
Abstract
In a world with an increasing population, an alternative for aiding healthcare systems is the use of sensors and wearable devices for monitoring patient physiological data. The analysis of collected data can help guide health services or the self-care of patients. This paper explores literature related to the collection and analysis of physiological data in smart environments by means of a systematic mapping study, organized in three steps: (1) identification of research questions; (2) elaboration of the search process; (3) definition of the criteria for filtering results. Papers were added using the snowball sampling method. This work encompassed 5870 papers published in the past 11 years, up to April 2019. The final selection resulted in 32 papers. Among these, 25 works collected cardiac data, 23 used Wi-Fi, Bluetooth, GSM, or ZigBee technologies, and 14 used techniques for the analysis of physiological data. Mapping verified the more prevalent trends and technologies in the collected and analyzed physiological data from smart environments. The filtering process allowed for a focus on communication technologies and vital sign data types. Three general questions (GQ), two specific questions (SQ), and two statistical questions (STQ) were answered. Similar reviews have already been conducted focusing on sensors, rather than collecting techniques and physiological data analysis. This denotes an opportunity for further studies in the vital sign analysis area.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
According to a recent study (United Nations Department of Economic and Social Affairs 2017), the global population is increasing and aging. This growing portion of the population will demand even more from health systems. The use of technological solutions can improve the quality of life of more people who require care; for example, by using a device that can detect a patient’s vital signs and sending an alert to a healthcare professional when these reach a critical threshold. An alternative is the use of automated systems that collect vital signs for analysis, advising anyone interested in the patient’s health condition accordingly. In this context, the actual challenges and trends related to collecting and analyzing physiological data need to be investigated. A literature revision can help to indicate the issues experienced in this domain for future work on the topic.
This paper used a systematic mapping method to study the use of technologies related to the collection and analysis of physiological data. Studies focusing on different research areas (Goncales et al. 2014; Vianna et al. 2017; Dias et al. 2018; Dalmina et al. 2019) have also applied this approach (Petersen et al. 2008, 2015; Cooper 2016). In addition, related studies have already been conducted in the specific research area highlighted in this paper (Zheng et al. 2014; Touati and Tabish 2013; Punj and Kumar 2018; Chen et al. 2010; Jovanov and Milenkovic 2011). However, these studies aimed at researching sensors, without enlisting communication techniques or the analysis of collected data.
Data analysis can provide a better understanding of patient conditions, despite the fact that some papers reviewed in this work (Kemp et al. 2008; Apiletti et al. 2009; Copetti et al. 2009; Chen 2012; Chen et al. 2013; Salim et al. 2014; Furberg et al. 2017; Fernandes and Lucena 2017; Hu et al. 2012; Achouri et al. 2017; Barreto et al. 2018; Choi and Shin 2018; Hassan et al. 2019) present techniques related to data analysis. Since each patient has different needs, a review is needed to establish whether analyzed data take into consideration individual user profiles. This may indicate an opportunity for future studies on physiological data analysis. This paper’s objective is to highlight the most-used technologies in the field of communication and the analysis of physiological data, thus serving as a basis for future work in this context.
The paper is organized as follows: the next section presents how the study was elaborated, starting with a selection of five computing and health databases. An initial selection of 5870 papers was found, and 32 papers were selected after the filtering process. Afterwards, a section addresses the papers filtered according to the research questions, as well as the results obtained. The penultimate section considers the possible threats to the validity of this work. Finally, the last section presents conclusions and future work.
2 Methods
This paper uses a systematic mapping study as a methodology for conducting a literature review (Budgen et al. 2008; Petersen et al. 2015; Cooper 2016) of research works that investigated how computing can aid in the collection and analysis of physiological data. This methodology is widely recognized and applied in areas such as medicine(Cooper 2016) and social sciences(Petticrew and Roberts 2006). The main objective of such a review is to identify evidence and trends in collections of literary works related to a topic of interest, thus reducing bias when single references are used. Based on the guidelines proposed by Petersen et al. (2015), the systematic mapping herein applied the following steps:
Elaboration of the research questions.
Elaboration of the search process.
Definition of the criteria for filtering results
2.1 Research questions
The research questions applied in this study delineated the discovery of papers that may be related to the collection and analysis of physiological data. Three general questions (GQ), two specific questions (SQ), and two statistical questions (STQ) were defined. The general questions sought basic information regarding the technologies used in smart environments and physiological data. The objective of the specific questions was to understand the quantitative details of selected papers, such as the most common vital signs collected, or whether analysis of the collected data had been effected. Finally, the objective of the statistical questions was to verify where papers had been published, and to define the chronological data of publications. Table 1 presents the research questions.
2.2 Research process
Three steps were defined for the research process: specify the search string, select the databases, and find the results. The first step identified the main terms and their most relevant synonyms. The terms chosen were ‘physiological data’ and ‘smart environments’ as primary terms, and ‘health data’, ‘biometric data’, and ‘ubiquitous environment’ as synonyms.
Once the terms and synonyms were defined, the search string was elaborated. As soon the search string was defined, the search parameters for use in the databases were determined. The second step was to select relevant databases to the study area in order to apply the search string. Seven search databases were used: ACM Digital Library, IEEE Xplore, JMIR, Springer Link, PubMed, Science Direct, and Wiley Online Library. The selection prioritized health and computer science research databases. These databases had previously been used in recent systematic review studies (Goncales et al. 2014; Vianna et al. 2017; Dias et al. 2018; Dalmina et al. 2019).
Research in ACM Digital Library and IEEE Xplore, Science Direct, and Wiley Online Library required the use of an advanced search feature. In the PubMed and JMIR databases, the advanced search was used in combination with the summary and title fields. Finally, in Springer Link, in addition to using the search string as the search query, it was necessary to remove documents categorized as ‘preview only’, and to select the search filter titled ‘computer science’ to obtain relevant results. The final step defined the study filters.
2.3 Study filtering
The studies were filtered in order to select the papers that best focused on the research area. The following inclusion criteria (IC) were defined:
IC 1: the study must have been published in a conference, workshop, or journal.
IC 2: the study should be related to the proposed theme – smart environments, as well as analysis and the collection of physiological data.
IC 3: the study should be a complete paper.
The Exclusion Criteria (EC) were defined, as follows:
EC 1: studies published prior to 2008.
EC 2: studies not written in English.
EC 3: studies published as dissertations or theses.
EC 4: studies that did not include data collection or analysis for smart environments.
EC 5: studies that did not have a relationship with the research questions.
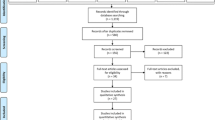
The inclusion and exclusion criteria allowed for obtaining the most relevant studies and to eliminate any noise generated in the research. Figure 1 shows the filtering process. The initial filtering of papers was effected by removing impurities that did not comply with exclusion criteria EC 1, EC 2, and EC 3. Subsequently, a filter was created from the title and keywords of the reviewed papers; finally, selected studies were filtered according to the content of the abstract of the mapped papers.

Filtering process
Three papers (Apiletti et al. 2009; Salim et al. 2014; Nikolidakis et al. 2010) were added using heuristics, as they were considered relevant to the study. These papers were related to the research questions and agreed with the criteria of the paper, even though they were not found in the search process. These papers were found using the snowball sampling method (Cooper 2016), which involved reading the references in the filtered papers and searching for papers that were not found in the initial search. The next filter represents an approach called the three-pass method (Keshav and S 2016).
The first step of three-pass method, comprised four stages: (1) read the title, abstract, and the introduction of each mapped paper; (2) read only the titles of each section and subsection, ignoring the rest; (3) look briefly at the mathematical content (if any) to review whether they are consistent with the theoretical grounds presented in the mapped paper; (4) read the conclusions. The second step involved carefully reviewing figures, diagrams, and other illustrations of papers, with specific attention given to figures.
Finally, the third step was to read the full text, observing exclusion criteria EC 4 and EC 5. The final filters enlisted the 32 remaining papers (see Appendix A). The papers were stored in software called Mendeley Desktop, and organized in different collections according to each search database.
3 Results
The final filter resulted in 32 papers (see Appendix A). The selected papers were analyzed at this stage according to their aims. In the final selection, five papers (Zheng et al. 2014; Touati and Tabish 2013; Punj and Kumar 2018; Chen et al. 2010; Jovanov and Milenkovic 2011) were systematic reviews and did not present the required elements to be answered according to the research questions. The remaining 27 papers were related to the collection or analysis of physiological data. The results of each research question are presented in this section.
3.1 GQ 1: How are smart environments using physiological data for healthcare?
Smart environments work through perceptions (sensors) and actions (controllers). The environment perceives a determined situation and acts through controllers in response to this situation (Cook and Das 2007). The papers below are described to gain a better understanding of how perception and action were effected using physiological data.
Kwon et al. (2008) propose a network architecture model for sending ubiquitous health data, making the packages smaller and adapting the transmission to reduce the energy spent by Internet if Things devices. This solution enhances security in the transmission of physiological data through the network. Kang et al. (2008) developed an architecture for collecting physiological data and displaying it via an internet page. The patient and doctor can track the data in real-time with proper access. The architecture also enables the selection of parameters and the definition of alerts, based on the patient’s current health status.
Kemp et al. (2008) effected the use of a sensor network to increase safety in bomb disposal missions. They created a wearable device to track heartbeat, respiratory flow, and skin temperature. With this information, in addition to environmental temperature, a mission commander can detect the stress of his subordinates, and decide whether they are sufficiently able to proceed in conducting the mission. Hu et al. (2009) propose a system to collect and analyze electrocardiogram (ECG) data of elders in a rest home. The proposed system uses an RFID tag and registers when an elderly individual takes their medication. All of this information is available to caregivers via a server in the rest home.
The study by Copetti et al. (2009) used a framework for the collection and context analysis of vital signs, specifically, heartbeat and blood pressure. The paper considers the current context of patients, their vital signs values, and their global positioning system (GPS) location to issue alerts in critical situations. Apiletti et al. (2009) proposes a model that analyses the patient’s context history to determine a critical situation. Once a critical situation is identified, alerts are made to emergency services or persons interested in monitoring the health status of the patient.
Nikolidakis et al. (2010) present a model that enables a secure means for collecting and sending healthcare data. The model uses health standards such as IMS (information medical statics) and HL7 (health level 7). Sugimoto and Kohno (2011) developed a system that collects ECG and skin temperature data for activity recognition. The system can predict the health status of the user using these data. (Young et al. 2012) monitored ECG during sleep. The system can define user status based on their behavior while sleeping. All of this data can be tracked in real-time through mobile devices.
Hu et al. (2012) used four types of pre-established patterns of activities that the patient may be performing by measuring ECG data. The proposed solution analyses whether the ECG data of the patient is above or below predetermined thresholds. When this occurs either way, the system sends alerts to contacts previously defined. Hung et al. (2012) tracked ECG using a jacket with a sensor, and a photoplethysmogram (detection of the amount of blood in a vessel) using a ring. The analysis of data in this instance was able to detect risk related to heart health. All data can be transmitted by Bluetooth to a nearby computer, where it can be displayed.
Chen (2012) employed a process that collects the ECG and GPS data of the user, and sends it to a center where health specialists analyze it in real-time to provide aid, if needed. Chen et al. (2013) monitored and analyzed the vital signs (ECG, respiratory flow, blood pressure) of the elderly. An image detection technique obtained through the surveillance system was used, alongside physiological data, to send alerts based on pre-established conditions. These conditions were modeled through an ontology.
Salim et al. (2014) monitored the vital signs of firemen during service in real-time. Using this data, as well as context data (GPS, environment temperature), it was possible to predict the physical condition of firemen. In the case of risk, an alert is sent to the mission commander. Touati et al. (2015) ) proposed a platform for collecting physiological data through a low energy IPV6 network. The sensors can be accessed directly using the proposed technology, without the need for a gateway or middleware. Adib et al. (2015) used a sensor for respiratory flow that does not need to be attached to the user. The technique works by calculating the distance between the sensor (which is fixed on a wall) and the user when he inhales and exhales.
Madias (2016) developed an application for tracking ECG through sensors linked to a smartphone. Following the collection of ECG data, said data is sent to cloud storage (also developed in his work). Hossain and Muhammad (2016) propose a framework for collecting and analyzing ECG data. The framework classifies the user’s current health status and aims to guarantee that collected data are not lost due to connection issues. Pham et al. (2016) introduced a smart home that monitors and provides advice about the user’s health status. The proposal used a ZigBee communication protocol and indoor localization through RFID to collect and analyze heartbeat and respiratory flow.
Siddharth and Deshpande (2016) proposed a smart wheelchair with heartbeat monitoring, fall detection, and GPS. The wheelchair works in outdoor environments, sending data through a global system for mobile (GSM) protocol to cloud storage. Achouri et al. (2017) described a framework for detecting user behavior. The data collected from the user (ECG, RFID indoor location) is analyzed, and with the use of ontologies, it is possible to detect if the current behavior of the user presents a risk to the user’s health. The framework proposed by Fernandes and Lucena (2017) allows for the monitoring of temperature and heartbeat through Bluetooth. The analysis of the data through a multi-agent architecture sends alerts in case of a detected risk. The alerts are based on a threshold previously parametrized.
Curmi et al. (2017) investigated the effect of the use of biometric data among online sports spectators. During a marathon, each spectator used a proposed application to receive athletes’ biometric and GPS data. Using the application, spectators were able to cheer for one of the athletes and the athlete wearable device vibrates indicating someone cheering for him during the marathon. After the marathon had been completed, the researchers conducted interviews with the participants and analyzed the interaction of spectators through the ‘cheers’ given using the application. The study sheds light on how biometric data can affect a spectator’s support of athletes. A study by Furberg et al. (2017) introduces a model for monitoring police officers in service. The application determines possible stressful situations, allowing the mission commander to monitor the stress levels of his subordinates.
Barreto et al. (2018) employed a platform based on feature selection and classification methods to detect cardiac arrhythmia. The proposed method can achieve accuracy of up to 90% in arrhythmia diagnosis. Choi and Shin (2018) developed a personalized service for healthcare using IoT devices. The service uses the concept of PHR (personal health records) to store user health data, and can determine risks in real-time. Finally, Hassan et al. (2019) proposed a hybrid real-time monitoring framework for users with chronic diseases. They employed a hybrid algorithm to analyze heartbeat, blood pressure, and respiratory flow, and to detect risks in real time.
3.2 GQ 2: What are the most common techniques and/or technologies for communication of collected physiological data in smart environments?
Figure 2 shows the types of communication technologies most used in the selected papers. Wi-Fi (Copetti et al. 2009; Chen et al. 2013; Furberg et al. 2017; Achouri et al. 2017; Nikolidakis et al. 2010; Young et al. 2012; Madias 2016; Touati et al. 2015; Hassan et al. 2019) and ZigBee (Salim et al. 2014; Nikolidakis et al. 2010; Young et al. 2012; Sugimoto and Kohno 2011; Kang et al. 2008; Pham et al. 2016; Kwon et al. 2008) were the most used, with Bluetooth (Kemp et al. 2008; Fernandes and Lucena 2017; Hu et al. 2012; Hung et al. 2012; Curmi et al. 2017; Choi and Shin 2018; Hassan et al. 2019) in third position. GSM was used in three studies (Chen 2012; Achouri et al. 2017; Siddharth and Deshpande 2016). In one case (Adib et al. 2015), a communication protocol was created specifically for the research, and described by the authors as ‘modulated frequency’.

Types of communication technologies
3.3 GQ 3: What are the most common techniques and/or technologies for the analysis of physiological data in smart environments?
Among the selected papers, a number of common types of analysis were identified, such as analysis of the patient’s current context (geolocation, ambient temperature) (Kemp et al. 2008; Copetti et al. 2009), as well as historic context (Apiletti et al. 2009), where the patient’s physiological data values over a period of time are stored and analyzed as a basis for determining whether a current situation is normal. A classification system was also found (Copetti et al. 2009; Hossain and Muhammad 2016; Barreto et al. 2018; Choi and Shin 2018; Hassan et al. 2019)in which data extraction was made, and data classified according to the aim of the proposal.
Two works byChen et al. (2013) and Achouri et al. (2017) used ontology inference to recommend a treatment, based on the patient’s current condition. In one paper (Chen 2012), the collected data was analyzed manually in real-time by a team of health professionals. Another paper (Salim et al. 2014) used a prediction context-based technique. In this paper, physiological and non-physiological data were analyzed to predict possible issues related to the patient’s health.
Finally, three studies (Furberg et al. 2017; Fernandes and Lucena 2017; Hu et al. 2012) identified pre-established maximum and minimum thresholds for vital signs data. Once data falls outside these limits, alerts will be sent to interested individuals or emergency services. Figure 3 shows the data extracted from the research.

Types of analysis techniques
3.4 SQ 1: What are the most common types of vital signs?
Eleven different types of vital signs were identified. The most common were ECG (Chen 2012; Chen et al. 2013; Hu et al. 2012; Nikolidakis et al. 2010; Young et al. 2012; Sugimoto and Kohno 2011; Madias 2016; Hung et al. 2012; Hu et al. 2009; Touati et al. 2015; Hossain and Muhammad 2016; Barreto et al. 2018; Choi and Shin 2018) and heart beat frequency (Copetti et al. 2009; Salim et al. 2014; Furberg et al. 2017; Fernandes and Lucena 2017; Kang et al. 2008; Pham et al. 2016; Siddharth and Deshpande 2016; Adib et al. 2015; Kemp et al. 2008; Apiletti et al. 2009; Curmi et al. 2017; Choi and Shin 2018; Hassan et al. 2019). This may indicate a trend in the area of monitoring information related to heart health. Figure 4 displays the most commonly used vital signs in the selected papers.

Types of vital signs collected
3.5 SQ 2: Was the user profile considered in the analysis of physiological data?
In one paper (Apiletti et al. 2009), the model considered user profiles and their historical contexts. The authors propose a framework in which the data for each vital sign collected was correlated with the user’s historical profile, thereby verifying whether the vital sign in question reflects a critical or normal situation.
3.6 STQ 1: Where were the studies published?
Figure 5 shows that the selected papers were distributed in journals, conferences, and workshops. Journals represent 50%, conferences 43.75%, and workshops represent 6.25% of total publications. The exact contexts in which studies were published is displayed in Appendix A, along with a relevant name and venue.

Where the included studies were published
3.7 STQ 2: How many publications occurred per year?
Figure 6 shows the distribution of papers according to year of publication. Data was collected up to April 2019, since the study was developed during this year. Research in the area has been ongoing since 2008, with a small variation of papers published over the years.

Publications per year
4 Threats to validity
Like any other systematic mapping study, this work includes risks that can affect its results. Risks are a consequence of decisions made during systematic mapping. Strategies were applied to mitigate their possible impacts.
Seven databases were researched to ensure more complete results. These databases are recognized for their relevance in the areas of computer science and healthcare. This diversity attenuated the risk that research sources limited the results obtained.
The search process and search criteria may have restricted access to papers, so that relevant work in the research area may not have been considered. In this sense, a relevant limitation is that, throughout the filtering process, the papers were analyzed and selected without a reviewer. This risk was mitigated by the application of the techniques proposed (Petersen et al. 2008, 2015; Cooper 2016), which were applied in papers (Goncales et al. 2014; Dias et al. 2018; Vianna et al. 2017; Dalmina et al. 2019). In addition, the composition of the search string considered two primary terms in the research area and three synonymous terms. This strategy broadened the research scope and allowed for better assertiveness in the results.
5 Discussion
Technological solutions applied to healthcare can be characterized as eHealth (Chen et al. 2010; Jovanov and Milenkovic 2011).The eHealth studies presented in the mapping conducted in the current study signify different aims and applications. The studies reviewed in this paper include different types of extensions in the eHealth domain; these may start with data collection, go on to data transmission, and then analyze the collected data. The reviewed papers may use two extension types at the same time. Collection and transmission of physiological data proposals generally display and/or store data. Collection and analysis of the data may have a limited scope of action. Transmission and analysis of the data without collection represent conceptual works. If the proposal used the three extensions within the eHealth domain at the same time, it achieved the full eHealth extension.
The study showed a small number of differences related to the collection of data. The physiological data generally consisted of heart beats per minute, temperature, blood pressure, and/or any other data that can be measured. Since the patient likely used a device to collect the data over a specific period, these must be comfortable and as non-invasive as possible. It can also be useful to collect non-physiological data such as GPS, body position, fall detection, and other contextual information that can be useful in addition to physiological data. The different types of data need to be analyzed or stored; to achieve this, it is important to have a trustworthy means of transmission.
Communication of the data varies according to the protocol adopted, because each context may need a different data transmission type. Generally, the means of transmission employed is wireless, providing mobility to users, and allowing them to transmit data within a limited area range. This range can differ; Bluetooth transmission has smaller coverage, while Wi-Fi solutions have a bigger range, but are always limited by the closest router. GSM communication can attend to a wider area and is generally the chosen protocol in outdoor environments. If communication cannot work in outdoor environments, this may reduce the amount of collected data.
The data may be stored for querying the user’s history and displaying it directly to health professionals. Real-time display of health data can be a powerful tool for anticipating risks. Additionally, the data can be analyzed, rather than simply displayed. The analysis can trigger an action in order to mitigate a possible risk and improve the user’s health. For example, analysis can alert the user or other people, previously defined by them, of any potential risks. Analysis of health data may be able to automatize the tasks of health professionals, increasing the effectiveness of a health service.
If data are only collected and analyzed, it may have a limited range of action. This type of proposal is not found in the reviewed papers and is not a common approach in eHealth systems. In medical practice works, e.g. regular medical appointments, the health professional receives the data and inputs it in a system for analysis. This approach has a limited area of actuation, since it does not use any means of transmission. Generally, it needs a person to manually input the data, which can make it impractical.
The conceptual works reviewed that comprise the use of transmission and analysis are generally based on models, architectures, or frameworks that do not collect data directly from a user. These studies (Apiletti et al. 2009; Achouri et al. 2017) ) propose a means of transmission that considers privacy and security measures in addition to data analysis, and generating alerts in case of risk detection. However, these works did not collect physiological data, and their evaluations are based on databases of real health data; nonetheless, they can still provide resourceful information to analysis. These studies have the potential to achieve the full eHealth extension in future works, since it will only be necessary to further develop their data collection aspects.
Solutions that only collect physiological data but do not analyze it are store/display type solutions. These papers(Kwon et al. 2008; Hu et al. 2009; Nikolidakis et al. 2010; Sugimoto and Kohno 2011; Hung et al. 2012; Young et al. 2012; Touati et al. 2015; Adib et al. 2015; Madias 2016; Pham et al. 2016; Siddharth and Deshpande 2016; Curmi et al. 2017)aim to collect and display health data for those who may require information, such as health services, health professionals, or the user themselves. Generally, the data is stored and can be recovered when needed to better understand the patient’s health history.
Finally, the full extension is achieved in studies that collect, transmit and analyze health data. Some works included in this review (Kemp et al. 2008; Copetti et al. 2009; Hu et al. 2012; Chen 2012; Chen et al. 2013; Salim et al. 2014; Hossain and Muhammad 2016; Fernandes and Lucena 2017; Furberg et al. 2017; Barreto et al. 2018; Choi and Shin 2018; Hassan et al. 2019) provide a solution in each of the three points of the eHealth domain. Wearable devices and health platforms are typically designed for a specific problem, and may not work properly with different platforms or devices. When the full extension is explored, since are all from the same source, this compatibility problem may not occur. The intersection of these three points can fulfill all of the collect, communication, and analysis extensions. Figure 7 shows where each paper in this research is delineated. The numbers refer to the paper ID, shown in Appendix A.

Intersections of the eHealth extension
This paper presented a systematic mapping study related to technologies for the collection and analysis of physiological data in smart environments. During the research, challenges and trends were identified. One of the most significant challenges is the effective use of techniques for the analysis of vital signs. In addition, there were significant research efforts on cardiac monitoring, denoting this focus as a strategic trend. This makes sense, since according to the World Health Organization (2016), 17.9 million people die every year due to heart-related diseases, a number that corresponds to 31% of all global deaths. Unhealthy patients are not the only ones who are requesting analysis to prevent or diagnose health problems; athletes also use eHealth solutions (Curmi et al. 2017) in order to improve their sporting results. Analysis of physiological signs are also used in high-stress situations, for example, in the work of police officers Furberg et al. (2017), firefighters (Salim et al. 2014), and even in bomb disposal missions (Kemp et al. 2008)
Although the collection of vital signs are being widely used in the included works, data analysis lacks the same level of adoption. Only 14 of the 32 selected studies included vital signs analysis techniques, and only 10 of the 14 collected, transmitted, and analyzed data. Among the technologies used to communicate data, a small number of studies (Chen 2012; Achouri et al. 2017; Siddharth and Deshpande 2016) used outdoor technologies such as GSM.
Technologies such as Wi-Fi, ZigBee, and Bluetooth were most commonly used for indoor environments, due to their limited connectivity. Outdoor environments typically do not support these technologies. This limitation can reduce the amount of data generated by the detection of vital signs. In this sense, communication technologies used for collecting vital signs in external areas can improve the scope of action, allowing for the monitoring of patients in real time, and consequently, increasing the quantity and quality of the collected data.
Communication of data has its own challenges, such as privacy, security, and the data persistence (Nikolidakis et al. 2010). Even with the coverage of wireless data transmissions, health systems must guarantee that the data will not be lost, since it can put users who are being monitored at risk. Nikolidakis et al. (2010) and Touati et al. (2015)considered alternatives for when a connection is lost, such as storing data locally until the connection is available.
Systematic mapping research is exposed to risks that may invalidate studies. Risks can originate from decisions made while conducting the research. In order to guarantee the best results, the current study used seven databases recognized for their relevance in computer science and health areas. This strategy allowed for mitigating the risk of databases affecting results.
The filtering process may have restricted the work, so that relevant studies may have been excluded. The filtering process was based on a technique widely adopted in academic research on systematic mapping (Cooper 2016), in order to mitigate this risk. Additionally, the snowball sampling method was used to find studies that did not appear in the filtering process.
6 Conclusion
This paper showed that research studies focused on collecting and monitoring vital signs data instead of the data analysis. Heart conditions represented the most observed information and as such, studies generated significant cardiac data to aid medical decisions. Through the analysis of a large amount of data, it is possible to predict or recommend a diagnostic or treatment in this area (Pittoli et al. 2018).
The use of the full extension of eHealth can potentially improve areas with significant problems related to interoperability. Since the platforms and solutions may not work alongside one another, is important to provide a full path to eHealth usability. Interoperability can be beneficial for everyone involved in healthcare services. For professionals, it can improve the amount of health data available, and with proper analysis, may be able to automatize tasks that generally requires human interaction. Patients can receive healthcare at the point of need and faster response in case of an emergency. Hospitals and clinics can share physiological data information about patients, thus negating the need for repeat tests, and thereby lowering costs through implementation and integration.
The improvement of data collection and transmission may be needed to avoid data loss, as data loss can pose a risk to users. One concern is the energy use of collection sensors and their battery life. Low battery autonomy may lead to a loss of health data. Unavailable communication also poses a risk of data loss. The next generation health systems must be prepared to avoid these risks situations.
Future research may wish to explore the analysis of vital signs to support decision-making related to health. In this sense, vital signs collected by current applications can be formatted as contexts (Dey and Abowd 2001) and stored in chronological databases, (Rosa et al. 2015) and used for context predictions (Rosa et al. 2015). Based on these databases, researchers can design trials for analytical techniques to verify their real effectiveness in aiding health systems. Based on these databases, researchers can design trials for analytical techniques in order to verify their effectiveness in aiding health systems with better compatibility and interoperability.
References
Achouri M, Alti A, Roose P (2017) A new two-Layered architecture for efficient situations management in smart environments. In: Proceedings of the 9th international conference on management of digital EcoSystems, pp 6–13
Adib F, Mao H, Kabelac Z, Katabi D, Miller RC (2015) Smart homes that monitor breathing and heart rate. In: Proceedings of the 33rd annual ACM conference on human factors in computing systems—CHI ’15, pp 837–846. https://doi.org/10.1145/2702123.2702200. URL http://dl.acm.org/citation.cfm?doid=2702123.2702200
Apiletti D, Baralis E, Bruno G, Cerquitelli T (2009) Real-time analysis of physiological data to support medical applications. IEEE Trans Inf Technol Biomed 13(3):313–321. https://doi.org/10.1109/TITB.2008.2010702 ISSN 10897771
Barreto C, da Silva A, Xavier-Júnior J, Soares de Aquino G (2018) A cardiac arrhythmia monitoring platform based on feature selection and classification methods. \(10^{\circ }\) Simpósio Brasileiro de Computação Ubíqua e Pervasiva (SBCUP 2018) 08
Budgen D, Turner M, Brereton P, Kitchenham B (2008) Using mapping studies in software engineering. Proc PPIG 2(01):2008
Chen M, Gonzalez S, Vasilakos A, Cao H, Leung VC (2010) Body area networks: a survey. Mobile Netw Appl 16(2):171–193. https://doi.org/10.1007/s11036-010-0260-8 ISSN 1383469X
Chen M-F (2012) Integrated circuits and systems toward smart ubiquitous patient-centered medical environment. In: Solid state circuits conference (A-SSCC), 2012 IEEE Asian, pp 121–124. https://doi.org/10.1109/IPEC.2012.6522620. URL http://ieeexplore.ieee.org/xpl/articleDetails.jsp?tp=&arnumber=6522620
Chen YL, Chiang HH, Lee, TT (2013) Design and realization of a knowledge-based framework for personalized home healthcare systems. In: 2013 CACS international automatic control conference, CACS 2013—conference digest, pp 180–185. https://doi.org/10.1109/CACS.2013.6734129
Choi A, Shin H (2018) Longitudinal healthcare data management platform of healthcare iot devices for personalized services. J Univers Comput Sci 24:1153–1169 01
Cook D, Das S (2007) How smart are our environments? an updated look at the state of the art. Pervasive Mobile Comput 3:53–73. https://doi.org/10.1016/j.pmcj.2006.12.001 03
Cooper ID (2016) What is a mapping study ? J Med Library Assoc 104(January):76–78. https://doi.org/10.3163/1536-5050.104.1.013
Copetti A, Loques O, Leite JCB, Barbosa TPC, da Nobrega ACL (2009) Intelligent context-aware monitoring of hypertensive patients. In: Proceedings of the 3d international ICST conference on pervasive computing technologies for healthcare. https://doi.org/10.4108/ICST.PERVASIVEHEALTH2009.6058. URL http://eudl.eu/doi/10.4108/ICST.PERVASIVEHEALTH2009.6058
Curmi F, Ferrario MA, Whittle J (2017) Biometric data sharing in the wild: Investigating the effects on online sports spectators. Int J Hum-Comput Stud 105:56 – 67. ISSN 1071-5819. https://doi.org/10.1016/j.ijhcs.2017.03.008. URL http://www.sciencedirect.com/science/article/pii/S1071581917300484
Dalmina L, Barbosa JLV, Vianna HD (2019) A systematic mapping study of gamification models oriented to motivational characteristics. Behav Inf Technol 1–18. https://doi.org/10.1080/0144929X.2019.1576768
Dey AK, Abowd GD (2001) A conceptual framework and a toolkit for supporting the rapid prototyping of context-aware applications. J Hum-Comput Interact 16:97–166
Dias LPS, Barbosa JLV, Vianna HD (2018) Gamification and serious games in depression care: a systematic mapping study. Telemat Inform 35(November 2017):213–224. https://doi.org/10.1016/j.tele.2017.11.002
Fernandes CO, Lucena CJPD (2017) A software framework for remote patient monitoring by using multi-agent systems support. JMIR Med Inform 5(1):e9. ISSN 2291-9694. https://doi.org/10.2196/medinform.6693. URL http://medinform.jmir.org/2017/1/e9/
Furberg RD, Taniguchi T, Aagaard B, Ortiz AM, Hegarty-Craver M, Gilchrist KH, Ridenour TA (2017) Biometrics and policing: a protocol for multichannel sensor data collection and exploratory analysis of contextualized psychophysiological response during law enforcement operations. JMIR Res Protoc 6(3):e44. ISSN 1929-0748. https://doi.org/10.2196/resprot.7499. URL http://www.researchprotocols.org/2017/3/e44/
Goncales L, Farias K, Scholl M, Veronez M, Oliveira T (2014) Model comparison: a systematic mapping study. PIPCA, University of Vale do Rio dos Sinos, p 6. https://doi.org/10.18293/seke2015-116
Hassan MK, Desouky AIE, Elghamrawy SM, Sarhan AM (2019) A hybrid real-time remote monitoring framework with nb-woa algorithm for patients with chronic diseases. Future Gener Comput Syst 93:77 – 95. ISSN 0167-739X. https://doi.org/10.1016/j.future.2018.10.021. URL http://www.sciencedirect.com/science/article/pii/S0167739X17326596
Hossain MS, Muhammad G (2016) Cloud-assisted industrial internet of things (iiot) - enabled framework for health monitoring. Comput Netw 101:192 – 202. ISSN 1389-1286. https://doi.org/10.1016/j.comnet.2016.01.009. URL http://www.sciencedirect.com/science/article/pii/S1389128616300019. Industrial Technologies and Applications for the Internet of Things
Hu F, Celentano L, Xiao Y (2009) Error-resistant rfid-assisted wireless sensor networks for cardiac telehealthcare. Wirel Commun Mobile Comput 9:85–101. https://doi.org/10.1002/wcm.607 01
Hu S, Wei H, Chen Y, Tan J (2012) A real-time cardiac arrhythmia classification system with wearable sensor networks. Sensors (Switzerland) 12(9):12844–12869. https://doi.org/10.3390/s120912844 ISSN 14248220
Hung K, Lee CC, Chan WM, Choy SO, Kwok P (2012) Development of a wearable system integrated with novel biomedical sensors for ubiquitous healthcare. In: Proceedings of the annual international conference of the IEEE engineering in medicine and biology society, EMBS, p 5802–5805. ISSN 1557170X. https://doi.org/10.1109/EMBC.2012.6347313
Jovanov E, Milenkovic A (2011) Body area networks for ubiquitous healthcare applications: opportunities and challenges. J Med Syst 35(5):1245–1254. https://doi.org/10.1007/s10916-011-9661-x ISSN 01485598
Kang K, Kim Y, Lee J, Choi H (2008) Ubiquitous health-assistant system based on accessory-type physiological signal sensing device. In: Digest of technical papers—IEEE international conference on consumer electronics, pp 2–3. ISSN 0747668X. https://doi.org/10.1109/ICCE.2008.4587923
Kemp J, Gaura EI, Brusey J, Thake CD (2008) Using body sensor networks for increased safety in bomb disposal missions. In: Proceedings—IEEE international conference on sensor networks, ubiquitous, and trustworthy computing, pp 81–89. https://doi.org/10.1109/SUTC.2008.25
Keshav SS (2016) How to read a paper. ACM SIGCOMM Comput Commun Rev 37(3):83. https://doi.org/10.1145/1273445.1273458 (ISSN 01464833)
Kwon HC, Na D, Ko BG, Lee S (2008) An energy-efficient communication method based on the relationships between biological signals for ubiquitous health monitoring. In: Conference proceedings : ... annual international conference of the IEEE engineering in medicine and biology society. IEEE Engineering in Medicine and Biology Society. Annual Conference, 2008:1541–1544. ISSN 1557-170X (Print). https://doi.org/10.1109/IEMBS.2008.4649463
Madias JE (2016) A proposal for monitoring patients with heart failure via smart phone technology-based electrocardiograms. J Electrocardiol 49(5):699–706. https://doi.org/10.1016/j.jelectrocard.2016.06.001 ISSN 15328430
Nikolidakis SA, Georgakakis E, Giotsas V, Vergados DD, Douligeris C (2010) A secure ubiquitous healthcare system based on IMS and the HL7 standards. In: Proceedings of the 3rd international conference on PErvasive Technologies Related to Assistive Environments - PETRA ’10, pp 1. https://doi.org/10.1145/1839294.1839345. URL http://portal.acm.org/citation.cfm?doid=1839294.1839345
Petersen K, Feldt R, Mujtaba S, Mattsson M (2008) Systematic mapping studies in software engineering. In: 12th international conference on evaluation and assessment in software engineering 17:10. ISSN 02181940. https://doi.org/10.1142/S0218194007003112
Petersen K, Vakkalanka S, Kuzniarz L (2015) Guidelines for conducting systematic mapping studies in software engineering: an update. Inf Softw Technol 64:1–18. https://doi.org/10.1016/j.infsof.2015.03.007 ISSN 09505849
Petticrew M, Roberts H (2006) Systematic reviews in the social sciences: a practical guide. Oxford: Blackwell. 352 pp. ISBN 1 4051 2110 6., volume 6. Routledge, 2006. https://doi.org/10.1080/14733140600986250
Pham M, Mengistu Y, Do HM, Sheng W (2016) Cloud-Based Smart Home Environment (CoSHE) for home healthcare. In: IEEE international conference on automation science and engineering 2016-Novem:483–488. ISSN 21618089. https://doi.org/10.1109/COASE.2016.7743444
Pittoli F, Damasceno H, Luis J, Barbosa V, Butzen E, Ângela M, Soares J (2018) An intelligent system for prognosis of noncommunicable diseases ’ risk factors. Telemat Inform 35(5):1222–1236. https://doi.org/10.1016/j.tele.2018.02.005
Punj R, Kumar R (2018) Technological aspects of WBANs for health monitoring: a comprehensive review. Wirel Netw 3:1–33. https://doi.org/10.1007/s11276-018-1694-3 ISSN 15728196
Rosa H, Barbosa JLV, Ribeiro GD (2015) ORACON: an adaptative model for context prediction. Expert Syst with Appl 25(January):455–492. https://doi.org/10.1016/j.eswa.2015.09.016 ISSN 0957-4174
Rosa JH, Barbosa JLV, Kich M, Brito L (2015) A multi-temporal context-aware system for competences management. Int J Artif Intell Educ 25(4):455–492. https://doi.org/10.1007/s40593-015-0047-y ISSN 1560-4306
Salim F, Belbasis A, Prohasky D, Houshyar S, Fuss FK (2014) Design and evaluation of smart wearable undergarment for monitoring physiological extremes in firefighting. In: Proceedings of the 2014 ACM international symposium on wearable computers adjunct program—ISWC ’14 Adjunct, pp 249–254. ISSN 15504816. https://doi.org/10.1145/2641248.2666716. URL http://dl.acm.org/citation.cfm?doid=2641248.2666716
Siddharth PD, Deshpande S (2016) Embedded system design for real-time interaction with Smart Wheelchair. In: 2016 symposium on colossal data analysis and networking, CDAN 2016. https://doi.org/10.1109/CDAN.2016.7570917
Sugimoto C, Kohno R (2011) Wireless sensing system for healthcare monitoring thermal physiological state and recognizing behavior. In: Proceedings—2011 international conference on broadband and wireless computing, communication and applications, BWCCA 2011, pp 285–291. https://doi.org/10.1109/BWCCA.2011.44
Touati F, Tabish R (2013) U-healthcare system: State-of-the-art review and challenges. J Med Syst 37(3). ISSN 01485598. https://doi.org/10.1007/s10916-013-9949-0
Touati F, Ben Mnaouer A, Erdene-Ochir O, Mehmood W, Hassan A, Gaabab B (2015) Feasibility and performance evaluation of a 6lowpan-enabled platform for ubiquitous healthcare monitoring: performance of a 6lowpan platform for ubiquitous healthcare monitoring. Wirel Commun Mobile Comput 16:05. https://doi.org/10.1002/wcm.2601
United Nations Department of Economic and Social Affairs (2017) World population prospects the 2017 revision key findings and advance tables
Vianna HD, Luis J, Barbosa V (2017) In search of computer-aided social support in non-communicable diseases care. Telemat Inform 34(8):1419–1432. https://doi.org/10.1016/j.tele.2017.06.005 ISSN 0736-5853
World Health Organization (2016) Cardiovascular disease. URL https://www.who.int/cardiovascular_diseases/world-heart-day/en/
Young CP, Chang DW, Liang SF, Shaw FZ (2012) A portable multi-channel behavioral state and physiological signal monitoring system. In: 2012 IEEE I2MTC—international instrumentation and measurement technology conference, proceedings, pp 2687–2691. https://doi.org/10.1109/I2MTC.2012.6229401
Zheng YL, Ding XR, Poon CCY, Lo BPL, Zhang H, Zhou XL, Yang GZ, Zhao N, Zhang YT (2014) Unobtrusive sensing and wearable devices for health informatics. IEEE Trans Biomed Eng 61(5):1538–1554. https://doi.org/10.1109/TBME.2014.2309951 ISSN 15582531
Acknowledgements
This work was financed in part by FAPERGS/Brazil (Foundation for the Supporting of Research in the State of Rio Grande do Sul - http://www.fapergs.rs.gov.br), CNPq/Brazil (National Council for Scientific and Technological Development - http://www.cnpq.br) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. We would also like to thank the University of Vale do Rio dos Sinos - Unisinos (http://www.unisinos.br) and the FEEVALE University (http://www.feevale.br) for embracing this research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A
Rights and permissions
About this article

Cite this article
Aranda, J.A.S., Dias, L.P.S., Barbosa, J.L.V. et al. Collection and analysis of physiological data in smart environments: a systematic mapping. J Ambient Intell Human Comput 11, 2883–2897 (2020). https://doi.org/10.1007/s12652-019-01409-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12652-019-01409-9