
Abstract
Purpose
Childhood overweight and obesity is on the rise in China and in Chinese cities in particular. The aim of this study is to explore the extent of income differences in childhood overweight in Shanghai, China, and examine demographic, social, and behavioral explanations for these differences.
Methods
Using the 2014 Child Well-Being Study of Shanghai, China—a survey that included extensive contextual information on children and their families in China’s most populous city, prevalence rates and adjusted odds ratios of child overweight and obesity at age 7 were calculated by income tercile controlling for a wide variety of sociodemographic variables.
Results
District aggregate income increases the odds of child overweight/obesity, but only for boys. In contrast, rural hukou status was associated with lower odds of overweight/obesity for girls.
Conclusions
Boys at age 7 are more likely to be overweight and obese than girls. District income further increases this likelihood for boys, while rural hukou status decreases this likelihood for girls, suggesting that preferences for boys and thinness ideals for girls may play a role in the income patterning of childhood overweight and obesity.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Child overweight and obesity is a global health epidemic that has long-term consequences for healthcare costs and society’s overall well-being and productivity [1,2,3]. Overweight and obesity is commonly thought to be a public health concern for wealthy nations, and in particular, the well-documented case of the United States (U.S.) has led the way in the international obesity crisis. Yet, despite the fact that wealthy countries such as the U.S. and its peers have experienced stagnation or declines in the growth of child overweight and obesity in recent years [4], research on this global public health issue remains largely focused on these countries.
However, obesity is no longer a health concern reserved for wealthy nations. Childhood obesity is also becoming a substantial public health issue in middle-income countries such as China [5]—where historically, undernourishment has been a concern. Less is known about patterns in these middle-income countries as compared to wealthy nations. For example, recent studies suggest that rates of childhood overweight and obesity in China have been on a rapid incline in the past 15 years [6,7,8,9], with variation in patterns across rural and urban settings [9]. This documented increase in overweight/obesity coincides with the nutrition transition in developing low- and middle-income countries, where in recent decades, the transition from nutrition deficits to nutrition surpluses is at different stages [10]. Due to mixed development in these middle-income countries, and China in particular, it is difficult to establish exactly where Chinese children fit along the nutrition transition spectrum [11].
Thus, the accelerating increase in childhood overweight and obesity in China today is complicated by the current stage of the nutritional transition in this diverse country. Developing countries at earlier stages of the nutritional transition are more likely to have higher rates of overweight/obesity among high-income families than low-income families, as these families have access to high-calorie foods [12]. In countries at later stages of development, for example Mexico or Brazil, the socioeconomic (SES) pattern in overweight/obesity looks more like that of wealthy countries, where high-calorie foods are inexpensive and more likely to be available to low-income families [12]. In China, it is quite likely that these patterns are variable by the region of the country, so studies focusing on the whole country may exclude detail on important regional differences [13]. Complicating this picture is the variation between urban and rural settings in China, where residents of a city such as Shanghai are likely to have greater access to high-calorie foods. Rural areas of the country have lower incomes than urban areas—particularly as compared to Shanghai—with less variation in SES. Evidence also suggests that childhood overweight/obesity has increased more rapidly among high-SES families than low-SES families between 1991 and 2006, particularly in urban areas [11], yet little is known about the factors associated with SES differences in overweight and obesity among children in China today.
The increase in childhood obesity and the resulting chronic health conditions such as heart disease and diabetes coincides with the dramatic rise in the Chinese economic development [14]. Much of the country’s economic development has been concentrated in large urban cities [15], and importantly, these cities are also where the highest rates of childhood obesity have been concentrated [6, 7, 9, 16,17,18,19,20]. Due to the increase in overweight and obesity rates in urban areas, studies that focus on the determinants of childhood overweight and obesity in cities are warranted to understand the burgeoning obesity epidemic in China.
Due to the availability of body mass index measures in general public health data, many of the prominent studies on childhood overweight and obesity in China have focused on broad trends over time and general prevalence rates. In addition, often these studies provide only bivariate (e.g., bivariate relationship between urban and overweight/obesity or between gender and overweight obesity) rather than multivariate analysis, which limits the thorough examination of the different sociodemographic predictors of child overweight and obesity. Most studies also use data that is now almost a decade old. This study takes advantage of the new 2014 Child Well-Being Study of Shanghai, China—a survey that included extensive contextual information on children and their families in China’s most populous city—to systematically examine the disparities in and determinants of childhood overweight and obesity in this rapidly changing city in this developing country. The focus on a specific city is the strength of this study, as the different stages of the nutrition transition throughout China do not complicate our analysis. Our primary research questions are as follows: (1) To what extent are socioeconomic differences in childhood overweight and obesity in early childhood present in Shanghai in 2014, and (2) What are the demographic, social, and behavioral factors that are related to overweight and obesity for these children?
Methods
Data
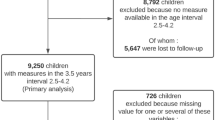
In this study, we used the 2014 Child Well-Being Study of Shanghai, China—a study modeled on child cohort studies in the United States. The Child Well-Being Survey was collected and managed by the New York University-East China Normal University (NYU-ECNU) Institute for Social Development at NYU Shanghai and received appropriate ethics approval through NYU [21]. Using a convenience sampling design, in the spring of 2014, we sampled seven districts in Shanghai, China. The selection of these specific seven districts was to ensure the data would include equal representation of children from a range of socioeconomic (SES) backgrounds. We used a convenience sampling strategy to sample between one to five schools from each of the seven districts totaling 17 schools and 73 classrooms with a total sample of 2280 first-grade children (average age, 7). Questionnaires were distributed through schools with permission from school administrators and parents. Parents, classroom teachers, and school administrators filled out different sets of questionnaires collecting detailed information on family background, family and school environments, parenting/children behaviors, and parent/children health status [21]. The response rate was 96% for parents and 100% for teachers and school administrators. All variables in our analysis are primary parent’s reports. Our outcome variable of interest, body mass index (BMI) was measured for 1629 children. Our final sample sizes for complete case (dropping cases with missing values on all independent and dependent variables) was 965 and was 1629 using multiple imputation ((MI) detailed below).
Measures
Body Mass Index
BMI was measured by child weight in kilograms divided by the square of height in centimeters. We used the International Obesity Task Force measure for Asia (IOTFA) as the primary measurement of childhood overweight and obesity [22]. The IOTFA measure specifies cutoff points for overweight and obesity based on cross-national BMI data, and this measure is useful for the purpose of country-level and cross-national comparisons focusing on Asian countries [23]. For the analysis, we focused on children designated overweight or obese. We also conducted sensitivity analyses using the measure established by the Centers for Disease Control and Prevention (CDC) using the 85th and 95th BMI percentiles to define childhood overweight and obesity, as well as the measure developed by the Working Group on Obesity in China (WGOC) based on Chinese samples aged 7 to 18 years [24, 25].
Socioeconomic Status
Our primary measure of SES was family income in terciles. Total family income was first adjusted by family size using the Organisation for Economic Co-operation and Development (OECD) square root equivalency scale [26]. Then the adjusted annual family income was categorized into low-, middle-, and high-income groups according to the cutoff points of the income distribution. These cut points were as follows: (1) low income: less than 50,000 renminbi (RMB) or (≈ US$7580); (2) middle income: between 50,000 and 92,376 RMB (≈ US$14,000); and (3) high income: more than 92,376 RMB. Parental education was measured by parents’ highest level of education (whether it is the mother or the father), classified into four groups: less than high school, high school degree, some college, and college or higher.
China uses an official household registration system to document household geographic information. This registration is called hukou status and is used to distinguish between urban and rural origins, as those with rural hukou status living in Chinese cities do not have full access to resources that are available only to residents holding urban hukou status—including education [27]. Our first-grade cohort, however, had access to schools because Shanghai has implemented a policy reform that incorporates migrant children into the public school system since 2008 [28]. We used a dichotomous variable indicating whether a family’s original residential area was urban or rural. Finally, school district SES was included to account for resource availability that may vary by districts/neighborhoods [29]. We categorized the school districts into high-, middle-, and low-income district terciles based on the sample distribution (bottom-third of the sample distribution, middle-third of sample distribution, and top-third of sample distribution).
Covariates
We included a dichotomous measure of child sex. Birth order was characterized as first- versus higher-order birth. We included a measure of whether or not a grandparent resides in the home. Childcare arrangements before first-grade included the following categories: parent care, grandparent care, formal childcare, or other type of childcare. Health insurance was dichotomized as having any or no insurance. Child overall health status was based on a 5-point scale. We coded excellent, very good, and good health as good overall health and fair or poor health as poor overall health. We included a measure of unhealthy eating that added up the frequencies of consuming different types of unhealthy foods (including sweetened beverages, French fries, fast food, and candy, sweets, or salty snacks) during the past week of the interview. A high score indicates a high frequency of unhealthy food consumption. Finally, we categorized mother’s work schedule into not working, working standard daytime hours, and working nonstandard hours.
Analysis Plan
We used Stata SE 14 to calculate overweight and obesity prevalence based on the covariates of interest. Although our response rate was over 95% overall, missing information on certain variables was still high. Only a few covariates had more than 10% of respondents with missing values, with the exception of family annual income (39%). We used multiple imputation (MI) with 20 multiple imputed datasets using the chained equation (mi impute chained) command in Stata to address the issue of missing data on independent variables [30, 31]. Our multiple imputation model considers all analyzed variables in addition to all outcome variables. We used original unimputed values for our outcome variables, as suggested by the literature [32].
We then estimated models using logistic regression to calculate odds ratios for overweight and obesity by family income level and stratified by gender (presented as models 1–3 for girls and boys in Table 3). Previous research on childhood overweight and obesity has shown different patterns by gender, and China is no exception [4, 8]. We estimated all logistic regression models using clustered robust standard errors and multilevel modeling respectively, two approaches to adjusting standard errors by accounting for the correlation between observations in the same group [33]. In our study, children from the same district were likely to be more alike on a variety of characteristics than those from different districts. For example, children in districts further from central Shanghai were more likely to be from low-income, rural migrant families. We reported findings from the clustered robust standard errors instead of those from the multilevel modeling because the small number of districts (N = 7) may produce bias and inaccurate estimates in multilevel logistic regression models [34]. We present these results using multiply imputed data in Table 3.
Results
Table 1 presents the descriptive characteristics of the non-missing sample. More boys than girls were in our sample (54 vs. 46%). We found a very high prevalence of overweight and obesity in first-grade children in Shanghai, 45 and 19%, respectively. Contextually, when using the official CDC cut points, the overweight and obesity rates (33 and 15%, respectively, shown in Appendix Table 4) were on par with childhood averages in the United States [35]. About 29% of children were from a family with annual income less than 50,000 RMB. Since district income was categorized into terciles, the sample was evenly distributed across low-, middle-, and high-income school districts in Shanghai, though slightly more children lived in high-income school districts. Parents were relatively well-educated in the sample, and 48% of children had at least one parent with a college degree. Notably, about 28% of children were originally from rural areas. This is important for social benefits qualification and economic mobility as children living in Shanghai with rural hukou status may have limited access to social benefits. About 47% of children co-resided with their grandparents. The majority of children were the firstborn in family (89%), had health insurance coverage (81%), were in good health condition (87%), and had a mother with a standard daytime work schedule (69%). Children in the sample, on average, consumed unhealthy foods eight times during the past week of the interview.
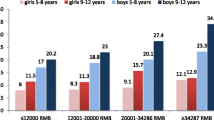
Table 2 presents overweight and obesity rates by gender and socioeconomic/behavioral characteristics. Girls were less likely to be overweight and obese than boys (40 and 49%, respectively). The prevalence of overweight was notably high among boys from high-income and middle-income families (50 and 51%) and high-income districts (56%). We also found gender differences in the prevalence of overweight and obesity by hukou status, general health status, and health insurance. For example, girls from urban areas were more likely to be overweight and obese than their rural counterparts, whereas boys showed a reverse pattern.
Table 3 presents results from the logistic regression analysis. The first model estimated odds ratios of overweight by considering family income only (model 1). The second model adjusted for hukou status and all the other family and individual covariates (model 2). The third model also included district income level in addition to the clustered standard error specified in all models. Odds ratios of the full models (Table 3, model 3) show that rural hukou status was significantly associated with lower likelihood of being overweight for girls (0.66, p < .05). For boys, the odds ratios of being overweight and obese were lower for children from low- or middle-income districts than for those from high-income districts (0.64, p < .001 and 0.80, p < .05, respectively). It is also worth noting that health insurance and parent-rated poor child health reduced the odds of being overweight or obese for boys.
We conducted multilevel logistic regression models to check the robustness of our findings from logistic regression models with clustered standard errors, and the results showed similar patterns. We ran sensitivity analyses using different cut points for overweight and obesity, and the results were similar (available upon request). We also tested interaction models with gender-district income and gender-hukou status. The results from the stratified models mirrored those from full sample models.
Discussion
Previous research has used public health data to highlight increasing rates of child overweight and obesity in China and includes some contextualization of these patterns. This paper used a new dataset, rich in covariates, to draw out the importance of SES patterns in Chinese child overweight and obesity in Shanghai. This study found that income at the district level mattered to childhood obesity in Shanghai, China—but only for boys. Boys from high-income districts were more likely to be overweight or obese than boys from low- or middle-income district families. The relationship between the district income and overweight and obesity for boys was statistically significant in all specified models and likely reflects the importance of the availability of high-calorie, and often fast food, diets available to families living in high-income areas in Shanghai. This finding is novel and warrants further investigation.
For girls, family and district income was not associated with overweight or obesity, though rural hukou status was associated with a lower risk of overweight/obesity. For girls in these families, lower body weight may reflect patterns found in rural parts of the country, where the nutritional transition may not be as advanced as it is in Shanghai [36]. The importance of hukou status may also be a proxy for a variety of other unobserved variables, for example, access to social and economic resources, which may matter for child weight.
Gender differences in overweight and obesity prevalence have been established in previous research, but less was understood about factors that may be driving these differences. China is one of a handful of countries with a growing obesity crisis, where there is a markedly higher rate of overweight and obesity among boys compared to girls [4]. The gender differences in the influence of district income on childhood overweight/obesity may be an artifact of boys’ higher overall likelihood of being overweight. Boys are more likely than girls to be overweight at all income levels, but the differences are largest for those in high-income districts. Alternatively, Chinese families may hold tight to traditional ideas about well-fed children representing wealth and health, and due to traditional gender preferences for boys, may only apply to families with male children [37]. Likewise, traditional ideas about slender girls may reach across the income spectrum, resulting in the lack of an income differential in overweight and obesity among girls in Shanghai. In fact, there is evidence that thinness ideals for females are more pronounced among those with high SES than those with low SES in China [38], and these attitudes may be driving some of the gender differences in childhood overweight and obesity.
In this study, a number of factors that have shown to be predictive of overweight and obesity in countries such as the United States, were not statistically significant in our Chinese sample. The factors that were important, such as district income, hukou status, and child health status, were variable by gender. These contextual factors are important to understand, and future research into the cultural norms shaping childhood overweight and obesity in Chinese cities would be an important development in the literature.
The finding that income—at the district level—increases the risk of overweight among boys in Shanghai, China suggests that despite high rates of childhood overweight and obesity, the patterning of overweight/obesity by SES in this sample reflects that of a low-GDP country [39]. Research shows that more developed countries show a reversal in the positive association between SES and overweight/obesity, which has not yet happened for children in Shanghai, China. This finding is important, given the rapid economic growth found in China’s most populous city.
In light of the contribution of this study, some discussion of limitations is necessary. While our data are innovative and include many contextual factors that have not been examined in relation to childhood obesity in China, it lacks the large sample size of public health data, so we are unable to stratify the sample beyond gender differences. We also had missingness on several of the variables of interest, namely family income. Yet, the results in both the complete case sensitivity analyses and multiple imputation analyses presented in Table 3 demonstrate that income, particularly measured at the district level, is an important predictor of childhood overweight and obesity for boys. Additionally, we were unable to control for parental BMI which may have important influence on the likelihood of children being overweight or obese. We did conduct sensitivity analysis to control for child’s low birthweight and the results were the same as those presented here. Our study provides an in-depth exploration of the determinants of childhood overweight and obesity in Shanghai—the largest and the fastest-growing city in China—but we cannot draw conclusions about rural regions of the country based on our findings. These results do warrant exploration of the determinants of childhood overweight and obesity in other Chinese cities, to confirm whether our results are generalizable across urban areas. Finally, we are focusing on a specific time in childhood, primary school entry at age 7, so we are unable to examine different patterns across childhood. As these children develop and become more influenced by school contexts and peers, future studies on these childhood contexts will be important in addressing this emerging public health concern.
Childhood overweight and obesity are rapidly increasing in China, and the rates in Shanghai appear to be on par with those found throughout the United States. Future research is needed to develop an understanding of the determinants of childhood overweight across the early life course and to parse out regional differences to understand this growing public health concern. As Chinese economic development continues expanding throughout the country, health and educational interventions for increasing childhood obesity are warranted.
References
Dietz W. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 1998;101(3):518–25.
Nader PR, O’Brien M, Houts R, et al. Identifying risk for obesity in early childhood. Pediatrics. 2006;118(3):E594–601. https://doi.org/10.1542/peds.2005-2801.
Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med. 1997;337(13):869–73. https://doi.org/10.1056/NEJM199709253371301.
OECD. Health at a glance, 2013. 2014; https://doi.org/10.1787/health_glance-2013-en.
Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25. https://doi.org/10.1080/17477160600586747.
Cui Z, Huxley R, Wu Y, Dibley MJ. Temporal trends in overweight and obesity of children and adolescents from nine provinces in China from 1991–2006. Int J Pediatr Obes. 2010;5(5):365–74. https://doi.org/10.3109/17477166.2010.490262.
Seo D, Niu J. Trends in underweight and overweight/obesity prevalence in Chinese youth, 2004–2009. Int J Behav Med. 2014;21(4):682–90.
Song Y, Wang H, Ma J, Wang Z. Secular trends of obesity prevalence in urban Chinese children from 1985 to 2010: gender disparity. PLoS One. 2013;8(1):e53069. https://doi.org/10.1371/journal.pone.0053069.
Song Y, Ma J, Wang H, et al. Secular trends of obesity prevalence in Chinese children from 1985 to 2010: urban-rural disparity. Obesity. 2015;23(2):448–53. https://doi.org/10.1002/oby.20938.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21.
He W, James SA, Merli MG, Zheng H. An increasing socioeconomic gap in childhood overweight and obesity in China. Am J Public Health. 2014;104(1):e14–22.
Monteiro C, Moura E, Conde W, Popkin B. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Organ. 2004;82(12):940–6.
Chen T, Modin B, Ji C, Hjern A. Regional, socioeconomic and urban-rural disparities in child and adolescent obesity in China: a multilevel analysis. Acta Paediatr. 2011;100(12):1583–9. https://doi.org/10.1111/j.1651-2227.2011.02397.x.
World Health Organization. China: health, poverty and economic development. Beijing: Office of the WHO Representative in China and Social Development Department of the China State Council Development Research Center; 2015.
Osnos E. Age of ambition: chasing fortune, truth, and faith in the new China. Macmillan. 2014;
Andegiorgish AK, Wang J, Zhang X, Liu X, Zhu H. Prevalence of overweight, obesity, and associated risk factors among school children and adolescents in Tianjin, China. Eur J Pediatr. 2012;171(4):697–703. https://doi.org/10.1007/s00431-011-1636-x.
Liu J, Ye R, Li S, et al. Prevalence of overweight/obesity in Chinese children. Arch Med Res. 2007;38(8):882–6. https://doi.org/10.1016/j.arcmed.2007.05.006.
Wang Y. Cross-national comparison of childhood obesity: the epidemic and the relationship between obesity and socioeconomic status. Int J Epidemiol. 2001;30(5):1129–36. https://doi.org/10.1093/ije/30.5.1129.
Yu Z, Han S, Chu J, Xu Z, Zhu C, Guo X. Trends in overweight and obesity among children and adolescents in China from 1981 to 2010: a meta-analysis. PLoS One. 2012;7(12):e51949. https://doi.org/10.1371/journal.pone.0051949.
Zhang M, Guo F, Tu Y, et al. Further increase of obesity prevalence in Chinese children and adolescents—cross-sectional data of two consecutive samples from the city of shanghai from 2003 to 2008. Pediatr Diabetes. 2012;13(7):572–7. https://doi.org/10.1111/j.1399-5448.2012.00877.x.
Han W-J, Wen J. Child well-being study, Shanghai, China. NYU_ECNU Institute for Social Development at NYU Shanghai; 2014. http://shanghai.nyu.edu/sites/default/files/media/ChildWellBeingStudy0908.pdf. Accessed 10 Mar 2015.
World Obesity Federation. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity in children. 2015. http://www.worldobesity.org/aboutobesity/child-obesity/newchildcutoffs. Accessed 3 Jul 2015.
Wang Y, Lim H. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int Rev Psychiatry. 2012;24(3):176–88. https://doi.org/10.3109/09540261.2012.688195.
Ji C. Cooperative study on childhood obesity, working group on obesity in China. Report on childhood obesity in China (1)—body mass index reference for screening overweight and obesity in Chinese school-age children. Biomed Environ Sci. 2005;18(6):390–400.
Ji C. Cooperative study childhood obesity. The prevalence of childhood overweight/obesity and the epidemic changes in 1985–2000 for Chinese school-age children and adolescents. Obes Rev. 2008;9:78–81. https://doi.org/10.1111/j.1467-789X.2007.00443.x.
OECD. What are equivalence scales? 2011. http://www.oecd.org/eco/growth/OECD-Note-EquivalenceScales.pdf. Accessed 1 Sep 2015.
Wong K, Fu D, Li CY, Song HX. Rural migrant workers in urban China: living a marginalised life. Int J Soc Welf. 2007;16(1):32–40.
Lan P. Segmented incorporation: the second generation of rural migrants in Shanghai. China Q. 2014;217:243–65.
Yang S, Wang MYL, Wang C. Socio-spatial restructuring in Shanghai: sorting out where you live by affordability and social status. Cities. 2015;47:23–34. https://doi.org/10.1016/j.cities.2014.12.008.
White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–99.
Stata 12 Multiple-Imputation Reference Manual. College Station: Stata Press. 2011.
von Hippel PT. Regression with missing Ys: an improved strategy for analyzing multiply imputed data. Sociol Methodol. 2007;37:83–117.
Cheah BC. Clustering standard errors or modeling multilevel data. 2009. Retrieved from http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.169.6644
Moineddin R, Matheson FI, Glazier RH. A simulation study of sample size for multilevel logistic regression models. BMC Med Res Methodol. 2007;7:34. https://doi.org/10.1186/1471-2288-7-34.
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311(8):806–14.
Dearth-Wesley T, Wang H, Popkin BM. Under- and overnutrition dynamics in Chinese children and adults (1991–2004). Eur J Clin Nutr. 2008;62(11):1302–7. https://doi.org/10.1038/sj.ejcn.1602853.
Hesketh T, Lu L, Xing Z. The effect of China’s one-child family policy after 25 years. N Engl J Med. 2005;353(11):1171–6. https://doi.org/10.1056/NEJMhpr051833.
Luo Y, Parish WL, Laumann EO. A population-based study of body image concerns among urban Chinese adults. Body Image. 2005;2(4):333–45.
Pampel FC, Denney JT, Krueger PM. Obesity, SES, and economic development: a test of the reversal hypothesis. Soc Sci Med. 2012;74(7):1073–81.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
This article uses secondary data and is exempt from human participant protocols. The original data collection was approved through the Institutional Review Board at New York University.
Conflict of Interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
ESM 1
(PDF 10 kb).
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Martinson, M.L., Chang, YL., Han, WJ. et al. Child Overweight and Obesity in Shanghai, China: Contextualizing Chinese Socioeconomic and Gender Differences. Int.J. Behav. Med. 25, 141–149 (2018). https://doi.org/10.1007/s12529-017-9688-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-017-9688-6