
Abstract
Background
Perianal fistula is one of the most challenging complications of Crohn’s disease (CD). We aimed to describe treatment response with surgical and medical therapies, and long-term complications.
Methods
We retrospectively analyzed records of patients with perianal fistulizing CD who were prospectively followed from January 2005 to December 2018.
Results
Among 807 patients, 81 (10%) had perianal fistula and 65 were included in the final analysis. The mean age of presentation was 27.4 ± 10.3 years, and 78.5% were males with a median duration of follow-up of 45 (IQR, 24–66) months. 75.4% (n = 49) had complex fistulae. 55.4% (n = 36) of patients received multiple courses (> 5 courses) of antibiotics. Complete response rates with immunomodulators, fistula surgery, biologicals, and diversion were 25%, 42.8%, 39.5%, and 45.4%, respectively. The relapse rate was highest after fistula surgery (52.6%). 44.6% of patients received medical (immunomodulators—21 and biologicals—8) whereas 46.1% received surgery as the first-line therapy. The absence of perianal abscess was associated with complete fistula closure. One patient developed malignancy and 4 (6.1%) died at the end of follow-up. Among the patients (n = 28) who received biologicals, TB reactivation occurred in one patient (3.5%).
Conclusion
Medical therapy should be offered as first-line therapy, and immunomodulators can be considered when patients cannot afford biologicals. Surgery offers temporary improvement and is associated with high relapse rates. Absence of perianal abscess predicts long-term complete fistula closure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Perianal fistula is one of the most challenging complications of Crohn’s disease (CD) because of its poor response to available medical or surgical therapy and high relapse rate [1]. It hampers the quality of life and poses a high economic burden in patients with CD. According to the American Gastroenterological Association (AGA) technical review, 2003, the spectrum of the perianal CD includes perianal skin lesions (anal skin tags, hemorrhoids), anal canal lesions (anal fissures, anal ulcers, anorectal strictures), perianal fistulas and abscesses, rectovaginal fistulas, and cancer complicating these lesions [2]. In a population-based study from Olmstead County, the cumulative risk of developing any fistula was 50% after 20 years, with approximately half of them being perianal fistulae [3]. The prevalence of perianal CD in other population-based studies from the West varies from 10% to 26% [4, 5], and in Asia, the prevalence of perianal CD varies from 18% to 24.8%, as reported by the Asia Pacific Crohn’s and Colitis Epidemiology Study (ACCESS) and another retrospective nationwide registry-based study from Hong Kong [6]. The Indian studies report the prevalence rates of perianal fistulas to vary from 6.9% to 40% [7,8,9,10].
Despite the advancements in immunosuppressive therapy, newer surgical techniques, and stem cell-based therapies, complete fistula closure can be achieved only in approximately 50% of patients. Medical treatment options include antibiotics, immunomodulators (azathioprine [AZA], 6-mercaptopurine [6-MP], methotrexate, etc.), anti-TNF drugs (infliximab [IFX], adalimumab [ADA], and certolizumab), anti-IL12/23 drugs (ustekinumab), and anti-integrin therapy (vedolizumab). Antibiotics can reduce the fistula output but do not result in complete closure, and can increase the response rates on biologics [11, 12]. Oral tacrolimus is associated with response and remission in 43% and 8% patients, respectively [13]. All biologics (IFX/ADA/certolizumab) are equally effective, but there are no head-to-head trial comparing these drugs in these patients. The role of immunomodulators like 6-MP/AZA in perianal fistula remains unexplored in clinical trials. Results from a meta-analysis showed 54% fistula healing compared to 21% with placebo; however, the definitions of fistula outcomes were not uniform across studies [14]. Surgical options vary from seton placement to major surgeries like proctectomy and newer options like video-assisted anal fistula surgery. However, the results of various therapies and associated long-term outcomes and complications of perianal fistula in CD are not well described from India and other developing countries where the IBD burden is on the rise [15]. Hence, this single-centre study was done to describe treatment response with surgical and medical therapies, and long-term complications in perianal fistulizing Crohn’s disease.
Methods
Study population
This single-centre study included patients with perianal fistulizing CD who were under follow-up at the inflammatory bowel disease (IBD) clinic, Department of Gastroenterology, All India Institute of Medical Sciences (AIIMS), New Delhi, India, from January 2005 to December 2018. Patients with clinical and radiological evidence of perianal fistulae who were on regular follow-up and had maintained medical records were included in the analysis. Patients with sinus tracts, perianal lesions other than fistulae like perianal ulcers, and fissure were excluded.
Study design and data collection
It was a retrospective analysis of a prospectively maintained database of patients with perianal fistulizing CD. The database is maintained through a file-paper system wherein data is entered by a team of gastroenterologists running the IBD clinic. Patient files contain all dated information concerning the demographic profile, disease phenotypes, radiological findings, follow-up symptom assessment, treatment types (both medical and surgical), and their outcomes. The following parameters were extracted from the database: demographic features, fistula characteristics (including location, extent, number of external openings, associated collection), type of fistula, endoscopic findings, radiological details, therapy received and response, and long-term complications. Any missing data was confirmed by interviewing the patient in person or over the phone.
Choice of therapy
At our centre, the treatment for perianal fistula is individualized and the choice of therapy depends on many factors like anatomy, presence of abscess, proctitis, involvement of bowel other than distal large bowel including small bowel, affordability of patient, and availability of newer treatment modalities. The treatment decision is made after a joint medical-surgical consult. Simple fistulae are managed with a combination of antibiotics and immunomodulators or surgery depending on the associated proctitis, luminal activity, patient preference, and anatomy. If there is no response to medical therapy or drainage procedures, further management is considered in lines of complex perianal fistula. Biologicals are preferred therapy in complex perianal fistula. However, affordability is the major limiting factor in developing countries like India [16, 17], and for non-affordable patients, surgery is the treatment of choice in presence of favorable anatomy. Immunomodulators are considered if surgery is not feasible, and some patients may require both options. Fecal diversion is considered in those patients who fail to achieve response with antibiotics, surgery, immunomodulators, or biologicals.
Ethical considerations
Ethical approval was obtained from the Institutional Ethics Committee.
Statistical analysis
Categorical variables were expressed as percentages and continuous variables were expressed as mean ± SD or median (range) as appropriate. Chi-square test was used to compare categorical variables between patients who were treated with medical therapy at the beginning vs. those who were treated with surgical therapy, and Student t test or Mann-Whitney U test was used to compare continuous variables as appropriate. P < 0.05 was considered statistically significant. SPSS software version 21.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Definitions
-
1.
Crohn’s disease: Diagnosis of CD was made as per European Crohn’s and Colitis Organization (ECCO) guidelines, based upon clinical, radiologic, endoscopic, and histologic features. Disease activity was measured by Crohn’s disease activity index (CDAI) [18].
-
2.
The disease location, behavior, and age at diagnosis were classified as per Montreal classification
-
a.
Age at diagnosis was classified as A1, age below 16 years; A2, between 17 and 40 years; and A3, more than 40 years [19].
-
b.
Behavior was classified as B1, non-stricturing, non-penetrating; B2, stricturing; and B3, penetrating behavior [19].
-
c.
Location was classified as L1, terminal ileal ± cecal; L2, colonic; L3, ileocolonic; and L4, proximal small bowel
-
a.
-
3.
Diagnosis of perianal fistula: Patients with perianal symptoms were examined locally and magnetic resonance imaging (MRI) pelvis was done to delineate anatomy and any collections, and perianal fistula was diagnosed in the presence of T2 hyperintense fistulous tract connecting skin and anorectum.
-
4.
Simple fistula: Low-lying fistula tract with single external opening, no perianal abscess, no evidence of a rectovaginal fistula, and no evidence of anorectal stricture [2].
-
5.
Complex fistula: High perianal fistula tract with multiple external openings or presence of perianal abscess or rectovaginal fistula or anorectal stricture or active proctitis [2].
-
6.
Complete response: Closure of all fistulae with no fistula drainage despite gentle finger compression, that were draining at baseline for at least 2 consecutive visits (i.e., at least 4 weeks apart) [2].
-
7.
Partial response: Improvement in drainage from baseline in the number of open draining fistulas of ≥ 50% for at least 2 consecutive visits (i.e. at least 4 weeks apart) [2]. Response was assessed at 14 weeks after infliximab and adalimumab administration whereas it was assessed at 12 weeks after starting immunomodulators [20, 28].
-
8.
Relapse: Recurrence of fistula after complete closure [2].
Results
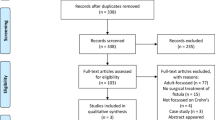
Eight hundred and seven patients with CD were screened, and among them, 81 (10%) had radiological and clinical evidence of perianal involvement. Sixty-five patients were included in the final analysis after excluding patients with perianal sinus tracts (without demonstrable internal opening), those with incomplete records, and those lost to follow-up (Fig. 1).

Flowchart showing screening and inclusion of patients in study
Baseline demographic and clinical profile of patients
The mean age of presentation was 27.4 ± 10.3 years (A1 = 12.3%, A2 = 75.4%, and A3 = 12.3%), and most of them were males (78.5%, n = 51). Median disease duration was 102 (interquartile range [IQR], 70–144) months, and the cohort had a median follow-up period of 45 (IQR, 24–66) months. In 29.2% (n = 19) patients, perianal symptoms like pus discharge from the fistula opening or abscess appeared either before or simultaneously with the onset of CD, and in 70.8% of patients (n = 46), fistulas appeared later in the disease course, after a median duration of 36 (IQR, 20–96) months of CD onset. The majority of the patients had colonic involvement (92.3%, n = 60), while isolated colonic involvement was seen in 44.6% (n = 29) patients. 75.4% (n = 49) patients had complex fistulae, and 26.2% (n = 17) had more than one fistulous tract (Table 1). Almost half of the patients (55.4%) had perianal abscess requiring drainage, and out of them, 19.4% (n = 7) required drainage more than once. Forty patients (61.5%) had active luminal symptoms in the form of diarrhea and abdominal pain during the presentation, and 7.7% (n = 5) had associated non-perianal fistulae. Extraintestinal manifestations (EIM) were seen in 43.1% patients, the commonest being arthralgia (29.2%, n = 19) followed by aphthous ulcer (15.4%, n = 10) (supplementary Table 1).
Treatment outcomes
Among 65 patients, twenty-eight were managed with monotherapy (IM—20%; surgery—4.6%; biologicals—13.8%, and antibiotics—4.6%) (Fig. 2). The remaining patients (n = 37) were treated with more than one treatment modality during the course of the disease (29.2%—surgery, biologicals, and immunomodulators; 27.7%—surgery and immunomodulators).

Details of medical and surgical treatment in perianal Crohn’s disease and response to treatment
Antibiotic therapy
Thirty-six (55.4%) patients received multiple courses (> 5 courses) of antibiotics during the course of the disease. Commonly used antibiotics were satranidazole, metronidazole, ciprofloxacin, and ofloxacin either singly or mostly in combination with immunosuppressant drugs, and half of the patients had a reduction in discharge following the antibiotic course. Complete closure of fistula with antibiotics was seen in only 4 patients.
Immunomodulators
Azathioprine, 6-MP, and methotrexate were used as immunomodulators (IM). IM as primary therapy was given in 55.3% (n = 36) patients, of whom 25% (n = 9) had a complete response and 19.4% (n = 7) had a partial response. Response (complete and partial) was maintained for a median period of 48 months (IQR, 34–70), and 37.5% of them relapsed requiring a change in therapy.
Biological therapy
Twenty-eight (43%) patients received biologicals (infliximab [IFX] and adalimumab [ADA]). Twenty-one received only IFX, 5 received only ADA, and 2 patients were treated with both sequentially when there was secondary loss of response or primary nonresponse to either drug. Complete response was achieved in 42.8% (n = 12) patients, and partial response was achieved in 46.4% (n = 13). The response (complete and partial) was maintained for a median duration of 16 months (IQR, 10–34). Those who achieved complete response with biologicals maintained response for a longer duration (26 months) than those who achieved only partial response (16 months). Primary nonresponse was seen in 10.7% (n = 3) at 8 weeks, and secondary loss of response was observed in 24% (n = 6) of patients after a median duration of 12 months (IQR, 7.7–16.5).
Surgical therapy
Thirty-eight (58.46%) patients had at least one fistula surgery during their disease course. The most common surgery was fistulectomy (47.3%, n = 18) followed by seton (23.7%, n = 9), video-assisted anal fistula treatment (VAAFT) (18.4%, n = 7), fistulotomy (7.8%, n = 3), and examination under anesthesia (EUA) along with surgical drainage in one patient. Complete response was seen in 39.5% (n = 15) and partial response in 10.5% (n = 4) of patients. Post-surgery, the response was maintained for a median duration of 24 months (IQR, 17–33) and 52.6% (n = 10) relapsed after a median duration of 20 months (IQR, 10.5–33.7), requiring medical therapy. Twenty-nine (44.6%) patients received medical therapy (IM—21 and biologicals—8) as first-line treatment. Among them, 10 patients required subsequent treatment change to either surgery (n = 8) or diversion (n = 2). Thirty (46.1%) patients were managed with surgery as first-line therapy and 90% (n = 27) of them required subsequent treatment change to another mode of therapy (Tables 2 and 3). Ten patients underwent repeat surgery before shifting to medical therapy.
Diversion surgery
18.4% (n = 12) of patients required diversion procedures (3 patients underwent diversion as first-line therapy, two after the failure of the initial surgical therapy, one after the failure of medical therapy, and 6 after failure of both medical and surgical therapies) like ileostomy or colostomy after a median duration of 56 months from the onset of fistula. Out of them, 41.6% (n = 5) had complete response and 41.6% (n = 5) had partial response. Forty percent (n = 4) relapsed after a median duration of 18 (IQR, 9–33) months, requiring treatment with biologicals, and the rest of the patients maintained response for a median duration of 56 months.
Predictors of complete fistula closure
At the last follow-up, among 65 patients, 32 patients had complete fistula closure with various therapies including biologicals, surgery, antibiotics, and immunomodulators. At the end of follow-up, 75% of simple fistulae were in complete remission compared to 40% in complex fistulae. Among all the factors, the absence of perianal abscess was the only factor associated with complete fistula closure on univariate analysis. Age at presentation, duration of disease, duration of fistula, smoking, ilea involvement, multiple tracts, complex fistula, early-onset fistula, presence of anorectal stricture, response to antibiotics, treatment with biologics, relapse following surgery, and EIM were not found to be significant (supplementary Table 2).
Complications
Four (6.1%) patients died at the end of follow-up. Two patients died because of an acute coronary event, one patient died while on chemotherapy schedule for adenocarcinoma arising from colo-vesical and perianal fistula, and the cause of death could not be ascertained in one patient. All patients had actively draining fistulas at the time of demise. In 15.4% (n = 10) of patients, the perianal fistula was complicated by anorectal stricture. 4.6% (n = 3) of patients developed fecal incontinence following fistula surgery, and one patient (1.5%) developed rectal perforation following fistulectomy requiring colostomy. Among the patients (n = 28) who received biologicals, TB reactivation occurred in one patient (3.5%) and one patient developed rash following infusion.
Discussion
Perianal fistula is one of the debilitating complications of CD and is associated with poor quality of life and significantly high medical and surgical morbidity [5, 21]. Despite the advances in management of perianal CD including stem cell-based therapies, the outcomes remain unsatisfactory [22]. The prevalence of perianal fistulizing CD appears to be as high in Asian populations as compared to the west [23,24,25]. The prevalence of perianal fistula in CD from hospital-based cohorts across India varies from 6.9% to 40% [7,8,9,10]. Due to the rising disease burden of IBD in developing countries, the IBD physicians in these regions are bound to encounter complications of IBD like the perianal fistulae, and it is imperative to have information on the treatment response and outcomes with various therapies in perianal CD from these resource constraint countries, which the present study had tried to provide.
In the present cohort, approximately 10% of patients with CD suffered from perianal fistulizing disease, with complex fistulae (according to AGA classification) being the predominant type, accounting for 3/4th of cases, similar to other reports. Similarly, in more than 2/3rd of patients, fistulae appeared later in the disease course and > 90% of patients had colonic involvement. More than 50% of patients had associated perianal abscess and 61.5% of patients had associated luminal symptoms. The treatment options for perianal fistulizing CD can be medical, surgical, or a combination of both, and the choice of therapy depends upon the nature of fistulae and associated complications like abscess, anal stricture and luminal symptoms. The medical options include antibiotics, immunomodulators, and biologics and surgically the fistulae can be managed by local procedures (fistula surgeries) or in refractory cases more extensive procedures like diversion surgery or proctectomy. Complex fistulae are more difficult to treat with frequent relapses after the initial response, while simple fistulae respond better, as shown in this and other studies [26]. At the end of follow-up, 75% of simple fistulae were in complete remission compared to 40% in complex fistulae. For complex perianal fistula, treatment outcomes appear to be better with a combination of medical and surgical therapy than either therapy alone [26, 27].
Antibiotics can reduce the fistula output but do not result in complete closure, and can increase the response rates on biologics [12]. In the present study also, though the fistula discharge was reduced in > 50% of patients on antibiotics, only 4 patients had complete closure of the fistula. The role of immunomodulators like 6-MP/AZA in perianal fistula remains unexplored in clinical trials, but has shown efficacy in early studies, either in combination with antibiotics or as maintenance therapy with an approximate efficacy of 30% to 40% [28, 29]. Subgroup analysis of a meta-analysis by Pearson et al. showed fistula response in 54% compared to 21% with placebo, but the definitions of response were not uniform across the studies [14]. Similarly, and interestingly, in the present study also, 25% of patients had a complete and 19.4% had a partial response on AZA/6-MP, of which, on follow-up, only 1/3rd required a treatment change (vs. 90% in the surgery group) and one patient required diversion (vs. 7 in surgery group). Immunomodulators have been considered less effective than biologicals (in the absence of direct evidence comparing these two therapies) and are usually prescribed in conjunction with biologicals. But results from the present study show that immunomodulators can be considered as the first-line therapy in resource-limited countries when patients cannot afford biologicals.
Response to biologicals varies from 20% to 50% in various series. Infliximab is the only monoclonal antibody studied in randomized controlled trials and has been found to be effective for induction and maintenance of response in perianal CD [30]. For other biologics, the evidence for perianal CD stems from a subgroup analysis of their respective RCTs (primarily done in luminal CD). In the subgroup analysis of CHARM and ADHERE trials (for adalimumab), 60% of patients with active draining fistulas had healing of fistulas by 2 years and certolizumab, ustekinumab, and vedolizumab have also been shown to be effective in perianal fistulizing CD [31,32,33]. In the present study, complete fistula closure with infliximab and adalimumab was observed in 42.8% patients which is similar to studies from the west.
Surgery plays an important role in the treatment of perianal fistula, and adequate drainage with concomitant immunosuppression gives the best results. Newer modalities like fibrin glue injection, anal fistula plug, ligation of intersphincteric fistula tract (LIFT), and VAAFT are promising, but data is limited. However, surgery alone results in a high recurrence rate [34, 35]. In the present cohort, approximately half of the patients relapsed after a median duration of 20 months, requiring medical therapy. In refractory cases, diversion or proctectomy can be considered, but in 25% of the cases, proctectomy can be complicated by poor wound healing and formation of a perineal sinus [36]. With advances in treatment, the rate of proctectomy has decreased drastically. In the present study, 12 patients required diversion procedure. However, even after diversion, only 41.6% had a complete response and 40% relapsed suggesting that diversion cannot be offered as a permanent solution in this situation.
Predictors of long-term remission in perianal CD are inconsistent across various studies. Characteristics associated with poor treatment outcomes include ileal location, rectal involvement, and need for more than one surgical procedure and long-term maintenance with biologicals [21]. In the present study, the presence of perianal abscess was negatively correlated with long-term remission.
Population-based studies from Europe indicate that CD is associated with increased risk of mortality, and a meta-analysis by Singh et al. showed a 19% increased risk of coronary artery disease (1.18 OR adjusted; 95% CI, 1.08–1.31) in patients with CD [37]. Systemic inflammatory mediators causing endothelial dysfunction and elevated homocysteine levels have been implicated as mechanisms responsible for atherosclerosis and increased cardiovascular events. In the present study also, there was significant high mortality (6.1%) at the end of follow-up, and all patients had active draining fistula at the time of demise. Among them two patients died because of acute coronary event and one patient died because of malignancy-related complications.
This is the first study from India, and one of the very few from Asia, which has described the treatment outcomes and complications (including malignancy) in patients with perianal CD. Though there are several cohort studies which have described the prevalence of perianal CD, there are none on treatment outcomes. Although biologics are the first-line treatment options for complex fistulae, less than 50% of patients could be treated with biologics, mostly because of their prohibitive cost, and best treatment options had to be replaced by affordable options like immunomodulators and surgery, which is the situation in most developing countries. The study is also limited by its retrospective, single-centre design and small sample size, although the data was extracted from a prospectively maintained database with a reasonably long follow-up. Further, the response was assessed clinically, and follow-up images were not available for all patients. Based on findings of our study and our experience, we present an algorithm geared towards management of perianal fistula in developing countries like India as shown in Fig. 3.

Algorithm for management of perianal fistulizing Crohn’s disease. EUA examination under anaesthesia, EUS endoscopic ultrasound, IM immunomodulator, LIFT ligation of intersphincteric tract, MSCs mesenchymal stem cell therapy, VAAFT video-assisted anal fistula treatment
To conclude, perianal fistulizing CD is a relapsing and remitting disease requiring multi-modality treatment. Immunomodulators can be considered when patients cannot afford biologicals. Surgery offers temporary improvement and is associated with high relapse rates. The absence of perianal abscess predicts long-term complete fistula closure.
References
Kotze PG, Shen B, Lightner A, et al. Modern management of perianal fistulas in Crohn’s disease: future directions. Gut. 2018;67:1181–94.
Sandborn WJ, Fazio VW, Feagan BG, Hanauer SB. American Gastroenterological Association Clinical Practice Committee. AGA technical review on perianal Crohn’s disease. Gastroenterology. 2003;125:1508–30.
Schwartz DA, Loftus EV Jr, Tremaine WJ, et al. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology. 2002;122:875–80.
Peyrin-Biroulet L, Loftus EV, Colombel J-F, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105:289–97.
Mak WY, Mak OS, Lee CK, et al. Significant medical and surgical morbidity in perianal Crohn’s disease: results from a territory-wide study. J Crohns Colitis. 2018;12:1392–8.
Ng SC, Tang W, Ching JY, et al. Incidence and phenotype of inflammatory bowel disease based on results from the Asia-Pacific Crohn’s and colitis epidemiology study. Gastroenterology. 2013;145:158–165.e2.
Das K, Ghoshal UC, Dhali GK, Benjamin J, Ahuja V, Makharia GK. Crohn’s disease in India: a multicenter study from a country where tuberculosis is endemic. Dig Dis Sci. 2009;54:1099–107.
Ramakrishna BS, Makharia GK, Ahuja V, et al. Indian Society of Gastroenterology consensus statements on Crohn’s disease in India. Indian J Gastroenterol. 2015;34:3–22.
Ray G. Inflammatory bowel disease in India - past, present and future. World J Gastroenterol. 2016;22:8123–36.
Goel A, Dutta AK, Pulimood AB, et al. Clinical profile and predictors of disease behavior and surgery in Indian patients with Crohn’s disease. Indian J Gastroenterol. 2013;32:184–9.
Thia KT, Mahadevan U, Feagan BG, et al. Ciprofloxacin or metronidazole for the treatment of perianal fistulas in patients with Crohn’s disease: a randomized, double-blind, placebo-controlled pilot study. Inflamm Bowel Dis. 2009;15:17–24.
Dewint P, Hansen BE, Verhey E, et al. Adalimumab combined with ciprofloxacin is superior to adalimumab monotherapy in perianal fistula closure in Crohn’s disease: a randomised, double-blind, placebo controlled trial (ADAFI). Gut. 2014;63:292–9.
Sandborn WJ, Present DH, Isaacs KL, et al. Tacrolimus for the treatment of fistulas in patients with Crohn’s disease: a randomized, placebo-controlled trial. Gastroenterology. 2003;125:380–8.
Pearson DC, May GR, Fick GH, Sutherland LR. Azathioprine and 6-mercaptopurine in Crohn disease. A meta-analysis. Ann Intern Med. 1995;123:132–42.
Kedia S, Ahuja V. Epidemiology of inflammatory bowel disease in India: the great shift east. Inflamm Intest Dis. 2017;2:102–15.
Makharia GK, Ramakrishna BS, Abraham P, et al. Survey of inflammatory bowel diseases in India. Indian J Gastroenterol. 2012;31:299–306.
Agarwal A, Kedia S, Jain S, et al. High risk of tuberculosis during infliximab therapy despite tuberculosis screening in inflammatory bowel disease patients in India. Intest Res. 2018;16:588–98.
Best WR, Becktel JM, Singleton JW, Kern F. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology. 1976;70:439–44.
Satsangi J, Silverberg MS, Vermeire S, Colombel J. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55:749–53.
Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med. 2004;350:876–85.
Panes J, Reinisch W, Rupniewska E, et al. Burden and outcomes for complex perianal fistulas in Crohn’s disease: systematic review. World J Gastroenterol. 2018;24:4821–34.
Panés J, Rimola J. Perianal fistulizing Crohn’s disease: pathogenesis, diagnosis and therapy. Nat Rev Gastroenterol Hepatol. 2017;14:652–64.
Kim JY, Yang S-K, Byeon J-S, et al. The incidence and natural history of perianal fistulas in Korean patients with Crohn’s disease. Intest Res. 2006;4:22–31.
Jangi S, Ruan A, Korzenik J, de Silva P. South Asian patients with inflammatory bowel disease in the United States demonstrate more fistulizing and perianal Crohn phenotype. Inflamm Bowel Dis. 2020. https://doi.org/10.1093/ibd/izaa029
Kochar B, Barnes EL, Herfarth HH, et al. Asians have more perianal Crohn disease and ocular manifestations compared with white Americans. Inflamm Intest Dis. 2018;2:147–53.
Molendijk I, Nuij VJAA, van der Meulen-de Jong AE, van der Woude CJ. Disappointing durable remission rates in complex Crohn’s disease fistula. Inflamm Bowel Dis. 2014;20:2022–8.
Hyder SA, Travis SPL, Jewell DP, McC Mortensen NJ, George BD. Fistulating anal Crohn’s disease: results of combined surgical and infliximab treatment. Dis Colon Rectum. 2006;49:1837–41.
Dejaco C, Harrer M, Waldhoer T, Miehsler W, Vogelsang H , Reinisch W. Antibiotics and azathioprine for the treatment of perianal fistulas in Crohn’s disease. Aliment Pharmacol Ther. 2003;18:1113–20.
Lecomte T, Contou J-F, Beaugerie L, et al. Predictive factors of response of perianal Crohn’s disease to azathioprine or 6-mercaptopurine. Dis Colon Rectum. 2003;46:1469–75.
Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med. 2004;350:876–85.
Colombel J-F, Schwartz DA, Sandborn WJ, et al. Adalimumab for the treatment of fistulas in patients with Crohn’s disease. Gut. 2009;58:940–8.
Feagan BG, Schwartz D, Danese S, et al. Efficacy of vedolizumab in fistulising Crohn’s disease: exploratory analyses of data from GEMINI 2. J Crohns Colitis. 2018;12:621–6.
Lee MJ, Parker CE, Taylor SR, et al. Efficacy of medical therapies for fistulizing Crohn’s disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16:1879–92.
Schwandner O. Video-assisted anal fistula treatment (VAAFT) combined with advancement flap repair in Crohn’s disease. Tech Coloproctol. 2013;17:221–5.
Jiang H-H, Liu H-L, Li Z, et al. Video-assisted anal fistula treatment (VAAFT) for complex anal fistula: a preliminary evaluation in China. Med Sci Monit. 2017;23:2065–71.
Park SH, Aniwan S, Scott Harmsen W, et al. Update on the natural course of fistulizing perianal Crohn’s disease in a population-based cohort. Inflamm Bowel Dis. 2019;25:1054–60.
Singh S, Singh H, Loftus EV, Pardi DS. Risk of cerebrovascular accidents and ischemic heart disease in patients with inflammatory bowel disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2014;12:382–93 e1: quiz e22.
Author information
Authors and Affiliations
Contributions
Sudheer K. Vuyyuru is responsible for the conception and design of the study, acquisition of data, analysis and interpretation of data, and drafting of the article. Pabitra Sahu, Bhaskar Kante, Peeyush Kumar, and Mukesh Kumar Ranjan are responsible for the analysis, interpretation of data, and revision of the manuscript. Saurabh Kedia, Raju Sharma, SD Gupta, Govind Makharia, and Peush Sahni are responsible for the analysis, interpretation of data, and revision of the manuscript. Prof. Vineet Ahuja is responsible for the conception and design of the study, revising the article critically for important intellectual content, and final approval of the version to be submitted.
Corresponding author
Ethics declarations
Conflict of interest
SKV, PS, SK, BK, PK, MKR, RS, GM, SDG, PS, and VA declare that they have no competing interests.
Ethics statement
The study was performed conforming to the Helsinki declaration of 1975, as revised in 2000 and 2008 concerning human and animal rights, and the authors followed the policy concerning informed consent as shown on Springer.com.Ethical approval was obtained from the Institutional Ethics Committee.
Disclaimer
The authors are solely responsible for the data and the contents of the paper. In no way, the Honorary Editor-in-Chief, Editorial Board Members, or the printer/publishers are responsible for the results/findings and content of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 14 kb)
Rights and permissions
About this article

Cite this article
Vuyyuru, S.K., Sahu, P., Kedia, S. et al. Long-term outcomes in perianal fistulizing Crohn’s disease in a resource-limited setting: A cohort analysis. Indian J Gastroenterol 39, 435–444 (2020). https://doi.org/10.1007/s12664-020-01054-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-020-01054-7