
Abstract
Caanine monocytic ehrlichiosis caused by Ehrlichia canis has gained wider significance owing to its potential to inflict significant deleterious effect on the health of companion animals. In the present study, 46 confirmed ehrlichiosis positive dogs were evaluated for the alterations in clinical, haematological and biochemical attributes. Depression, anorexia, pyrexia, anaemia, weakness, jaundice, melana, vomition and diarrhoea were the main clinical symptoms onserved. Haematological alterations included pancytopenia especially thrombocytopenia. Significant changes were noticed in WBC, RBC, Hgb, McHc, Platelets, ALT values while rest all the studied haematological and biochemical parameters showed non-significant alterations within normal range in comparison to normal healthy controls. The findings substantiate that ehrlichiosis cause significant clinical, haematological and biochemical alterations of the varied intensity in dogs, even with lower grades of parasitaemia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ehrlichia canis the causative agent for canine monocytic ehrlichiosis (CME) is known to possess special affinity for the monocytes and macrophages. The condition is worldwide with a higher incidence rates in tropical and subtropical regions (Milanjeet et al. 2014). So far as Indian scenario is concerned, canine ehrlichiosis has been reported from different parts of the country (Harikrishnan et al. 2009; Milanjeet et al. 2014). Clinically the disease is encountered in three forms viz., acute, subclinical and chronic (Heerden 1982). The diagnosis of canine ehrlichiosis is very challenging to the clinician due to wide range of non-specific clinical symptoms along with resemblances to a number of diseases that mimics ehrlichiosis in clinical presentation. The aim of this study was systematically describe the clinical, haematological, biochemical findings of dogs naturally infected with E. canis, so as to develop a clear clinical pictorial model the disease presentation.
Materials and methods
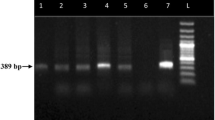
Blood samples were collected from dogs already confirmed for E. canis infection by routine Giemsa staining technique. Briefly, 2 ml of blood was collected from each animal by cephalic vein puncture in vacutainer tubes with and without EDTA. Collected blood samples were equally used to separate out serum and whole blood for analyzing different blood parameters (Jain 1993). Complete blood count was carried out using fully automated Haematology analyser (Diatron). The serum samples were subjected to the estimation of various parameters by using Semi auto chemistry analyser (Electronics India) using commercially available kits (Span cogent diagnostic). The data on clinical manifestations upon clinical examination was done as per score card method described by Varshney et al. (2008) using the clinical histories filled out during the consultation, clinical examination and parasitological results. Alongside, 10 healthy dogs from a kennel were used as control for comparison of attributes.
Statistical analysis
The haemato-biochemical parameters were analyzed by independent samples T test using SPSS statistical software.
Results and discussion
Clinical manifestations
The dogs affected with canine ehrlichiosis showed a wide variability in clinical presentations. The main clinical signs noticed were pyrexia followed by weakness, anorexia, anaemia, epitaxis, melena, ocular signs, jaundice and yellow coloured urine (Table 1).
Haemato-biochemical alterations
The details of the blood parameters examined viz., red blood corpuscle (RBCs) count, white blood corpuscle (WBCs) count, haemoglobin (Hb), haematocrite value (HCT), mean corpuscular volume (MCV), red blood cells distribution width concentration (RDWc), mean corpuscular haemoglobin (MCH), mean corpuscular haemoglobin concentration (MCHC), platelet blood test (PLT) along with lymphocyte, monocyte and granulocyte count are complied in Table 2 alongside the variability in levels ALT, AST, ALP, albumin, total protein, calcium, phosphorus, creatinine (Table 3). Significant changes were noticed in WBC, RBC, Hgb, McHc, Platelets, ALT values while rest all the parameters showed non-significant alterations within normal range in comparison to normal healthy controls.
More or less similar types of clinical manifestations have earlier been reported by several workers. The mild variations in these clinical signs could be very much attributed to a number of factors including variability in pathogenicity of various strains of Ehrlichia, breeds of dogs, concurrence with other diseases, immune status of dogs, etc. The most important clinical findings that may raise suspicion for ehrlichiosis included pyrexia, depression, pale mucosa, bleeding tendencies in form of epitaxis and malena. Amongst these, epistaxis may be considered as the single most finding attributing suspicion of ehrlichiosis (Troy et al. 1980). The melena and epitaxis and other bleeding tendencies could be attributed to thrombocytopenia and the deposition of immune complexes on the vascular wall (Rungsipipat et al. 2009). Amongst the main haemato-biochemical variables, significant pancytopenia, decreases in plasma proteins along with haemoglobin levels are thought to be cardinal for ehrlichiosis (de Castro et al. 2004). The alterations in the protein metabolism in liver due to tissue damage alongside bone marrow suppression may be supposed to be the contributing factor for these changes (de Castro et al. 2004). Significant decrease in the plasma protein levels and colloidal osmotic pressure subsequent to hepatic necrosis eventually accounts for oedema in CME (Rungsipipat et al. 2009). Hematological abnormalities like non regenerative anemia and thrombocytopenia alongside hyperglobulinemia, hypoalbuminemia and low albumin-globulin ratio are the other biochemical abnormalities frequently encountered in CME (Neer and Harrus 2006).Platelet consumption, increased splenic sequestration and decreased platelet lifespan are the possible attributes for thrombocytopenia (Harrus et al. 1999). Depleted synthesis of coagulation proteins in the liver due to necrosis may also cause increased platelet aggregation further aggravating the thrombocytopenia (Rungsipipat et al. 2009). Thrombocytopenia, mainly due to large-scale destruction of the cells in the spleen that begins a few days after the infection (Smith et al. 1975) alongside bone marrow hypoplasia, are also amongst the primary causes of pancytopenia including thrombocytopenia (Waner 2008).
Nonregenerative anemia, thrombocytopenia and mild leucopenia are the generally accepted three cardinal hematological attributes subsequent to acute to subacute infection of CME. The non regenerative anaemia is incriminated to bone marrow hypoplasia leading to impaired production of cellular components of blood. Many of the clinical symptoms in CME like fever are attributed to over production of interleukin-1 by the antigen-presenting cells and B cells or even because of exogenous pyrogenic products of the causative agent (de Castro et al. 2004). Again immunopathological mechanisms involving significant increase in levels of serum antiplatelet IgG resulting in the removal of antibody adsorbed thrombocytes by the mononuclear phagocyte system in the liver and spleen also contribute significantly to thrombocytopenia (Waner et al. 2001). Transient suppression of bone marrow activity along with its hypoplasticity due to accumulation of marrow fat and subsequent decrease of erythroid cell series is the prime factor responsible for anemia and thrombocytopenia (Rungsipipat et al. 2009). Thrombocytopenia is often seen as a diagnostic identity for CME. Though a number of supporting factors are stated in literature pertaining to thrombocytopenia yet the basics lies in the increase of antiplatelet antibodies and subsequent decrease in circulating half-life of the platelets causing acute destruction of platelets accounting for the foundations of pathogenesis of thrombocytopenia. These phenomena also demonstrates the other clinical signs in CME like skin and subcutaneous hemorrhages pale visceral organs, ascites, and jaundice.
Along with these changes, generalized lymphadenopathy and splenomegaly also occurs due to proliferation of lymphocytes of medullary and paracortical region and is further aggravated by the aggregation of reactive histiocytes (Rungsipipat et al. 2009). This is histopathologically demonstrated by the presence of increased extramedullary hemopoiesis and hemosiderosis (de Castro et al. 2004; Rungsipipat et al. 2009). A linear relationship exists between the increase in titers of immunolabeled IgM and IgG coated cells and presence of anti-E canis IgG antibodies in the lymph nodes (Cadman et al. 1994). All these contributing factors signify the central role of spleen and lymph nodes in the immunopathogenesis of CME. Alongside, liver is widely regarded as the target organ affected with CME as is exemplified by seen in the increase in activity of specific liver enzymes (AST, ALT, AP, bilirubin) along with histological alterations pertaining to severe diffuse centrilobular degeneration and chronic active hepatitis along with generalized hypoproteinemia, hypoalbuminemia (Rungsipipat et al. 2009). Functional loss of several of the liver functions is depicted on the host in the form of ascites, bleeding disorders, prerenal azotemia, hepatic encephalopathy, and is the major cause of death (Rungsipipat et al. 2009).
In conclusion, it can be concluded that anaemia, leucopaenia and thrombocytopaenia must be included in the differential diagnosis when observed during routine laboratory evaluations for diagnosis of canine ehrlichiosis. Besides these, the clinical score card is also very important for routine and timely diagnosis of CME.
References
Cadman HF, Kelly PJ, Matthewman LA, Zhou R, Mason PR (1994) Comparison of the dot-blot enzyme linked immunoassay with immunofluorescence for detecting antibodies to Ehrlichia canis. Vet Rec 135(15):362
de Castro MB, Machado RZ, de Aquino LP, Alessi AC, Costa MT (2004) Experimental acute canine monocytic ehrlichiosis: clinicopathological and immunopathological findings. Vet Parasitol 119:73–86
Harikrishnan TJ, Chellappa DJ, Pazhanivel N, Rajavelu G (2009) Serodiagnosis of canine ehrlichiosis by enzyme linked immunosorbent assays. Indian Vet J 86:668–670
Harrus S, Waner T, Bark H, Jongejan F, Cornelissen AW (1999) Recent advances in determining the pathogenesis of canine monocytic ehrlichiosis. J Clin Microbiol 37:2745–2749
Heerden JV (1982) A retrospective study in 120 natural cases of canine ehrlichiosis. J South Afr Vet Assoc 53:17–22
Jain NC (1993) Physiology of blood with some comments on response to disease. Int J Anim Sci 8:195–231
Milanjeet Singh H, Singh NK, Singh ND, Singh C, Rath SS (2014) Molecular prevalence and risk factors for the occurrence of canine monocytic ehrlichiosis. Vet Med 59(3):129–136
Neer TM, Harrus SH (2006) Canine monocytotropic ehrlichiosis and neorickettsiosis. In: Greene CE (ed) Infectious diseases of the dog and cat, 3rd edn. W.B. Saunders Co., St. Louis, pp 203–219
Rungsipipat A, Oda M, Kumpoosiri N et al (2009) Clinicopathological study of experimentally induced canine monocytic ehrlichiosis. Comp Clin Pathol 18:13–22
Smith RD, Ristic M, Huxsoll DL, Wangnaitham S, Poosoonthontham R, Komkaew W, Suksawat F, Ryoji Y (1975) Platelet kinetics in canine ehrlichiosis: evidence for increased platelet destruction as the cause of thrombocytopenia. Infect Immun 11:1216–1221
Troy GC, Vulgamott JC, Turnwald GH (1980) Canine ehrlichiosis: a retrospective study of 30 naturally occurring cases. J Am Anim Hosp Assoc 16:181–187
Varshney JP, Deshmukh VV, Chaudhary PS (2008) Multisystemic effects of canine babesiosis and management of critical cases. Intas Polivet 9(2):281–287
Waner T (2008) Hematopathological changes in dogs infected with Ehrlichia canis. Israel Vet Med J 63:1–8
Waner T, Harrus S, Jongejan F, Keysary A, Cornelissen AW (2001) Significance of serological testing for ehrlichial diseases in dogs with special emphasis on the diagnosis of canine monocytic ehrlichiosis caused by Ehrlichia canis. Vet Parasitol 95:1–15
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Parashar, R., Sudan, V., Jaiswal, A.K. et al. Evaluation of clinical, biochemical and haematological markers in natural infection of canine monocytic ehrlichiosis. J Parasit Dis 40, 1351–1354 (2016). https://doi.org/10.1007/s12639-015-0688-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12639-015-0688-7