
Abstract
Studies have shown that exposure to heavy metals increases the risk of osteoporosis in the elderly population and leads to fractures. However, epidemiologic studies focus on combined effects of multiple metals on bone strength among preschoolers are scarce. Therefore, this study was conducted to examine associations of multiple metals exposure with the risk of insufficient bone strength (IBS) among 1399 children aged 2–6 years in China. Urine concentrations of 23 metals were measured using an inductively coupled plasma mass spectrometer, while bone strength was assessed using a quantitative ultrasound instrument. The weighted quantile sum (WQS) and Bayesian kernel machine regression (BKMR) models were conducted to investigate the associations between exposure to metal mixtures and IBS. In the single metal exposure model, urine cobalt and zinc were identified to be negatively associated with IBS, whereas urine lead was positively associated with IBS. Furthermore, WQS regression and BKMR analyses consistently showed that exposure to metal mixtures was inversely related to IBS, and cobalt was the main contributor to the combined effects. Such associations were more evident in children aged 2–4 years. Our findings suggested that exposure to metal mixtures was associated with bone strength among children, and cobalt was the main contributor to the overall effects.
Graphical Abstract

Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Considerable evidence now exists that childhood and adolescence, which accumulate 50–80% of bone mass and bone strength in a person's life, is a critical period of bone development and plays a decisive role in the health of bones (Weaver et al. 2016). Low bone strength increases the risk of fracture in children, leading to an increased risk of osteoporosis (Hans et al. 2017). It is estimated that there will be 5.99 million patients with osteoporotic fractures by 2050 in China (Si et al. 2015). Although osteoporosis symptoms generally manifest in the elderly, the disease is thought to have roots at the beginning of childhood (Maggioli and Stagi 2017). It is essential to explore children's bone health and related factors, timely detection of bone strength, to reduce the risk of developing bone diseases.
Despite numerous factors, including genetic factors, physical activity, and dietary nutrition, are related to the development of bone strength (Di Marcello et al. 2022; Katerina and Fernando 2019; Moradi et al. 2018), environmental factors are increasingly recognized as significant contributors to bone health, especially metal exposure (Li et al. 2018; Rodriguez and Mandalunis 2018). Essential metals, including zinc and copper, play a crucial role as cofactors for enzymes that regulate bone metabolism. Imbalances in the levels of these metals can have adverse effects on bone integrity, as noted by Rodriguez and Mandalunis (2018). While heavy metals such as lead and cadmium are known to be detrimental to bone cells, primarily by impeding osteoblast differentiation, synthesis activity, and extracellular matrix mineralization. The imbalance in bone remodeling may potentially lead to the emergence of bone ailments, such as osteopenia and osteoporosis (Akesson et al. 2006). Additionally, heavy metals can accumulate in the extracellular bone matrix, causing severe harm even at low concentrations in cases of long-term metal exposure. Epidemiological and experimental studies have indicated environmental exposure to metals was associated with bone strength, such as Cd (Chung 2022; Kim et al. 2021), Cu (Qu et al. 2018), Se (Galvez-Fernandez et al. 2021; Wu et al. 2020), Pb (Jalili et al. 2020), Zn (Wang et al. 2021).
However, most metal-bone strength studies focused on subjects from the general adult population, post-menopausal women or men aged ≥ 50 years, and information about children is limited. In addition, existing studies only concerned associations of single-metal exposure with bone strength. Little is known about the overall health effect of joint exposure to multiple metals, while simultaneous exposure to various metals is more common than exposure to a single one. In recent years, the use of weighted quantile sum (WQS) regression and Bayesian kernel machine regression (BKMR) models has become widespread in epidemiology to analyze the independent and joint effects of multiple correlated exposures. These models enable us to dissect the relationship between exposure to multiple metals and bone strength.
Quantitative ultrasound, a radiation-free method that measures the speed of sound (SOS) along cortical bones, is increasingly being applied for the direct measurement of bone strength and the assessment of bone properties in children (Inose et al. 2006; Lequin et al. 2000). Hence, this study was performed to examine the single and overall effects of 23 heavy metals in urine on bone strength based on a cross-sectional study in Chinese children. We used the quantitative ultrasound method to measure the bone strength and inductively coupled plasma-mass spectrometry to measure the concentration of 23 metals in urine. The generalized linear model was conducted to investigate the relationship between exposure to single metal and insufficient bone strength (IBS). The WQS and BKMR models were applied to investigate the overall relationship and non-linear dose–response relationship between exposure to metal mixtures and IBS, as well as interactions between the meta. Interaction effects were conducted to further explore the association between exposure to metal mixtures and age on IBS based on a cross-sectional study in Chinese preschoolers.
Material and Methods
Study Population
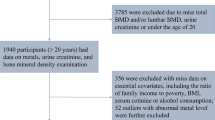
We used cluster sampling to investigate 7 kindergartens in Shiyan City, Hubei Province, China in 2019. A total of 1595 preschoolers aged 2–6 years old were included in the study. Briefly, an interviewer-administered questionnaire on demographic characteristics including basic information for children (e. g. sex, age, birth weight, birth status, feeding patterns, outdoor time, eating habits (fruit, vegetable, animal protein, milk and bean), etc.), parental smoking status and family income were gathered by trained interviewers. Guardians of children were asked to complete the questionnaire and provide morning urine specimens (5 mL). Physical examination including height and weight was performed by qualified physicians. Body mass index (BMI) was calculated as body mass / height2 (kg/m2). Overweight and obesity were defined by BMI using child growth standards established by the World Health Organization. After excluding those with unrecovered questionnaires (n = 50, a recovery rate of 96.87%), missing basic information (n = 110), missing physical examination (n = 27), insufficient urine samples (n = 9), a total of 1399 children were eligible for further analysis. The study was approved by the Ethics Committee of Hubei University of Medicine (2019-TH-80), and informed consent from guardians of children was obtained before completing the questionnaire.
Urinary Metal Measurements
Urinary concentrations of 23 metals (aluminum (Al), titanium (Ti), vanadium (V), chromium (Cr), manganese (Mn), iron (Fe), cobalt (Co), nickel (Ni), copper (Cu), zinc (Zn), arsenic (As), selenium (Se), rubidium (Rb), strontium (Sr), molybdenum (Mo), cadmium (Cd), tin (Sn), antimony (Sb), barium (Ba), tungsten (W), thallium (Tl), lead (Pb), uranium (U)) were measured using inductively coupled plasma-mass spectrometer (ICP-MS, Thermo Fisher, USA) based on a previously published protocol for the measurement of urinary metal concentrations with minor modifications (Heitland and Koster 2006). All the collected samples were sent to the laboratory within 4 h, and then stored at − 80 °C before further analysis. Before analysis, frozen urine samples were thawed at room temperature before centrifugation. A total of 200 μL of the supernatant was transferred to 5 mL polypropylene tubes and acidified with 40 μL nitric acid (Thermo Fisher, USA) at 4 °C overnight. The urine samples were allowed to stand at room temperature for 30 min the next day, brought to room temperature and diluted to 4 mL with butanol, and then centrifuged (3000 r/min, r = 20 cm, 10 min). The accuracy of ICP-MS was checked by analyzing multi-element reserve solution and internal standard liquid (United States), urinary sample quality controls (Sero, Billingstad, Norway)) and standard reference materials 1640a (Trace Elements in Natural Water, National Institute of Standards and Technology, Gaithersburg, MD) in every 50 samples. We further utilized a spiked pooled urine sample (100 samples randomly pooled together) as an inter-laboratory comparison to ensure the precise and accurate detection of titanium, iron, rubidium, strontium, molybdenum, barium, tungsten, uranium (no available certified reference agents). The standard recovery rate was in the range of 73.51–126.44% and the regression coefficients (r2) of the calibration standard solutions were greater than 0.999. The limits of detection (LOD) of each element were in the range 0.10–134.57 ng/L, which have been provided in a previous published study (Liu et al. 2022), and values below the LOD were given the value LOD/2.
Measurement of Bone Strength
The bone strength was performed by Omnisense7000p quantitative ultrasound instrument (Sunlight Medical Ltd. Israel). The middle tibia of the left leg of children under 3 years of age and the distal radius of the left upper limb of children over 3 years of age were measured by a trained operator. To classify bone strength in Asian children, the Sunlight Corporation has developed a system based on the percentage of SOS value. This system divides children into two categories based on their age and sex: normal bone strength (NBS, the percentage of SOS > 25%) and IBS (the percentage of SOS ≤ 25%) including mild (10–25%), moderate (3–10%) and severe (< 3%) IBS.
Statistical Analysis
Baseline characteristics were compared using t-tests or Mann Whitney U tests for continuous variables and chi-square tests for categorical variables. We used Spearman's rank correlation analysis to explore correlations between urine metal concentrations, after natural log-transformation to account for their right-skewed distributions. The generalized linear model was used to estimate odds ratios (OR) and 95% confidence intervals (CIs) for IBS among the participants and individual urine metals categorized into quartiles according to distributions. The lowest quartile was assigned to be the reference groups. Linear trend P-values were derived by modeling the median value of each metal quartile as a continuous variable in the regression model. Model 1 was adjusted for sex (boys, girls), age (continuous), BMI (continuous), birthweight (continuous), birth status (term birth or not), parents smoking (yes or no), family income(RMB) (< 4999, 5000–11,999 and > 12,000), and urine creatinine (continuous), and model 2 was further adjusted for outdoor time (< 2 h/d, ≥ 2 h/d), feeding patterns (breast feeding, mixed feeding, artificial feeding), calcium supplement (yes or no), vitamin D supplement (yes or no), eating habits (fruit, vegetable, animal protein, milk and bean) (< 7 times/week, ≥ 7 times/week).
WQS regression was applied to explore the effects of mixed metals exposure on IBS (Carrico et al. 2015). R package (“gWQS”) can empirically calculate the WQS index comprised of weighted sums of individual metal concentrations. The WQS index (ranging from 0 to 1) represented the mixed exposure level of metals, and the components of concern were identified by non-negligible weights. The final result was interpreted as the simultaneous effect on IBS of a one-quantile increase of mixed metals.
Besides, to account for possible non-linearity and interactions between multiple metals and IBS, we applied the BKMR model, which is a statistical method for a mixture of multiple metals and can flexibly simulate the combined effects of mixtures (Bobb et al. 2015). The R package “bkmr” (version 0.2.0, Bobb et al. 2018) was used to conduct the BKMR analysis. In the BKMR model, the outcome “IBS” denoted by Y, exposures “metals” denoted by X and the covariates denoted by Z. Binomial kernel function was chosen to establish this model running 10,000 iterations for model fit with default priors, of which as follows:
where the function h() is a dose–response function, which contains nonlinear and/or interactions between components, and Z = Z1,…, Zp are p covariates. Specifically, we computed the overall effect of multiple metals, by comparing the estimated value when other metals are at a particular quantile as compared to when all of them are at their 50th percentile. Then we summarized the contribution of the individual metals to IBS where all of the other metals are fixed at a particular percentile. In addition, we visualized a dose–response relationship of each metal with IBS while fixing the other metal at their 50th percentile. Finally, we also plotted the bivariate exposure–response function for two metals to test the possible interaction.
We also stratified the metal concentration by the median into low exposure (≤ 50th percentile) and high exposure (> 50th percentile) subgroups. Interaction effects between metal exposure (Low, high) and age (2–4 years old, 5–6 years old) on IBS were conducted after adjusting for all covariates. There was statistical significance for P value ≤ 0.05. All data were analyzed using R software (3.6.2).
Results
Characteristics of Study Participants
Table 1 showed the characteristics of the study participants. Among the 1399 children, 1140 (81.5%) individuals had NBS, while 259 (18.5%) individuals had IBS. There were no statistical differences between the NBS and IBS group in birthweight, birth status, feeding patterns, outdoor time, eating habits (fruit, vegetable, animal protein, milk and bean), calcium and vitamin D supplement, family income and urine creatinine. Compared with the NBS group, children with IBS were older, more likely to be girls, had higher body mass index, with a higher percentage of parents smoking, and lower percentage of SOS value (all P < 0.05).
Distributions of the Urinary Metals
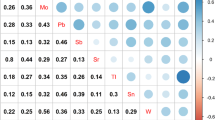
Concentrations (μg/L) of urine 23 urine metals are presented in Table S1. Undetected rates (N% < LOD) of all the metals were < 1.3%. Compared with NBS, children with IBS had lower concentrations of Co and Pb (both P < 0.05, see Table S2). In Spearman's rank correlation analysis, we found positive and significant associations among most metals, with rs ranging from 0.05 to 0.92 (P < 0.05) (see Fig. S1).
The Generalized Linear Model to Assess the Association Between Metals Exposure and IBS
Associations of the single metal exposure with IBS were investigated in the generalized linear model (see Table 2). After adjusting for sex, age, body mass index, birthweight, birth status, parents smoking, family income, and urine creatinine, urine Co, Zn, and Pb concentrations were related to IBS (all P < 0.05). Compared with those in the lowest quartile, the highest quartile of Co and Zn concentrations appeared a significant inverse association with IBS [OR (95% CI): 0.61 (0.39, 0.94), 0.57 (0.34, 0.94), respectively]. Urine Pb was positively associated with IBS in the second quartile compared to the reference group (OR 1.49, 95% CI 1.02–2.19).
These associations remained unchanged after additionally adjusted for outdoor time, feeding patterns, calcium supplement, vitamin D supplement, eating habits (fruit, vegetable, animal protein, milk and bean), and OR (95%CI) for extreme quartiles was 0.60 (0.39, 0.94) for Co, 0.54 (0.32, 0.90) for Zn, and 1.47 (1.00, 2.18) for Pb, respectively. Meanwhile, we observed a significant linear dose–response relationship of the single metal (Co, Zn and Pb) with IBS (all P for trend < 0.05). There were no significant associations of other metal exposure with IBS, and the detailed data was presented in Table 2.
WQS Regression Model to Assess the Association Between Mixed Metals Exposure and IBS
Exposure to mixed metals was statistically associated with IBS (Table 2). In the fully adjusted model, a one-quantile increase in the WQS index was statistically significantly associated with IBS (OR 0.87, 95%CI 0.80, 0.95). The association still existed even when the WQS index was divided into quartiles, and children in the highest quartile of WQS index had a 0.48-fold (95% CI 0.30 to 0.77) decreased odds of IBS, compared with the lowest quartile. A negative dose–response relation was observed for the WQS index with IBS (P for trend = 0.004). As for the estimated metal weight for the three positive metals: the highest weighted metal was Co, with a weight of 79.9%, followed by Zn (14.6%), and Pb (5.5%).
BKMR Model to Assess the Association Between Exposure to Metal Mixtures and IBS
Figures 1 illustrated the estimated joint effect of Co, Zn and Pb on IBS among children using BKMR models. First, we observed the overall association of mixed metals. In particular, compared to when all metals were at their median values, the overall association was statistically significant when all metals were at or above their 55th percentile, and the association increased at higher levels of the three joint exposures (Fig. 1a). Then, we estimated univariate summaries of risk change for IBS associated with a change in a single metal at the 75th vs. 25th percentile, when all the other metals are fixed at either the 25th, 50th, or 75th percentile. The change in Co concentration from the 25th to the 75th percentile was negatively associated with the risk of IBS, with − 0.16 (− 0.26, − 0.06), − 0.17 (− 0.26, − 0.08) and − 0.18 (− 0.29, − 0.07) standard deviations when Zn and Pb were set at the 25th, 50th, and 75th percentiles, respectively (Fig. 1b). Figure 1c showed the univariate exposure response relationship for each metal with the risk of IBS when the other metals fixed at the median. The plot suggested there was a linear relationship between Co and IBS (P for overall = 0.004, P for nonlinear = 0.161), and a nonlinear relationship between Pb and IBS (P for overall = 0.007; P for nonlinear = 0.006), while we did not find the linear or nonlinear relationship between Zn and IBS (P for overall = 0.109, P for nonlinear = 0.123). Finally, our research indicated that there was no interaction between the three metals on the risk of IBS (Fig. 1d).

Associations between urinary metals with IBS among preschool children by BKMR model. The model adjusted for sex, age, body mass index, birthweight, birth status, parents smoking, family income, and urine creatinine, outdoor time, feeding patterns, calcium supplement, vitamin D supplement, eating habits (fruit, vegetable, animal protein, milk and bean). a Overall effects of urinary multiple metals (estimated value and 95% confidence interval). Compared with other metals in the 50th percentile, the metals are in a specific percentile (X-axis). b The single-metal effect (estimates and 95% credible intervals). This plot compares the IBS when a single metal is at the 75th vs. 25th percentile, when all the other metals are fixed at either the 25th, 50th, or 75th percentile. c Univariate exposure–response functions and 95% confidence bands for each urinary metal with the other metals fixed at the median. d Bivariate exposure response function of each two metals in IBS
Stratified Analyses and Interaction Effects
The association of metal exposure (continuous) with IBS stratified by children’s age was shown in Fig. 2. There was a statistically significant relationship between exposure to Co, Zn and mixed metals (shown as WQS index) and IBS in children aged 2–4 years. The adjusted OR (95%CI) was 0.51 (0.34, 0.76) for Co, 0.59 (0.34, 1.00) for Zn and 0.43 (0.26, 0.69) for mixed metals, respectively.

Stratified analysis according to children’s age of the association between metal exposure (continuous) and IBS
In addition, the interaction effect of age on the associations of exposure to single metals and mixed metals with IBS was indicated in Table 3(P for interaction < 0.05). For children aged 2–4 years, high exposure to urine Co, Zn and Pb had a significantly lower risk of IBS than those with low exposure. Whereas children aged 5–6 years had a significantly higher risk of IBS than those with 2–4 years among low exposure to Co, Zn and Pb. A similar relationship remained when exposed to mixed metals. Compared with children combined with low mixed metals exposure and aged 2–4 years, children had a 0.47-fold (95% CI 0.29 to 0.76) decreased odds of IBS among those combined with high mixed metals exposure and aged 2–4 years, while had a 1.53-fold (95% CI 1.04 to 2.27) increased odds of IBS among combined with low mixed metals exposure and aged 5–6 years.
Discussion
In this study, we explored the relationships of urinary 23 metals with IBS among children aged 2–6 years in China. Overall, we observed negative associations of urine Co and Zn with risk of IBS in the single metal model, and a positive association of urine Pb. The WQS model and BKMR model identified that overall mixed exposure was significantly associated with IBS, which was mainly driven by Co. The univariate exposure–response function of the BKMR model revealed nonlinear relationships of Pb with IBS. Besides, there was an interaction effect of exposure to metal mixtures and children’s age on the risk of IBS.
Although there are some studies to explore the association between Co levels and the bone health, the association was still limited and controversial. For example, continuous NHANES survey data including 72,000 participants indicated no association between cumulative Co burden with BMD, which is an important index of bone strength (Park and An 2022). Another study among 12,584 U.S. adults based on the NHANES data identified Co was positively associated with osteoarthritis risk; participants in the highest quartile of Co had a 1.59-fold (95% CI 1.20 to 2.10) increased risk of osteoarthritis compared to the lowest quartile (Chen et al. 2022). Chang et al. found similar associations that a high concentration of Co in the bone was closely related to low bone strength (Chang et al. 2018). However, the present study observed inverse associations of urine Co concentrations with IBS. Therefore, whether the Co concentration was associated with bone strength needed to be investigated in further studies. Additionally, there are substantial differences in study design, study populations (e.g., race and age groups), metals sample (i.e., blood, urine, or bone), and bone strength assessment protocols, which may account for the variability observed in the existing literature. Co is an essential metal present in the diet as part of vitamin B12 (Leyssens et al. 2017), whereas in vitro experiments demonstrated that the ionic form of Co, may be toxic for humans (Simonsen et al. 2012). Free Co2 + could affect the human body through several molecular mechanisms of action that can have significant effects on the human body. One of the most notable mechanisms is the generation of reactive oxygen species and lipid peroxidation. This can lead to oxidative stress, which can damage cells and contribute to the development of various diseases (Paustenbach et al. 2013). And free Co2 + can induce cytotoxic effects on osteoblasts, inhibiting their ability to secrete and express type I collagen. This can lead to decreased bone density and an increased risk of fractures (Chang et al. 2018). Unfortunately, we did not detect the valence state of Co in this study. We will further improve the method in the follow-up study.
Zn is an essential component for our body. Over 85 percent of body Zn total is found in skeletal muscles and bones (King and Keen 1999). Zn has many important functions in bone formation; it stimulates osteoblast proliferation and osteoproteger in activity (Liang et al. 2012), plate during long bone growth (Oviedo-Rondón et al. 2006), and gene transcription at the growth whereas the deficiency in zinc levels significantly affects bone integrity, and reduces collagenase activity and subsequently collagen synthesis and mineralization of bone (Hyun et al. 2004; Starcher et al. 1980). An overview included 16 eligible studies indicated that the supplementation of zinc in an amount equal to 40–50 g could have beneficial effects on bone health in terms of maintaining bone mineral density and faster healing in the event of fractures (Rondanelli et al. 2021). The study of Alghadir et al. in older adults found lower levels of Zn in serum samples from participants with low bone strength than in normal controls (Alghadir et al. 2016). A case–control study in postmenopausal women suggested that urine Zn level could be considered an appropriate marker for bone absorption, and usage of Zn supplements may result in a beneficial increment in bone strength (Razmandeh et al. 2014). Also in an animal experimental pilot study, it has been shown that zinc deficiency initiated during adolescence was associated with reduced bone strength (Ryz et al. 2009). Our data provided a supporting result on the negative association of urine Zn with the risk of IBS, which are in accordance with the previous studies. In addition, significant interactions were found between the urine Zn concentration and age in our study. Urine Zn concentration was more strongly associated with IBS in children aged 2–4 years old.
Pb is a widely used industrialized and naturally toxic heavy metal, and approximately 90% of Pb is stored in bone in the body. Accumulating epidemiological studies have demonstrated an increased risk for osteoporosis of Pb exposure. A systematic review of 14 eligible studies with 15,421 adults publishing between 2002 and 2019 demonstrated exposure to Pb (OR 1.15; 95% CI 1.00 to 1.32) was associated with an increased risk of IBS (Jalili et al. 2020). A case control study with 60 participants suggested that high Pb was negatively correlated to BMD and increased the risk factor for osteoporosis (Banjabi et al. 2021). Several population-based studies showed that elevated Pb levels were positively associated with low BMD among children, adolescents and adults (Li et al. 2022; Lim et al. 2016; Wang et al. 2019; Wei et al. 2021). In line with the above literature, this study showed exposure to Pb was positively associated with IBS among children. Additionally, the nonlinear relationship between Pb exposure and IBS was also reported in Li et al. study, which observed an N-shaped curve association between Pb exposure and total and subtotal BMD for the whole population among 13,951 children and adolescents aged 8–19 years (Li et al. 2022). The harmful effect of Pb on skeletons may be attributable to its function of inhibiting vitamin D activity, dietary calcium absorption, and osteoblast functions (Beier et al. 2013; Dowd et al. 2001; Silbergeld et al. 1988). Pb has been shown to accelerate bone turnover and reduce bone mineralization and mineral density (Moran et al. 2013). Meanwhile, Pb inhibits the function of chondrocytes and osteoblasts and induces osteoblastic apoptosis, thereby altering many aspects of bone cell formation (Campbell and Auinger 2007; Rodriguez and Mandalunis 2018).
In this study, urinary Co and Zn were negatively correlated with IBS, while urinary Pb was positively correlated with IBS. This result could assist governments and public health institutions to better formulate and implement relevant policies and measures, such as strengthening environmental monitoring and control to reduce children's environmental exposure to toxic metals. In addition, regular bone strength testing could be performed to strengthen monitoring and protection of children's bone health. These policies and measures can help prevent and control the occurrence and spread of accidental injuries such as fractures in children, and improve their bone strength and overall health. Although our results found that Pb was positively associated with IBS, mixed metal exposure showed a negative association with IBS in the WQS and BKMR mixed-effect models. It has been known for decades that the toxicity of some pollutants can be affected by nutritional status (Mahaffey and Vanderveen 1979). In many cases, the results suggest that the positive association between trace elements and certain outcomes may be weakened at higher levels of toxic metals (Howe et al. 2021; Liu et al. 2018). However, due to variations in mixture composition across different populations, study contexts, and timing of exposure assessment, comparability across studies can be challenging. Despite these challenges, it is still crucial to conduct such studies in diverse settings.
However, several limitations should be noticed. Firstly, only the relationship between metal exposure and bone strength was explored. More parameters of bone property should be considered in future studies. Secondly, spot urine samples were used to measure the internal exposure levels of metals, which might lead to exposure misclassification. Additionally, measurements of 23 metals in the same urine sample might lead to measurement errors and increase the false positive rates. Finally, the current findings were based on a cross-sectional study, thus we could not ensure the causal relationship of metal exposure with bone strength. Further studies with prospective design are required to confirm our findings.
In summary, the WQS regression and BKMR models were applied to assess the association between exposure to metal mixtures and IBS among children aged 2–6 years in China. We concluded that an inverse overall association between exposure to the metal mixture (Co, Zn and Pb) and IBS, especially in children aged 2–4 years, and Co was the main contributor. Further studies are warranted to confirm our findings in prospective cohorts and to elucidate the underlying biological mechanism.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Akesson A, Bjellerup P, Lundh T, Lidfeldt J, Nerbrand C, Samsioe G et al (2006) Cadmium-induced effects on bone in a population-based study of women. Environ Health Perspect 114:830–834. https://doi.org/10.1289/ehp.8763
Alghadir AH, Gabr SA, Al-Eisa ES, Alghadir MH (2016) Correlation between bone mineral density and serum trace elements in response to supervised aerobic training in older adults. Clin Interv Aging 11:265–273. https://doi.org/10.2147/CIA.S100566
Banjabi AA, Kannan K, Kumosani TA, Yousef JM, Abulnaja KO, Moselhy SS (2021) Association of blood heavy metal levels with osteocalcin abnormality and incidence of osteoporosis in Saudi subjects. Braz J Biol 83:e248828. https://doi.org/10.1590/1519-6984.248828
Beier EE, Maher JR, Sheu T-J et al (2013) Heavy metal lead exposure, osteoporotic-like phenotype in an animal model, and depression of Wnt signaling. Environ Health Perspect 121:97–104. https://doi.org/10.1289/ehp.1205374
Bobb JF, Valeri L, Claus Henn B, Christiani DC, Wright RO, Mazumdar M et al (2015) Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 16:493–508. https://doi.org/10.1093/biostatistics/kxu058
Bobb JF, Claus Henn B, Valeri L, Coull BA (2018) Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ Health 17:67. https://doi.org/10.1186/s12940-018-0413-y
Campbell JR, Auinger P (2007) The association between blood lead levels and osteoporosis among adults–results from the third national health and nutrition examination survey (NHANES III). Environ Health Perspect 115:1018–1022. https://doi.org/10.1289/ehp.9716
Carrico C, Gennings C, Wheeler DC, Factor-Litvak P (2015) Characterization of weighted quantile sum regression for highly correlated data in a risk analysis setting. J Agric Biol Environ Stat 20:100–120. https://doi.org/10.1007/s13253-014-0180-3
Chang L, Shen S, Zhang Z, Song X, Jiang Q (2018) Study on the relationship between age and the concentrations of heavy metal elements in human bone. Ann Transl Med 6:320–327
Chen L, Zhao Y, Liu F, Chen H, Tan T, Yao P et al (2022) Biological aging mediates the associations between urinary metals and osteoarthritis among U.S. adults. BMC Med 20:207–219. https://doi.org/10.1186/s12916-022-02403-3
Chung SM (2022) Long-term sex-specific effects of cadmium exposure on osteoporosis and bone density: a 10-year community-based cohort study. J Clin Med 11:2899–2909. https://doi.org/10.3390/jcm11102899
Di Marcello F, Di Donato G, d’Angelo DM, Breda L, Chiarelli F (2022) Bone health in children with rheumatic disorders: focus on molecular mechanisms, diagnosis, and management. Int J Mol Sci 23:5725–5749. https://doi.org/10.3390/ijms23105725
Dowd TL, Rosen JF, Mints L, Gundberg CM (2001) The effect of Pb2+ on the structure and hydroxyapatite binding properties of osteocalcin. Biochem Biophys Acta 1535:153–163. https://doi.org/10.1016/s0925-4439(00)00094-6
Galvez-Fernandez M, Grau-Perez M, Garcia-Barrera T, Ramirez-Acosta S, Gomez-Ariza JL, Perez-Gomez B et al (2021) Arsenic, cadmium, and selenium exposures and bone mineral density-related endpoints: the HORTEGA study. Free Radic Biol Med 162:392–400. https://doi.org/10.1016/j.freeradbiomed.2020.10.318
Hans D, Šteňová E, Lamy O (2017) The trabecular bone score (TBS) complements DXA and the FRAX as a fracture risk assessment tool in routine clinical practice. Curr Osteoporos Rep 15:521–531. https://doi.org/10.1007/s11914-017-0410-z
Heitland P, Koster HD (2006) Biomonitoring of 30 trace elements in urine of children and adults by ICP-MS. Clin Chim Acta 365:310–318. https://doi.org/10.1016/j.cca.2005.09.013
Howe CG, Margetaki K, Vafeiadi M, Roumeliotaki T, Karachaliou M, Kogevinas M et al (2021) Prenatal metal mixtures and child blood pressure in the Rhea mother-child cohort in Greece. Environ Health 20:1–16. https://doi.org/10.1186/s12940-020-00685-9
Hyun TH, Elizabeth BC, Milne DB (2004) Zinc intakes and plasma concentrations in men with osteoporosis: the Rancho Bernardo Study. Am J Clin Nutr. https://doi.org/10.1556/AAlim.33.2004.3.13
Inose T, Takano T, Nakamura K, Kizuki M, Seino K (2006) Tibial cortical bone properties of preadolescents and their mothers in an urban area associated with lifestyle: a longitudinal study. Acta Paediatr 95:276–282. https://doi.org/10.1080/08035250500352169
Jalili C, Kazemi M, Taheri E, Mohammadi H, Boozari B, Hadi A et al (2020) Exposure to heavy metals and the risk of osteopenia or osteoporosis: a systematic review and meta-analysis. Osteoporos Int 31:1671–1682. https://doi.org/10.1007/s00198-020-05429-6
Katerina T, Fernando R (2019) The genetic architecture of osteoporosis and fracture risk. Bone 126:2–10. https://doi.org/10.1016/j.bone.2019.04.005
Kim ES, Shin S, Lee YJ, Ha IH (2021) Association between blood cadmium levels and the risk of osteopenia and osteoporosis in Korean post-menopausal women. Arch Osteoporos 16:22–32. https://doi.org/10.1007/s11657-021-00887-9
King J, Keen C (1999) Zinc. In: Shils M, Olson J, Shike M (eds) Modern nutrition in health and disease. Williams & Wilkins, Baltimore, pp 223–239
Lequin MH, Rijn RRV, Robben SGF, Hop WCJ, Kuijk CV (2000) Normal values for tibial quantitative ultrasonometry in Caucasian children and adolescents (aged 6 to 19 years). Calcif Tissue Int 67:101–105. https://doi.org/10.1007/s00223001119
Leyssens L, Vinck B, Van Der Straeten C, Wuyts F et al (2017) Cobalt toxicity in humans—a review of the potential sources and systemic health effects. Toxicology 387:43–56. https://doi.org/10.1016/j.tox.2017.05.015
Li JJ, Pang LN, Wu S, Zeng M (2018) Advances in the effect of heavy metals in aquatic environment on the health risks for bone. IOP Conf Ser 186:012057–012066. https://doi.org/10.1088/1755-1315/186/3/012057
Li T, Xie Y, Wang L, Huang G, Cheng Y, Hou D et al (2022) The association between lead exposure and bone mineral density in childhood and adolescence: results from NHANES 1999–2006 and 2011–2018. Nutrients 14:1523–1532. https://doi.org/10.3390/nu14071523
Liang D, Yang M, Guo B, Cao J, Yang L, Guo XD (2012) Zinc upregulates the expression of osteoprotegerin in mouse osteoblasts MC3T3-E1 through PKC/MAPK pathways. Biol Trace Elem Res 146:340–348. https://doi.org/10.1007/s12011-011-9254-z
Lim HS, Lee HH, Kim TH, Lee BR (2016) Relationship between heavy metal exposure and bone mineral density in Korean adult. J Bone Metab 23:223–231
Liu SH, Bobb JF, Claus Henn B, Gennings C, Schnaas L, Tellez-Rojo M et al (2018) Bayesian varying coefficient kernel machine regression to assess neurodevelopmental trajectories associated with exposure to complex mixtures. Stat Med 37:4680–4694. https://doi.org/10.1002/sim.7947
Liu Y, Yu L, Zhu M, Lin W, Liu Y, Li M et al (2022) Associations of exposure to multiple metals with blood pressure and hypertension: a cross-sectional study in Chinese preschool children. Chemosphere 307:135985–136004. https://doi.org/10.1016/j.chemosphere.2022.135985
Maggioli C, Stagi S (2017) Bone modeling, remodeling, and skeletal health in children and adolescents: mineral accrual, assessment and treatment. Ann Pediatr Endocrinol Metab 22:1–5. https://doi.org/10.6065/apem.2017.22.1.1
Mahaffey KR, Vanderveen JE (1979) Nutrient-toxicant interactions: susceptible populations. Environ Health Perspect 29:81–87. https://doi.org/10.1289/ehp.792981
Moradi S, Khorrami-Nezhad L, Ali-Akbar S, Zare F, Alipour T, Azadeh DKB et al (2018) The associations between dietary patterns and bone health, according to the TGF-β1 T869→C polymorphism, in postmenopausal Iranian women. Aging Clin Exp Res 30:563–571. https://doi.org/10.1007/s40520-017-0828-2
Moran JM, Lopez-Arza LG, Lavado-Garcia JM, Pedrera-Canal M, Rey-Sanchez P, Rodriguez-Velasco FJ et al (2013) Hormonal relationships to bone mass in elderly Spanish men as influenced by dietary calcium and vitamin D. Nutrients 5:4924–4937. https://doi.org/10.3390/nu5124924
Oviedo-Rondón E, Ferket PR, Havestein GB (2006) Understanding long bone development in broilers and turkeys. Avian Poultry Biol Rev 17:77–88
Park RM, An Y (2022) Continuous NHANES survey data for environmental ambient and occupational hazard identification-feasibility and preliminary findings for osteoporosis and kidney disease. J Occup Environ Hygiene. https://doi.org/10.1080/15459624.2022.2088769
Paustenbach DJ, Tvermoes BE, Unice KM, Finley BL, Kerger BD (2013) A review of the health hazards posed by cobalt. Crit Rev Toxicol 43:316–362. https://doi.org/10.3109/10408444.2013.779633
Qu X, He Z, Qiao H, Zhai Z, Mao Z, Yu Z et al (2018) Serum copper levels are associated with bone mineral density and total fracture. J Orthop Transl 14:34–44. https://doi.org/10.1016/j.jot.2018.05.001
Razmandeh R, Nasli-Esfahani E, Heydarpour R, Faridbod F, Ganjali MR, Norouzi P et al (2014) Association of zinc, copper and magnesium with bone mineral density in Iranian postmenopausal women—a case control study. J Diabetes Metab Disord 13:43–49. https://doi.org/10.1186/2251-6581-13-43
Rodriguez J, Mandalunis PM (2018) A review of metal exposure and its effects on bone health. J Toxicol 2018:4854152–4854163. https://doi.org/10.1155/2018/4854152
Rondanelli M, Peroni G, Gasparri C, Infantino V, Naso M, Riva A et al (2021) An overview on the correlation between blood zinc, zinc intake, zinc supplementation and bone mineral density in humans. Acta Ortop Mex 35:142–152
Ryz NR, Weiler HA, Taylor CG (2009) Zinc deficiency reduces bone mineral density in the spine of young adult rats: a pilot study. Ann Nutr Metab 54:218–226. https://doi.org/10.1159/000224627
Si L, Winzenberg TM, Jiang Q, Chen M, Palmer AJ (2015) Projection of osteoporosis-related fractures and costs in China: 2010–2050. Osteoporos Int 26:1929–1937. https://doi.org/10.1007/s00198-015-3093-2
Silbergeld EK, Schwartz J, Mahaffey K (1988) Lead and osteoporosis: mobilization of lead from bone in postmenopausal women. Environ Res 47:79–94. https://doi.org/10.1016/s0013-9351(88)80023-9
Simonsen LO, Harbak H, Bennekou P (2012) Cobalt metabolism and toxicology—a brief update. Sci Total Environ 432:210–215. https://doi.org/10.1016/j.scitotenv.2012.06.009
Starcher BC, Hill CH, Madaras JG (1980) Effect of zinc deficiency on bone collagenase and collagen turnover. J Nutr 110:2095–2102. https://doi.org/10.1093/jn/110.10.2095
Wang WJ, Wu CC, Jung WT, Lin CY (2019) The associations among lead exposure, bone mineral density, and FRAX score: NHANES, 2013 to 2014. Bone 128:115045. https://doi.org/10.1016/j.bone.2019.115045
Wang WJ, Huang MN, Wang CK, Yang AM, Lin CY (2021) Zinc status is independently related to the bone mineral density, fracture risk assessment tool result, and bone fracture history: results from a US nationally representative survey. J Trace Elem Med Biol 67:126765. https://doi.org/10.1016/j.jtemb.2021.126765
Weaver CM, Gordon CM, Janz KF, Kalkwarf HJ, Lappe JM, Lewis R et al (2016) The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int 27:1281–1386. https://doi.org/10.1007/s00198-015-3440-3
Wei MH, Cui Y, Zhou HL, Song WJ, Di DS, Zhang RY et al (2021) Associations of multiple metals with bone mineral density: a population-based study in US adults. Chemosphere 282:131150–131158. https://doi.org/10.1016/j.chemosphere.2021.131150
Wu C-C, Wang C-K, Yang A-M, Lu C-S, Lin C-Y (2020) Selenium status is independently related to bone mineral density, FRAX score, and bone fracture history: NHANES, 2013 to 2014. Bone 143:115631. https://doi.org/10.1016/j.bone.2020.115631
Acknowledgements
We thank all study participants for their valuable time and their support of our study. Furthermore, we would like to thank in particular Shiyan Maternal and Child Health Hospital for their help in collecting the biological sample and interviewing the study population participants.
Funding
This work was supported by the National Nature Science Foundation of China [Nos. 81872698 and 71774049]; Innovative Research Team of Hubei Provincial Department of Education [T2021014]; Advantages Discipline Group (Public health) Project in Higher Education of Hubei Province (2021–2025) [2022PHXKQ3]; Starting Fund of Hubei University of Medicine [2020QDJZR029].
Author information
Authors and Affiliations
Contributions
YL and YW have contributed equally to the work and share first authorship. YL and YW: conceptualization, formal analysis, visualization, data curation, writing—original draft preparation. YF, YL, ML, and MH: data curation, investigation, data collection, visualization. YZ, CL and HD: investigation, project administration, resources, supervision. XL and HJ: investigation, data curation, resources, supervision, project administration. JW: conceptualization, writing—review and editing, supervision, project administration, funding acquisition. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, Y., Wang, Y., Fu, Y. et al. Associations Between Exposure to Metal Mixtures and Insufficient Bone Strength: A Cross-Sectional Study Among Children Aged 2–6 Years. Expo Health 16, 791–803 (2024). https://doi.org/10.1007/s12403-023-00591-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-023-00591-8