
Abstract
The sternal foramen, usually an asymptomatic osteological defect, can lead to catastrophic consequences if not recognized prior to certain medical procedures. This study reports the prevalence of a sternal foramen in two South Amerindian populations compared with other published populations. We evaluated the presence of sternal foramina using thoracic computed tomography scans of 1334 (48% female) participants from two indigenous populations of Bolivia (n = 900 Tsimane, 434 Moseten). The prevalence of sternal foramina was compared to two U.S. populations of similar sex/age distribution (n = 572 Midwest Americans, 131 self-identified Native North Americans) via similar CT scans. A sternal foramen was significantly more common in the two Bolivian populations (prevalence ranging from 12.8 to 13.4%), compared to 4.4–5.1% in the two U.S. groups, consistent with prior estimates in studies from industrialized populations. Males had higher frequency of a sternal foramen compared to females in each of the four groups (OR = 1.904, 95% CI: 1.418–2.568, p < 0.001). Age was not associated with sternal foramen presence. These data show both a higher rate of sternal foramina in the South Amerindian populations versus comparator populations in North America and the highest rate of any studied living population. Although it is not possible to determine from our data the relative contribution of genetics versus early life or environmental causes to the higher rates of sternal foramen, we note that small prior studies have likewise demonstrated a higher prevalence in lower income countries. Further determination of the contributing factors warrants greater investigation and research.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
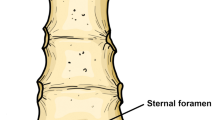
An oval defect in the body of the sternum is known as a sternal foramen (Fig. 1) and very rarely causes symptoms. However, when unrecognized, it can lead to severe injuries during certain medical procedures such as bone marrow aspiration, biopsy, or acupuncture of the sternum (Babinski et al. 2015, El-Busaid et al. 2012, Gkantsinikoudis et al. 2017, Gossner, 2013, Kirum 2017, Kuzucuoglu and Albayrak 2020, Turkay et al. 2017, Vulovic 2019, Yekeler et al. 2006). If not considered during imaging or autopsy examination, a sternal foramen can be misidentified as an osteolytic lesion or as the result of previous penetrating trauma (Babinski et al. 2015; El-Busaid et al. 2012; Gkantsinikoudis et al. 2017; Kirum 2017; Turkay et al. 2017; Yekeler et al. 2006). A sternal foramen results from an imperfect process of mesenchymal bands joining after growing circumferentially around the chest cavity to form ribs or in the subsequent chondrification and ossification of the mesenchymal tissue to form the sternal bone (Ashley 1956; Bayaroğulları et al. 2014; Choi et al. 2017; Cooper et al. 1988; Moore et al. 2020). The prevalence of a sternal foramen is generally reported to be between 4.5 and 8.4% in large autopsy and chest computed tomography (CT) scan studies from adults in industrialized countries (Gossner, 2013; Kuzucuoglu and Albayrak 2020; Peuker et al. 1999; Turkay et al. 2017; Vulovic 2019; Yekeler et al. 2006). Recently, the Tsimane Health & Life History Project (THLHP) and the HORUS Study Teams performed extensive evaluation, including chest CT scanning, of two genetically related South Amerindian populations, Tsimane and Moseten, both residing in central Bolivia (Kaplan 2017).

Volume-rendered CT scan image showing a sternal foramen in the body of the sternum in a Tsimane male participant
The Tsimane people live in remote villages without running water or modern sanitation and obtain over 90% of their food from small-scale horticulture, fishing, and hunting (Kraft et al. 2018; Gurven 2017). The Moseten previously lived a similar subsistence lifestyle as the Tsimane until the last half century as a result of greater infrastructure changes in the region they inhabit. Intensive exposure to Jesuit missionaries since the eighteenth century promoted integration of Moseten into broader Bolivian society; all Moseten speak Spanish (unlike Tsimane), are more market-integrated than Tsimane (with greater reliance on wage labor and consumption of market goods), and have access to indoor plumbing and electricity. While evaluating CT scans performed on these individuals for cardiovascular and pulmonary studies, we noticed the frequent occurrence of sternal foramina (Kaplan 2017). This observation motivated a more formal assessment of sternal foramina prevalence in these two Bolivian Amerindian populations. To contextualize the Bolivian results, we compare sternal foramina prevalence among patients from North America evaluated using similar CT methods.
Tsimane and Moseten are provocative study populations in the evaluation of sternal foramina prevalence and its contributing factors: the two populations are genetically related but vary in lifestyle and ecology. Although, the environment and nutrition of adult Moseten who are currently 40–90 years old was very similar to the Tsimane when they were in utero and small children, the current Moseten environment is intermediate between the traditional Tsimane lifestyle and urban industrialized populations and there is potential for maternal/postnatal nutritional deficits and diverse infections—each of which may affect growth (child) or maintenance (mother). The Tsimane and Moseten also both have overall low energy surplus (from high physical activity levels relative to consumption, and high parasite and pathogen load). Prior studies show compromised bone strength among Tsimane compared to industrialized populations (Stieglitz et al. 2014; Stieglitz 2019). This natural experiment provides the opportunity to evaluate whether early life environmental factors might ‘write the script’ for later life conditions and contribute to intergenerational patterns.
Materials and methods
Non-contrast, gated chest CT scans were performed as part of the THLHP on 900 Tsimane (48.4% female) and 434 Moseten (46.3% female) individuals (Kaplan 2017). The CT scans were initially performed for evaluation of coronary atherosclerosis, and after frequent sternal defects were noticed, all CT scans were systematically evaluated for sternal foramina. For a comparator population, 572 (49.8% female) patients who had self-referred for coronary calcium scoring at St. Luke's Mid-America Heart Institute (MAHI) of Kansas City and had undergone similarly performed gated chest CT scans were randomly selected from the MAHI database, and the CT images of the sternum for each patient were similarly reviewed for defects by the same physicians (BDG, ADN, RCT). Patients in this database did not have established coronary heart disease and were either self-referred for a screening coronary calcium score (≈ 65%), were referred for calcium score screening by their physician because of cardiac concerns such as a positive family history (≈ 10%), or the calcium score imaging was obtained as part of a diagnostic myocardial perfusion imaging examination ordered for possible cardiac symptoms (≈ 25%). This “Midwest American” population is a self-reported 89% white, 10% African American, and 1% Asian, with less than 1% Native American, roughly mirroring the population of the Kansas City metropolitan area. To compare a group that might be more genetically similar to the South Amerindians, we further searched the MAHI database and identified 131 patients (60.3% female) who self-identified as Native North American and had undergone CT coronary calcium scoring, and we included their images as another comparator group, labeled as “Native American” population.
The details of the gated CT scan acquisition for the Tsimane and Moseten populations are previously described (Kaplan 2017; Thompson 2005). In brief, Tsimane and Moseten subjects were transported by THLHP personnel from their villages to the regional town of Trinidad, Bolivia, where they underwent ECG-gated CT imaging from the apex of the lungs to just below the caudal edge of the heart on a GE Brightspeed 16 slice scanner (Milwaukee, WI, USA) (kV 120, variable mA, 2.5 mm thickness with 50% overlap) between July 2014 and October 2018. The North American comparator populations had undergone CT scanning for coronary calcium scoring using standard calcium scoring CT protocols similar to the protocol used for scanning the Tsimane and Moseten, generally on Siemens CT scanners (Erlangen, Germany) of various vintages. All images from the study population and the comparator population were reviewed on a Siemens Healthineers syngo.via workstation. The CT images of the sternum were examined on volume-rendered reconstructions and cross-sectional images by investigators (BDG, ADN, RCT) and all sternal defects were confirmed by re-review by the senior author (RCT). Sternal foramen was considered present if a complete anterior-to-posterior defect was identified on volume-rendered and multiplanar reformatted CT images that was greater than 2 mm in diameter.
Logistic regression models were used to assess the differences in sternal foramen prevalence between populations, while controlling for age and sex. All reported analyses were conducted in STATA 15.
This study was approved by the University of New Mexico and University of California, Santa Barbara human subjects review committees and by the Institutional Review Board of St. Luke’s Hospital of Kansas City. Written informed consent was obtained from all Tsimane and Moseten participants after having had the procedure and risks explained to them in their respective native language; approval was also granted at the village level, and by each tribal government (Gran Consejo Tsimane; Gran Consejo Regional Moseten). The radiation dose was low (≈ 2 mSv), and all the participants were mature adults (≥ 40 years).
The shape of the xyphoid process is extremely variable and details were not captured in this study. All uses of the phrase “sternal foramen” refer to a defect in the body of the sternum greater than 2 mm and do not reference any defects of the xiphoid process. No defects were observed in the manubrium.
Results
Table 1 shows prevalence of sternal foramina within our four studied populations, both as crude prevalence and prevalence based on sex. The pooled South Amerindian population combines the data from the Tsimane and the Moseten people, whereas the pooled North American population combines the data from the Native North American and Midwest American groups.
Overall, the odds ratio calculated per each population shows that the prevalence of sternal foramina is greater for males across populations examined controlling for age (OR = 1.904, 95% CI: 1.418–2.568, p < 0.001). Tsimane and Moseten have significantly higher crude prevalences of sternal foramen than Americans (ORTsimane vs. US = 2.682, 95% CI: 1.756–4.098, p < 0.001; ORMoseten vs. US = 2.853, 95% CI: 1.791–4.546, p < 0.001), controlling for age and sex. Compared to Native Americans, Tsimane and Moseten had significantly higher crude prevalences of sternal foramen (ORTsimane vs. Native American = 2.854, 95% CI: 1.225–6.650, p = 0.015; ORMoseten vs. Native American = 2.892, 95% CI: 1.210–6.914, p = 0.017).
Table 2 shows prevalence of sternal foramina in each population divided into age cohorts. Cohorts were assigned by decades after the youngest scanned participant (40 years) and combining all patients 70 years and greater into a single cohort to compensate for the reduced patient population in higher decades associated with age-related mortality.
There is no significant difference in sternal foramen prevalence between Tsimane and Moseten (Tables 1 and 2). In all studied groups, age was not associated with sternal foramen (Table 2), but male sex predicted higher odds (Table 1).
Discussion
Development of the sternum begins with the ventrolateral emergence of vertical mesenchymal bands, also referred to as the sternal bars, from the body wall (Moore et al. 2020). As the bars grow anteromedially around the forming chest cavity, they begin chondrification. By week ten of gestation, the two lateral cartilaginous sternal bars fuse craniocaudally along the anterior median plane, forming cartilaginous masses of the manubrium, sternobrae (segments of the sternal body), and xiphoid process. Within weeks prior to full-gestation birth, the cartilaginous sternal body (presternum) begins to form bilateral ossification centers which turn the soft cartilage structure into a hard calcified flat bone matrix. These paired ossification centers fuse within the sixth to twelfth year of life, and completely fuse vertically between the fused pairs by around the mid-second decade of life, forming a fully calcified sternum (Ashley 1956; Bayaroğulları et al. 2014; Choi et al. 2017; Cooper et al. 1988; Gumeler et al. 2019; Moore et al. 2020).
Formation of foramina in the sternum could result from two influences: an inherent decreased quantity of cartilaginous precursors (including an incomplete fusion of the cartilaginous lateral sternal bars) or a decreased capacity for the cartilaginous precursors to ossify (Ashley, 1956; Bayaroğulları et al. 2014; Choi et al. 2017; Cooper et al. 1988; Gumeler et al. 2019; Moore et al. 2020). Previous studies show Tsimane adult females have lower calcaneal and thoracic vertebral body mineral density than age-matched American adult females despite better cardiovascular health (Stieglitz et al. 2014; Stieglitz 2019). Additionally, the Tsimane do not enjoy the benefits of modern sanitation and have limited access to prenatal medical care; many pregnant Tsimane adult females may have suboptimal nutrition and/or vitamin and mineral deficiencies, including the documented average dietary calcium intake for both sexes being below 400 mg/day (Dinkel 2019; Kraft et al. 2018). The Moseten, although currently more acculturated than the Tsimane, likewise did not enjoy the benefits of modern sanitation or prenatal care 40–90 years ago when the adult participants in this study would have been small children or in utero. Although bone density results from multiple neuroendocrine and nutritional processes, the lowered bone density seen in the South Amerindians could be a contributing factor to their high prevalence of sternal foramen.
This is the largest study to date of sternal foramen prevalence, and in populations of different ancestry, and Table 3 shows relatively large individual reports from European populations and smaller series from African and South American populations. Evidence from the small studies in Brazil, Kenya, and Uganda show a higher prevalence of sternal foramen, all greater than 10% (Table 3). This finding is similar to the high prevalence rate found in our studied South Amerindian populations (13.0%). Conversely, the European studies in Germany, Greece, Turkey, and Serbia demonstrate a lower prevalence of sternal foramen, all less than 7% (Table 3). This finding is similar to the low prevalence rates fond in our studied North American (5.4%) and our Native American populations (4.4%). Furthermore, our Native North American population demonstrates the lowest recorded prevalence, and our South Amerindian populations show the highest sternal foramen prevalence of any studied population, among living populations and cadaveric populations reviewed (Table 3). Consistent with prior studies, we found that sternal foramina are more common in males than females (Choi et al. 2017; Gkantsinikoudis et al. 2017). This finding was the case in each of our subgroups and all prior studies (Table 3).
With all populations showing no significant difference in sternal foramen prevalence between the adult age cohorts (Table 2), we support the hypothesis that the sternum completes its formation and full ossification prior to the third decade of life, and that the influences affecting the sternal foramen formation occur in early life. It is not possible to determine from our current investigation whether the higher observed prevalence of sternal foramina in the Tsimane and Moseten is from a genetic variant or is related to in utero/early life environmental factors including high pathogen load and low energy surplus (Anderson 2019; Blackwell 2015, 2016; Hové 2020).
Limitations
As noted above, it is not possible to determine the extent of causality in the differences in prevalences between the studied groups are a result of genetics, early life environmental factors, or a combination/interaction of both. Using current data, we can only speculate the precise mechanisms of this sternal defect and its influences on the differing prevalences. Our data focused on a single, relatively common sternal defect (sternal body) and did not catalog the full extent of sternal variations within our subjects. We are not able to compare the prevalence of sternal defects in the subgroups of U.S. White, Black, and Hispanic populations because of incomplete information about exact ethnicity in the MAHI database.
This study evaluated only the presence or absence of a sternal foramen within participants. Further research into the causality of sternal foramen formation would include documenting the exact diameter, shape, and location of sternal foramen found in participants of this study for comparison to other published data of differing populations.
Beyond the location of the imaging health system, the precise ethnicity and local environment for published populations in Table 3 are ambiguous. This lack of specificity prevents accurate comparisons to our studied population based on both genetic and environmental influences. Precise demographic data of populations from full genomic sequencing would be necessary to begin definitive discussions as to the causality of a sternal foramen and the differing prevalences between published populations.
Due to cardiac screening being the intention for collecting our study CT images, the chest CT field of view was not wide enough to view any long bones or cranial bones of any participants (Kaplan 2017). Use of these data could have aided in comparing Harris lines or dental enamel hypoplasia to sternal foramen presence and provided definitive lifetime nutritional timeline data for each individual where census of information is unreliable or unavailable (Beom et al. 2014; Sheetal et al. 2013).
Conclusions
We found that two populations of South Amerindians, the Tsimane and Moseten, have a high prevalence of sternal foramen defects, i.e., much higher than Midwest North American, Native American, and all other large, published samples from diverse continents. The prevalence of sternal foramen is also substantially higher in males than females in all four populations examined. These data, combined with prior reports of higher prevalence of sternal foramina in relatively small series from lower income countries in Africa and South America, raise the possibility that this defect may be related to early environmental factors (potential candidates include prenatal nutrition and pathogen exposure), perhaps in additive or interactive fashion with genetic variation.
References
Anderson AS et al (2019) Old friends and friendly fire: pregnancy, hookworm infection, and anemia among tropical horticulturists. Am J Hum Biol 32(2):e23337. https://doi.org/10.1002/ajhb.23337
Ashley GT (1956) The relationship between the pattern of ossification and the definitive shape of the mesosternum in man. J Anat 90(1):87–105
Babinski MA, de Lemos L, Babinski MS, Gonçalves MV, De Paula RC, Fernandes RM (2015) Frequency of sternal foramen evaluated by MDCT: a minor variation of great relevance. Surg Radiol Anat 37(3):287–291. https://doi.org/10.1007/s00276-014-1339-x
Bayaroğulları H, Yengil E, Davran R, Ağlagül E, Karazincir S, Balcı A (2014) Evaluation of the postnatal development of the sternum and sternal variations using multidetector CT. Diagn Interv Radiol 20(1):82–89. https://doi.org/10.5152/dir.2013.13121
Beom J, Woo EJ, Lee IS, Kim MJ, Kim YS, Oh CS, Lee SS, Lim SB, Shin DH (2014) Harris lines observed in human skeletons of Joseon Dynasty, Korea. Anat Cell Bio 47(1):66–72. https://doi.org/10.5115/acb.2014.47.1.66
Blackwell AD et al (2015) Helminth infection, fecundity, and age of first pregnancy in women. Science 350(6263):970–972. https://doi.org/10.1126/science.aac7902
Blackwell AD et al (2016) Immune function in Amazonian horticulturalists. Ann of Hum Biol 43(4):382–396. https://doi.org/10.1080/03014460.2016.1189963
Choi PJ, Iwanaga J, Tubbs RS (2017) A comprehensive review of the sternal foramina and its clinical significance. Cureus 9(12):e1929. https://doi.org/10.7759/cureus.1929
Cooper PD, Stewart JH, McCormick WF (1988) Development and morphology of the sternal foramen. Am J Forensic Med Pathol 9:342–347. https://doi.org/10.1097/00000433-198812000-00016
Dinkel KA et al (2019) Relationship of sanitation, water boiling, and mosquito nets to health biomarkers in a rural subsistence population. Am J Hum Biol 32(1):e23356. https://doi.org/10.1002/ajhb.23356
El-Busaid H, Kaisha W, Hassanali J, Hassan S, Ogeng’o J, Mandela P (2012) Sternal foramina and variant xiphoid morphology in a Kenyan population. Folia Morphol (warsz) 71(1):19–22
Gkantsinikoudis N, Chaniotakis C, Gkasdaris G, Georgiou N, Kapetanakis S (2017) Morphological approach of the sternal foramen: an anatomic study and a short review of the literature. Folia Morphol (warsz) 76(3):484–490. https://doi.org/10.5603/FM.a2017.0006
Gossner J (2013) Relationship of sternal foramina to vital structures of the chest: a computed tomographic study. Anat Res Int. https://doi.org/10.1155/2013/780193
Gumeler E, Akpinar E, Ariyurek OM (2019) MDCT evaluation of sternal development. Surg Radiol Anat 41(3):281–286. https://doi.org/10.1007/s00276-019-02189-9
Gurven M et al (2017) The Tsimane health and life history project: integrating anthropology and biomedicine. Evol Anthropol 26(2):54–73. https://doi.org/10.1002/evan.21515
Hové C et al (2020) Immune function during pregnancy varies between ecologically distinct populations. Evol Med Public Health 1:114–128. https://doi.org/10.1093/emph/eoaa022
Kaplan H et al (2017) Native South American Tsimane have the lowest levels of coronary atherosclerosis ever reported. Lancet 389(10080):1730–1739. https://doi.org/10.1016/S0140-6736(17)30752-3
Kirum GG et al (2017) Anatomical variations of the sternal angle and anomalies of adult human sterna from the Galloway osteological collection at Makerere University Anatomy Department. Folia Morphol 76(4):689–694. https://doi.org/10.5603/FM.a2017.0026
Kraft TS, Stieglitz J, Trumble BC, Martin M, Kaplan H, Gurven M (2018) Nutrition transition in 2 lowland Bolivian subsistence populations. Am J Clin Nutr 108(6):1183–1195. https://doi.org/10.1093/ajcn/nqy250
Kuzucuoglu M, Albayrak I (2020) Topographic evaluation of sternal foramen patients with thoracic computed tomography. Surg Radiol Anat 42:405–409. https://doi.org/10.1007/s00276-019-02416-3
Moore KL, Persaud TVN, Torchia MG (2020) The developing human: clinically oriented embryology. Elsevier Inc, Amsterdam
Paraskevas G, Tzika M, Anastasopoulos N, Kitsoulis P, Sofidis G, Natsis K (2015) Sternal foramina: incidence in Greek population, anatomy and clinical considerations. Surg Radiol Anat 37(7):845–851. https://doi.org/10.1007/s00276-014-1412-5
Peuker ET, White A, Ernst E, Pera F, Filler TJ (1999) Traumatic complications of acupuncture: therapists need to know human anatomy. Arch Fam Med 8(6):553–558
Sheetal A, Hiremath VK, Patil AG, Sajjansetty S, Kumar SR (2013) Malnutrition and its oral outcome—a review. J Clin Diagn 7(1):178–180. https://doi.org/10.7860/JCDR/2012/5104.2702
Stieglitz J, Beheim BA, Trumble BC, Madimenos FC, Kaplan H, Gurven M (2014) Low mineral density of a weight-bearing bone among adult women in a high fertility population. Am J Phys Anthropol 156(4):637–648. https://doi.org/10.1002/ajpa.22681
Stieglitz J et al (2019) Computed tomography shows high fracture prevalence among physically active forager-horticulturists with high fertility. BMC Evol Biol eLife 8:e48607. https://doi.org/10.7554/eLife.48607
Thompson RC et al (2005) Clinical utility of coronary calcium scoring following non-ischemic myocardial perfusion imaging. J Nucl Cardiol 12(4):392–400. https://doi.org/10.1016/j.nuclcard.2005.04.006
Turkay R, Inci E, Ors S, Nalbant MO, Gurses IA (2017) Frequency of sternal variations in living individuals. Surg Radiol Anat 39(11):1273–1278. https://doi.org/10.1007/s00276-017-1854-7
Vulovic M et al (2019) Multidetector computed tomography (MDCT) estimation of prevalence and anatomic characteristics of sternal body foramen in population of central Serbia. Vojnosanit Pregl 76(2):186–191. https://doi.org/10.2298/VSP170321084V
Yekeler E, Tunaci M, Tunaci A, Dursun M, Acunas G (2006) Frequency of sternal variations and anomalies evaluated by MDCT. AJR Am J Roentgenol 186(4):956–960. https://doi.org/10.2214/AJR.04.1779
Acknowledgements
The authors thank the Tsimane and US participants, and the THLHP team for their relentless efforts. We also thank the HORUS Study Team for assistance in conducting the study.
Funding
The Tsimane Health and Life History Project (THLHP) is funded by the National Institute on Aging within the National Institute of Health (RF1AG054442 and 3RF1AG054442-02S2) and by National Science Foundation (1748282). RCT acknowledges funding from St. Luke’s Hospital Foundation of Kansas City. BCS1440212). JS acknowledges the Institute for Advanced Study in Toulouse (IAST) funding from the French National Research Agency (ANR) under grant ANR-17-EURE-0010 (Investissements d’Avenir program).
Author information
Authors and Affiliations
Consortia
Contributions
BDG: Data collection, data analysis, manuscript writing and editing; ADN: Data collection and data analysis; LJU: Manuscript writing and editing; BCT: Subject recruitment, data analysis, manuscript writing and editing; DKC: Data analysis, manuscript writing and editing; LSW: Data collection, data analysis, manuscript framing writing and editing; KRL: Data collection and manuscript editing; AM: Data collection and manuscript editing; DER: Data collection and manuscript editing; DEM: Data analysis and manuscript editing; CJR: Data collection and manuscript editing; CEF: Data gathering and critical manuscript editing; MLS: Data gathering and manuscript editing; JDS: Data gathering and manuscript editing; AHA: Data gathering and manuscript editing. JS: Subject recruitment, obtaining funding, data collection, and manuscript editing; MG: Protocol/project development, obtaining funding, data collection, and manuscript editing; HK: Protocol/project development, obtaining funding, data analysis, and manuscript editing; GST: Study concept, data analysis, and manuscript editing; RCT: Protocol/project development, data collection, data analysis, and manuscript writing and editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by the University of New Mexico and University of California, Santa Barbara human subject review committees and by the Institutional Review Board of St. Luke’s Hospital of Kansas City.
Consent to participate
Written informed consent was obtained from all Tsimane and Moseten participants after the procedure and risks were explained to them in their respective native language, as well as from each village, and by the tribal governments (Gran Consejo Tsimane; Gran Consejo Regional Moseten). Radiation dose was low (≈ 2 mSv), and all participants were mature adults (≥ 40 years). Informed consent for the US patients was waived by the St. Luke’s Hospital IRB as the study was conducted by a retrospective chart review of existing medical records.
Consent for publication
The authors affirm that human research participants provided informed consent for publication of their data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gans, B.D., Neunuebel, A.D., Umbarger, L.J. et al. High prevalence of sternal foramina in indigenous Bolivians compared to Midwest Americans and indigenous North Americans (sternal foramina in indigenous Bolivians). Anat Sci Int 96, 517–523 (2021). https://doi.org/10.1007/s12565-021-00618-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12565-021-00618-7