
Abstract
Human beings are exposed to heavy metals through various ways in daily life. However, the effect of heavy metal mixtures on muscle strength in children and adolescents remains unclear. We aimed to investigate the relationship of exposure to heavy metal mixtures (barium, cadmium, cobalt, manganese, molybdenum, lead, antimony, strontium, tin, thallium, tungsten, uranium, and cesium) with muscle strength in children and adolescents. A total of 1357 (boys, 50.8%) participants aged between 8 and 17 were extracted from the National Health and Nutrition Examination Surveys 2011–2014. Urine metals were measured by inductively coupled plasma-mass spectrometry. Muscle strength was measured through a grip test using a handgrip dynamometer. Weighted quantile sum regression was performed to estimate the mixture effect of urinary metals on muscle strength. After adjusting for potential confounders, comparing participants in the highest versus lowest quartiles of cobalt, molybdenum, lead, antimony, strontium, thallium, and cesium, the handgrip strength decreased by − 4.48 kg (95% CI: − 6.93, − 2.03), − 6.13 kg (− 8.76, − 3.51), − 2.26 kg (− 4.22, − 0.30), − 2.38 kg (− 4.68, − 0.08), − 2.29 kg (− 4.45, − 0.13), − 4.78 kg (− 7.13, − 2.44), and − 5.68 kg (− 9.20, − 2.17), respectively. Furthermore, exposure to a mixture of metals were also significantly associated with decreased muscle strength (β: − 2.62 kg; 95% CI: − 3.71, − 1.54). Findings from the present study suggest that higher heavy metal exposure and the exposure levels of a mixture of metals in urine are inversely related to handgrip strength, implying that children’s grip strength is not entirely explained by energy intake or lack of exercise, but may be related to environmental pollutants.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Metals are significant natural components of all soils and are present widely in the geological environment (Violante et al. 2010). While many metals are essential to plants and animals, they are potentially toxic at higher enough doses (Tchounwou et al. 2012). For the past decades, metal discharges caused by anthropogenic activities such as the manufacture of metal goods and a wide range of industrial and agricultural activities pose a great threat to public health (Tchounwou et al. 2012).
In 2019, the United States Agency for Toxic Substances and Disease Registry ranked many metals (e.g., cadmium (Cd), cobalt (Co), uranium (U), barium (Ba)) within the top 275 priority substances according to their frequency, toxicity, and potential for human exposure (Registry). Because of the plant enrichment, atmospheric sedimentation, and environment dissemination, human beings tend to be exposed to metals through the consumption of contaminated water or food and through the inhalation of polluted air in daily life (Järup 2003; Tchounwou et al. 2012). Notably, children and adolescents exhibit higher rates of intestinal absorption and lower rates of renal excretion than do adults (Ilmiawati et al. 2015). Moreover, these age groups are particularly susceptible to the adverse environmental conditions because of their physiology or their behavior (Moya et al. 2004). With these in mind, a growing number of epidemiological studies have been conducted among the children’s population and suggested that metal exposures are associated with a variety of adverse health conditions (e.g., obesity, delayed pubertal development, and intellectual impairment) (Jakubowski 2011; Reynolds et al. 2020; Shao et al. 2017; Vecchi Brumatti et al. 2021). To fully understand the effects of metals on children’s health conditions, metal exposures in mixtures manner is getting extra attention. The associations of exposure to mixture of metals with poor growth or other health conditions in children have been reported in previous studies (Moody et al. 2020; Sanders et al. 2019), but the potential effects of heavy metal mixtures on childhood muscle strength remain understudied.
Handgrip strength is a commonly used reliable marker of muscle strength and has been labeled as a marker of aging because of the potential links with future disability, morbidity, and mortality (Sayer and Kirkwood 2015). A growing number of studies showed that high handgrip strength is a protective factor for cardiometabolic health among children and adolescents (Artero et al. 2011; Clark et al. 2011; Peterson et al. 2014, 2016), and may be beneficial to lung health (Smith et al. 2018), and even related to longitudinal health maintenance and health improvements in adolescents (Peterson et al. 2018). The health benefits from muscular strength in childhood may also extend into adulthood (Fraser et al. 2021), with increased levels correlated to decreased risk of a variety of negative health outcomes, including falls, type 2 diabetes, hypertension, arterial stiffness, and cardiovascular mortality in the general population (König et al. 2021; Maslow et al. 2010; Ruiz et al. 2008; Tarp et al. 2019; Yates et al. 2017). Therefore, identifying the potential influence factors (e.g., environmental determinants) for weaker muscle strength in children and adolescents might provide more insights for the early prevention of aging-related diseases.
In the present study, the primary objective was to examine the associations of single-metal exposure (Cd, Co, U, Ba, lead (Pb), thallium (Tl), manganese (Mn), molybdenum (Mo), antimony (Sb), strontium (Sr), tin (Sn), tungsten (W), and cesium (Cs)) and heavy metal mixtures with handgrip strength in US children and adolescents using the data of the National Health and Nutrition Examination Survey (NHANES).
Methods
Study population
The data of the current study were extracted from 2011–2014 cycles of the NHANES, of which are ongoing, stratified, multistage probability surveys of the non-institutionalized civilian population of the USA conducted by the National Center for Health Statistics. Survey participants were asked to complete the in-home personal interview, and physical examinations at mobile examination centers where biological samples and anthropometric and health data were collected. NHANES procedures were approved by the National Center for Health Statistics research ethics review board, and the informed consent was obtained from all participants prior to their inclusion in the surveys.
During the 2011–2014 cycles of the NHANES, a total of 7954 participants aged < 18 years constituted the original study sample. From these subjects, a total of 1357 participants had valid information on urine metal and handgrip strength.
Study variables
Urinary metals
Spot urine samples were collected from eligible participants at mobile examination centers and stored at the National Centers for Disease Control and Prevention. Urinary metals (Ba, Cd, Co, Mn, Mo, Pb, Sb, Sr, Tl, Sn, W, U, and Cs) were all examined by inductively coupled plasma–mass spectrometry. For the present study, urinary Cd and urinary Mn were excluded in further analyses due to the low detection rates (< 75%). Participants with metal concentration below the limit of detection were assigned a value equal to the detection limit divided by the square root of 2 (Hewett and Ganser 2007). To account for urine dilution, we divided urine metal levels by urine creatinine (μg/g). Of note, all samples (blanks, calibrators, quality control, or patient samples) are combined with the diluent during the sample preparation step before analysis. Incomplete data or improbable values were sent to the performing laboratory for confirmation. More detailed laboratory methods and quality control/quality assurance were summarized in the official website of NHANES (Caldwell 2012).
Muscle strength
Muscle strength was measured through a grip test using a handgrip dynamometer (Takei Digital Grip Strength Dynamometer, Model T.K.K.5401; Takei Scientific Instruments Co., Niigata, Japan). Calibration checks were performed at the beginning of each test to confirm the working status of the dynamometer. Before measurement of handgrip strength, the dynamometer grip size was adjusted properly for each hand. Participants were asked to keep standing posture and squeeze the dynamometer using one hand as strong as they could. For each eligible participant, handgrip strength was tested three times for each hand, with alternating hands between tests with a 60-s rest between measurements on the same hand. The combined handgrip strength defined as the sum of the largest reading from each hand was used as the outcome variable in the present study. Detailed descriptions of the protocol are provided in the NHANES Muscle Strength/Grip Test Procedure Manual available on the NHANES website (https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/MGX_G.htm).
Covariates
Demographic information (e.g., age, sex, and ethnicity/race) as well as lifestyle (e.g., computer use) were ascertained by standard questionnaires. Body weight and body height was measured through physical examination. The BMI z-score was calculated using LMS approach (Flegal and Cole 2013). A previous study has reported a significant relationship between secondhand tobacco smoke and reduced muscle strength (Carrasco-Rios et al. 2019). Therefore, the secondhand smoke may be a confounding factor for the relationship between metal exposure and muscle strength in children and adolescents. In this study, the levels of serum cotinine, a marker for active smoking and secondhand smoking, was measured using an isotope-dilution high-performance liquid chromatography/atmospheric pressure chemical ionization tandem mass spectrometric method. The ratio of family income to poverty (PIR) was used to reflect social economic level. In addition, the dietary energy intake and protein intake estimated by 24-h recall method was considered as potential covariates related to nutritional factors in this study.
Statistical analyses
Categorical variables were presented as counts (percentages), and continuous variables were presented as means (SDs) if data presented a normal distribution or presented as medians (25th–75th) if data presented a skewed distribution. Due to the potential differences in handgrip strength between boys and girls, the description results were presented according to sex. The categorical variables were compared between boys and girls using the χ2 test, while the continuous variables were compared using the t test or Kruskal–Wallis test. The confounders with missing values were imputed by applying multiple imputation method. The associations between single urinary metal and handgrip strength were evaluated using linear regression model. Variables that potentially showed association with metal concentrations or muscle strength were selected as covariates. In this study, the potential covariates include age (years), sex (boy and girl), ethnicity/race (non-Hispanic white, non-Hispanic black, Hispanic, and other race), BMI z-score, PIR, serum cotinine concentration (ng/mL), computer use (not use, < 1 h, and ≥ 1 h), total energy intake (kcal), and protein intake (g) (Carrasco-Rios et al. 2019; Edelson et al. 2016; Ng et al. 2020; Wolfe et al. 2020). Three multivariable models were performed in this study: Model 0 was crude model; Model 1 was adjusted for age and sex; Model 2 was adjusted for age, sex, ethnicity/race, BMI z-score, PIR, serum cotinine concentration, computer use, total energy intake, and protein intake.
To identify important metals and estimate the joint effect of the mixture urinary metals on muscle strength, weighted quantile sum (WQS) regression was performed. The WQS method can utilize high-dimensional dataset (i.e., environmental metals exposure) through a weighted index and estimate the joint effect of mixture exposures. Briefly, WQS assigns each metal within the mixture a weight that reflects the strength of that metal–outcome association. This weight would be lower if a given metal highly correlated with another metal in the mixture. In this case, the sum of the weights between two metals reflect the contribution of the correlated metals to the overall mixture effect (Carrico et al. 2015). WQS model in the present study takes the form \({Y}_{i}={\beta }_{0}+{\beta }_{1}{\Sigma }_{j}{{w}_{j}q}_{ij}+{\beta }_{2}{x}_{i}+{\varepsilon }_{j}\), where wj is a weight for the jth metal estimated by 500 bootstraps, qij is the quartile corresponding to the jth metal for the ith person, and β1 represents the joint effect scale of the mixture metal exposures. The weight for each metal was constrained to add up to 1.0 and to fall between 0 and 1, and this was used to identify important metals (highly weighted) for the effects on handgrip strength.
Survey weights were constructed for survey years as recommended by NHANES. Specifically, the updated urine metal subsample weight for each subject was used in linear regression models. All data cleaning and statistical analyses were performed using R version 4.0.2 statistical software (R Foundation for Statistical Computing, https://www.r-project.org/). P < 0.05 was regarded as significantly different.
Results
The demographic characteristics of the study population are presented in Table 1. In total, 1357 subjects (boy, 50.8%) were included in this study. The mean chronological age was 11 ± 3.3 and the mean BMI z-score was 0.7 ± 1.2. The proportion of participants who did not use computer was 17.2%.
The distribution of the urine metal exposures of the study population is shown in Table 2. The median values of the urine Ba, Co, Mo, Pb, Sb, Sr, Tl, Sn, W, U, and Cs concentrations were 1.36, 0.52, 62.58, 0.31, 0.07, 92.95, 0.19, 0.92, 0.14, 0.006, and 4.65 μg/g, respectively. We found significant correlations among the urinary metals (Fig. 1). Urinary Ba was found to have a strong correlation with Sr (r = 0.80).

Spearman’s correlations among the urinary metals (N = 1357), NHANES 2011–2014. All correlations: P < 0.05. Ba, barium; Co, cobalt; Mo, molybdenum; Pb, lead; Sb, antimony; Sr, strontium; Tl, thallium; Sn, tin; W, tungsten; U, uranium; Cs, cesium. This is a heat map with a correlation matrix. The darker the color with larger circular area, the greater the correlation coefficient between the corresponding two metals’ concentrations. For example, the maximum was the correlation between Ba and Sr (r = 0.8), and the darkest color was drawn on the diagram
The associations of single-metal exposure with handgrip strength are shown in Table 3. In models adjusted for age, sex, ethnicity/race, BMI z-score, PIR, computer use, serum cotinine, dietary energy intake and protein intake, and comparing participants in the highest versus lowest quartiles of Pb and Tl concentrations in urine, the combined handgrip strength decreased by − 2.26 kg (− 4.22, − 0.30) and − 4.78 kg (− 7.13, − 2.44), respectively. Similar results were observed for Co, Mo, Sb, Sr, and Cs, and the combined handgrip strength decreased by − 4.48 kg (− 6.93, − 2.03), − 6.13 kg (− 8.76, − 3.51), − 2.38 kg (− 4.68, − 0.08), − 2.29 kg (− 4.45, − 0.13), and − 5.68 kg (− 9.20, − 2.17), respectively.
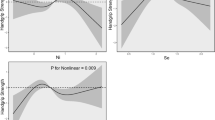
The results of the WQS regression model are shown in Table 4. The WQS index had a significant negative association with handgrip strength after fully adjusting for potential covariates (β: − 2.62 kg; 95% CI: − 3.71, − 1.54). We also calculated the estimated metal weights in the WQS regression model, which are presented in Fig. 2. The highest weighted metal in fully adjusted model was W (weighted 0.127), followed by Sn and U (weighted 0.123 and 0.113, respectively). Considering the potential sex differences in the correlation between increased levels of metal mixture exposure and handgrip strength in children and adolescents, we carried out stratification analyses by sex. Results from the stratification analyses indicated that exposure to a mixture of urinary heavy metals was correlated negatively with handgrip strength among boys (β: − 2.46 kg; 95% CI: − 4.10, − 0.82) and girls (β: − 2.55 kg; 95% CI: − 3.71, − 1.39) (Table 4).

WQS model regression index weights for handgrip strength. Ba, barium; Co, cobalt; Mo, molybdenum; Pb, lead; Sb, antimony; Sr, strontium; Tl, thallium; Sn, tin; W, tungsten; U, uranium; Cs, cesium
Discussion
The present study investigated the associations of urinary metals with muscle strength in US children and adolescents. Urinary Co, Mo, Pb, Sb, Sr, Tl, and Cs were found to be associated with decreased handgrip strength. These observed findings persisted even after adjusting for multiple potential confounders. Furthermore, exposure to urinary metal mixtures was also significantly associated with decreased muscle strength. To the best of our knowledge, the present study is the first to investigate the association of urinary metal exposure with muscle strength in children and adolescents.
Although much research effort has been devoted to examine the associations between environmental pollutants and health conditions (Xu et al. 2020), few studies have reported the association between metal exposure and muscle strength. To our knowledge, there are only two investigations that have examined the relationship of metal exposure with muscle strength. Data from 983 Korean adult participants indicated a significant relationship of Cd exposure with lower handgrip strength (Kim et al. 2016). Another more recent study also reported that higher Cd exposure was associated with decreased handgrip strength among 4197 US adults. In the present study, we did not analyze the association between Cd and handgrip strength due to the low detection rate of Cd (about 52.84%). A few studies had evaluated the association of Pb exposure and frailty, an age-related syndrome characterized by reductions in muscle strength (García-Esquinas et al. 2015; Khalil et al. 2014). A cross-sectional study reported an association between Co exposure and increased measured time to walk a 20-ft course (Lang et al. 2009). In an experimental study, low doses of heavy metal exposure were also observed to be associated with muscular fiber changes (Méndez-Armenta et al. 2011). Although these abovementioned studies were not directly focused on grip strength, their findings may provide indirect evidence for the adverse effects of heavy metals on muscle strength. In the present study, a number of urine metals (e.g., Mo, Sb, Sr, and Cs) were found to be associated with decreased handgrip strength, which implied that children’s grip strength is not entirely explained by energy intake or lack of exercise, but may be related to environmental pollutants. Co-exposure of these metals may be more common because they are widely dispersed in the environment. In our study, a mixture exposure of metals was also significantly associated with the decreased handgrip strength, which provided new insights into the existing limited evidence and highlighted the important effects of mixture exposure of metals on health conditions in childhood. However, because of the lack of relevant studies on this issue so far, further investigations from different countries or regions are warranted to confirm our findings.
Biologic mechanisms underlying the association between the metal exposure and handgrip strength remain unclear. The generation of reactive oxygen species (ROS) and obesogenic effects may be possible hypotheses for the unfavorable correlation between heavy metals and handgrip strength. Several metals (e.g., Pb, Tl, and Cs) were found to promote the oxidative stress (Ashrap et al. 2021), and induce a significant increase in mitochondrial ROS formation by impairing mitochondrial functioning (Eskandari et al. 2015). This may lead to the alterations of electron transport chain and remarkably induce oxidative deterioration of biological macromolecules, finally resulting in the cellular damage in organs and tissues, including muscle tissue (Fatouros and Jamurtas 2016; Méndez-Armenta et al. 2011). Moreover, adipose tissue may act as a target of obesogenic pollutants including heavy metals. Many experimental and epidemiologic evidences have demonstrated the associations between metals and increased skinfold (Barrientos et al. 2020; Freire et al. 2020), or the increased risk of obesity (Wang et al. 2018). Since intramuscular adipose tissue can significantly reduce muscle strength (Biltz et al. 2020), the obesogenic effects of metals observed from above studies may provide the indirect evidence for the biological explanation of the observed relationships in this study.
Findings from the present study have important practical implications. Decreased muscle strength was associated with various negative health outcomes, and it was reported that muscular strength levels in childhood are critical in predicting strength levels throughout the life course to adulthood (Fraser et al. 2021). Therefore, the lower muscle strength at the childhood may increase the disease susceptibility throughout the lifespan. In addition, metals are widely distributed in the environment because of anthropogenic activities, which may lead to continuous low-dose exposure of metals through dietary intake of plant-derived food and drinking water in children and adolescents. Children have immature detoxification function and are particularly susceptible to the adverse environmental conditions because of their physiology or their behavior (e.g., children drink more water per unit of body weight than adults, and more likely to contact with the ground and the dust). Therefore, these age groups may be more likely exposed to metals in daily life. Moreover, population-based observational studies and animal-based experimental studies support the concept that the environmental metal exposure has a significant impact on human health, even at low-dose exposure levels (Duan et al. 2020; Gleason et al. 2020; Moody et al. 2020; Sanders et al. 2019; Xu et al. 2020). Therefore, revealing the association between urine metal exposure and muscle strength in children and adolescents may provide new insight into health management across the lifespan time.
Several limitations of this study should be pointed out. First, although significant correlations of single metal or mixture exposure of metals with handgrip strength were observed in children and adolescents, the causal or temporal association is unclear because of the cross-sectional design in NHANES. Second, although we adjusted for potential confounders, the residual confounding effects (i.e., psychological and genetic factors) could still bias our findings. Third, although we considered a mixture of metals in this study, several unmeasured pollutants (e.g., pesticides) might have an effect on muscle strength through ROS or mitochondria dysfunction, and it may bias the present findings. Lastly, the assessment of exposure based on single urine sample cannot completely rule out the potential exposure misclassification errors.
Conclusion
In conclusion, our findings suggest that urinary heavy metal mixture exposures are associated with decreased muscle strength in children and adolescents. Our findings might have critical public health implications because increasing and widespread exposure to environmental metals and their mixtures may be a key contributor to human health conditions.
Data availability
Original data can be found in the official website (https://www.cdc.gov/nchs/nhanes/index.htm).
References
Artero EG, Ruiz JR, Ortega FB, España-Romero V, Vicente-Rodríguez G, Molnar D et al (2011) Muscular and cardiorespiratory fitness are independently associated with metabolic risk in adolescents: the Helena study. Pediatr Diabetes 12:704–712. https://doi.org/10.1111/j.1399-5448.2011.00769.x
Agency of Toxic Substances and Disease Registry (2019) ATSDR’s substance priority list in. Available: https://www.atsdr.cdc.gov/spl/. Accessed 16 Dec 2021
Ashrap P, Watkins DJ, Milne GL, Ferguson KK, Loch-Caruso R, Fernandez J, et al. (2021) Maternal urinary metal and metalloid concentrations in association with oxidative stress biomarkers. Antioxidants (Basel) 10. https://doi.org/10.3390/antiox10010114
Barrientos G, Alves J, Toro V, Robles MC, Muñoz D, Maynar M (2020) Association between trace elements and body composition parameters in endurance runners. Int J Environ Res Public Health 17. https://doi.org/10.3390/ijerph17186563
Biltz NK, Collins KH, Shen KC, Schwartz K, Harris CA, Meyer GA (2020) Infiltration of intramuscular adipose tissue impairs skeletal muscle contraction. J Physiol 598:2669–2683. https://doi.org/10.1113/jp279595
Caldwell KL (2012) Laboratory procedure manual. Available: https://wwwn.cdc.gov/n;chs/data/nhanes/2011-2012/labmethods/uhm_g_met_heavy_metals.pdf. Accessed 16 Dec 2021
Carrasco-Rios M, Ortolá R, Rodríguez-Artalejo F, García-Esquinas E (2019) Exposure to secondhand tobacco smoke is associated with reduced muscle strength in us adults. Aging (albany NY) 11:12674–12684. https://doi.org/10.18632/aging.102594
Carrico C, Gennings C, Wheeler DC, Factor-Litvak P (2015) Characterization of weighted quantile sum regression for highly correlated data in a risk analysis setting. J Agric Biol Environ Stat 20:100–120. https://doi.org/10.1007/s13253-014-0180-3
Clark EM, Tobias JH, Murray L, Boreham C (2011) Children with low muscle strength are at an increased risk of fracture with exposure to exercise. J Musculoskelet Neuronal Interact 11:196–202
Duan W, Xu C, Liu Q, Xu J, Weng Z, Zhang X et al (2020) Levels of a mixture of heavy metals in blood and urine and all-cause, cardiovascular disease and cancer mortality: a population-based cohort study. Environ Pollut 263:114630. https://doi.org/10.1016/j.envpol.2020.114630
Edelson LR, Mathias KC, Fulgoni VL 3rd, Karagounis LG (2016) Screen-based sedentary behavior and associations with functional strength in 6–15 year-old children in the United States. BMC Public Health 16:116. https://doi.org/10.1186/s12889-016-2791-9
Eskandari MR, Mashayekhi V, Aslani M, Hosseini MJ (2015) Toxicity of thallium on isolated rat liver mitochondria: the role of oxidative stress and MPT pore opening. Environ Toxicol 30:232–241. https://doi.org/10.1002/tox.21900
Fatouros IG, Jamurtas AZ (2016) Insights into the molecular etiology of exercise-induced inflammation: opportunities for optimizing performance. J Inflamm Res 9:175–186. https://doi.org/10.2147/jir.s114635
Flegal KM, Cole TJ (2013) Construction of LMS parameters for the Centers for Disease Control and Prevention 2000 growth charts. Natl Health Stat Report:1–3
Fraser BJ, Blizzard L, Buscot MJ, Schmidt MD, Dwyer T, Venn AJ et al (2021) Muscular strength across the life course: the tracking and trajectory patterns of muscular strength between childhood and mid-adulthood in an Australian cohort. J Sci Med Sport. https://doi.org/10.1016/j.jsams.2021.01.011
Freire C, Vrhovnik P, Fiket Ž, Salcedo-Bellido I, Echeverría R, Martín-Olmedo P et al (2020) Adipose tissue concentrations of arsenic, nickel, lead, tin, and titanium in adults from Gramo cohort in Southern Spain: an exploratory study. Sci Total Environ 719:137458. https://doi.org/10.1016/j.scitotenv.2020.137458
García-Esquinas E, Navas-Acien A, Pérez-Gómez B, Artalejo FR (2015) Association of lead and cadmium exposure with frailty in US older adults. Environ Res 137:424–431. https://doi.org/10.1016/j.envres.2015.01.013
Gleason KM, Valeri L, Shankar AH, Obrycki JF, Ibne Hasan MOS, Mostofa G et al (2020) Stunting and lead: using causal mediation analysis to better understand how environmental lead exposure affects cognitive outcomes in children. J Neurodev Disord 12:39. https://doi.org/10.1186/s11689-020-09346-x
Hewett P, Ganser GH (2007) A comparison of several methods for analyzing censored data. Ann Occup Hyg 51:611–632. https://doi.org/10.1093/annhyg/mem045
Ilmiawati C, Yoshida T, Itoh T, Nakagi Y, Saijo Y, Sugioka Y et al (2015) Biomonitoring of mercury, cadmium, and lead exposure in japanese children: a cross-sectional study. Environ Health Prev Med 20:18–27. https://doi.org/10.1007/s12199-014-0416-4
Jakubowski M (2011) Low-level environmental lead exposure and intellectual impairment in children—the current concepts of risk assessment. Int J Occup Med Environ Health 24:1–7. https://doi.org/10.2478/s13382-011-0009-z
Järup L (2003) Hazards of heavy metal contamination. Br Med Bull 68:167–182. https://doi.org/10.1093/bmb/ldg032
Khalil N, Faulkner KA, Greenspan SL, Cauley JA (2014) Associations between bone mineral density, grip strength, and lead body burden in older men. J Am Geriatr Soc 62:141–146. https://doi.org/10.1111/jgs.12603
Kim KN, Lee MR, Choi YH, Lee BE, Hong YC (2016) Associations of blood cadmium levels with depression and lower handgrip strength in a community-dwelling elderly population: a repeated-measures panel study. J Gerontol A Biol Sci Med Sci 71:1525–1530. https://doi.org/10.1093/gerona/glw119
König M, Buchmann N, Seeland U, Spira D, Steinhagen-Thiessen E, Demuth I (2021) Low muscle strength and increased arterial stiffness go hand in hand. Sci Rep 11:2906. https://doi.org/10.1038/s41598-021-81084-z
Lang IA, Scarlett A, Guralnik JM, Depledge MH, Melzer D, Galloway TS (2009) Age-related impairments of mobility associated with cobalt and other heavy metals: data from NHANES 1999–2004. J Toxicol Environ Health A 72:402–409. https://doi.org/10.1080/15287390802647336
Maslow AL, Sui X, Colabianchi N, Hussey J, Blair SN (2010) Muscular strength and incident hypertension in normotensive and prehypertensive men. Med Sci Sports Exerc 42:288–295. https://doi.org/10.1249/MSS.0b013e3181b2f0a4
Méndez-Armenta M, Nava-Ruiz C, Fernández-Valverde F, Sánchez-García A, Rios C (2011) Histochemical changes in muscle of rats exposed subchronically to low doses of heavy metals. Environ Toxicol Pharmacol 32:107–112. https://doi.org/10.1016/j.etap.2011.03.001
Moody EC, Colicino E, Wright RO, Mupere E, Jaramillo EG, Amarasiriwardena C et al (2020) Environmental exposure to metal mixtures and linear growth in healthy ugandan children. PLoS ONE 15:e0233108. https://doi.org/10.1371/journal.pone.0233108
Moya J, Bearer CF, Etzel RA (2004) Children’s behavior and physiology and how it affects exposure to environmental contaminants. Pediatrics 113:996–1006
Ng AK, Hairi NN, Dahlui M, Su TT, Jalaludin MY, Abdul Majid H (2020) The longitudinal relationship between dietary intake, physical activity and muscle strength among adolescents. Br J Nutr 124:1207–1218. https://doi.org/10.1017/s0007114520002202
Peterson MD, Saltarelli WA, Visich PS, Gordon PM (2014) Strength capacity and cardiometabolic risk clustering in adolescents. Pediatrics 133:e896-903. https://doi.org/10.1542/peds.2013-3169
Peterson MD, Zhang P, Saltarelli WA, Visich PS, Gordon PM (2016) Low muscle strength thresholds for the detection of cardiometabolic risk in adolescents. Am J Prev Med 50:593–599. https://doi.org/10.1016/j.amepre.2015.09.019
Peterson MD, Gordon PM, Smeding S, Visich P (2018) Grip strength is associated with longitudinal health maintenance and improvement in adolescents. J Pediatr 202:226–230. https://doi.org/10.1016/j.jpeds.2018.07.020
Reynolds P, Canchola AJ, Duffy CN, Hurley S, Neuhausen SL, Horn-Ross PL et al (2020) Urinary cadmium and timing of menarche and pubertal development in girls. Environ Res 183:109224. https://doi.org/10.1016/j.envres.2020.109224
Ruiz JR, Sui X, Lobelo F, Morrow JR Jr, Jackson AW, Sjöström M et al (2008) Association between muscular strength and mortality in men: prospective cohort study. BMJ 337:a439. https://doi.org/10.1136/bmj.a439
Sanders AP, Mazzella MJ, Malin AJ, Hair GM, Busgang SA, Saland JM et al (2019) Combined exposure to lead, cadmium, mercury, and arsenic and kidney health in adolescents age 12–19 in NHANES 2009–2014. Environ Int 131:104993. https://doi.org/10.1016/j.envint.2019.104993
Sayer AA, Kirkwood TB (2015) Grip strength and mortality: a biomarker of ageing? Lancet 386:226–227. https://doi.org/10.1016/s0140-6736(14)62349-7
Shao W, Liu Q, He X, Liu H, Gu A, Jiang Z (2017) Association between level of urinary trace heavy metals and obesity among children aged 6–19 years: NHANES 1999–2011. Environ Sci Pollut Res Int 24:11573–11581. https://doi.org/10.1007/s11356-017-8803-1
Smith MP, Standl M, Berdel D, von Berg A, Bauer CP, Schikowski T et al (2018) Handgrip strength is associated with improved spirometry in adolescents. PLoS ONE 13:e0194560. https://doi.org/10.1371/journal.pone.0194560
Tarp J, Støle AP, Blond K, Grøntved A (2019) Cardiorespiratory fitness, muscular strength and risk of type 2 diabetes: a systematic review and meta-analysis. Diabetologia 62:1129–1142. https://doi.org/10.1007/s00125-019-4867-4
Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ (2012) Heavy metal toxicity and the environment. Exp Suppl 101:133–164. https://doi.org/10.1007/978-3-7643-8340-4_6
Vecchi Brumatti L, Rosolen V, Mariuz M, Piscianz E, Valencic E, Bin M et al (2021) Impact of methylmercury and other heavy metals exposure on neurocognitive function in children aged 7 years: study protocol of the follow-up. J Epidemiol 31:157–163. https://doi.org/10.2188/jea.JE20190284
Violante ACV, Perelomov L, Caporale AG, Pigna M (2010) Mobility and bioavailability of heavy metals and metalloids in soil environments. J Soil Sci Plant Nutri 10:268–292
Wang X, Mukherjee B, Park SK (2018) Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003–2014. Environ Int 121:683–694. https://doi.org/10.1016/j.envint.2018.09.035
Wolfe AM, Lee JA, Laurson KR (2020) Socioeconomic status and physical fitness in youth: findings from the NHANES national youth fitness survey. J Sports Sci 38:534–541. https://doi.org/10.1080/02640414.2020.1713688
Xu Y, Wei Y, Long T, Wang R, Li Z, Yu C et al (2020) Association between urinary metals levels and metabolic phenotypes in overweight and obese individuals. Chemosphere 254:126763. https://doi.org/10.1016/j.chemosphere.2020.126763
Yates T, Zaccardi F, Dhalwani NN, Davies MJ, Bakrania K, Celis-Morales CA et al (2017) Association of walking pace and handgrip strength with all-cause, cardiovascular, and cancer mortality: a UK Biobank observational study. Eur Heart J 38:3232–3240. https://doi.org/10.1093/eurheartj/ehx449
Acknowledgements
The authors of this manuscript certify that they comply with the ethical guidelines for authorship and publishing in the Environmental Science and Pollution Research.
Funding
This research was not funded by a specific project grant.
Author information
Authors and Affiliations
Contributions
M.W.: conceptualization, methodology, data curation, and writing—original draft. Y.S.: conceptualization and writing—original draft. Y.W.: data curation and writing—reviewing and editing.
Corresponding author
Ethics declarations
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
The authors affirm that human research participants provided informed consent for publication of the aggregate data produced in the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wu, M., Shu, Y. & Wang, Y. Exposure to mixture of heavy metals and muscle strength in children and adolescents: a population-based study. Environ Sci Pollut Res 29, 60269–60277 (2022). https://doi.org/10.1007/s11356-022-19916-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-022-19916-2