens 32(6):1170–1177
Ashavaid TF, Shalia KK, Nair KG, Dalal JJ (2000) ACE and AT1R gene polymorphisms and hypertension in Indian population. J Clin Lab Anal 14(5):230–237
Badaruddoza SN (2012) No evidence for association between ACE gene insertion (I)/deletion (D) polymorphism and hypertension in North Indian Punjabi population. Int J Hum Genet 12(3):179–185
Baudin B (2002) New aspects on angiotensin-converting enzyme: from gene to disease. Clin Chem Lab Med 40(3):256–265
Bhat RU, Arora A, Unnikrishnan B, Holla R (2015) Modifiable risk factors for myocardial infarction among hypertensive patients visiting outpatient clinics of tertiary care hospitals in coastal South India. Asian J Pharm Clin Res 8(6):204–206
Bloom D, Fonseca CE, Candeias V, Adashi E, Bloom L, Gurfein L, Llopis JE, Lubet A, Mitgang E, Carroll OJ, Saxena A (2014) Economics of non-communicable diseases in India: the costs and returns on investment of interventions to promote healthy living and prevent, treat and manage NCDs. World Economic Forum. Harvard School of Public Health, Cambridge
Choudhury I, Jothimalar R, Patra AK (2012) Angiotensin converting enzyme gene polymorphism and its association with hypertension in South Indian population. Indian J Clin Biochem 27(3):265–269
Coates D (2003) The angiotensin converting enzyme (ACE). Int J Biochem Cell Biol 35(6):769–773
CSELS 2017 available at https://phgkb.cdc.gov/HuGENavigator/phenoPedia.do?firstQuery=Hypertension&cuiID=C0020538%20%20&typeSubmit=GO&check=y&which=2&pubOrderType=pubD Accessed on Dec 22 2016
Ekblom-Bak E, Ekblom B, Vikström M, de Faire U, Hellénius ML (2014) The importance of non-exercise physical activity for cardiovascular health and longevity. Br J Sports Med 48(3):233–238
Erdmann J, Linsel-Nitschke P, Schunkert H (2010) Genetic causes of myocardial infarction. Dtsch Arzebl Int 107:694–699
Fiuza-Luces C, Ruiz JR, Rodríguez-Romo G, Santiago C, Gómez-Gallego F, Cano-Nieto A, Garatachea N, Rodríguez-Moreno I, Morán M, Lucia A (2011) Is the ACE I/D polymorphism associated with extreme longevity? A study on a Spanish cohort. J Renin-Angiotensin-Aldosterone Syst 12(3):202–207
Fleming I (2006) Signaling by the angiotensin-converting enzyme. Circ Res 98(7):887–896
Garatachea N, Marín PJ, Lucia A (2013) The ACE DD genotype and D-allele are associated with exceptional longevity: a meta-analysis. Ageing Res Rev 12(4):1079–1087
Gupta S, Agrawal BK, Goel RK, Sehajpal PK (2009) Angiotensin-converting enzyme gene polymorphism in hypertensive rural population of Haryana, India. J Emerg Trauma Shock 2(3):150–154
JNC-7 (2004) available at https://www.nhlbi.nih.gov/files/docs/guidelines/jnc7full.pdf Accessed 21 Dec 2016
Key TJ, Fraser GE, Thorogood M, Appleby PN, Beral V, Reeves G, Burr ML, Chang-Claude J, Frentzel-Beyme R, Kuzma JW, Mann J (1999) Mortality in vegetarians and nonvegetarians: detailed findings from a collaborative analysis of 5 prospective studies. Am J Clin Nutr 70(3):516–524
Krishnan R, Sekar D, Subramanium S (2016) Association of angiotensin converting enzyme gene insertion/deletion polymorphism with essential hypertension in south Indian population. Genes Dis 3(2):159–163
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, AlMazroa MA, Amann M, Anderson HR, Andrews KG, Aryee M (2013) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease study. Lancet 380(9859):2224–2260
Martinez E, Puras A, Escribano J, Sanchis C, Carrión L, Artigao M, Divison JA, Masso J, Vidal A, Fernández JA (2000) Angiotensin-converting enzyme (ACE) gene polymorphisms, serum ACE activity and blood pressure in a Spanish-Mediterranean population. J Hum Hypertens 14(2):131–135
Nair KG, Shalia KK, Ashavaid TF, Dalal JJ (2003) Coronary heart disease, hypertension, and angiotensinogen gene variants in Indian population. J Clin Lab Anal 17(5):141–146
Paramasivam R, Nandakumar R, Arumugam D, Krishnan P (2016) Association of ACE DD genotype with hypertension among the tribal populations of South India. ILNS 52:1–8
Petranović MZ, Škarić-Jurić T, Narančić NS, Tomas Ž, Krajačić P, Miličić J, Barbalić M, Tomek-Roksandić S (2012) Angiotensin-converting enzyme deletion allele is beneficial for the longevity of Europeans. Age 34(3):583–595
Qi Q, Forman JP, Jensen MK, Flint A, Curhan GC, Rimm EB, Hu FB, Qi L (2012) Genetic predisposition to high blood pressure associates with cardiovascular complications among patients with type 2 diabetes. Diabetes 61(11):3026–3032
Randhawa NK, Kumar A, Matharoo K, Bhanwer AJ (2006) Association study of angiotensin-converting enzyme ins/del polymorphism with hypertension in Punjabi population. Indian J Hum Genet 6(4):317–321
Rigat B, Hubert C, Alhenc-Gelas F, Cambien F, Corvol P, Soubrier F (1990) An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Invest 86(4):1343–1346
Rinaldi M (2012) I/D ACE gene polymorphism distribution in the world and human prehistoric migrations. J Biol Res – Boll Soc It Biol Sper 85(1):168–169
Saraswathy KN, Kiranmala N, Murry B, Sinha E, Saksena D, Kaur H, Sachdeva MP, Kalla AK (2009) A genomic insight into diversity among tribal and nontribal population groups of Manipur. India Biochem Genet 47(9–10):694–706
Sayed-Tabatabaei FA, Oostra BA, Isaacs A, Van Duijn CM, Witteman JC (2006) ACE polymorphisms. Circ Res 98(9):1123–1133
Schachter F, Faure-Delanef L, Guénot F, Rouger H, Froguel P, Lesueur-Ginot L, Cohen D (1994) Genetic associations with human longevity at the APOE and ACE loci. Nat Genet 6(1):29–32
Shanmuganathan R, Kumaresan R, Giri P (2014) Prevalence of angiotensin converting enzyme (ACE) gene insertion/deletion polymorphism in South Indian population with hypertension and chronic kidney disease. J Postgrad Med 61(4):230–234
Singh M, Singh AK, Singh S, Pandey P, Chandra S, Gambhir IS (2016) Angiotensin-converting enzyme gene I/D polymorphism increases the susceptibility to hypertension and aDDitive diseases: a study on north Indian patients. Clin Exp Hypertens 38(3):305–311
Tiret L, Rigat B, Visvikis S, Breda C, Corvol P, Cambien F, Soubrier F (1992) Evidence, from combined segregation and linkage analysis, that a variant of the angiotensin I-converting enzyme (ACE) gene controls plasma ACE levels. Am J Hum Genet 51(1):197–205
WHO 2015 available at http://www.who.int/features/qa/82/en/ Accessed 21 Dec 2016
Woods D, Hickman M, Jamshidi Y, Brull D, Vassiliou V, Jones A, Humphries S, Montgomery H (2001) Elite swimmers and the D allele of the ACE I/D polymorphism. Hum Genet 108(3):230–232
Zarouk WA, Hussein IR, Esmaeil NN, Raslan HM, Reheim HA, Moguib O, Emara NA, Aly AA, Hamed M (2011) Association of angiotensin converting enzyme gene (I/D) polymorphism with hypertension and type 2 diabetes. Bratisl Lek Listy 113(1):14–18
Acknowledgements
The authors would like to acknowledge Department of Biotechnology, Ministry of Science of Technology, Government of India, for financial assistance and all the participants in the present study for their cooperation. The authors would also like to express sincere gratitude to Prof. P. K. Ghosh and Prof. V. R. Rao for their timely suggestions during the entire study period.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
ESM 1
(DOCX 24 kb)
Rights and permissions
About this article

Cite this article
Rana, G., Yadav, S., Joshi, S. et al. Association of DD genotype of angiotensin-converting enzyme gene (I/D) polymorphism with hypertension among a North Indian population. J Community Genet 9, 51–55 (2018). https://doi.org/10.1007/s12687-017-0321-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12687-017-0321-9