
Abstract
Dizziness and vertigo are among the most common symptoms occurring in clinical practice. However, the data on the main causes of dizziness and vertigo remain contradictory. We have analyzed the causes of dizziness in 590 outpatients who were referred to the neurologist. The most common causes of vertigo and dizziness in outpatient practice were benign paroxysmal positional vertigo (BPPV) (33.9 %), phobic postural vertigo (PPV) (21.4 %), Ménière’s disease/delayed endolymphatic hydrops (20 %), vestibular neuronitis/labyrinthitis (8.1 %), and vestibular migraine (4.1 %). Stroke as a cause of vertigo or dizziness was diagnosed only in 0.8 % of patients. Peripheral vestibular disorders were the most frequent cause of vertigo and dizziness in all age groups of patients: in patients younger than 45 years they were diagnosed in 57 % and in patients older than 60 years in 63.3 % of cases. PPV was the second most common cause of dizziness in patients younger than 45 years (37.4 %) but was established only in 7.6 % of patients older than 60 years. Most of the causes of vertigo and dizziness can be reliably diagnosed with bedside examination while laboratory investigation can be considered as an important but complementary entity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Up to 30 % of the population encounter dizziness to a varying degree [1, 2]. Dizziness is one of the most frequent reasons to visit a neurologist, a general practitioner, or an otolaryngologist. Although this symptom is widespread, diagnostics of the underlying diseases that cause vertigo and dizziness remains difficult. In outpatient practice, the following diagnoses are often mistakenly considered as the causes of dizziness: cerebrovascular pathology (“vertebrobasilar insufficiency,” “hypertensive crisis”) and cervical spondyloarthrosis. On the other hand, peripheral vestibular disorders are not appropriately diagnosed in 74–81 % cases [3, 4]. Meanwhile, numerous recent studies show that the most common causes of dizziness and vertigo are peripheral vestibular disorders (benign paroxysmal positional vertigo (BPPV), Ménière’s disease (MD)) and vestibular migraine, as well as psychogenic disorders [5, 6]. Reliable identification of the most common as well as the most serious and dangerous causes of vertigo and dizziness is a priority in the clinical investigation of such patients in an outpatient unit as well as in the emergency room.
The aim of the research was to identify the main causes of dizziness and vertigo in outpatients referred to the neurologists. Taking into account the most frequent causes of vertigo and dizziness, we also tried to predict the most reliable tests for bedside investigation of outpatients with vertigo and dizziness.
2 Materials and Methods
Between 2007 and 2012, 590 patients who visited the neurologist with complaints of dizziness and/or vertigo were analyzed in our specialized vertigo unit. Informed consent was obtained from all individual participants included in the study. Dizziness or vertigo were the main, and in most cases, the only complaints that triggered the visit to a neurologist.
General physical, neurological, and neuro-otological examinations were done. Clinical diagnoses were made using standardized criteria. To evaluate the vestibular system, the following specific tests were done in all patients: tests of spontaneous and gaze-evoked nystagmus, Dix-Hallpike test and supine roll test, Halmagyi head thrust test, head-shaking test, dynamic visual acuity test, test of skew deviation, Fukuda stepping test, Romberg test, and gait test. We carried out videonystagmography with infrared video system, studying spontaneous, gaze-evoked and positional nystagmus, saccadic eye movements and smooth pursuit, optokinetic nystagmus, and caloric nystagmus.
To refine the diagnosis, the patients had a complete blood count, blood glucose level evaluation, hearing evaluation, vestibular evoked myogenic potential, electrocochleography, posturography or stabilometry, ultrasound carotid imaging, MRI, or CT of the brain.
3 Results
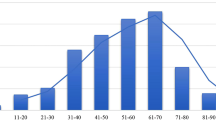
We analyzed the causes of dizziness in 590 patients aged between 16 and 88 years old. The average age of the patients was 49.4 ± 14.6 years. Among these patients, 416 (70.5 %) were females and 174 (29.5 %) were males. The age distribution of patients is shown in Fig. 1.

Age distribution of the patients
The causes of vertigo and dizziness in 590 patients are summarized in Table 1.
We found that the most common cause of dizziness in outpatients was the peripheral vestibular disease (65.9 % of patients). The most common diseases in this group were BPPV (33.9 %), MD and delayed endolymphatic hydrops (20 %), and vestibular neuronitis or labyrinthitis (8.1 %). Less frequently, other peripheral vestibular diseases such as bilateral vestibulopathy, vestibular paroxysms, or labyrinthine infarction were diagnosed.
Phobic postural vertigo (PPV) was the second most common cause of dizziness in the analyzed group of patients (21.4 %).
Central causes of vertigo and dizziness were relatively rare (10.9 %). The most common were vestibular migraine (4.1 %) and unsteadiness (dizziness) due to white matter lesions provoked by cerebral small vessel disease in patients with arterial hypertension, atherosclerosis, and diabetes mellitus (2.7 %).
The distribution of the most common causes of vertigo and dizziness among different age groups is shown in Fig. 2.

Distribution of the most common causes of vertigo and dizziness in different age groups (%)
It was found that in the youngest group of patients (less than 45 years old), the most important causes of vertigo and dizziness were PPV (37.4 %), BPPV (26.7 %), MD/delayed endolymphatic hydrops (15.1 %), and vestibular neuronitis/labirinthitis (11.6 %). In the oldest group (60 years and older), BPPV and MD/delayed endolymphatic hydrops were also common (36.7 and 20.3 %, respectively), but PPV was diagnosed considerably less frequent (7.6 %). Instead of it, important causes of dizziness among the oldest patients in our series were white matter lesion due to cerebral small vessel disease (10.1 %), neurodegenerative diseases with unsteadiness (6.9 %), and multisensory disequilibrium (3.8 %).
Peripheral vestibular disorders were the main cause of vertigo and dizziness in all age groups in our series. In the youngest group, peripheral vestibular disorders were diagnosed in 63.3 % of patients, while in the oldest—in 57 %.
4 Discussion
Vertigo and dizziness are among the most common reasons for consultation and referral to a neurologist and general practitioner [7].
The majority of patients in our series were younger than 60 years. This differs slightly from the results of other studies where it was demonstrated that dizziness and vertigo are the most frequent complaints among patients older than 60 years [8, 9]. These discrepancies may be due to the particular nature of the analyzed group of patients: we investigated causes of vertigo and dizziness in outpatient practice while older patients with vertigo and dizziness, especially acute, are often referred directly to the emergency department.
The presence of multiple concomitant autonomic signs and symptoms during an acute vertigo (elevated blood pressure or collapse, nausea and vomiting) or the comorbidity of numerous cerebrovascular disorders in elderly patients with vertigo and dizziness is a reason of overestimation of vascular origin of these common symptoms. Meanwhile, in our series, the majority of patients had peripheral vestibular diseases as a cause of their vertigo or dizziness, and BPPV was the most common form of those. Other frequent causes of damage of the peripheral vestibular system were MD and delayed endolymphatic hydrops, vestibular neuronitis, and labyrinthitis. We found out that peripheral vestibular disorders were almost equally common in the youngest and oldest groups of patients (57 and 63.3 %, respectively). Similar results were reported in other studies where incidence of peripheral causes of vertigo and dizziness was up to 66 % [10, 11].
Psychogenic factors play an important role in the origin of the perception of dizziness or unsteadiness: according to the results of our study, PPV was the second, after BPPV, cause of dizziness in outpatients (21.4 % of patients). These results were close to the results of other studies according to which PPV was diagnosed in 15.6–26 % of patients of dizziness unit [12–15]. Patients with PPV were younger than those who suffered from other common causes of dizziness. They described their dizziness as light headedness, feeling of derealization, the sense of subjective instability rather than the spinning sensation.
Contrary to the popular belief, cerebrovascular diseases were infrequent causes of dizziness or vertigo in outpatients. In our series, these disorders were diagnosed in 3.5 % of patients. Moreover, stroke was diagnosed among patients with vertigo and dizziness only in 0.8 %. These dates are close to the results of another recent study, which show that a stroke or transient ischemic attack in patients hospitalized with isolated vertigo were diagnosed in 0.7 % of cases [16]. Cerebrovascular diseases were relatively important reason of dizziness (unsteadiness) among the oldest group in our series: white matter lesion as a result of small vessel disease was diagnosed in 10.1 % of patients of 60 years and older. All of these patients, besides dizziness and unsteadiness, had multiple focal neurologic signs and different extent of cognitive impairment as a result of diffuse cerebral vascular lesion.
In general practice, the role of cerebrovascular diseases in vertigo and dizziness patients can be considerably overestimated. Increased blood pressure in patients with acute vertigo is often the consequence but not the cause of it. Apparently, high blood pressure can be considered as an emotional reaction to the severe dizziness.
On the other hand, according to our experience, peripheral vestibular disorders in vertigo or dizziness patients are still an under-recognized entity. Meanwhile, most diseases that were recognized in our patients with vertigo and dizziness can be reliably established by detailed history taking and general neuro-otological examination.
Several algorithms of bedside examination of vertigo and dizziness patients have been proposed recently [17–19]. These studies were mainly focused on developing of the algorithm to examine patients in the emergency unit. It has been demonstrated that clinical investigation is an even more reliable method for differentiation stroke and peripheral vestibular vertigo than MRI [17].
Taking into consideration the most important causes of dizziness and vertigo recognized in our study, the bedside examination of outpatient with vertigo and dizziness should consist of standard neurological assessment, test of spontaneous and gaze-evoked nystagmus, positional tests (Dix-Hallpike; supine roll test), Halmagyi head thrust test and an approximate estimation of hearing. These tests are able to reveal most common causes of dizziness and vertigo and reliably distinguish central and peripheral vertigo.
5 Conclusions
Peripheral vestibular disorders are the most common reason of vertigo and dizziness among outpatients referred to the neurologist. The most common forms of peripheral vestibular disorders, irrespective of the age of patients, are BPPV, MD and delayed endolymphatic hydrops, and vestibular neuronitis/labirinthitis. In younger patients, the second most common reason of dizziness is PPV, while in elderly patients, small cerebral vessel lesions, neurodegenerative disorders, and multisensory disequilibrium play an important role in the development of dizziness/unsteadiness. Most common causes of vertigo and dizziness can be reliably diagnosed with bedside neurological and neuro-otological test while laboratory examination can be considered as important but complementary procedures.
References
Murdin, L., & Schilder, A. G. (2015). Epidemiology of balance symptoms and disorders in the community: a systematic review. Otol Neurotol, 36, 387–92. doi:10.1097/MAO.0000000000000691.
Davis, A., & Moorjani, P. (2003). The epidemiology of hearing and balance disorders. In L. Luxon, J. M. Furman, A. Martini, & D. Stephens (Eds.), Textbook of audiological medicine (pp. 89–99). London: Martin Dunitz.
Kerber, K. A., Morgenstern, L. B., Meurer, W. J., McLaughlin, T., Hall, P. A., Forman, J., et al. (2011). Nystagmus assessments documented by emergency physicians in acute dizziness presentations: a target for decision support? Acad Emerg Med, 18, 619–26. doi:10.1111/j.1553-2712.2011.01093.x.
Royl, G., Ploner, C. J., Leithner, C. (2011). Dizziness in the emergency room: diagnoses and misdiagnoses. Eur Neurol, 66, 256–63. doi:10.1159/000331046.
Hanley, K., & O’Dowd, T. (2002). Symptoms of vertigo in general practice: a prospective study of diagnosis. Br J Gen Pract, 52, 809–12.
Isaradisaikul, S., Navacharoen, N., Hanprasertpong, C., Kangsanarak, J., Panyathong, R. (2010). Causes and time-course of vertigo in an ear, nose, and throat clinic. Eur Arch Otorhinolaryngol, 267, 1837–41. doi:10.1007/s00405-010-1309-9.
Dommaraju, S., & Perera, E. (2016). An approach to vertigo in general practice. Aust Fam Physician, 45, 190–4.
Furman, J. M., Raz, Y., Whitney, S. L. (2010). Geriatric vestibulopathy assessment and management. Curr Opin Otolaryngol Head Neck Surg, 18, 386–391. doi:10.1097/MOO.0b013e32833ce5a6.
Lin, H. W., & Bhattacharyya, N. (2012). Balance disorders in the elderly: epidemiology and functional impact. Laryngoscope, 122, 1858–61. doi:10.1002/lary.23376.
Arya, A. K., & Nunez, D. A. (2008). What proportion of patients referred to an otolaryngology vertigo clinic have an otological cause for their symptoms? J Laryngol Otol, 122, 145–9.
Philip, R., & Prepageran, N. (2009). Dizziness, a review of walk-in patients at a specialised neurotology clinic. Med J Malaysia, 64, 56–8.
Ciríaco, J. G., Alexandre, P. L., Pereira, C. B., Wang, Y. P., Scaff, M. (2004). Phobic postural vertigo: clinical aspects and course of illness. Arq Neuropsiquiatr, 62, 669–673.
Lahmann, C., Henningsen, P., Brandt, T., Strupp, M., Jahn, K., Dieterich, M., et al. (2015). Psychiatric comorbidity and psychosocial impairment among patients with vertigo and dizziness. J Neurol Neurosurg Psychiatry, 86, 302–308. doi:10.1136/jnnp-2014-307601.
Strupp, M., & Brandt, T. (2008). Diagnosis and treatment of vertigo and dizziness. Dtsch Arztebl Int, 105, 173–180. doi:10.3238/arztebl.2008.0173.
Obermann, M., Bock, E., Sabev, N., Lehmann, N., Weber, R., Gerwig, M., et al. (2015). Long-term outcome of vertigo and dizziness associated disorders following treatment in specialized tertiary care: the Dizziness and Vertigo Registry (DiVeR) Study. J Neurol, 262, 2083–91. doi:10.1007/s00415-015-7803-7.
Kerber, K. A., Brown, D. L., Lisabeth, L. D., Smith, M. A., Morgenstern, L. B. (2006). Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: a population-based study. Stroke, 37, 2484–2487.
Kattah, J. C., Talkad, A. V., Wang, D. Z., Hsieh, Y. H., Newman-Toker, D. E. (2009). HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke, 40, 3504–3510. doi:10.1161/STROKEAHA.109.551234.
Newman-Toker, D. E., Kattah, J. C., Alvernia, J. E., Wang, D. Z. (2008). Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis. Neurology, 70, 2378–2385. doi:10.1212/01.wnl.0000314685.01433.0d.
Newman-Toker, D. E., Kerber, K. A., Hsieh, Y. H., Pula, J. H., Omron, R., Saber Tehrani, A. S., et al. (2013). HINTS outperforms ABCD2 to screen for stroke in acute continuous vertigo and dizziness. Acad Emerg Med, 10, 986–96. doi:10.1111/acem.12223.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Zamergrad, M.V., Parfenov, V.A., Yakhno, N.N. et al. Common Causes of Vertigo and Dizziness in Different Age Groups of Patients. BioNanoSci. 7, 259–262 (2017). https://doi.org/10.1007/s12668-016-0351-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12668-016-0351-5