
Abstract
Spinocerebellar ataxia type 10 (SCA10) is an autosomal dominant disorder in which patients have a slowly progressive cerebellar ataxia, with dysarthria, dysphagia, and epilepsy. The aims of this study were to characterize the phenotypic expression of SCA10 and to examine its genotype-phenotype relationships. Ninety-one Brazilian patients with SCA10 from 16 families were selected. Clinical and epidemiological data were assessed by a standardized protocol, and severity of disease was measured by the Scale for the Assessment and Rating of Ataxia (SARA). The mean age of onset of symptoms was 34.8 ± 9.4 years. Sixty-two (68.2%) patients presented exclusively with pure cerebellar ataxia. Only 6 (6.6%) of the patients presented with epilepsy. Patients with epilepsy had a mean age of onset of symptoms lower than that of patients without epilepsy (23.5 ± 15.5 years vs 35.4 ± 8.7 years, p = 0.021, respectively). All cases of intention tremor were in women from one family. This family also had the lowest mean age of onset of symptoms, and a higher percentage of SCA10 cases in women. There was a positive correlation between duration of disease and severity of ataxia (rho = 0.272, p = 0.016), as quantified by SARA. We did not find a statistically significant correlation between age of onset of symptoms and expansion size (r = − 0.163, p = 0.185). The most common clinical presentation of SCA10 was pure cerebellar ataxia. Our data suggest that patients with epilepsy may have a lower age of onset of symptoms than those who do not have epilepsy. These findings and the description of a family with intention tremor in women with earlier onset of symptoms draw further attention to the phenotypic variability of SCA10.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Spinocerebellar ataxias (SCAs) are a group of rare neurodegenerative disorders, genetically and clinically heterogeneous, characterized by progressive cerebellar dysfunction (mainly gait and limb ataxia) variably associated with extracerebellar signs such as ophthalmoplegia, parkinsonism, cognitive impairment, epilepsy, and peripheral neuropathy [1]. There are many different types of SCAs, and they are classified based on the gene mutation responsible for the particular SCA type. There are at least 48 genetic loci that have been associated with SCAs [2, 3]. The most common mutations described are secondary to repetition of nucleotide expansions [4, 5].
Spinocerebellar ataxia type 10 (SCA10) is characterized by slowly progressive cerebellar ataxia, dysarthria, dysphagia, epilepsy, and non-motor symptoms—such as dysautonomia, chronic pain, cognitive impairment, psychiatric disorders, and sleep disturbances [6,7,8]. SCA10 is caused by expansion of ATTCT pentanucleotide repeats in the ATXN10 gene and inherited in an autosomal dominant manner [9]. An additional feature of SCA10 is its phenotypic heterogeneity. For instance, particularly in regard to epilepsy, the prevalence of epilepsy in patients with SCA10 was found to be 3.5% in families from specific states in Brazil (Paraná and Santa Catarina) whereas this figure was found to be 64.7% in families from other Brazilian states [10, 11]. In Mexican families with SCA10, 72.2% of these individuals were estimated to have epilepsy [12]. Other phenotypic heterogeneities in SCA10 include age of onset of symptoms and expansion size [9, 13, 14].
In this context, the aims of this study were to expand the phenotypic spectrum of SCA10 and to investigate genotype-phenotype correlations in this population of patients.
Materials and Methods
Subjects
We reviewed charts of patients diagnosed with SCAs and followed at the Ataxia Clinic in our institution, from February 2012 to February 2017, and collected clinical and epidemiological data. We selected 91 patients with SCA10 (Table 1), from 16 families from Southern Brazil. This group consisted of patients diagnosed by genetic testing (ATTCT repeat expansion, size between 800 and 4500 repeats, in the ATXN10 gene) and their clinically compatible relatives. This study was approved by our institution’s ethics committee.
Clinical Evaluation
The patients included in the study were classified based on the severity of their ataxia according to the Scale for the Assessment and Rating of Ataxia (SARA), which has been validated for the Brazilian population. Scores range from 0 (no ataxia) to 40 (most severe ataxia) [15, 16]. The Mini Mental State Exam (MMSE) was the screening test used for cognition deficits assessment, using the cutoffs for dementia adapted for the Brazilian population [17]. Age of onset of symptoms was defined as the age at which an individual acquired, developed, or first experienced the symptoms of SCA10, such as gait ataxia. Brain imaging (computerized tomography, CT, or magnetic resonance imaging, MRI) was performed to evaluate for central nervous system abnormalities, especially in the cerebellar topography.
Statistical Analysis
Results are presented as means, medians, minimum and maximum values, and standard deviations (for quantitative variables) or as frequencies and percentages (for categorical variables). The normality of the variables was evaluated by the Shapiro-Wilk test. ANOVA with one factor, Student’s t test, or the non-parametric Kruskal-Wallis test and non-parametric Mann-Whitney U test were used to compare groups in terms of quantitative variables. Chi-square or the Fisher’s tests were used for the comparison of the groups in relation to categorical variables. The Pearson or Spearman correlation coefficient was estimated, depending on the normality of the variables, and utilized to evaluate possible associations between two quantitative variables. Values of p < 0.05 indicated statistical significance. Statistical analyses were conducted using Stata/IC, version 13.1 (StataCorp LP, Texas, USA, http://www.stata.com).
Results
Among the 91 patients with SCA10, 44 (48.4%) were men. The mean age of onset of symptoms was 34.8 ± 9.4 years (Table 2). The phenotypic presentations varied both among patients from the same family and in patients from different families (Table 1). Only six patients (6.6%) presented with epilepsy. These patients had a lower mean age of onset of symptoms and a shorter disease duration than patients without epilepsy (Table 2). Most patients (n = 62, 68.2%) presented exclusively with a combination of cerebellar findings; these included gait ataxia, limb ataxia, dysarthria, dysmetria, and nystagmus (pure cerebellar ataxia). The most common signs and symptoms were gait ataxia, dysarthria, and ophthalmologic findings (Table 3).
Among the 16 families studied, four of them had 10 or more affected members each. These four families were compared for clinical and epidemiological characteristics. There were statistical differences in relation to gender, age of onset of symptoms, and SARA score (Table 4). When clinical symptoms were analyzed, we observed that all cases of intention tremor were in Family 2. All cases of tremor occurred in women. This family also had the lowest mean age of onset of symptoms and a higher percentage of SCA10 cases in women (Table 4).
There was a positive correlation between disease duration and ataxia severity (rho = 0.272, p = 0.016), as quantified by SARA. We did not find a statistically significant correlation between age of onset of symptoms and expansion size (r = − 0.163, p = 0.185) and ataxia severity (rho = 0.18, p = 0.119). There was no statistically significant correlation between expansion size and ataxia severity (rho = − 0.232, p = 0.056) and disease duration (rho = − 0.0270, p = 0.828).
Discussion
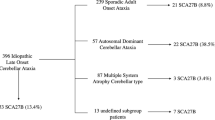
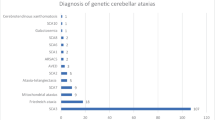
The phenotypic presentations of SCA10 have been a controversial topic over the years. This study showed that 68.2% of our population of SCA10 patients had pure cerebellar ataxia. Moreover, the combination of patients with pure ataxia and ophthalmoparesis has been found to comprise 79.1% of this population. SCA10 was first described in Mexican families, after which this particular SCA was associated with epilepsy [4,5,6,7, 12]. In 2004, Teive et al. [14] reported 28 SCA10 patients from Brazilian families with a new phenotype—pure cerebellar ataxia, without epilepsy—and also showed that SCA10 is the second most common autosomal dominant cerebellar ataxia in Southern Brazil, in the states of Paraná and Santa Catarina, second only to SCA3. In a subsequent study, Teive et al. [10] found that 3.75% of Brazilian SCA10 patients presented with epilepsy, a rate above the estimated prevalence of active epilepsy in the general population—0.54% in Brazil [18] and 1.2% in the USA [19]. The 3.75% figure was lower than the previously known prevalence of patients with SCA10 and epilepsy, which was published as 72.2% (ranging from 25 to 80%) in a select Mexican cohort of SCA10 patients [6, 9]. In other regions of Brazil, the prevalence of epilepsy in SCA10 patients (64.7%) was similar to findings in Mexican studies [11]. In this study, however, we found six (6.6%) patients with epilepsy. The previous study by Teive et al. [10] with 80 patients, which was conducted at the same medical center, identified an epilepsy prevalence in SCA10 of 3.75%. Despite the increase in total number of patients and six new families, the number of patients with epilepsy in Southern Brazil is still lower than in other centers in Brazil and worldwide.
In our study, the patients with SCA10 and epilepsy (6.6%) were noted to have had earlier onset of symptoms—approximately 12 years before than patients without epilepsy. Among the patients with both SCA10 and epilepsy, one of them had the most severe disease (SARA score = 34/40). In addition to epilepsy and cerebellar abnormalities, this patient also had ophthalmological findings and cognitive decline. Furthermore, she was the patient with the fewest ATTCT repeats (12/930) at SCA10. The phenotype of this patient was different from all others in our cohort; however, it was similar to that described in a patient in Venezuela by Gallardo and Sotto [20], with the difference that the testing on their patient showed an expansion of 4400 ATTCT repeats at the SCA10 locus. Other cases with SCA10 and epilepsy have been described in Argentina [21], Peru [22], China [23], and Japan [24]. Although the mechanism underlying the phenotypic variability remains unknown, genetic modifiers, such as locus-specific cis-elements and trans-factors, may influence the phenotypic expression [21]. McFarland et al. demonstrated in 2014 that repeat interruptions in SCA10 expansions are strongly associated with epileptic seizures [25].
All cases that had intention tremor belonged to Family 2. This family had a lower mean age of onset of symptoms and a higher percentage of female patients than the other three families with more than 10 cases studied. All cases with tremor were in women. This phenotype was similar to that described by Leonardi et al. [22] in a 47-year-old Peruvian woman with intention tremor, cerebellar symptoms, bilateral fixation nystagmus, and saccadic pursuit. Differently from our patient, she also had epilepsy. It is interesting to note that she had one affected brother with no tremor and two sons without SCA10. Intention tremor is not a common symptom reported among SCA10 patients in other series, although it is present in several degenerative diseases of the cerebellum and has its pathophysiology related to cerebellar and thalamic structures and pathways [26]. Despite the difference in the prevalence of epilepsy and intention tremor, the other manifestations seen in our patients were similar to the ones described in other studies [2, 11, 12, 20,21,22,23,24].
We did not find a significant correlation between age of onset of symptoms and ATTCT repeat size (r = − 0.163, p = 0.185). This result was similar to that found by Rasmussen et al. [12] in a sample involving 18 patients from four Mexican families (n = 14, r = − 0.02, p > 0.96). In 2004, with a smaller number of families, we found a significant correlation (n = 18, r2 = 0.532, p < 0.01) [11]. Matsuura et al. [9] studied five Mexican families and noted a weak inverse correlation between expansion size and age of onset (n = 26, r2 = 0.34, p = 0.018). Grewal et al. [13] studied two Mexican families and observed a strong inverse correlation between age of onset and repeat number in one of the families (n = 12, r2 = 0.79, p = 0.001). In the other family, however, no correlation was identified. It was noted that paternal transmission, but not maternal transmission, resulted in repeat instability in successive generations. In a subsequent study [27], it was found that the family in which the strong correlation was observed displayed uninterrupted ATTCT expansions, whereas the other family showed multiple interruptions of the ATTCT repeat by non-consensus repeat units, suggesting that differences in the sequence interruption patterns might explain their variable effect on phenotype and patterns of instability. Patients with interruptions in SCA10 repeat expansions have a 6.3-fold increased risk of developing epilepsy, when compared with patients that do not carry interruptions [25].
Our study had limitations. Firstly, the clinical examinations were performed by different physicians. Moreover, we did not assess each family individually, thereby possibly missing the opportunity of identifying anticipation among generations. Additionally, we did not account for instability patterns in disease transmission. We did not evaluate for the presence of interruptions within the ATTCT expansion, mainly due to technical difficulties and economic issues in our institution. Interruptions may be the basis for understanding the complex relationship between ATTCT repeats length and disease severity, and it is known that SCA10 expansions with interruptions significantly differ from SCA10 expansions without detectable interruption in repeat-size-instability dynamics and pathogenicity [25, 27]. Finally, it is important to emphasize that this cohort of SCA10 patients studied in Southern Brazil can represent a group of families originated from the same geographical area in the Santa Catarina state, previously known [28], and the correlation of genotype and phenotype could be influenced by a founder effect.
Conclusion
With a sample size of 91 patients from 16 families, this was one of the largest studies involving SCA10 patients to date. We observed that the frequency of epilepsy was relatively rare among Brazilian patients from Paraná and Santa Catarina states with SCA10, and the most common phenotype was pure cerebellar ataxia, unlike other areas of Brazil and worldwide. Our data suggest that patients with epilepsy may have a lower age of onset of symptoms of SCA10. These findings and the description of a family with intention tremor in women and earlier onset of symptoms draw further attention to the phenotypic variability of SCA10.
References
Harding A. Clinical features and classification of inherited ataxias. Adv Neurol. 1993;61:1–14.
Schöls L, Bauer P, Schmidt T, Schulte T, Riess O. Autosomal dominant cerebellar ataxias: clinical features, genetics, and pathogenesis. Lancet Neurol. 2004;3:291–304.
Bird T (2018). Hereditary ataxia overview [internet]. Ncbi.nlm.nih.gov. [cited 7 June 2018]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1138/
Teive HAG, Ashizawa T. Primary and secondary ataxias. Curr Opin Neurol. 2015;28:413–22.
Hersheson J, Haworth A, Houlden H. The inherited ataxias: genetic heterogeneity, mutation databases and future directions in research and clinical diagnostics. Hum Mutat. 2012;33:1324–32.
Ashizawa T. Spinocerebellar ataxia type 10. Handb Clin Neurol. 2012;103:507–19.
Teive HAG, Munhoz RP, Arruda WO, Raskin S, Werneck LC, Ashizawa T. Spinocerebellar ataxia type 10 – a review. Parkinsonism Relat Disord. 2011;17(9):655–61.
Moro A, Munhoz RP, Moscovich M, Arruda WO, Raskin S, Silveira-Moriyama L, et al. Nonmotor symptoms in patients with spinocerebellar ataxia type 10. Cerebellum. 2017;16(5–6):938–44.
Matsuura T, Yamagata T, Burgess DL, Rasmussen A, Grewal RP, Watase K, et al. Large expansion of the ATTCT pentanucleotide repeat in spinocerebellar ataxia type 10. Nat Genet. 2000;26:191–4.
Teive HAG, Munhoz RP, Raskin S, Arruda WO, de Paola L, Werneck LC, et al. Spinocerebellar ataxia type 10: frequency of epilepsy in a large sample of Brazilian patients. Mov Disord. 2010;25:2875–8.
de Castilhos RM, Furtado GV, Gheno TC, et al. Spinocerebellar ataxias in Brazil—frequencies and modulating effects of related genes. Cerebellum. 2014;13:17–28.
Rasmussen A, Matsuura T, Ruano L, Yescas P, Ochoa A, Ashizawa T, et al. Clinical and genetic analysis of four Mexican families with spinocerebellar ataxia type 10. Ann Neurol. 2001;50:234–9.
Grewal RP, Achari M, Matsuura T, Durazo A, Tayag E, Zu L, et al. Clinical features and ATTCT repeat expansion in spinocerebellar ataxia type 10. Arch Neurol. 2002;59:1285–90.
Teive HAG, Roa BB, Raskin S, Fang P, Arruda WO, Neto YC, et al. Clinical phenotype of Brazilian families with spinocerebellar ataxia 10. Neurology. 2004;63:1509–12.
Schmitz-Hübsch T, du Montcel ST, Baliko L, et al. Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology. 2006;66:1717–20.
Braga-Neto P, Godeiro-Junior C, Dutra LA, Pedroso JL, Barsottini OGP. Translation and validation into Brazilian version of the scale of the assessment and rating of ataxia (SARA). Arq Neuropsiquiatr. 2010;68:228–30.
Bertolucci P, Brucki S, Campacci S, Juliano Y. O Mini-Exame do Estado Mental em uma população geral: impacto da escolaridade. Arq Neuropsiquiatr. 1994;52(1):1–7.
Li LM, Fernandes PT, Noronha ALA, Marques LHN, Borges MA, Cendes F, et al. Demonstration project on epilepsy in Brazil: situation assessment. Arq Neuropsiquiatr. 2007;65:5–13.
Zack MM, Kobau R. National and state estimates of the numbers of adults and children with active epilepsy — United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66:821–5.
Gallardo M, Soto A. Clinical characterization of a Venezuelan family with spinocerebellar ataxia type 10. Mov Disord. 2009;24:S12.
Gatto EM, Gao R, White MC, Uribe Roca MC, Etcheverry JL, Persi G, et al. Ethnic origin and extrapyramidal signs in an Argentinean spinocerebellar ataxia type 10 family. Neurology. 2007;69(2):216–8.
Leonardi L, Marcotulli C, McFarland KN, Tessa A, DiFabio R, Santorelli FM, et al. Spinocerebellar ataxia type 10 in Peru: the missing link in the Amerindian origin of the disease. J Neurol. 2014;261:1691–4.
Wang K, McFarland KN, Liu J, et al. Spinocerebellar ataxia type 10 in Chinese Han. Neurol Genet. 2015;1:e26.
Naito H, Takahashi T, Kamada M, Morino H, Yoshino H, Hattori N, et al. First report of a Japanese family with spinocerebellar ataxia type 10: the second report from Asia after a report from China. PLoS One. 2017;12:e0177955.
McFarland KN, Liu J, Landrian I, et al. Repeat interruptions in spinocerebellar ataxia type 10 expansions are strongly associated with epileptic seizures. Neurogenetics. 2014;15:59–64.
Zakaria R, Lenz FA, Hua S, Avin BH, Liu CC, Mari Z. Thalamic physiology of intentional essential tremor is more like cerebellar tremor than postural essential tremor. Brain Res: Sep. 2013;5(1529):188–99.
McFarland KN, Liu J, Landrian I, et al. Paradoxical effects of repeat interruptions on spinocerebellar ataxia type 10 expansions and repeat instability. Eur J Hum Genet. 2013;21:1272–6.
Teive HA, Moro A, Moscovich M, Arruda WO, Munhoz RP, Raskin S, et al. Spinocerebellar ataxia type 10 in the south of Brazil: the Amerindian-Belgian connection. Arq Neuropsiquiatr: Aug. 2015;73(8):725–7.
Author information
Authors and Affiliations
Contributions
The authors alone are responsible for the content and writing of this paper.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Domingues, B.M.D., Nascimento, F.A., Meira, A.T. et al. Clinical and Genetic Evaluation of Spinocerebellar Ataxia Type 10 in 16 Brazilian Families. Cerebellum 18, 849–854 (2019). https://doi.org/10.1007/s12311-019-01064-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-019-01064-y