
Abstract
Background
SPECT myocardial perfusion imaging (MPI) provides an assessment of LV mechanical dyssynchrony (LVMD) which correlates with CVD outcomes in diverse populations including those awaiting renal transplant (RT). The current study examines the association of LVMD on pre-transplant MPI with long-term CVD mortality post RT.
Methods
We identified consecutive patients who underwent RT at the University of Alabama at Birmingham between 2008 and 2012 from our prospectively collected database. 675 patients in the database underwent MPI and had images amenable for phase analysis. A blinded investigator retrieved the studies and derived LVMD indices including histogram bandwidth (BW), standard deviation (SD), phase peak, phase skewness, and phase kurtosis. The primary outcome was CVD death after RT.
Results
The study cohort had a median age of 54 years, 56% were men, 43% had diabetes, and 7% had prior myocardial infarction. Patients were on dialysis for a median of 3.4 years prior to RT and 34% received living donor transplants. During a median follow-up time after RT of 4.7 years (IQR 3.5 to 6.3 years) 59 patients (9%) succumbed to CVD death. Patients with wider BW, wider SD, lower skewness, and lower kurtosis had an increased risk of CVD death. On multivariate adjustment, BW and skewness remained as independent predictors of CVD deaths.
Conclusions
LVMD by phase analysis of gated SPECT MPI is associated with increased risk of CVD death after RT. This association is independent of demographics, comorbidities, and traditional findings on MPI and added incremental prognostic information. Assessment of LVMD should be considered for risk stratification in these patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Cardiovascular disease (CVD) is the leading cause of death in patients with chronic kidney disease, especially those with end-stage renal disease (ESRD).1,2,3 While renal transplantation (RT) offers a viable treatment option for patients with ESRD, it is largely limited by the shortage of available organs, and CVD continues to be a major cause of death even after RT.3 Prior to undergoing RT, patients generally undergo a thorough multi-system evaluation that includes an assessment of CVD and its risk factors.4,5 Risk assessment prior to RT is different than that performed prior to non-transplant-related procedures in that it has to account for long-term risk to make the best use of the available donor organs.6,7 The scientific statement by the American Heart Association (AHA) and the American College of Cardiology (ACC) on cardiac disease evaluation and management among kidney and liver transplantation candidates, which was endorsed by the American Society of Transplant Surgeons, American Society of Transplantation, and National Kidney Foundation, recommends the use of non-invasive cardiac stress testing for risk stratification in RT candidates based on the presence of risk factors.5 We and others have demonstrated the value of cardiac stress testing with single-photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) performed during the pre-transplant evaluation process on predicting long-term outcomes after RT.8,9
While MPI provides important information regarding myocardial perfusion and left ventricular ejection fraction (LVEF), it can also provide an assessment of LV mechanical dyssynchrony (LVMD).10,11 LVMD is associated with inefficient cardiac contractility, remodeling, heart failure, arrhythmias, and death.12 Multiple studies have demonstrated that the presence of LVMD on phase analysis of MPI provides prognostic data in diverse populations including those with ESRD awaiting RT.13,14,15,16,17,18,19,20 In the current study, we examine the association of LVMD on pre-transplant MPI with long-term CVD mortality post RT.
Methods
Patient Selection
We identified consecutive patients who underwent RT at the University of Alabama at Birmingham between 2008 and 2012 from our prospectively collected database. This cohort has been previously described in detail.8 Of the 1,189 patients in the database, 370 did not have an MPI during evaluation for RT, and we were unable to perform phase analysis on 144 patients due to improper image archiving or gating artifact. Thus, the remaining 675 patients with phase analysis data from MPI performed during evaluation for RT constituted the cohort for the current study.
The study was approved by the institutional review board and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Clinical Data
Patient demographics and clinical information such as medication intake and comorbidities at time of RT evaluation were obtained from chart review. Hypertension was defined as systolic blood pressure > 140 mm Hg, or diastolic blood pressure > 90 mm Hg or intake of anti-hypertensive medications. Diabetes mellitus was defined as fasting blood glucose ≥ 126 mg/dL, or A1c ≥ 6.5% or intake of hypoglycemic agents or insulin. Dyslipidemia was defined as elevated total cholesterol or low-density lipoprotein levels beyond the values set by the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III guidelines.21 Myocardial infarction was defined using the Fourth Universal Definition of Myocardial Infarction.22 Patients were segregated based on whether they were on dialysis at the time of evaluation for RT and the mode of dialysis (hemodialysis or peritoneal dialysis) and on the type of RT received (living or deceased donor).
Stress MPI and Phase Analysis
Stress MPI was performed as part of RT evaluation at the discretion of the clinical team. Gated Tc-99m sestamibi single-photon emission computed tomography MPI was performed using stress/rest or stress-only one-day protocol according to the American Society of Nuclear Cardiology guidelines as previously described.8,23,24 Rest images were performed if the stress images were abnormal or if there was uncertainty in the interpretation of the stress images. Image interpretation was performed in the absence of attenuation or scatter correction. The presence and extent of perfusion abnormalities was determined by a software program (Corridor4DM) with visual supervision.25 MPI was considered abnormal when there was a perfusion defect involving more than 5% of LV myocardium or when LVEF was less than 50%. The gated image datasets were retrieved and processed for phase analysis by a single investigator who was blinded to the clinical characteristics of the patients (except for gender) and their outcome as previously described. In brief, a three-dimensional count distribution was extracted from each of the LV short-axis datasets and submitted to a Fourier analysis, generating a phase distribution (0° to 360°) representing the onset of mechanical contraction spanning a duration of one R–R interval and displayed on a histogram using a validated software program (Emory Cardiac Toolbox). The LVMD indices derived from the phase analysis include histogram bandwidth (BW), standard deviation (SD), phase peak, phase skewness, and phase kurtosis. Phase peak represents the peak of the phase histogram. Phase SD is the SD of the phase distribution, while BW comprises 95% of the phase distribution. Phase skewness refers to the symmetry of the phase histogram—a higher skewness indicates distribution more skewed to the right with a longer tail to the right of the peak phase. Phase kurtosis accounts for how peaked the distribution is.11
Outcomes
The primary outcome was CVD death after RT. Outcomes were obtained from chart review, contacting referring physicians, and using the Social Security Death Index. The outcomes were adjudicated by a blinded reviewer. When the cause of death was not known, it was considered to be from CVD causes.
Statistical Analysis
Continuous data were expressed as median and interquartile ranges (IQR) and compared using the Mann–Whitney test. Categorical data were displayed as frequencies and percentages and compared using Pearson’s Chi-square test. Kaplan–Meier survival curves were constructed to evaluate cumulative event rates and the log-rank test was used to assess for differences between groups. Patients were categorized into groups based on cut-offs for phase BW (> 56\(^\circ \)) and SD (≥ 21\(^\circ \)) based on a previous study that assessed the prognostic value of these parameters in patients with ESRD.13 Since we are not aware of prior data with phase skewness and outcomes in this population, we divided the cohort based on median skewness. Outcome analysis treated the date of RT as “time 0.” Follow-up time was defined by a qualifying event or last event-free encounter up to June 16, 2016. Cox proportional hazards models were used to estimate the unadjusted, age- and gender-adjusted, and multivariate-adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for CVD death for the different LVMD parameters expressed as continuous variables. For the multivariate model, we adjusted for variables that were different between patients who had or did not have CVD death after renal transplantation (P < 0.1 in Table 2). The proportional hazards assumption with respect to Cox-regression modeling was confirmed using “log minus log” survival plots. To test for incremental value of LVMD indices, nested Cox models were performed with and without these indices; the increase in Chi-square value was then reported and the corresponding P value up to 1° of freedom was obtained. All tests were 2-tailed, and a P value < 0.05 was considered statistically significant. All statistical analyses were carried out with SPSS Statistics version 25 (IBM, Inc., Armonk, NY).
Results
The baseline characteristics of the study cohort are shown in Table 1. Notably, the median age at transplant was 54 years and the majority of participants were male (56%). As expected in patients undergoing RT, the prevalence of comorbidities including hypertension, hyperlipidemia, and diabetes mellitus was high. However, only a small subset of patients had a history of prior myocardial infarction (7%). A good proportion of the patients were receiving cardiac medications as can be expected from their co-morbidity profile and more than one in every four patients were on insulin therapy. Most patients were on dialysis while awaiting RT. RT occurred at a median of 1.5 years (IQR 0.6 to 4 years) from the time of MPI. Around one-third of the patients received a living RT.
The cohort had a median (IQR) phase SD of 14° (11-19°), BW of 41° (31-53°), peak of 140° (126-155°), skewness of 3.9 (3.4-4.5), and kurtosis of 17 (12-23). Phase SD, BW, skewness, and kurtosis were highly linearly correlated (R values ranging from a low of 0.306 for SD and kurtosis, to a high of 0.929 for SD and BW, and 0.967 for skewness and kurtosis, all P values < 0.05). A phase SD ≥ 21° was present in 126 (19%) patients and BW > 56° in 134 (20%) patients. The distribution of the baseline characteristics according to these LVMD parameters are shown in Table 1. Patients with LVMD were more likely to be men, younger in age, and have abnormal MPI but the other baseline characteristics were not statistically different between the two groups.
During a median follow-up time after RT of 4.7 years (IQR 3.5 to 6.3 years), 59 patients (9%) succumbed to CVD death. The baseline characteristics stratified by CVD death are shown in Table 2. Patients who experienced a CVD death were older, more likely to have diabetes, were on dialysis for a longer period of time prior to RT, were more likely to have received a deceased vs. a living donor transplant, and more likely to have abnormal MPI. The LVMD parameters according to whether the patients experienced CVD death are shown in Table 3. Patients who died from a CVD cause had a wider BW, lower skewness and kurtosis, and borderline wider SD. On Kaplan–Meier analysis, patients with wider BW (Figure 1A), wider SD (Figure 1B), lower skewness (Figure 1C), and lower kurtosis (Figure 1D) had an increased risk of CVD death. A wider BW was associated with worse outcomes in patients irrespective of whether they received a deceased or living donor transplants, and whether they had been on dialysis for less than or more than 3.5 years (Figure 2). When analyzed as continuous variables, the LVMD parameters were associated with worse outcomes on unadjusted and age and gender adjusted analysis (Table 4). On multivariate adjustment, BW and skewness remained as independent predictors of CVD death, whereas the association with kurtosis (P = 0.054) and SD (P = 0.08) became non-significant (Table 4). Both phase skewness and BW added incremental prognostic value with the increase in chi-square from 29 to 34 (P = 0.02) and 35 (P = 0.01), respectively.

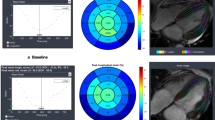
Impact of phase analysis parameters by SPECT MPI performed for RT evaluation on CVD mortality after RT. Kaplan–Meier survival plots stratified by A phase bandwidth, B standard deviation, C skewness, and D kurtosis

Impact of LVMD (assessed by bandwidth on phase histogram) on CVD mortality in patients receiving A deceased donor or B living donor kidney, and whether they have been on dialysis for C less than or D more than 3.5 years prior to RT
Discussion
The main finding of our study is that LVMD parameters derived from phase analysis of gated SPECT MPI performed during the evaluation for RT is associated with CVD death after transplantation. These data extend the prognostic value of LVMD parameters to the post-RT population and enhance the risk stratification capability of MPI performed during the RT evaluation process. Importantly, these data are incremental to what is currently used for risk stratification and can be derived from routinely performed MPI without the need for introducing additional testing.
Gated SPECT MPI has been shown to be an excellent tool for identifying patients with LVMD.26,27 LVMD is reflective of structural, electrical, and mechanical processes that occur at the myocardial, cellular, and molecular levels.12 LVMD has been linked to LV hypertrophy and fibrosis which are common in patients with ESRD.28 Indeed, patients with ESRD have been shown to have evidence of LVMD by MPI.29,30 In accordance with this, the median phase SD and BW in our study were higher than, and skewness and kurtosis lower than, what has been reported in normal populations which is consistent with the presence of LVMD in our patients.10 LVMD parameters derived from MPI associate with CVD outcomes in patients with coronary artery disease,14,17 heart failure,15,16,18,19 and the general population.20 In a cohort of 828 ESRD patients who were being evaluated for RT, we previously demonstrated that LVMD on MPI (reflected by phase BW >56° or SD ≥21°) correlated with lower 5-year survival.13 This association was independent of other factors including traditional findings on MPI. In the current study, we examined the outcome of patients who underwent RT. RT is associated with improved survival and quality of life compared to dialysis and therefore data derived in ESRD patients may not apply after RT.31 In this regard, we have recently shown that while LVEF and electrical repolarization (QT interval on electrocardiography) improve with RT, LVMD parameters are unaltered.32 Thus, our current finding that LVMD assessed on MPI pre-RT associates with worse CVD outcomes after RT is consistent with the literature.
CVD is the leading cause of death after RT.3 Patients with RT are known to have higher prevalence of coronary artery disease risk factors and are at increased risk of coronary events.33,34 Manifestation of CVD in the RT population is not limited to coronary artery disease, but also includes arrhythmia and sudden cardiac death.35 While the etiology of sudden cardiac death in patients with RT is not well defined, it is believed to be related to a complex interplay between myocardial remodeling, electrical remodeling, autonomic dysfunction, inflammation, hemodynamic factors, and electrolyte disturbances.36 Many of these factors can adversely impact LVMD. We have previously demonstrated that LVMD is independently associated with potential sudden cardiac death events in 917 patients with heart failure and reduced LVEF.18 While it is plausible that LVMD is associated with increased risk of sudden cardiac death in patients after RT, it is not possible to evaluate that in our study and this will need to be evaluated in future prospective studies.
We evaluated LVMD using an automated software that determines the onset of mechanical contraction based on Fourier analysis as previously described.11 In addition to being automated, this technique has been shown to have high reproducibility and repeatability.37 The application of this field to clinical care, therefore, requires only a software program that can assess phase analysis and basic quality control measures. Most prior studies discussed above used BW and SD as the LVMD parameters when evaluating prognosis. Our study confirmed, in a unique population of RT recipients, the prognostic value of these parameters. Using cut-off values from a prior study in ESRD, we reported a 2-fold increased risk for patients with wider phase distribution (comparable hazard ratios for phase BW > 56° and SD ≥ 21°). We have further found that phase kurtosis and skewness are also associated with increased risk. Our analysis indicates that skewness may be an important prognostic indicator in ESRD patients who underwent RT. Since there is scant data on skewness in other populations, we are not able to conjecture whether this is unique to patients post RT or more broadly generalizable, but it is certainly worth investigating in future studies.
To the best of our knowledge, our study is the first to evaluate the prognostic value of LVMD by phase analysis of MPI in patients after RT. However, we acknowledge several limitations. First, this is a retrospective study from a single tertiary care center and therefore suffers from the usual limitations of similar studies including selection and referral bias. Second, we were unable to include a subset of the MPI studies for phase analysis (inability to locate the study, improper image archiving or gating artifact) further contributing to selection bias. Third, we evaluated LVMD at one point in time prior to RT. Whether changes in LVMD parameters prior to or after RT impact CVD outcomes cannot be determined from our study.
New Knowledge Gained
The presence of LVMD by phase analysis of gated SPECT MPI performed for RT evaluation is associated with increased risk of CVD death after RT. This association is independent of demographics, comorbidities, and traditional findings on MPI and added incremental prognostic information. Routine assessment of LVMD should be considered for risk stratification in these patients.
Abbreviations
- BW:
-
Histogram bandwidth
- CVD:
-
Cardiovascular disease
- ESRD:
-
End-stage renal disease
- LVEF:
-
Left ventricular ejection fraction
- LVMD:
-
Left ventricular mechanical dyssynchrony
- MPI:
-
Myocardial perfusion imaging
- RT:
-
Renal transplant
- SD:
-
Standard deviation
- SPECT:
-
Single-photon emission computed tomography
References
Hage FG, Venkataraman R, Zoghbi GJ, Perry GJ, DeMattos AM, Iskandrian AE. The scope of coronary heart disease in patients with chronic kidney disease. J Am Coll Cardiol 2009;53:2129‐40.
Makar MS, Pun PH. Sudden cardiac death among hemodialysis patients. Am J Kidney Dis 2017;69:684‐95.
System USRD. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD.
Chadban SJ, Ahn C, Axelrod DA, Foster BJ, Kasiske BL, Kher V. KDIGO clinical practice guideline on the evaluation and management of candidates for kidney transplantation. Transplantation 2020;104:S11‐103.
Lentine KL, Costa SP, Weir MR, Robb JF, Fleisher LA, Kasiske BL, et al. Cardiac disease evaluation and management among kidney and liver transplantation candidates: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. J Am Coll Cardiol 2012;60:434‐80.
Rizk DV, Riad S, Hage FG. Screening for coronary artery disease in kidney transplant candidates. J Nucl Cardiol 2015;22:297‐300.
Bourque JM, Iskandrian AE, Hage FG. Screening pre-renal transplant: Risk factors appear key but important questions remain. J Nucl Cardiol 2018;25:2069‐71.
Ives CW, AlJaroudi WA, Kumar V, Farag A, Rizk DV, Oparil S, et al. Prognostic value of myocardial perfusion imaging performed pre-renal transplantation: Post-transplantation follow-up and outcomes. Eur J Nucl Med Mol Imaging 2018;45:1998‐2008.
Doukky R, Fughhi I, Campagnoli T, Wassouf M, Kharouta M, Vij A, et al. Validation of a clinical pathway to assess asymptomatic renal transplant candidates using myocardial perfusion imaging. J Nucl Cardiol 2018;25:2058‐68.
Trimble MA, Borges-Neto S, Smallheiser S, Chen J, Honeycutt EF, Shaw LK, et al. Evaluation of left ventricular mechanical dyssynchrony as determined by phase analysis of ECG-gated SPECT myocardial perfusion imaging in patients with left ventricular dysfunction and conduction disturbances. J Nucl Cardiol 2007;14:298‐307.
Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: Development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol 2005;12:687‐95.
Nguyen UC, Verzaal NJ, van Nieuwenhoven FA, Vernooy K, Prinzen FW. Pathobiology of cardiac dyssynchrony and resynchronization therapy. Europace 2018;20:1898‐909.
Aggarwal H, AlJaroudi WA, Mehta S, Mannon R, Heo J, Iskandrian AE, et al. The prognostic value of left ventricular mechanical dyssynchrony using gated myocardial perfusion imaging in patients with end-stage renal disease. J Nucl Cardiol 2014;21:739‐46.
Hess PL, Shaw LK, Fudim M, Iskandrian AE, Borges-Neto S. The prognostic value of mechanical left ventricular dyssynchrony defined by phase analysis from gated single-photon emission computed tomography myocardial perfusion imaging among patients with coronary heart disease. J Nucl Cardiol 2017;24:482‐90.
AlJaroudi W, Alraies MC, Hachamovitch R, Jaber WA, Brunken R, Cerqueira MD, et al. Association of left ventricular mechanical dyssynchrony with survival benefit from revascularization: A study of gated positron emission tomography in patients with ischemic LV dysfunction and narrow QRS. Eur J Nucl Med Mol Imaging 2012;39:1581‐91.
Goldberg AS, Alraies MC, Cerqueira MD, Jaber WA, Aljaroudi WA. Prognostic value of left ventricular mechanical dyssynchrony by phase analysis in patients with non-ischemic cardiomyopathy with ejection fraction 35-50% and QRS<150 ms. J Nucl Cardiol 2013;In Press.
Fudim M, Fathallah M, Shaw LK, Liu PR, James O, Samad Z, et al. The prognostic value of diastolic and systolic mechanical left ventricular dyssynchrony among patients with coronary heart disease. JACC Cardiovasc Imaging 2019;12:1215‐26.
Hage FG, Aggarwal H, Patel K, Chen J, Jacobson AF, Heo J, et al. The relationship of left ventricular mechanical dyssynchrony and cardiac sympathetic denervation to potential sudden cardiac death events in systolic heart failure. J Nucl Cardiol 2014;21:78‐85.
Zafrir N, Bental T, Strasberg B, Solodky A, Mats I, Gutstein A, et al. Yield of left ventricular dyssynchrony by gated SPECT MPI in patients with heart failure prior to implantable cardioverter-defibrillator or cardiac resynchronization therapy with a defibrillator: Characteristics and prediction of cardiac outcome. J Nucl Cardiol 2017;24:122‐9.
Modin D, Biering-Sorensen SR, Mogelvang R, Jensen JS, Biering-Sorensen T. Prognostic importance of left ventricular mechanical dyssynchrony in predicting cardiovascular death in the general population. Circ Cardiovasc Imaging 2018;11:e007528.
Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation 2004;110:227‐39.
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction. J Am Coll Cardiol 2018;72:2231‐64.
Henzlova MJ, Duvall WL, Einstein AJ, Travin MI, Verberne HJ. ASNC imaging guidelines for SPECT nuclear cardiology procedures: Stress, protocols, and tracers. J Nucl Cardiol 2016;23:606‐39.
Hage FG, Ghimire G, Lester D, McKay J, Bleich S, El-Hajj S, et al. The prognostic value of regadenoson myocardial perfusion imaging. J Nucl Cardiol 2015;22:1214‐21.
Ficaro EP, Lee BC, Kritzman JN, Corbett JR. Corridor4DM: The Michigan method for quantitative nuclear cardiology. J Nucl Cardiol 2007;14:455‐65.
Romero-Farina G, Aguade-Bruix S. Perspective and future direction of intraventricular mechanical dyssynchrony assessment. J Nucl Cardiol 2021;28:65‐71.
Aguade-Bruix S, Romero-Farina G, Candell-Riera J, Pizzi MN, Garcia-Dorado D. Mechanical dyssynchrony according to validated cut-off values using gated SPECT myocardial perfusion imaging. J Nucl Cardiol 2018;25:999‐1008.
Mall G, Rambausek M, Neumeister A, Kollmar S, Vetterlein F, Ritz E. Myocardial interstitial fibrosis in experimental uremia–implications for cardiac compliance. Kidney Int 1988;33:804‐11.
Aljaroudi W, Koneru J, Iqbal F, Aggarwal H, Heo J, Iskandrian AE. Left ventricular mechanical dyssynchrony by phase analysis of gated single photon emission computed tomography in end-stage renal disease. Am J Cardiol 2010;106:1042‐7.
Chen J, Kalogeropoulos AP, Verdes L, Butler J, Garcia EV. Left-ventricular systolic and diastolic dyssynchrony as assessed by multi-harmonic phase analysis of gated SPECT myocardial perfusion imaging in patients with end-stage renal disease and normal LVEF. J Nucl Cardiol 2011;18:299‐308.
Hart A, Lentine KL, Smith JM, Miller JM, Skeans MA, Prentice M, et al. OPTN/SRTR 2019 Annual Data Report: Kidney. Am J Transpl 2021;21:21‐137.
Crosland W, Aggarwal H, Farag A, Mehta S, Mannon RB, Heo J, et al. The effect of renal transplantation on left ventricular function, electrocardiography, and mechanical synchrony by gated myocardial perfusion imaging. J Nucl Cardiol 2019;26:1962‐70.
United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2020.
Jardine AG, Gaston RS, Fellstrom BC, Holdaas H. Prevention of cardiovascular disease in adult recipients of kidney transplants. Lancet 2011;378:1419‐27.
Rao NN, Coates PT. Cardiovascular disease after kidney transplant. Semin Nephrol 2018;38:291‐7.
Di Lullo L, Rivera R, Barbera V, Bellasi A, Cozzolino M, Russo D, et al. Sudden cardiac death and chronic kidney disease: From pathophysiology to treatment strategies. Int J Cardiol 2016;217:16‐27.
Chen J, Garcia EV, Bax JJ, Iskandrian AE, Borges-Neto S, Soman P. SPECT myocardial perfusion imaging for the assessment of left ventricular mechanical dyssynchrony. J Nucl Cardiol 2011;18:685‐94.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
All editorial decisions for this article, including selection of reviewers and the final decision, were made by guest editor Saurabh Malhotra, MD, MPH.
Rights and permissions
About this article

Cite this article
Morgan, W.S., Ives, C.W., Farag, A.A. et al. Effect of left ventricular mechanical dyssynchrony assessed pre-renal transplantation on cardiovascular death post transplantation. J. Nucl. Cardiol. 29, 2896–2905 (2022). https://doi.org/10.1007/s12350-021-02818-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-021-02818-0