
Abstract
Background
This study aimed to investigate the effects of different intra-session exercise orders during concurrent training (CT) on endurance performance in elderly men, as well as to verify its influence on individual responses in endurance performance.
Design
Twenty-five healthy elderly men (64.7 ± 4.1 years) were placed into two groups: strength training prior to endurance training (SE, n=13), and one in the reverse order (ES, n=12). CT was performed three times a week during 12 weeks. Before and after training, peak oxygen uptake (VO2peak), maximal workload (Wmax), absolute and relative cycling economy at 25, 50, 75 and 100 W (i.e., average VO2 at different stages) were assessed.
Results
Similar increases in VO2peak were observed in the SE and ES groups (SE: 8.1 ± 9.9%; ES: 9.3 ± 9.8%; P<0.001), as well as in Wmax (SE: 19.9 ± 19.3%; ES: 24.1 ± 24.0%; P<0.001). Moreover, significant reductions were observed in the absolute VO2 at 100 W (P<0.05) in the SE and ES groups. No difference between groups was observed. In the ES group, one subject did not respond positively in terms of both VO2max and Wmax, whereas 4 subjects did not respond positively in terms of both VO2max and Wmax in SE group.
Conclusions
CT improved maximal and submaximal endurance performance in elderly men, independent of intra-session exercise order. However, it seems that the ES order elicited more individual responsiveness in terms of maximal endurance performance than SE order..
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Along with a decline in neuromuscular function, aging is associated with a decrease in cardiorespiratory fitness that results in an impaired capacity to perform daily activities and maintain independence and quality of life (1-4). In fact, it is well established that low cardiorespiratory fitness is associated with mortality in elderly men and women (5, 6). To counteract this effect, regular exercise training can prevent the loss of cardiorespiratory function and age-associated diseases such as hypertension, diabetes and dyslipidemia. Although endurance training promotes more pronounced cardiorespiratory adaptations, such as maximal aerobic power (VO2peak) (7, 8) strength training also induces increases in submaximal endurance performance, which can contribute to overall cardiorespiratory enhancement in the elderly (3-9). Indeed, submaximal endurance performance may be particularly important in the elderly because most activities of daily living are performed at low rates of oxygen consumption (10).
A combination of strength and endurance training (i.e., concurrent training) in elderly populations appears to be the most effective strategy for improving both neuromuscular and cardiorespiratory functions during aging (7, 9, 11). In addition, concurrent training promotes endurance adaptations similar to those produced by endurance training alone (7, 9, 12, 13). Previously, we showed that different intra-session concurrent exercise sequences (i.e., strength-endurance or endurance-strength) resulted in similar increases in peak oxygen uptake, maximal workload on a cycle ergometer, and power at the second ventilatory threshold (14). However, we observed in that study that only the strength-endurance order improved power at the first ventilatory threshold (14), we hypothesized that greater contrasts between different exercise sequences could occur for other endurance performance markers, such as cycling economy. Nevertheless, to the best of our knowledge, only one study conducted in young men and women has previously addressed the order effect on submaximal endurance parameters (15). This study demonstrated a reduction in the submaximal oxygen consumption during exercise on a cycle ergometer for both exercise orders after concurrent training in young men after 24 weeks of training but not after 12 weeks. Notwithstanding, due to the evident difference in physical fitness between young and elderly individuals (1), there is a need to expand the knowledge regarding the effects of different exercise sequences during concurrent training on submaximal endurance performance in the elderly, because the order effects on sub-maximal oxygen consumption have not been investigated in health elderly performing concurrent training.
There is considerable interindividual variability in response to endurance training (i.e., VO2max and Wmax) that has not been clarified in elderly (16-19). This means that under the same stimulus, some subjects may achieve positive benefits after training (i.e., responders – R) (16, 20, 21) while others exhibit a worsened or unchanged response and are thus termed non-responders (NRs) (18, 21-23). Recently, it has been shown that responders to high-intensity interval endurance training (HIIT) do not necessarily respond to low-intensity continuous endurance training (21). Although variability in individual responses to endurance training is well established (16, 20, 21, 24), the influence of intra-session exercise order during concurrent training on individual endurance performance responsiveness has not been investigated in elderly populations. This knowledge could be especially important for determining which intra-session exercise order would produce greater responsiveness in a group of elderly men.
Considering the relevance of submaximal endurance performance in the elderly, the present study aimed to investigate the prevalence of non-responders and the effects of different intra-session exercise orders during concurrent training on maximal and submaximal endurance (i.e., cycling economy) performance in healthy elderly men. Because of the greater strength gains obtained in the strength-endurance order (14), we hypothesized that this order (i.e., strength-endurance) during a concurrent training would provide greater improvements in cycling economy at different intensities in elderly individuals when compared with the inverse order. In addition, a second purpose of this study was to verify the influence of intra-session exercise order during concurrent training on individual responses in terms of maximal endurance performance. We also hypothesized that both exercise orders would provide similar prevalence of non-responders.
Material and methods
Experimental design and approach to the problem
To investigate the effects of the exercise sequence of concurrent endurance and strength training on cycling economy in elderly subjects, two training groups performed prolonged training that had previously resulted in marked improvements in both endurance and strength performance (7, 25). The present study is part of a larger research project in which we aimed to investigate the neuromuscular and cardiovascular adaptations to different concurrent strength and endurance training protocols in elderly men (14). Because the aim of the present study was to expand our previous results by comparing the cardiovascular adaptations to two different ways of prescribing concurrent training (i.e., different intra-session exercise orders), a control group was not tested. However, to test the stability and reliability of the performance variables, some of the subjects were evaluated twice before the start of training (weeks –4 and 0). Testing pre- and post-intervention was performed by the same investigator, who was blinded to the training group to which the subjects belonged. The ambient conditions were kept constant throughout all tests (temperature: 22-24°C). This study was conducted according to the Declaration of Helsinki and was approved by the Ethics Committee of Federal University of Rio Grande do Sul, Brazil.
Subjects
Twenty-five healthy community-dwelling elderly men (mean ± SD: 64.7 ± 4.1 years) who had not engaged in any regular and systematic training program in the previous 12 months volunteered for this study after completing an ethical consent form. The subjects volunteered for the present investigation following announcements in a widely read local newspaper. The subjects were carefully informed about the design of the study, and special information was given regarding the possible risks and discomfort related to the procedures. Subsequently, the subjects were randomly assigned and placed into two groups: strength training prior to endurance training (SE, n=13) or endurance training prior to strength training (ES, n=12). Concealment was guaranteed by a researched who was blinded with respect to participants. The sample size was calculated using the G POWER software (version 3.0.1), which determined that a sample of n=13 subjects would provide a statistical power of over 0.85 for all variables. Eight subjects (66.0 ± 2.7 years) were evaluated twice before the start of training (weeks –4 and 0).
The exclusion criteria included any history of neuromuscular, metabolic, hormonal and cardiovas-cular diseases. The subjects were not taking any medications that could influence hormonal or neuromuscular metabolism. The subjects were advised to maintain their normal dietary intake throughout the study. Medical evaluations were performed using clinical anamnesis and an effort electro-cardiograph (ECG) test to ensure each subject’s suitability for the testing procedure. The physical characteristics of the subjects are shown in Table 1. Body mass and height were measured using an Asimed analog scale (resolution of 0.1 kg) and an Asimed stadiometer (resolution of 1 mm), respectively. Body composition was assessed using the skinfold technique. A seven-site skinfold equation was used to estimate body density (26), and body fat was subsequently calculated using the Siri equation (27). The subjects’ characteristics are shown in Table 1.
Peak Oxygen Uptake, Ventilatory thresholds and Maximal workload
The subjects performed an incremental test on a cycle ergometer (Cybex, USA) to determine their peak oxygen uptake (VO2peak), second ventilatory threshold (VT2), maximal workload (Wmax), and cycling economy at 25, 50, 75 and 100 W. We chose to assess the metabolic economy at intensities up to 100 watts to guarantee that all our subjects were able to complete these intensities before and after training. During the test, the subjects initially cycled with a 25 W load, which was progressively increased by 25 W every two minutes, while maintaining a cadence of 70-75 rpm until exhaustion. The test was finished when the subjects were no longer able to maintain a cadence of 70 rpm. All the incremental tests were conducted in the presence of a physician. The participants were instructed to not to perform vigorous physical activity 24 h before the test, not to consume any stimulant beverages (i.e., with caffeine) and to sleep at least 8 h the night before the test. Expired gas was analyzed breath by breath using a metabolic cart (CPX/D, Medical Graphics Corporation, St. Paul, MN). VT2 was determined using the second breakpoint in the ventilation using an intensity curve and corresponded to the point of exponential increase in the ventilation in relation to the load (25). In addition, to confirm the data, VT2 was determined using the CO2 ventilatory equivalent (VE/VCO2). The maximum VO2 value (mL·kg-1·min-1) obtained close to exhaustion was considered the VO2peak. Wmax (watts) was calculated using the formula Wmax= Wcom+(t/120).ΔW, in which Wcom was the load at the last stage completed, t was the time at the last incomplete stage and ΔW was the load increment in the last stage (25 watts) (2). The cycling economy at each intensity was determined as the average oxygen consumption during the entire stage (i.e., two minutes) (15). The maximum test was considered valid if at least 2 of the 3 following criteria were met: 1) the maximum heart rate predicted by age was reached (220 - age); 2) the cadence of 70 rpm was not maintained; and 3) an RER greater than 1.1 was obtained. Three experienced, independent physiologists deter-mined the corresponding points. For the data analysis, the curves for exhaled and inhaled gases were smoothed by visual analysis using the software Cardiorespiratory Diagnostic Software Breeze Ex version 3.06. Heart rate (HR) was measured using a Polar monitor (model FS1, Kempele, Finland). The test-retest reliability coefficients (ICC) ranged from 0.85 to 0.88 for all the cardiorespiratory and workload variables.
Determination of responders and non-responders
Responsiveness to concurrent training was determined using the typical error criteria (19, 21). Eight participants in this study completed the maximal endurance test on a cycle ergometer twice before the start of the concurrent training intervention to determine the typical error in the VO2max and Wmax. The typical error (TE) of measurement was calculated using the equation TE = SDdiff/√2, in which SDdiff is the standard deviation of the difference scores observed between the 2 tests performed (28). Non-responders for VO2max and Wmax were defined as subjects who failed to achieve an increase or decrease that was greater than two times the TE away from zero. A change beyond two times the TE indicates a high probability (i.e., 12 to 1 odds) that the response is a real physiological adaptation greater than might be expected to result from biological and/or technical variability (21, 29). The calculated typical error was 1.15 mL·kg-1·min-1 for VO2max and 8 watts for Wmax.
Concurrent training programs
The participants in the study performed both strength and endurance training in the same session three times a week on non-consecutive days. One group performed the strength training prior to the endurance training (SE), and the other group performed the endurance training prior to the strength training (ES). Prior to the intervention, the subjects completed two familiarization sessions to practice the exercises they would perform during the training period. The strength and endurance training programs have been previously described in detail (7, 25). The subjects performed nine exercises (bench press, inclined leg-press, seated row, knee extension, inverse fly, leg curl, triceps curl, biceps curl and abdominal exercises). During weeks one and two, the subjects performed two sets of 18-20 repetitions maximum (RM; i.e., the heaviest possible load was used for the designated number of repetitions; mean ± SD of relative load: 39.8 ± 7.4% of pre-training 1 RM), progressing to 15-17 RM (weeks 3-4; 48.3 ± 5.7% of pre-training 1RM). In weeks five to seven, the subjects performed two sets of 12-14 RM (64.1 ± 8.7% of pre-training 1RM), eventually progressing to three sets of 8-10 RM (weeks 8-10; 81.3 ± 12.3% of pre-training 1RM) and advancing to 6-8 RM (weeks 11-12; 93.1 ± 14% of pre-training 1 RM). The workload was adjusted when the repetitions performed were either above or below the number of repetitions established. All sets were performed until failure (29). The recovery time between sets was 90 to 120 seconds. The strength training sessions lasted approximately 40 minutes.
The endurance training was performed using a cycle ergometer at an intensity relative to the heart rate (HRVT2) corresponding to the VT2. During the first two weeks, the subjects cycled for 20 minutes at 80% of HRVT2, progressing to 25 minutes at 85-90% of HRVT2 during weeks five to six. During weeks seven to ten, the subjects cycled for 30 minutes at 95% of HRVT2, and in the last two weeks of training, the subjects performed six four-minute bouts at 100% of HRVT2 (weeks 11-12) with one minute of active recovery between bouts. VT2 was used as a parameter to prescribe the intensity of endurance training; it corresponded to 73.8 ± 4.9% of the VO2peak. All the training sessions were carefully supervised by at least three experienced personal trainers.
Statistical Analysis
The SPSS statistical software package was used to analyze the data. Normal distribution and homogeneity parameters were checked using Shapiro-Wilk and Levene tests, respectively. The results are reported as the mean ± SD. Statistical comparisons during the control period (from week –4 to week 0, n=8) were performed using Student’s paired t-tests. The effects of training were assessed using a two-way analysis of variance (ANOVA) with repeated measures (group x time). Selected relative changes between groups were compared via a one-way ANOVA. The effect size (ES) between pre and post training for each group was calculated using Hedges’ effect size based on the following formula:effect size = (Mpost - Mpre)/SDpre, where Mpost is the mean post-training measure, Mpre is the mean pre-training measure for each group, and SDpre is the SD of the pre measurements (30). Threshold values for assessing the magnitude of standardized effects, which are a fraction or multiple of the baseline standard deviation, were 0.20, 0.60, 1.2 and 2.0 for small, moderate, large and very large, respectively (31). The retrospective statistical power provided by SPSS after analysis was 1.00 for all variables in which a significant time-effect was observed. Statistical significance was accepted when p<0.05.

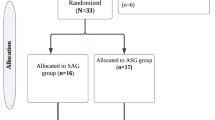
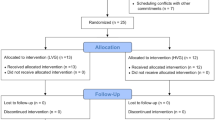
Flowchart for screening, recruitment, allocation and intervention
Results
Of the 39 elderly who were approached, 30 agreed to participate in the trial. From the initial sample of 30 elderly who volunteered to take part in this study and met the inclusion criteria. Five subjects dropped out due to reasons like change of address to a different city (2) or related to professional reasons (3). Twenty-five elderly men completed the pre- and post-measurements (SE group: n=13; and ES group: n=12) (Figure 1).
During the control period (i.e., between week -4 and week 0), no significant changes were observed in VO2peak (28.7 ± 3.8 vs. 27.6 ± 3.6 mL·kg-1·min-1.) and Wmax (129.0 ± 20.0 vs. 130.7 ± 21.3 watts). At baseline, there were no differences between the groups in body mass (kg), height (cm), age (years) and body fat percentage (%). Additionally, VO2peak and Wmax, absolute and relative VT2, and cycling economy at 25, 50, 75 and 100 W did not statistically differ between the two groups (Figures 1 and 2).
Maximal aerobic performance (i.e., VO2peak and Wmax) are shown in Table 1. Throughout the train-ing period, similar increases (P<0.001) in the VO2peak in SE (27.4 ± 6.1 vs. 29.5 ± 6.6 mL·kg-1·min-1., effect size: 0.34) and ES (26.6 ± 6.9 vs. 28.8 ± 6.5 mL.kg.min-1, effect size: 0.33) were found, with no differences between groups (SE: 8.1 ± 9.9%; ES: 9.3 ± 9.8%). In addition, significant increases were observed in Wmax in SE (121.0 ± 13.4 vs. 143.9 ± 19.8 W, effect size: 1.71) and ES (125.2 ± 40.8 vs. 155.3 ± 44.0 W effect size: 0.74), with no difference between groups (SE: 19.9 ± 19.3%; ES: 24.1 ± 24.0%).

Physical characteristics cardiorespiratory fitness before and after training. Mean ± SD
There were no significant differences in the relative and absolute VO2 at 25, 50 and 75 W after training in both the SE and ES groups. However, after training, significant reductions were observed in the absolute VO2 at 100 W (P<0.05, effect size: 0.37 and 0.48 for SE and ES, respectively) in SE and ES, with no differences between groups (Figure 2). In addition, there was a strong trend toward significant differences in the relative VO2 at 100 W (P=0.058, effect size: 0.38 and 0.35 for SE and ES, respectively) in the SE and ES groups, with no differences between groups (Figure 3). After training, all the absolute loads performed during incremental test (i.e., 25, 50, 75 and 100 watts) represented significantly less relatively to Wmax (P<0.001), with no differences between SE and ES (Table 2).
The inter-individual variability results are shown in Figures 3 (VO2peak) and 4 (Wmax). Regarding VO2peak, the ES group presented 10 responders and 2 non-responders (16.6%), while the SE group presented 8 responders and 5 non-responders (38.4%). Regarding Wmax, the ES group presented 9 responders and 3 non-responders (25%), while the SE group presented 8 responders and 5 non-responders (38.4%) for this variable. In Wmax, both the ES and SE groups included 1 subject whose scores were close enough to be considered a responder (i.e., 2 watts less than two times the typical error). In the ES group, only one subject did not respond positively on both VO2peak and Wmax (8.3%). Regarding the SE group, 4 subjects did not respond positively on both VO2peak and Wmax (30.7%).

Mean ± SD of absolute oxigen uptake (VO2) (L.min-1) pre and post 12 weeks of concurrent training. SE, strength prior to endurance training; ES, endurance prior to strength training

Mean ± SD of relative oxigen uptake (VO2) (mL·kg-1·min-1) pre and post 12 weeks of concurrent training. SE, strength prior to endurance training; ES, endurance prior to strength training

Absolute loads relative to maximal power at cycle ergometer (Wmax) characteristics cardiorespiratory fitness before and after training. Mean ± SD

Mean of individual absolute changes of relative maximal oxigen uptake (VO2peak) (mL·kg-1·min-1)

Mean of individual absolute changes of maximal workload at cycle ergometer (Wmax) (Watts)
Discussion
The main finding of the present study was that both intrasession exercise orders during concurrent training led to improved cycling economy at the highest intensity assessed (i.e., 100 W, which corresponded to 70.2 ± 15.6% of the Wmax after training). In addition, both concurrent endurance and strength training regimes led to similar enhancements of peak oxygen consumption and maximal workload during an incremental cycling ergometer test. Hence, the present study indicates that concurrent training improves maximal and submaximal aerobic performance in healthy elderly men irrespective of the exercise order. However, when considering individual responses, the ES group presented greater responsiveness since only 1 subject did not respond positively in terms of both VO2peak and Wmax, whereas 4 subjects did not respond positively in the SE group.
Concurrent strength and endurance training typically lead to similar improvements in maximal aerobic performance (i.e., VO2peak) compared with endurance training alone in elderly populations (8, 9, 11-13, 25). Furthermore, changes in the maximal aerobic capacity do not differ when endurance training is preceded by strength training or vice versa (14). Previous studies have shown that strength and power development may improve metabolic cost at submaximal intensities during aerobic exercise (3) and during activities of daily living (10). Interestingly, in the present study we observed a significant reduction in the absolute oxygen consumption at 100 watts (corresponding to 85.6 and 70.2% of Wmax before and after training, respectively) and a statistical trend toward significant reductions in relative oxygen consumption at the same intensity. However, it is unclear why our subjects were not able to improve the economy of their movement at lower intensities. The changes may have been observed only at the highest intensity because the subjects performed at a high-intensity during the strength (i.e., 14 - 6 RM) and endurance (90 - 100% of anaerobic threshold) training during the latter half of the training program. As we have previously shown (14), after a concurrent training period in health elderly men, cycling power at the second ventilatory threshold ranges from approximately 100 to 150 watts, which indicates that the subjects performed a major part of their training close to 100 watts and as a result, the changes were more prominent. This result agrees with the specificity principle of training.
Increased exercise economy has typically been attributed to earlier findings showing that an increase in maximal strength leads to a larger recruitment of type I fibers for the same submaximal load, adjustments in firing rate, and/or better muscular coordination and therefore better mechanical efficiency, subsequently reducing oxygen consumption for the same submaximal intensity (2, 3, 10). In fact, it has previously been shown that after 12 weeks of concurrent training, elderly subjects reduced their electromyographic (EMG) activity when performing at submaximal intensities during cycling exercise (i.e., neuromuscular economy), which also suggests a reduction in the recruitment of type II fibers (32). Moreover, in the present study, absolute rather than relative workloads were used to investigate exercise economy. Thus, the observed changes in the economy may simply be the result of a training-induced increase in the maximal workload and, therefore, a lower % of activated motor units at submaximal exercise intensities (2, 3, 10, 25). The absence of changes at lighter intensities could also be explained by the fact that at these intensities, subjects were sufficiently economical because many typical activities of daily living occur at these intensities (10). However, this explanation should be further investigated and remains to be elucidated. An improvement on metabolic economy at submaximal effort has an important clinical consequence: if older subjects are metabolically more economic during daily living activities, it means that the cardiovascular responses to a such effort will be lower and consequently, the cardiac risk will be also lower. Furthermore, it also means that elderly can displace/lift the same load with the same meta-bolic cost compared to the pre training condition. This result could be especially important to elderly individuals with decreased ability to perform daily living activities. However, the feasibility of the training regimens used in the present study and its adaptations should be further investigated in elderly with impaired functional capacity before to extrapolate these findings.
Interestingly, in the present study, no difference in metabolic economy was observed between different intra-session exercise orders during concurrent training. These results are partially in agreement with those from of Schumann et al. (15), who demonstrated a reduction in submaximal oxygen consumption on a cycle ergometer after concurrent training performed in both exercise orders in young men after 24 weeks of training, but not after 12 weeks. However, the subjects in the previous study were physically active and, as such, accustomed to cycling exercise. This discrepancy can be explained by different exercise intensities, the initial training status of the subjects and the different ages of their subjects and ours (i.e., young versus elderly men).
Studies using endurance training in adults have described the occurrence of interindividual variability in response to its stimuli in performance variables, such as VO2max and Wmax (16, 21, 24). In addition, it seems that the same is observed when endurance training is performed simultaneously with strength training (i.e., concurrent training) (20). More recently, it has been shown that under the same HIIT or resistance training regimens or under different health status conditions, there are similar and different prevalences of NRs (i.e., percentage of NR cases) defined by improved anthropometric, cardiovascular, metabolic and performance variables in adults (19). The present study has shown that while ES and SE increased similarly to VO2peak and Wmax, at the group level, there was a higher responsiveness in the maximal endurance performance in ES group considering VO2peak (16 vs. 38% for ES and SE, respectively) and Wmax (25 vs. 38% for ES and SE, respectively). This finding may suggest that some individuals who are exposed to both strength and endurance training in the same training session may experience impaired endurance performance when endurance training is preceded by strength training. This phenomenon can be explained by the acute effect phenomena related to peripheral or central fatigue resulting from the first modality of concurrent training session (33). Indeed, it has been shown in young subjects that different strength training protocols may impair endurance performance when the latter is performed immediately before the former exercise (34). Notwithstanding, previous studies have confirmed the hypothesis that individuals may be more sensitive to a given exercise protocol and may not respond to a different one (18, 21, 35). In this case, the mechanisms underlying individual variability could be different peripheral adaptations, such as different changes in skeletal muscle oxidation capacity, glycogen content and different fiber-type predominance between groups (36) as well as different central adaptations (37). Nevertheless, because we did not use a cross-over design in the present study, we could not verify this hypothesis. It should also be stated that the use of two times the typical error to define our subjects as responders or non-responders may have led to greater incidences of nonresponders since this method is considered as very conservative (21, 28) compared with other methods (35, 38). However, it should be noted that some individuals who did not respond in some physical manner after 12 weeks had a positive response after longer period of training (i.e., 24 weeks) (39) or after the training frequency was increased (40).
The present study has some limitations. First, there was an absence of an assessment of cycling economy at intensities higher than 100 watts. However, we chose to assess the metabolic economy at intensities of up to 100 watts to guarantee that all our subjects were able to complete these intensities before and after training. In addition, we only assessed the inter-individual variability in maximal endurance adaptations, and not the individual response in submaximal endurance. Moreover, we did not perform a cross-over design in the present study, and therefore, we cannot conclude whether the differences in the subjects’ responsiveness between ES and SE groups were based on individual sensitiveness or different training regimens. Future studies with a cross-over design are required to confirm if the different prevalence of nonresponders observed is due to an individual sensitiveness or due to the different concurrent training regimens. On the other hand, our results expand the knowledge regarding the effects of different intra-session exercise orders during concurrent training in maximal and submaximal aerobic performance in healthy elderly. The key-findings of the study are presented in the Box 1.

Key-findings of the study
In summary, concurrent strength and endurance training performed three times a week improved cycling economy at a greater intensity (i.e., 100 watts) independent of intra-session exercise orders; and, similar improvements in the maximal aerobic power were noted. From a practical standpoint, to improve maximal and submaximal endurance capacity, concurrent training can be performed in either strength-endurance and endurance-strength exercise orders in healthy elderly men. However, based on individual responses, it can be concluded that ES order may induce greater responsiveness in the maximal endurance performance, and this result should be strongly considered when prescribing concurrent training in elderly men.
Acknowlegments: The authors thank specially to CAPES and CNPq Brazilian Government Associations for its support to this project. The authors also are indebted the Spanish Net on Aging and frailty; (RETICEF)] (FEDER) and Centro de Investigación Biomédica en Red (CIBER) en Fragilidad y Envejecimiento Saludable (CIBERFES; CB16/10/00315) del Instituto de Salud Carlos III, (FEDER), respectively. We also gratefully acknowledge to all the subjects who participated in this research and made this project possible.
Conflict of interest: The authors do not have any conflict of interest to disclose.
Ethical Standards: The authors declare that the study’s procedures comply with the current laws of the country in which it was performed.
References
Fleg JL, Lakatta G. Role of muscle loss in the age-associated reduction in VO2max. J Appl Physiol 2009;65:1147–1151.
Izquierdo M, Hakkinen K, Antón A, Garrues M, Ibañez J, Ruesta, M, Gorostiaga EM. Maximal strength power, endurance performance, and serum hormones in middleaged and elderly men. Med Sci Sports Exer 2001;33:1577–1587.
Izquierdo M, Hakkinen K, Ibanez J, Anton A, Garrues M, Ruesta M, Gorostiaga EM. Effects of strength training on submaximal and maximal endurance performance capacity in middle-aged and older men. J Strength Cond Res 2003;17:129–139.
Aagaard P, Suetta C, Caserotti P, Magnusson SP, Kjaer M. Role of the nervous sys-tem in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports 2010;20:49–64.
Blair SN, Kampert JB, Kohl 3rd HW, Barlow CE, Macera CA, Paffenbarger RS Jr, Gibbons LW. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 1996;276:205–210.
Farrell SW, Finley CE, Haskell WL, Grundy SM. Is there a gradient of mortality risk among men with low cardiorespiratory fitness? Med Sci Sports Exerc 2014;47:1825–1832.
Cadore, EL, Pinto RS, Alberton CL, Pinto SS, Lhullier LFR, Tartaruga MP, Correa CS, Al-meida APV, Silva EM, Laitano O, Kruel LFM. Neuromuscular economy, strength and endurance in healthy elderly men. J. Strength Cond. Res 2011;25:997–1003.
Karavirta L, Häkkinen A, Sillanpää E, Garcia-Lopez D, Kauhanen A, Haapasaari A, Alen, M, Pakarinen A, Kramer WJ, Izquierdo M, Gorostiaga EM, Häkkinen K. Effects of combined endurance and strength training on muscle strength, power and hypertrophy in 40-67-year-old men. Scand. J. Med. Sci. Sports 2011;21:401–411.
Izquierdo M, Ibañez J, Häkkinen K, Kraemer WJ, Larrión JL, Gorostiaga EM. Once weekly combined resistance and cardiovascular training in healthy older men. Med Sci Sports Exerc 2004;36:435–443.
Hartman MJ, Fields DA, Byrne NM, Hunter GR. Resistance training improves meta-bolic economy during functional tasks in older adults. J Strength Cond Res 2007;21:91–95.
Wood RH, Reyes R, Welsch MA, Favaloro-Sabatier J, Sabatier M, Matthew Lee C, Johnson LG, Hooper PF. Concurrent cardiovascular and resistance training in healthy older adults. Med Sci Sports Exerc 2001;33:1751-1758.
Sillampää E, Häkkinen A, Punnonen K, Häkkinen K, Laaksonen DE. Effects of strength and endurance training on metabolic risk factors in healthy 40-65-year-old men. Scand J Med Sci Sports 19:885–895.
Holviala J, Häkkinen A, Karavirta L, Nyman K, Izquierdo M, Gorostiaga EM, Avela J, Korhonen J, Knuutila VP, Kraemer WJ, Häkkinen K. Effects of combined strength and endurance training on treadmill load carrying walking performance in aging men. J Strength Cond Res 2010;21:1583–1595.
Cadore EL, Izquierdo M, Alberton, CL, Pinto RS, Conceição M, Cunha G, Radaelli R, Bottaro M, Trindade GT, Kruel LF. Strength prior to endurance intra-session exercise se-quence optimizes neuromuscular and cardiovascular gains in elderly men. Exp Gerontol 2012;47:164–169.
Schumann M, Yli-Peltola K, Abbis CR, Häkkinen K. Cardiorespiratory adaptations during concurrent aerobic and strength training in men and women. PLoS One 2015. Doi: 10.1371/journal.pone.0139279.
Bouchard C, Rankinen T. Individual differences in response to regular physical activity. Med Sci Sports Exerc 2001;33:446–451.
Skinner JS, Jaskólski A, Jaskólska A, Krasnoff J, Gagnon J, Leon AS, Rao DC, Wilmore JH, Bouchard C. Age, sex, race, initial fitness, and response to training: The HERIT-AGE Family Study. J Appl Physiol 2001;90:1770–1776.
Sisson SB, Katzmarzyk PT, Earnest CP, Bouchard C, Blair SN, Church TS. Volume of exercise and fitness nonresponse in sedentary, postmenopausal women. Med Sci Sports Exerc 2009;41:539–545.
Alvarez C, Ramírez-Campillo R, Ramírez-Vélez R, Izquierdo M. Effects and Prevalence of Non-Responders after 12 weeks of High-Intensity Interval or Resistance Training in Adult Woman with Insulin Resistance: A Randomized Trial. J Appl Physiol 2017;122:985–996.
Karavirta L, Häkkinen A, Sillanpää E, García-López D, Kauhanen A, Haapasaari A, Alen M, Pakarinen A, Kraemer WJ, Izquierdo M, Gorostiaga E, Häkkinen, K. Effects of combined endurance and strength training on muscle strength, power and hypertrophy in 40-67-year-old men. Scand J Med Sci Sports 2011;21:401–411.
Bonafiglia JT, Rotundo MP, Whittall JP, Scribbans TD, Graham RB, Gurd, BJ. Inter-Individual variability in the adaptive responses to endurance and Sprint interval training: A randomized crossover study. PLoS One 2016. Doi:10.1371/journal. pone.0167790.
Bouchard C, Blair SN, Church TS, Earnest CP, Hagberg JM, Häkkinen K, Jenkins NT, Karavirta L, Kraus WE, Leon AS, Rao DC, Sarzynski MA, Skinner JS, Slentz CA, Rankinen T. Adverse metabolic response to regular exercise: is it a rare of common occurrence? PLoS One, 2012.doi: 10.1371/journal.pone.0037887.
Gurd BJ, Giles MD, Bonafiglia JT, Raleigh JP, Boyd JC, Ma JK, Zelt JG, Scribbans TD. Incidence of nonresponse and individual patterns of response following Sprint inter-val training. Appl Physiol Nutr Metab 2016;41:229–234.
Scharhag-Rosenberger F, Walitzek S, Kindermann W, Meyer T. Differences in adaptations to 1 year of aerobic endurance training: Individual patterns of nonresponse. Scand J Med Sci Sports 2012;22:113–118.
Cadore EL, Pinto RS, Lhullier FLR, Correa CS, Alberton CL, Pinto SS, Almeida AP, Tarta-ruga MP, Silva EM, Kruel LF. Physiological effects of concurrent training in elderly men. Int J Sports Med 2010;31:689–697.
Jackson AS, Pollock ML. Generalized equations for predicting body density of men. Brit J Nutr 1978;40:497–504.
Siri WE. Body composition from fluid spaces and density: analysis of methods. Nu-trition 1993;9:480–491.
Hopkins WG. Measures of reliability in sports medicine and Science. Sports Med 2000;30:1–15.
Izquierdo-Gabarren M, Expósito RGT, García-Pallarés J, Sánchez-Medina L, De Villarreal ES, Izquierdo M. Concurrent endurance and strength training not to failure optimizes performance gains. Med Sci Sports Exerc 2010;41:1191–1199.
Hedgess LV, Olkin I. Statistical methods for meta-analysis. 1st ed. Academic Press: Orlando FL p. 369, 1985.
Hopkins WG, S.W. Marshall SW, Batterham AM, Hanin J. Progressive statistics for studies in sports medicine and exercise Science. Med Sci Sports Exerc 2009;41:3–13.
Cadore EL, Pinto RS, Lhullier FLR, Correa CS, Alberton CL, Pinto SS, Almeida APV, Tar-taruga MP, Silva EM, Kruel LFM. Effects of strength, endurance and concurrent training on aerobic power and dynamic neuromuscular economy in elderly men. J Strength Cond Res 2011;25:758–766.
Baar K. Training for endurance and strength: Lessons from cell signaling. Med Sci Sports Exerc 2006;38:1939–1944.
Conceição M, Cadore EL, González-Izal M, Izquierdo M, Liedtke GV, Wilhelm EN, Pinto RS, Goltz FR, Schneider CD, Ferrari R, Bottaro M, Kruel LFM. Strength training prior to endurance exercise: Impact on the neuromuscular system, endurance performance and cardiorespiratory responses. J Hum Kinet 2014;44:171–181.
Ross R, de Lannoy L, Stotz PJ. Separate effects of Intensity and amount of exercise on interindividual cardiorespiratory fitness response. Mayo Clin Proc 2015;90:1–9.
Scribbans TD, Edgett BA, Vorobej K, Mitchell AS, Joanisse SD, Matusiak JB, Parise G, Quadrilatero J, Gurd BJ. Fibre-specific responses to endurance and low volume high intensity interval training: striking similarities in acute and chronic adaptation. PLoS One, 2014. Doi: 10.1371/journal.pone.0098119.
Montero D, Cathomen A, Jacobs RA, Flück D, de Leur J, Keiser S, Bonne T, Kirk N, Lundby AK, Lundby C. Haematological rather than skeletal muscle adaptations con-tribute to the increase in peak oxygen uptake induced by moderate endurance training. J Physiol 2015;593:4677–4688.
Astorino TA, Schubert MM. Individual responses to completion of short-term and chronic interval training: A retrospective study. PLoS One, 2014. Soi: 10.1371/ journal.pone.0097638.
Churchward-Venne TA, Tieland M, Verdijk LB, Leenders M, Dirks ML, de Groot LC, van Loon LJ. There are no nonresponders to resistance-type exercise training in older men and women. J Am Med Dir Assoc 2015;16:400–411.
Montero D, Lundby C. Refuting the myth of non-response to exercise training: ‘non-responders’ do respond to higher dose of training. J Physiol 2017 doi: 10.1113/ JP273480.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cadore, E.L., Pinto, R.S., Teodoro, J.L. et al. Cardiorespiratory Adaptations in Elderly Men Following Different Concurrent Training Regimes. J Nutr Health Aging 22, 483–490 (2018). https://doi.org/10.1007/s12603-017-0958-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-017-0958-4