
Abstract
An 84-year-old woman with pneumonia, congestive heart failure and chronic renal failure presented for iron-deficiency anemia and appetite loss. Esophagogastroduodenoscopy revealed a 60-mm sub-pedunculated tumor arising from the antrum of the stomach. The tumor was friable, with bleeding, and prolapsed into the duodenal bulb, the ball valve syndrome. The tumor was considered the cause of the anemia and appetite loss. Attempted endoscopic reduction of the prolapsing tumor was unsuccessful, but the base of its stalk could be identified through the transparent hood; thus, we removed the tumor with endoscopic submucosal dissection. The tumor was retrieved successfully, and pathohistological examination revealed the tumor to be a well-differentiated adenocarcinoma. This case suggests that endoscopic submucosal dissection is useful as an alternative to surgery for removal of gastric tumors that have prolapsed into the duodenal bulb when polypectomy was difficult, but provided the tumor’s attachment site can be identified endoscopically.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Polyps in the gastric antrum on rare occasions prolapse into the duodenal bulb and cause gastric outlet obstruction, the ball valve syndrome. Here we report a case of sub-pedunculated early gastric cancer with ball valve syndrome that was successfully and safely treated with endoscopic submucosal dissection (ESD).
Case report
An 84-year-old woman with pneumonia, chronic renal failure (serum creatinine, 1.26 mg/dl; glomerular filtration rate, 31.2 ml/min/1.73 m2), and congestive heart failure presented with iron-deficiency anemia and appetite loss. She was receiving oral anticoagulant therapy for atrial fibrillation and post-mitral valve replacement. Her hemoglobin level was 6.1 g/dl, and blood transfusions were required.
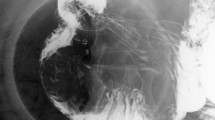
Abdominal computed tomography revealed a 60-mm tumor located in the pylorus and extending into the duodenum (Fig. 1). Esophagogastroduodenoscopy (EGD) revealed a large tumor arising from the antrum of the stomach. The tumor was friable, bleeding and prolapsed into the duodenum (Fig. 2). Ball valve syndrome caused by hyperplastic polyp or gastric cancer was suspected. The lesion was considered the cause of her anemia and appetite loss. Six days later, EGD showed that the tumor still prolapsed into duodenum. The tumor was large but villous and seemed soft; thus, we assumed that we could retrieve the tumor if we could catch the tumor head with grasping forceps, but could not grasp it because of its position in the duodenal bulb. Then, we tried to pull back the tumor by grasping its stalk in the antrum, but the attempt was also unsuccessful because the base of the stalk was too close to the pylorus ring. Although observation of entire shape of the prolapsed tumor was difficult, the base of its stalk could be identified through the transparent hood; thus, we planned to cut off the tumor from its stalk using the ESD technique, then, to move the resected tumor head to a good position to catch it, and to retrieve the tumor with grasping forceps. ESD was performed with Flash knife-BT (DK261JB; Fujifilm Medical Co. Ltd, Tokyo, Japan). Mucosal incision and submucosal dissection were performed from the oral side, and en bloc resection of the tumor was achieved without complication. After ESD, the entire tumor head had moved into the duodenal bulb. We moved the resected tumor to an appropriate position in the duodenal bulb, grasped it with a Pentapod grasping forceps (FG-46L-1, Olympus Medical Systems Co, Tokyo, Japan), and successfully retrieved it. Histopathologic examination revealed the tumor to be a well-differentiated adenocarcinoma, 60 × 30 mm (Fig. 3). The resection margin was tumor-negative without submucosal invasion or lymphovascular involvement. Her appetite loss and anemia improved after ESD. Her hemoglobin levels improved to 11.9 g/dl, and no recurrence of gastric cancer was evident after 7 months’ follow-up.

Abdominal computed tomography scan revealing a tumor of 60-mm diameter located in the pylorus and extending into the duodenal bulb (arrow)

Endoscopic photographs showing a large tumor arising from the antrum of the stomach and prolapsing into the duodenum. a A stalk of the tumor. b A part of tumor head in the duodenal bulb

Macroscopic and microscopic photos of the resected specimen. The tumor is 60 × 30 mm (a) and composed of well-differentiated adenocarcinoma (b) H&E staining; original magnification ×200
Discussion
To our knowledge, this is the first case of early gastric cancer with ball valve syndrome successfully treated with ESD. Large polypoid lesions in the gastric antrum occasionally cause gastric outlet obstruction, with symptoms such as abdominal pain, nausea and vomiting [1, 2], which is called the ball valve syndrome [3]. Hyperplastic polyps, polypoid adenomas or adenocarcinomas, submucosal lipomas or leiomyomas, and inflammatory fibroid polyps have been reported to be causes of ball valve syndrome [1, 4].The management strategy for gastric polyps with gastric outlet obstruction is complete resection either endoscopically or surgically. Endoscopic treatment, such as snare polypectomy or ESD, of polypoid gastric cancer is considered when gastric tumor prolapsing into the duodenal bulb can be reduced. On the other hand, surgical treatment will be selected if the attempted reduction was unsuccessful [4, 5]. In a published report, the median size of polyps removed endoscopically was 30 mm (range 15–80 mm), whereas the median size of those removed surgically was 60 mm (range 35–130 mm) [4]. In our case, we chose ESD excision over other endoscopic treatments or surgical resection for these reasons: the tumor was large (60 mm diameter) and could not be reduced from the duodenum by endoscopic maneuvers, which prevented snare polypectomy, but its attachment site could be cleanly identified through the transparent hood. A reported advantage of ESD for gastric lesions is that it enables en bloc resection regardless of tumor size, shape and location, even if the tumor cannot be entirely seen, provided the attachment site can be identified endoscopically [6]. The procedure also permits definitive histological evaluation of the polyp and extent of resection. In our case, the large size of the polyp suggested it had undergone malignant transformation, and histopathologic examination confirmed that it was a well-differentiated adenocarcinoma and had been entirely removed. We were concerned that the large polyp, having migrated into the distal duodenum, would not be retrieved and remain lodged causing intestinal obstruction. However, the tumor had stayed in the duodenal bulb probably due to its size, and we located it to the appropriate position to grasp and could retrieve the tumor by promptly catching it with the grasping forceps.
In conclusion, this case suggests that ESD is useful as an alternative to surgery for removal of gastric tumors that have prolapsed into the duodenal bulb when polypectomy was difficult, but provided the tumor’s attachment site can be identified endoscopically.
References
Macedo G, Lopes S, Albuquerque A. Ball valve syndrome: gastric polypectomy as a safe endoscopic treatment of a potentially troublesome condition. Gastrointest Endosc. 2012;76:1080–1.
Sun CK, Yang KC, Liao CS. Endoscopic management of gastric polyp with outlet obstruction without polypectomy. Case Rep Gastroenterol. 2011;5:267–71.
Hobbs WH, Cohen SE. Gastroduodenal invagination due to a submucous lipoma of the stomach. Am J Surg. 1946;71:505–18.
Parikh M, Kelley B, Rendon G, et al. Intermittent gastric outlet obstruction caused by a prolapsing antral gastric polyp. World J Gastrointest Oncol. 2010;2:242–6.
Yamauchi K, Iwamuro M, Ishii E, et al. Gastroduodenal intussusception with a gastric gastrointestinal stromal tumor treated by endoscopic submucosal dissection. Intern Med. 2017;56:1515–9.
Gotoda T, Ho KY, Soetikno R, et al. Gastric ESD: current status and future directions of devices and training. Gastrointest Endosc Clin N Am. 2014;24:213–33.
Acknowledgements
The authors thank Dr. William R. Brown (Denver, Colorado, United States) for assistance in preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest associated with this manuscript.
Human and animal rights
All procedures followed have been performed in accordance with the ethical standards Declaration of Helsinki in 1964 and its later amendments.
Informed Consent
Informed consent was obtained from a patient prior to treatment.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Miyake, M., Nishimura, N., Shimodate, Y. et al. Early gastric cancer with ball valve syndrome treated by endoscopic submucosal dissection. Clin J Gastroenterol 12, 307–309 (2019). https://doi.org/10.1007/s12328-019-00955-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12328-019-00955-1