
Abstract
Human exposure to arsenic (As) is a global public health concern that frequently occurs through both dietary and non-dietary pathways. This is the first systematic field study that investigated the drinking water (n = 190) for concentrations of total As (AsT) and its inorganic species such as arsenate As(V) and arsenite As(III) and organic species including monomethylarsonic acid (MMA) and dimethylarsenic acid (DMA) collected from Khyber Pakhtunkhwa, Pakistan. The concentrations of AsT surpassed (from 1.2- to 23-fold) the world health organization (WHO) drinking water guidelines in 28% samples collected from Dera Ismail Khan (D.I. Khan) and Lakki Marwat. Results revealed that among As species, As(III) showed the highest concentration (116 µg L−1) in drinking water samples. In addition, the results revealed that the chronic or non-cancer risk (HQ > 1) and cancer risk (1.0E-03 to 1.0E-06) values were above their respective safe limits. Further, As species concentrations were determined in consumer biomarkers (n = 60) such as blood (red blood cells and plasma), hair, nails, and urine. The highest AsT (170 µg kg−1) accumulation was observed in hair samples collected from the resident of D.I. Khan District. The study revealed that high As-contaminated drinking water led to its accumulation in human body that could threaten the exposed population with hazardous chronic and cancer diseases.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Arsenic (As) is one of the most hazardous and ubiquitous metalloids occurring in natural water systems (Hare et al. 2019; Shukla et al. 2018; Zeng et al. 2018). As originates in water from the anthropogenic and natural sources (Kippler et al. 2016; Kumarathilaka et al. 2018). The As-contaminated drinking water has been reported in more than 70 countries and threatens over 130 million human populations (Gunduz et al. 2017; Rasool et al. 2016). Exposure to As contamination in drinking water led to both chronic and acute health problems (Rasheed et al. 2017; Sun et al. 2014). Chronic health effects include abdominal pain, black foot disease, cardiovascular disease, diabetes, hypertension, nausea, severe diarrhea, vomiting, gastroenteritis and neurological manifestations, reproductive disorder, fetal mortality, inhabit the mental growth of children, DNA damage and immune deficiency, hyper- and hypo-pigmentation, keratosis, and respiratory problems, and increase male infertility risk. The carcinogenic effects of As include cancer (bladder, kidney, liver, lungs, skin, and prostrate) (Brahman et al. 2016; Muhammad et al. 2010; Tabassum et al. 2018; Twaddle et al. 2018).
Arsenic has both organic and inorganic species in water, which differs not only in properties (biological, chemical, and physical) but also in their toxicities (Devesa et al. 2008). Inorganic species such as arsenate As(V) and arsenite As(III) have higher toxicity than organic species, including monomethylarsonic acid (MMA) and dimethylarsinic acid (DMA) (WHO 2011). Among inorganic species, As(III) is more hazardous and prominent as compared to As(V) in natural water (Lim et al. 2007). However, depending on the ecological factors (temperature, pH, microorganisms, and oxygen) both species are inter-convertible (Hall 1999; Pizarro et al. 2003). Therefore, information about the As speciation is critical for true data on the biogeochemical cycling and health hazards (Brahman et al. 2016; Tchounwou et al. 2003). Generally, the inorganic species constitute more than 95% of total As (AsT) in drinking water. The As species could be absorbed in the digestive tract and lungs (Kazi et al. 2011). Kidneys eliminate (50–70%) of the absorbed As via methylation and passed through urine. However, when ingested As is higher than the amount excreted, the surplus amounts are accumulated in nails, hair, and other body tissues (Nielsen 2001). Various studies around the world had extensively measured the As concentrations in human hair and other biomarkers including blood and nails for epidemiological studies (Brima et al. 2006; Sampson et al. 2008).
Arsenic concentration in drinking water and human exposure have been reported from various parts of the world, i.e., Bangladesh (Wasserman et al. 2018), China (Li et al. 2018), India (Chatterjee et al. 2018), and USA (Hoover et al. 2017). Arsenic contamination in vegetables of the study area has been reported by Rahman et al. (2015). However, no attention was paid to the most sensitive and vulnerable compartment of ecosystem, i.e., water of the study area. Therefore, the present study was aimed to investigate the As contamination in drinking water and evaluate the potential risk to consumers including chronic risk such as average daily doze (ADD) and hazard quotient (HQ), and cancer risk (CR). This is the first systematic research study in Khyber Pakhtunkhwa province that investigated AsT, As(III), As(V), MMA, and DMA in drinking water and consumer biomarkers.
Materials and Methods
Study Area
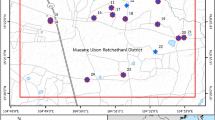
This study consisting of five districts: Karak, Lakki Marwat, Tank, Dera Ismail Khan (D.I. Khan), and Bannu of the Khyber Pakhtunkwa province in Pakistan (Fig. 1). The total human population in the study area is about 4.95 million. The area is very warm (48.9 °C) in summer and cold (2.8 °C) in winter. Hand pumps, bore holes, dug wells, tube wells, and springs/streams are used for drinking, household, and agriculture field irrigation. River Indus, Kuram and Gambila, and tub wells are mainly used for irrigation in the area. Agriculture is the main profession of the area with major crops including sugarcane, wheat, maize, barley, grams, rice, and vegetables.

Location map of the study area showing sampling sites
Water Sampling, Preparation, and Analysis
Drinking water (n = 5–18 replicates of each source in a district) from the hand pumps, bore holes, dug wells, tube wells, springs/streams, and ponds having total samples of n = 190 was collected within the study area. Water sources (hand pumps, bore holes, dug wells, and tube wells) were allowed to flow for 3–5 min before sample collection. Water from springs/streams and ponds were collected at a distance of three feet from banks and one feet depth. Electrical conductivity (EC) and pH were determined on-site using multi-parameter analyzers (COSORT C6030). Representative sealed bottles were pre-washed three times with respective sample and filled (100 mL). After collection, water was filtered with (0.45 mm) filter papers and acidified with 150 µL of nitric acid (65% HNO3) and stored in cooling blocks (– 20 °C) accordingly to the adopted method from Kippler et al. (2016). The latitudes and longitudes of each sampling points were measured by global position system (GPS, Garman eTrex 30) and used for distribution maps in the geographic information system (GIS) software.
Acidified water was analyzed for AsT using the inductively coupled plasma mass spectrometer (ICP-MS, Perkin Elmer Optima 7000 DV, USA) and the As species by high-performance liquid chromatography (HPLC) and ICP-MS through a column as HPLC–ICP-MS (PRP X-100, Hamilton Company, USA).
Standards and blanks were run on column to ascertain the accuracy of results in start and with regular interval of 10 water samples. The peaks developed were thoroughly studied for various As species. The column was washed with interval of 20 min during analysis.
Human Biomarkers Sampling and Preparation
Human biomarkers such as urine, blood, hair, and nails were used for As internal dose (Davis et al. 2017; Marchiset-Ferlay et al. 2012). In the study area, fasting human biomarkers (n = 60) samples such as blood, mid-stream spot urine, hair, and nails were collected early morning from the individuals having skin lesion symptoms to measure the As species concentrations. Adult and parents of children participants were given their consents for participation in this research.
Fasting blood samples were collected from the patients in K2 EDTA tubes. Blood were centrifuged to separate RBCs and plasma. Fasting mid-stream urine samples were collected in properly marked 100-mL sterilized plastic bottles. Blood and urine samples were acidified with HNO3 (65%) and preserved in cooling blocks (– 20 °C) for analyses.
Samples of 25 mL of urine and blood were put in 100-mL polypropylene tubes and one mL of 1% HNO3 (65%) was added and kept overnight as adopted from the method of Ettinger et al. (2017). AsT was determined using ICP-MS, while As(V), As(III), MMA, and DMA using HPLC–ICP-MS, connected through an anion-exchange column (PRP X-100, Hamilton Company, USA). Total inorganic As was then calculated by adding the concentrations of As(III) and As(V).
Scalp hair and nail samples were collected by stainless steel scissors and nail clippers, respectively. Each sample was sealed separately in zip-locked polyethylene bags. These samples were cleaned by washing and dried according to method adopted from Gault et al. (2008).
Hair and nail samples (100 mg) were put in polypropylene tubes of 50 mL and add 2 mL of concentrated HNO3 (65%) and 1 mL of H2O2 and kept overnight as adopted from Rahman et al. (2015). Samples were digested for 15 min each at 70 °C and 115 °C in the microwave-accelerated reaction system (CEM-Mars.V.194A05), respectively. Then digested samples were cooled and diluted with 1% of HNO3. AsT was determined using ICP-MS, while As(V), As(III), MMA, and DMA using HPLC–ICP-MS, connected through an anion-exchange column (PRP X-100, Hamilton Company, USA).
Precision and Accuracy
The accuracy of data was verified using samples of hair and urine as certified reference materials. Detection limit of instrument for As was 30 ng L−1. Recoveries of As concentration were observed at level of 96.4 ± 5.5% for standard reference materials and 98.5 ± 4.2% of sample triplicates. Glass wares and new plastic bottles were washed with 2% HNO3 (65%) and Milli-Q water. In this study, we followed the relevant human subject guidelines set by the ethical Committee University of Peshawar, Peshawar, Pakistan.
Risk Assessment
Basic information such as age, body weight, drinking water sources, containers, pre-treatment, and habits was collected using the constructed questionnaire and interview schedule during the field survey. Respondents, including children (1–16 years) and adults (17–65 years) both male and female, participated in this research. The As-contaminated drinking water through oral ingestion is the major human exposure pathway; therefore, risk assessments were calculated for chronic and carcinogenic risk categories.
Chronic Risk
Chronic risk or non-carcinogenic risk was calculated using exposure through ADD and HQ. The ADD values were calculated as adopted from the US (1998):
where C is the As contamination in drinking water (mg L−1), IR the rate (2 L day−1) of water ingestion, EF the exposure frequency (365 days year−1), ED the exposure duration (30 years), BW the body weight (adults 70 kg and children 30.6 kg), and AT is the average time 365 days year−1 × ED for non-carcinogens (Muhammad et al. 2010).
The values of ADD of As were used for the calculation of HQ as adopted from the US (1998):
where RfD is the reference dose (mg kg−1-day) having the value of 0.0003 mg kg−1-day (US 1998). The exposed population is assumed to be safe if HQ < 1 (Adimalla 2018; Adimalla et al. 2018; Muhammad et al. 2011).
Cancer Risk
Cancer risk was calculated according to equation following equitation:
where SF stands for As cancer slope factor and its value 1.5 was used in this study.
Mapping
Global positioning system data were put in GIS software (ArcGIS, ver. 9.3) and various concentration distribution maps were produced as adopted from Adimalla (2018) and Tabios and Salas (1985). Briefly, the AsT and its species concentrations in drinking water were evaluated with the WHO drinking water guidelines and interpolation was performed by the spatial analysis module using ArcGIS. The base map of Khyber Pakhtunkhwa was digitized from survey of Pakistan toposheets using Arc GIS software. The GPS data were imported in GIS platform and plotted using interpolation technique and the spatial distribution of AsT and its species such as As(V), As(III), MMA, and DMA was obtained (Fig. 2).

Concentration maps of AsT and its species at various sampling sites of the study area
Statistical Analysis
Data collected in the field and laboratory after analyzing the water and biomarkers samples were evaluated for ranges, mean, and standard deviation and plotted in Sigma plot ver. 12.5. Statistical analyses such as one-way ANOVA and correlation were performed by SPSS 26 (SPSS Inc., Chicago, IL, USA).
Results and Discussion
Basic Properties of Water
The pH of drinking water ranged 6.5–8.3, 6.0–8.2, 5.8–8.5, 6.0–8.2, and 6.5–8.5 with average values of 7.4, 7.3, 7.1, 7.3, and 7.3 in the D.I. Khan, Bannu, Lakki Marwat, Karak, and Tank Districts, respectively (Table 1). Drinking water pH showed slightly alkaline nature in the study area. The pH of drinking water has no direct effect on human health (Adimalla 2018; Adimalla and Venkatayogi 2017), but it can indirectly affect metals’ solubility and pathogen survival in aquatic habitats. The EC is also an important water quality parameter that represents the presence of salts in water. The values of EC ranged 210–395, 210–400, 210–390, 210–400, and 230–390 µS cm−1 with mean values of 286, 298, 299, 297, and 291 µS cm−1 in the D.I. Khan, Bannu, Karak, Lakki Marwat, and Tank Districts, respectively (Table 1). The highest pH and EC values were observed in samples collected from D.I. Khan and Karak Districts. Results showed that pH and EC values of drinking water in the studied districts were found within their respective safe drinking water permissible limits (WHO 2011). In the study area, pH values of drinking water were found lower, while those of EC are higher than those determined in Kohistan region, northern Pakistan by Muhammad et al. (2010).
Arsenic in Drinking Water
The concentrations of As species in water are summarized in Table 1 and that of each sampling site in Fig. 2. The concentrations of AsT ranged 0.06–231, 0.22–8.71, 0.19–12.2, 0.02–5.37, and 0.12–0.61 µg L−1 in the drinking water collected from D.I. Khan, Bannu, Lakki Marwat, Karak, and Tank District, respectively (Table 1). AsT and As(III) showed highest mean concentrations of 21.8 µg L−1 and 10.9 µg L−1 in the D.I. Khan District followed by 1.36 µg L−1 and 1.18 µg L−1 in Lakki Marwat. As(V) revealed highest mean concentrations of 6.94 µg L−1 in the D.I. Khan, followed by Bannu (0.52 µg L−1). The DMA (2.36 µg L−1) and MMA (1.41 µg L−1) revealed significantly (p < 0.001) higher mean concentrations in the D.I. Khan as compared to other studied districts (Fig. 2). Result revealed that inorganic As species exhibited higher levels as compared to organic. The AsT concentrations had surpassed the safe drinking water guidelines formulated by WHO (2011) in 28% and 2% samples of D.I. Khan and Lakki Marwat by 1.4–23 and 1.2-fold, respectively. Higher contamination of AsT in the studied drinking water was consistent with previous study from Sindh, southern Pakistan (Brahman et al. 2013). The As contamination in drinking water of the study area was observed multifold lower than that of the Cambodia, Taiwan, and southern Pakistan (Fig. 3). Higher contamination of As could result in higher potential chronic and carcinogenic risks in those parts of the world.

Comparison of AsT and its species concentrations reported from different countries of the world a (Brahman et al. 2016; Brahman et al. 2013; Gault et al. 2008; Lin et al. 1998; Mandal et al. 2003; Meza et al. 2004; Monrad et al. 2017) and As species concentrations in biomarkers of this study with precious studies conducted in other countries b (Brahman et al. 2016; Dhar et al. 1997; Janasik et al. 2017; Lin et al. 1998; Mandal et al. 2003; Sakamoto et al. 2010)
Arsenic contamination in water originates from natural (weathering of bedrocks and ore deposits, and chemical release of As-bound minerals under anoxic or oxic conditions) (Smedley and Kinniburgh 2002; Fendorf et al. 2010; Michael 2013) and anthropogenic (agrochemicals mining, groundwater over abstraction, and industrial waste) sources (Azizullah et al. 2011; Mandal and Suzuki 2002; Winkel et al. 2011). Higher As contaminations in drinking water of D.I. Khan District could be attributed to the disbanding of As-rich mineral sediments supplied from the Himalayas by the Indus River. The As contamination may be precipitated with time and percolated or leached down to the groundwater through biogeochemical processes (Baig et al. 2010; Brahman et al. 2016). The As-contaminated groundwater and surface water used for drinking purposes could result in direct human exposure (Muhammad et al. 2010) or indirectly by uptake of food grown on contaminated water (Davis et al. 2017). Chronic human exposure to As(III), As(V), and AsT through consumption of contaminated water and food has been associated with hyperkeratosis, skin pigmentation, spotted melanosis, and lung cancer (Yoshida et al. 2004). The toxicity of As depends on its species that are inter-convertible (Brima et al. 2006). Inorganic As specie like As(V) is metabolized and reduced to As(III), followed by oxidative methylation in human blood. Then they were taken up by hepatocytes and detoxified to methylate of DMA and MMA (Hsueh et al. 1998). These metabolized methylated organic As species are less toxic than inorganic species (Adair et al. 2005). However, recently, the metabolized As organic species have been identified to be more genotoxic than inorganic one (Brima et al. 2006; Hsueh et al. 1998).
Risk Assessment
Arsenic ingestion through oral pathway is the major human exposure route (ATSDR 2000). Water and food through oral intake have been reported as the major source of As, with minor share inhalation/ingestion or dermal absorption of airborne soil particles (Brahman et al. 2016; Meacher et al. 2002; Sharifi et al. 2018). Daily enrichment of As through water consumption is a more precise tool for calculating human exposure. Human exposure to AsT concentrations through drinking water consumptions in five districts of Khyber Pakhtunkwa has been summarized in Fig. 4a–c. Results showed the highest (6.24E–04 mg Kg−1-day) ADD values through drinking water consumption for consumers of D.I. Khan District, followed by Lakki Marwat, while the lowest in Tank District (Fig. 4a). Higher consumptions of As in the D.I. Khan District were attributed to higher contamination of drinking water as compared to other districts. As is one of the most hazardous elements; therefore, the prevalence of increase in skin lesion disease was reported even at a low level (5–10 µg L−1) of As exposure in drinking water (Yoshida et al. 2004).

Health risk assessment via drinking water exposure in five districts of Khyber Pakhtunkwa, Pakistan: a average daily intake of AsT, b HQ values, and c CR for the local people
Exposure to higher rate of As consumption in the study area led to higher HQ values > 3, and CR values 1.0E-03 for adults and children in the D.I. Khan District (Fig. 4b, Fig. 4c). Chronic and carcinogenic risk values in the D.I. Khan District of the study area had surpassed the safe limits set by USEPA (1999). Children showed higher consumption of As, HQ, and CR values. Children are more vulnerable to the As toxicity and risk through oral consumption (Waheed et al. 2013). The CR values for both adults and children residing in D.I. Khan District were highest and observed to have potential for developing various health problems, including cancer. Additionally, the intake of As-contaminated water for 8–10 years develops the symptoms of arsenicosis in exposed population (Anawar et al. 2002; Sampson et al. 2008). Chronic and cancer risk values were observed multifold higher than those reported for drinking water of Kohistan region by Muhammad et al. (2010) but lower than those reported in Muzzafar Garh, south Punjab, Pakistan (Nickson et al. 2005). Findings of this study indicated that As intake through water is subjected to the amount of ingested water and As contamination levels.
Low-level long-term As exposure causes various human organ toxicities as reported in the clinical investigation (Kapaj et al. 2006; Rahman et al. 2005). Residents in D.I. Khan showed the highest health issues, including skin diseases, kidney problems, diabetes, gastroenteritis, developmental abnormalities, liver failures and cardiovascular diseases, skin lesions, and cancer as compared to other selected districts (Table 2). During the survey, it was observed that the population of the study area belongs to high rate of poverty, ignorance, and illiteracy. Women play a key role in the management of household and bring water at a distance from remote area to meet their needs. Unfortunately, female population lack awareness of drinking water and sanitation importance and modern approaches of hygiene promotion and behavior change. Skin lesions and diabetes are the prevailing health problem in As-poisoning countries like Bangladesh, China, and India (Juan Guo et al. 2001; Kippler et al. 2016; Smith et al. 2000).
Arsenic Concentrations in Human Biomarkers
Arsenic species concentrations in the human biomarkers including hair, nails, plasma, RBCs, and urine of the five studied districts were summarized (Table 3). Hair showed the highest mean AsT concentrations (84.6 µg g−1), followed by As(III) (35.3 µg g−1) in the D.I. Khan, while the lowest (BD) concentration of As(V) and MMA in Karak (Table 3). Nails showed the highest mean AsT concentrations (79.5 µg g−1), followed by As(III) (18.6 µg g−1) in the D.I. Khan, while the lowest (BD) concentrations of DMA and MMA in Karak (Table 3). Plasma showed the highest mean AsT concentrations (32.1 µg L−1) in the Lakki Marwat followed by Bannu District. The highest concentrations of As(III) were 23.7 µg g−1 in the hair samples of Bannu, while the lowest (BD) concentrations of DMA and MMA were reported in Karak and Lakki Marwat Districts (Table 3). The RBCs showed the highest mean AsT concentrations (47.5 µg L−1), followed by As(III) (23.7 µg L−1), while the lowest (BD) concentrations for As(V), DMA, and MMA in Lakki Marwat District (Table 3). Urine showed the highest mean concentrations (48.1 µg L−1) of AsT, while the lowest (BD) concentrations for As(V), MMA, and DMA in Lakki Marwat (Table 3). Higher AsT concentration was consistent with previous reported studies (a comparison is given in Fig. 3). The As levels in hair and other human biomarkers suggest the toxic effects. Results showed considerably higher As concentrations in hair than other human tissues. Higher As concentrations in hair could be attributed to its natural protein composition (α-keratin), which has multiple subunits as cysteine enriched with sulfur-containing amino acids. Sulfur-containing or reduced sulfur groups regularly offer spots for complexation of metalloids such as As expelled by the body (Byrne et al. 2010). Thus, As enrichment in hair could be used as a pinpointing sign of As toxicity (Brahman et al. 2016; Freeman et al. 2004; Karagas et al. 2004).
Conclusions
Arsenic contamination levels in drinking water of the D.I. Khan District were the highest as compared to the studied districts and had surpassed (23-fold) the safe drinking water WHO guidelines.
Higher As contamination led to greater human exposure and accumulation in biomarkers and posed higher risk to the consumers (adults and children) in D.I. Khan District. Drinking water of D.I. Khan District showed positive correlation with the human biomarkers. Arsenicosis clinical complications, including skin disorders, gastrointestinal, respiratory, and weakness problems, were reported among residents.
This study concluded that D.I. Khan water is unsuitable for drinking purposes and household daily uses. Therefore, it is imperative for policy-making bodies to take strict actions for water remediation and formulate policies to create awareness in the local community of water collection, storage, and remediation.
References
Adair BM, Waters SB, Devesa V, Drobna Z, Styblo M, Thomas DJ (2005) Commonalities in metabolism of arsenicals. Environ Chem 2:161–166
Adimalla N (2018) Groundwater quality for drinking and irrigation purposes and potential health risks assessment: a case study from semi-arid region of south India. Expo Health. https://doi.org/10.1007/s12403-018-0288-8
Adimalla N, Venkatayogi S (2017) Mechanism of fluoride enrichment in groundwater of hard rock aquifers in Medak, Telangana State, South India. Environ Earth Sci 76:45
Adimalla N, Li P, Qian H (2018) Evaluation of groundwater contamination for fluoride and nitrate in semi-arid region of Nirmal Province, south India: a special emphasis on human health risk assessment (HHRA). Hum Ecol Risk Assess. https://doi.org/10.1080/10807039.2018.1460579
Anawar H, Akai J, Mostofa K, Safiullah S, Tareq S (2002) Arsenic poisoning in groundwater: health risk and geochemical sources in Bangladesh. Environ Int 27:597–604
ATSDR (2000) Toxicology Profile for Arsenic. Agency for Toxic Substances and Disease Registry, US Department of Health and Human Services, TP-92/02, Atlanta, Georgia
Azizullah A, Khattak MNK, Richter P, Häder D-P (2011) Water pollution in Pakistan and its impact on public health—a review. Environ Int 37:479–497
Baig JA, Kazi TG, Shah AQ, Kandhro GA, Afridi HI, Khan S, Kolachi NF (2010) Biosorption studies on powder of stem of Acacia nilotica: removal of arsenic from surface water. J Hazard Mater 178:941–948
Brahman KD, Kazi TG, Afridi HI, Naseem S, Arain SS, Ullah N (2013) Evaluation of high levels of fluoride, arsenic species and other physicochemical parameters in underground water of two sub districts of Tharparkar, Pakistan: a multivariate study. Water Res 47:1005–1020
Brahman KD et al (2016) Exposure of children to arsenic in drinking water in the Tharparkar region of Sindh, Pakistan. Sci Total Environ 544:653–660
Brima EI, Haris PI, Jenkins RO, Polya DA, Gault AG, Harrington CF (2006) Understanding arsenic metabolism through a comparative study of arsenic levels in the urine, hair and fingernails of healthy volunteers from three unexposed ethnic groups in the United Kingdom. Toxicol Appl Pharmacol 216:122–130. https://doi.org/10.1016/j.taap.2006.04.004
Byrne S et al (2010) Were Chinchorros exposed to arsenic? Arsenic determination in Chinchorro mummies’ hair by laser ablation inductively coupled plasma-mass spectrometry (LA-ICP-MS). Microchem J 94:28–35
Chatterjee D, Adak S, Banerjee N, Bhattacharjee P, Bandyopadhyay AK, Giri AK (2018) Evaluatıon of health effects, genetıc damage and telomere length ın children exposed to arsenic in West Bengal, İndia. Mutat Res, Genet Toxicol Environ Mutagen 1:2. https://doi.org/10.1016/j.mrgentox.2018.06.012
Davis MA et al (2017) Assessment of human dietary exposure to arsenic through rice. Sci Total Environ 586:1237–1244
Devesa V, Velez D, Montoro R (2008) Effect of thermal treatments on arsenic species contents in food. Food Chem Toxicol 46:1–8
Dhar RK et al (1997) Groundwater arsenic calamity in Bangladesh. Curr Sci 73:48–59
EPA U (1999) US Environmental Protection Agency (US EPA), A Risk Assessment – Multiway Exposure Spreadsheet Calculation Tool. Washington, DC
Ettinger AS et al (2017) Arsenic levels among pregnant women and newborns in Canada: results from the Maternal-Infant Research on Environmental Chemicals (MIREC) cohort. Environ Res 153:8–16
Fendorf S, Michael HA, van Geen A (2010) Spatial and temporal variations of groundwater arsenic in South and Southeast Asia. Science 328:1123–1127. https://doi.org/10.1126/science.1172974
Freeman LEB, Dennis LK, Lynch CF, Thorne PS, Just CL (2004) Toenail arsenic content and cutaneous melanoma in Iowa. Am J Epidemiol 160:679–687
Gault AG et al (2008) Arsenic in hair and nails of individuals exposed to arsenic-rich groundwaters in Kandal province, Cambodia. Sci Total Environ 393:168–176
Gunduz O et al (2017) The health risk associated with chronic diseases in villages with high arsenic levels in drinking water supplies. Expo Health 9:261–273. https://doi.org/10.1007/s12403-016-0238-2
Guo JX, Fujino Y, Kaneko S, Wu K, Xia Y, Yoshimura T (2001) Arsenic contamination of groundwater and prevalence of arsenical dermatosis in the Hetao plain area, Inner Mongolia, China. In: Shi X, Castranova V, Vallyathan V (eds) Molecular mechanisms of metal toxicity and carcinogenesis. Springer, New York, pp 137–140
Hall GM (1999) Stability of inorganic arsenic (III) and arsenic (V) in water samples. J Anal At Spectrom 14:205–213
Hare V, Chowdhary P, Kumar B, Sharma D, Baghel VS (2019) Arsenic toxicity and its remediation strategies for fighting the environmental threat. In: Chowdhary P, Bharagava RN (eds) Emerging and eco-friendly approaches for waste management. Springer, Singapore, pp 143–170
Hoover J, Gonzales M, Shuey C, Barney Y, Lewis J (2017) Elevated arsenic and uranium concentrations in unregulated water sources on the Navajo Nation, USA. Expo Health 9:113–124
Hsueh Y-M, Wu W-L, Huang Y-L, Chiou H-Y, Tseng C-H, Chen C-J (1998) Low serum carotene level and increased risk of ischemic heart disease related to long-term arsenic exposure. Atherosclerosis 141:249–257
Janasik B, Zawisza A, Malachowska B, Fendler W, Stanislawska M, Kuras R, Wasowicz W (2017) Relationship between arsenic and selenium in workers occupationally exposed to inorganic arsenic. J Trace Elem Med Biol 42:76–80. https://doi.org/10.1016/j.jtemb.2017.04.007
Kapaj S, Peterson H, Liber K, Bhattacharya P (2006) Human health effects from chronic arsenic poisoning–a review. J Environ Sci Health, Part A 41:2399–2428
Karagas MR, Tosteson TD, Morris JS, Demidenko E, Mott LA, Heaney J, Schned A (2004) Incidence of transitional cell carcinoma of the bladder and arsenic exposure in New Hampshire. Cancer Causes Control 15:465–472
Kazi TG et al (2011) Determination of arsenic in scalp hair of children and its correlation with drinking water in exposed areas of Sindh Pakistan. Biol Trace Elem Res 143:153–162
Kippler M, Skröder H, Rahman SM, Tofail F, Vahter M (2016) Elevated childhood exposure to arsenic despite reduced drinking water concentrations—a longitudinal cohort study in rural Bangladesh. Environ Int 86:119–125
Kumarathilaka P, Seneweera S, Meharg A, Bundschuh J (2018) Arsenic speciation dynamics in paddy rice soil-water environment: sources, physico-chemical, and biological factors-a review. Water Res 140:403–414
Li R, Kuo Y-M, Liu W-W, Jang C-S, Zhao E, Yao L (2018) Potential health risk assessment through ingestion and dermal contact arsenic-contaminated groundwater in Jianghan Plain. China. Environ Geochem Health 40(4):1585–1599
Lim M-S, Yeo IW, Clement TP, Roh Y, Lee K-K (2007) Mathematical model for predicting microbial reduction and transport of arsenic in groundwater systems. Water Res 41:2079–2088
Lin T-H, Huang Y-L, Wang M-Y (1998) Arsenic species in drinking water, hair, fingernails, and urine of patients with Blackfoot disease. J Toxicol Environ Health Part A 53:85–93. https://doi.org/10.1080/009841098159376
Mandal BK, Suzuki KT (2002) Arsenic round the world: a review. Talanta 58:201–235
Mandal BK, Ogra Y, Suzuki KT (2003) Speciation of arsenic in human nail and hair from arsenic-affected area by HPLC-inductively coupled argon plasma mass spectrometry. Toxicol Appl Pharmacol 189:73–83. https://doi.org/10.1016/S0041-008X(03)00088-7
Marchiset-Ferlay N, Savanovitch C, Sauvant-Rochat M-P (2012) What is the best biomarker to assess arsenic exposure via drinking water? Environ Int 39:150–171
Meacher DM et al (2002) Estimation of multimedia inorganic arsenic intake in the US population. Hum Ecol Risk Assess 8:1697–1721
Meza MM, Kopplin MJ, Burgess JL, Gandolfi AJ (2004) Arsenic drinking water exposure and urinary excretion among adults in the Yaqui Valley, Sonora, Mexico. Environ Res 96:119–126
Michael HA (2013) An arsenic forecast for China. Science 341:852–853
Monrad M et al (2017) Low-level arsenic in drinking water and risk of incident myocardial infarction: a cohort study. Environ Res 154:318–324
Muhammad S, Shah MT, Khan S (2010) Arsenic health risk assessment in drinking water and source apportionment using multivariate statistical techniques in Kohistan region, northern Pakistan. Food Chem Toxicol 48:2855–2864
Muhammad S, Shah MT, Khan S (2011) Health risk assessment of heavy metals and their source apportionment in drinking water of Kohistan region, northern Pakistan. Microchem J 98:334–343
Nickson R, McArthur J, Shrestha B, Kyaw-Myint T, Lowry D (2005) Arsenic and other drinking water quality issues, Muzaffargarh District, Pakistan. Appl Geochem 20:55–68
Nielsen FH (2001) Trace minerals. In: Shills M, Olson J, Shike M, Ross AC (eds) Nutrition in health and sickness, 9th edn. McGraw-Hill, Mexico City, pp 328–331
Pizarro I, Gómez M, Cámara C, Palacios M (2003) Arsenic speciation in environmental and biological samples: extraction and stability studies. Anal Chim Acta 495:85–98
Rahman MM et al (2005) Murshidabad—One of the nine groundwater arsenic-affected districts of West Bengal, India. Part I: magnitude of contamination and population at risk. Clin Toxicol 43:823–834
Rahman M et al (2015) Associations of total arsenic in drinking water, hair and nails with serum vascular endothelial growth factor in arsenic-endemic individuals in Bangladesh. Chemosphere 120:336–342
Rasheed H, Slack R, Kay P, Gong YY (2017) Refinement of arsenic attributable health risks in rural Pakistan using population specific dietary intake values. Environ Int 99:331–342
Rasool A, Farooqi A, Xiao T, Masood S, Kamran MA (2016) Elevated levels of arsenic and trace metals in drinking water of Tehsil Mailsi, Punjab, Pakistan. J Geochem Explor 169:89–99
Sakamoto M, Murata K, Kubota M, Nakai K, Satoh H (2010) Mercury and heavy metal profiles of maternal and umbilical cord RBCs in Japanese population. Ecotoxicol Environ Saf 73:1–6
Sampson M, Bostick B, Chiew H, Hagan J, Shantz A (2008) Arsenicosis in Cambodia: case studies and policy response. Appl Geochem 23:2977–2986
Sharifi R, Moore F, Keshavarzi B, Badiei S (2018) Assessment of health risks of arsenic exposure via consumption of crops. Expo Health 10:129–143. https://doi.org/10.1007/s12403-017-0250-1
Shukla T, Khare R, Kumar S, Lakhwani D, Sharma D, Asif MH, Trivedi PK (2018) Differential transcriptome modulation leads to variation in arsenic stress response in Arabidopsis thaliana accessions. J Hazard Mater 351:1–10
Smedley PL, Kinniburgh DG (2002) A review of the source, behaviour and distribution of arsenic in natural waters. Appl Geochem 17:517–568. https://doi.org/10.1016/S0883-2927(02)00018-5
Smith AH et al (2000) Arsenic-induced skin lesions among Atacameno people in Northern Chile despite good nutrition and centuries of exposure. Environ Health Perspect 108:617
Sun H-J, Rathinasabapathi B, Wu B, Luo J, Pu L-P, Ma LQ (2014) Arsenic and selenium toxicity and their interactive effects in humans. Environ Int 69:148–158
Tabassum RA et al (2018) Health risk assessment of drinking arsenic-containing groundwater in Hasilpur, Pakistan: effect of sampling area, depth, and source. Environ Sci Pollut Res Int. https://doi.org/10.1007/s11356-018-1276-z
Tabios GQ III, Salas JD (1985) A comparative analysis of techniques for spatial interpolation of precipitation JAWRA. J Am Water Resour Assoc 21:365–380
Tchounwou PB, Patlolla AK, Centeno JA (2003) Invited reviews: carcinogenic and systemic health effects associated with arsenic exposure—a critical review. Toxicol Pathol 31:575–588
Twaddle NC, Vanlandingham M, Beland FA, Doerge DR (2018) Metabolism and disposition of arsenic species after repeated oral dosing with sodium arsenite in drinking water. II. Measurements in pregnant and fetal CD-1 mice. Food Chem Toxicol 115:178–184
US EPA (1998) United States Environmental Protection Agency, Integrated Risk Information System (IRIS)
Waheed S, Malik RN, Jahan S (2013) Health risk from As contaminated fish consumption by population living around River Chenab, Pakistan. Environ Toxicol Pharmacol 36:579–587
Wasserman GA et al (2018) A cross-sectional study of water arsenic exposure and intellectual function in adolescence in Araihazar, Bangladesh. Environ Int 118:304–313
WHO (2011) Guidelines for drinking water quality, 4th edn. Recommendations, Geneva
Winkel LH et al (2011) Arsenic pollution of groundwater in Vietnam exacerbated by deep aquifer exploitation for more than a century. Proc Natl Acad Sci 108:1246–1251
Yoshida T, Yamauchi H, Sun GF (2004) Chronic health effects in people exposed to arsenic via the drinking water: dose–response relationships in review. Toxicol Appl Pharmacol 198:243–252
Zeng Y, Zhou Y, Zhou J, Jia R, Wu J (2018) Distribution and Enrichment factors of high-arsenic groundwater in Inland Arid area of P. R. China: a case study of the Shihezi area, Xinjiang. Expo Health 10:1–13. https://doi.org/10.1007/s12403-016-0241-7
Acknowledgements
This research work was financially supported by the Higher Education Commission (HEC), Islamabad, Pakistan and University of Peshawar, Pakistan.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rehman, U., Khan, S. & Muhammad, S. Ingestion of Arsenic-Contaminated Drinking Water Leads to Health Risk and Traces in Human Biomarkers (Hair, Nails, Blood, and Urine), Pakistan. Expo Health 12, 243–254 (2020). https://doi.org/10.1007/s12403-019-00308-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-019-00308-w