
Abstract
Endovascular therapy has been the first option for many vascular diseases. Due to the increasing development of endovascular devices and techniques in recent decades, endovascular procedures could be applied in treating those cases with complex anatomy. Two or three vascular access routes are required to establish through-and-through access in endovascular therapy for arterial occlusive disease and complex aortic aneurysm. Guidewire snaring with a snare kit is essential but sometimes time-consuming in the establishment of through-and-through access. To simplify the procedure, we design the magnetic kissing guidewire (MKG) with a magnetic tip that attracts each other to establish a guidewire route that meets the needs of clinical practice. We conducted the in vitro test to evaluate its magnetic force and the in vivo test to assess its performance in the arteries of twelve sheep. The results revealed that this novel guidewire significantly simplified the establishment of through-and-through access.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Endovascular techniques are increasingly used in challenging and complex anatomical situations [1, 2]. Multiple access routes, a variety of guidewires, or hybrid techniques are involved in these procedures [3]. Although intraluminal crossing is the best approach for endovascular revascularization in patients with chronic total occlusion (CTO) of the iliofemoral artery, subintimal crossing partially and guidewire crossing through two different arterial accesses are alternative ways in some cases with challenging anatomic characteristics [4]. Besides, establishing a guidewire route through the left brachial artery access and the femoral artery access for gate cannulation is required in some cases with severe tortuous abdominal aortic aneurysm (AAA) before placement of iliac limb in the procedure of endovascular repair of the aneurysm [5]. In the situations mentioned above, through-and-through access is created via loop snare over the guidewire and retrieval from the arterial sheaths, which sometimes can be time-consuming.
In recent years, magnetic materials have been used in many operations [6, 7]. Therefore, we envisaged the creation of the guidewire with a magnetic tip that can quickly and efficiently establish a guidewire route through two arterial accesses by the mutual attraction of the two guidewires. In this article, we introduced and tested the safety and feasibility of this guidewire.
Materials and Methods
Design of a Magnetic Guidewire
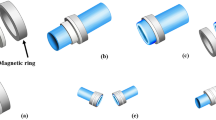
Since these guidewires quickly establish a safe working route through a mechanism of magnetic tip attraction to each other, we define this device as magnetic kiss guidewire (MKG). The structure of the guidewire mainly includes the main body of the guidewire, a magnetic tip, and the bonding material, as shown in Fig. 1. The main body is a superhard 0.038-in. guidewire that contains a core wire made of SUS304 stainless steel. The radiopaque part is made of platinum-nickel alloy and coated with polytetrafluoroethylene (PTFE). The magnetic tip is composed of a piece of cylindrical NdFeB N50 material with a diameter of 1.4 mm and a length of 4.2 mm, which is suitable for a 6-F or larger catheter. The polarity of the tip determines the pole of the guidewire. As a result, each guidewire kit consists of one wire with a North-pole (N-pole) tip and one with a South-pole (S-pole) tip. The magnetic tip is tightly connected to the head end of the guidewire body by Loctite M-31CL, a medical epoxy resin AB glue.

Structure of the magnetic kissing guidewire
In Vitro Study
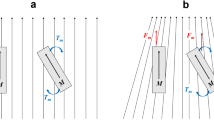
Professional testing institutions determined the specific physical, chemical, and biological properties of the guidewire, and the in vitro test we performed here was mainly to evaluate those parameters related to the effects of the device during the endovascular procedure. The kissing distance is a threshold that two different magnetic tips attract and finally connected without additional assistance. The separation force refers to the minimum strength that can successfully separate the connected guidewires. The kissing distance and the separation force were measured several times using a scale and digital dynamometer. The average kissing distance and separation force were obtained. Additionally, we tested whether the kissing force could tolerate the resistance generated by the hemostatic valve of the sheath. The whole in vitro test was manually performed on the smooth surface of the desk.
In Vivo Study
Animals and Anesthesia
The safety and feasibility tests of the MKG were performed in sheep models. We chose a group of adult sheep of similar varieties containing both genders. The sheep had an average age and weighed 50–60 kg. Twelve sheep were randomly divided into groups A and B, and then general anesthesia was performed. After anesthesia was induced with Rompun (2.2 mg/kg) and zoletil (6 mg/kg), oral endotracheal intubation was performed. The maintenance of anesthesia was continued using ketaminol (4 g/1000 ml) and fentanyl (0.5 mg/1000 ml) at a rate of 8 ml/kg/h [8]. Blood pressure and heart rate were monitored in real time during the operation. The left brachial artery and one side of the femoral artery were prepared in group A, and the bilateral femoral artery was prepared in group B. Systemic heparinization was administered and the activated clotting time was controlled between 250 and 300 s. At the termination of the procedure, during anesthesia, the animals were sacrificed by an intravenously injected potassium chloride. The animal arteries, including the distal abdominal aorta and bilateral common iliac artery, were obtained for pathological examination and to evaluate the injury extent of the arterial wall.
Test Procedure
Due to the incompatibility of the guidewire’s main body with the 6-F catheter used in the experiment, there was blood leakage, and we, therefore, assembled a kissing guidewire kit. The kit includes a 6-F guiding catheter, a Y-shaped hemostasis valve, a tee valve, and a piece of magnetic guidewire. This kit was used to assist in the kissing process of the magnetic tips and to reduce blood leakage around the guidewire.
The right femoral artery and left brachial artery were surgically exposed and were punctured retrogradely with modified Seldinger technique in group A. The bilateral femoral arteries were exposed and punctured in group B. 7-F short sheaths were placed subsequently to establish the vascular accesses. In group A, we advanced a 5-F pigtail catheter over guidewire from the femoral access to perform angiography to evaluate the anatomy of the abdominal aorta. The S-pole magnetic guidewire inserted through the brachial access was attempted to attract the N-pole guidewire inserted through the femoral access at the level of the renal artery. After the kissing of the tips was achieved, the connected guidewires were withdrawn into the anterograde or retrograde catheter, externalizing the guidewires from the sheaths to establish through-and-through access. In group B, a pigtail catheter was inserted from any side of the femoral access to perform angiography to evaluate the anatomy of the distal abdominal aorta and iliac arteries. The guidewire kits were then advanced from the two femoral accesses and were attempted to attract at the level of one side of the common iliac artery. Following successful kissing, the guidewires were drawn into one catheter and were pulled out to establish through-and-through access. The performance of the kissing guidewire and its compatibility with the 6-F guiding catheter were evaluated in the experiment and the operation time was recorded. At the end of the procedure, we performed angiography to determine whether there were complications, such as arterial rupture, dissection, and thrombosis.
Measurement of Kissing Distance and Force
During the procedure, we measured the kissing distance based on dynamic digital subtraction angiography images. Once the guidewires had kissed successfully, we connected a digital dynamometer to one side of the guidewire to obtain the separation force value. Additionally, we performed another procedure of withdrawing the kissed wires through the 7-F sheath to observe whether the attractive force could withstand the resistance of the 7-F sheath hemostasis valve.
Results
In Vitro Test of MKG
We successfully constructed the MKG, as shown in Fig. 2. After ten times of tests, the average kissing distance of the guidewire was determined to be 0.65 cm. When the distance between the two tips was less than 0.65 cm, they kissed each other automatically. The average force required to separate the connected guidewires was 0.7 Newton (N). The resistance generated by the hemostatic valve of the short sheath was 0.5 N, and the attractive force between the guidewires effectively withstood this resistance.

The physical photo of one N-pole and one S-pole guidewire
In Vivo Test of MKG
The guidewire kit allowed excellent operability and no blood leakage (Fig. 3). The guidewire traveled well in blood vessels, and the magnetic tip and the guidewire’s main body were firmly connected and encountered no separation. In group A, five sheep had normal abdominal aorta in which the guidewires kissed quickly (Fig. 4). Due to aortic tortuosity, several attempts were made in one sheep before the guidewires kissed and were successfully pulled out of the vascular access. The average operation time was 15 s (Table 1). The average kissing distance was 0.64 cm, and the average separation force of the guidewire was 0.7 N. No procedure-related arterial dissection, filling defect, or contrast agent extravasation were observed, and the abdominal aorta pathology was normal. In group B, the guidewires kissed and were pulled out smoothly in five sheep with normal iliac arteries (Fig. 5). In addition, the magnetic guidewires successfully kissed after several attempts in one sheep with a severely twisted iliac artery. The average operation time was 12 s (Table 1). The average kissing distance was 0.65 cm, and the average separation force of the guidewire heads was 0.7 N. There was no procedure-related complication in angiography or pathology. After the guiding catheter was removed, the kissed MKG effectively withstood the resistance of the vascular sheath hemostasis valve.

The guidewire kit including a 6-F guiding catheter, a Y-shaped hemostasis valve, a tee valve, and a piece of magnetic guidewire

a Angiography shows a normal abdominal aorta. b Entering the N-pole and the S-pole guidewire from brachial and femoral access respectively. c Two guidewires successfully kiss in abdominal aorta. d Kissed guidewires are withdrawn into one guiding catheter

a Angiography shows normal iliac arteries. b Entering the N-pole and S-pole guidewire from two femoral accesses respectively. c Two guidewires successfully kiss at the level of external iliac artery. d Kissed guidewires are withdrawn into catheter
Discussion
In the present study, we developed a novel magnetic guidewire by bonding a NdFeB permanent magnet to the head end of a superhard guidewire. The MKG exhibited reasonably good performance via in vitro and in vivo experiments.
The findings of in vitro tests showed that the MKG well adapted to a 6-F guiding catheter. If the distance between two magnetic tips is less than the kissing distance (that is 0.65 cm), they strongly attracted to each other without the assistance of additional force and firmly connected in the end. Moreover, the interconnected guidewire tips did not separate during extraction from the sheath. It provided evidence that the magnetic force between the two guidewire tips can withstand the resistance created by the hemostasis valve of the vascular sheath. In fact, we do not need to withdraw the guide wires through the short sheath in clinical practice but could directly withdraw them through the 6-F guiding catheter. In animal experiments, we found that the diameter of the 6-F catheter was larger than that of the guidewire body, which caused blood leakage from the catheter. Therefore, we connected the catheter to a Y-shaped hemostatic valve and a tee valve. The result of the in vivo test was similar to that of the in vitro test. The kissing process of the MKG was easily completed and through-and-through access was established quickly. Arterial angiography did not show procedure-related complications, such as dissection, perforation, and thrombosis. Besides, postoperative pathology did not show damage to the arterial wall.
Guidewires play an essential role in endovascular procedures and mediate intraluminal diagnosis and treatment. Passing the guidewire over the lesion is essential for the following therapeutic steps. However, it usually takes two or three vascular accesses to treat a lesion with complex anatomy [3]. It is sometimes difficult to thread a guidewire into the graft with the retrograde approach to perform gate cannulation in the procedure of endovascular repair of AAA for patients with a large and distorted aneurysm sac [9, 10]. The most common backup method involves accessing the gate from the contralateral side with the use of an “up-and-over” catheter or from the left brachial artery with an “up-and-down” approach. In each method, the guidewire is snared and retrieved from ipsilateral femoral access after the wire is passed down to the iliac artery [5]. No matter in the “up-and-over” or “up-and-down” approach, we simplified the establishment of the through-and-through access with the assistance of MKG.
Similarly, MKG is helpful for the quick establishment of through-and-through access in endovascular therapy for peripheral arterial disease (PAD). Subintimal crossing approach is commonly used but is not always feasible for revascularization in patients with CTO lesions [11, 12]. Regarding aortoiliac artery CTO lesions, the subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) technique combined with “double-balloon technique” are alternative options for revascularization failure of single femoral access [13, 14]. One retrograde approaching MKG attracted and firmly connected with one antegrade approaching MKG in the subintimal space. The through-and-through access was obtained by pulling out the kissed MKG from either femoral access. The MKG is theoretically suitable for the establishment of through-and-through access in the cases of infrainguinal occlusive disease. The use of the MKG will significantly reduce the operation time and radiation exposure. Furthermore, the MKG has potential application prospects in the subclavian or carotid fenestration during the thoracic endovascular aortic repair.
The use of magnetic materials is not uncommon in medical fields. Since the development of magnetic resonance imaging technology in the 1970s, magnetic materials have been used in the fields of orthodontics and surgery [6]. Magnetic instruments, such as vascular anastomats, intestinal staplers, cholangioenterosal stents, and pancreaticointestinal staplers, have been invented and examined in clinical trials and were found to reduce operative time and complication rates significantly [15,16,17]. Magnetic navigation platforms and magnetic capsule endoscopes developed based on magnetic anchoring and guidance systems have also been used in clinical practice [7, 18,19,20]. As the third-generation rare earth permanent magnetic material, NdFeB has the most powerful magnetic properties. NdFeB exerts only a tiny amount of cytotoxicity even when directly contacting human tissue, and this ensures its broad prospects for application in the field of magnetic surgery [21].
This study has some limitations. The procedure is performed in normal sheep rather than in sheep with AAA or PAD, a situation that is significantly different from clinical practice, and that may have led to bias in the results. The guidewire has some shortcomings as well. First, the diameter of the magnetic tip is too large to fit a 5-F catheter, which makes it not suitable in the endovascular therapy for infrainguinal occlusive disease. We will further refine the magnetic tip to fit thinner catheters. Second, it is challenging for the MKGs to kiss each other in extremely large or distorted aneurysms because of the stiff property of the wire. Therefore, we will further soften the guidewire so that the tips swing in the arterial blood flow which increases the chance of kissing.
Conclusion
In summary, this safe and effective guidewire meets clinical needs. The MKG displayed good performance in the experiment. This novel guidewire significantly simplifies the establishment of through-and-through access in endovascular procedures for iliac artery lesions or abdominal aortic aneurysms.
Abbreviations
- AAA:
-
Abdominal aortic aneurysm
- CTO:
-
Chronic total occlusion
- F (size):
-
French
- MKG:
-
Kissing guidewire
- N-pole:
-
North-pole
- N (unit):
-
Newton
- PTFE:
-
Polytetrafluoroethylene
- PAD:
-
Peripheral arterial disease
- SAFARI:
-
Antegrade-retrograde intervention
- S-pole :
-
South-pole
References
Altit, R., & Gray, W. A. (2017). New innovations in drug-eluting stents for peripheral arterial disease. Current Cardiology Reports, 19(11), 117. https://doi.org/10.1007/s11886-017-0926-y.
Huff, C. M., Silver, M. J., & Ansel, G. M. (2018). Percutaneous endovascular aortic aneurysm repair for abdominal aortic aneurysm. Current Cardiology Reports, 20(9), 79. https://doi.org/10.1007/s11886-018-1023-6.
Etkin, Y., Baig, A., Foley, P. J., Wang, G. J., Woo, E. Y., Carpenter, J. P., et al. (2017). Management of difficult access during endovascular aneurysm repair. Annals of Vascular Surgery, 44, 77–82. https://doi.org/10.1016/j.avsg.2017.03.190.
Diamantopoulos, A., Santonocito, S., Thulasidasan, N., Gkoutzios, P., Ahmed, I., Zayed, H., et al. (2018). Initial experience with the outback catheter for targeted reentry during subintimal angioplasty of the infragenicular arteries. Journal of Endovascular Therapy, 25(2), 178–182. https://doi.org/10.1177/1526602818757409.
Titus, J. M., Cragg, A., Alden, P., Alexander, J., Manunga, J., Stephenson, E., et al. (2017). A prospective randomized comparison of contralateral snare versus retrograde gate cannulation in endovascular aneurysm repair. Journal of Vascular Surgery, 66(2), 387–391. https://doi.org/10.1016/j.jvs.2017.01.038.
Blechman, A. M., & Smiley, H. (1978). Magnetic force in orthodontics. American Journal of Orthodontics, 74(4), 435–443. https://doi.org/10.1016/0002-9416(78)90066-0.
Leong, F., Garbin, N., Natali, C. D., Mohammadi, A., Thiruchelvam, D., Oetomo, D., et al. (2016). Magnetic surgical instruments for robotic abdominal surgery. IEEE Reviews in Biomedical Engineering, 9, 66–78. https://doi.org/10.1109/rbme.2016.2521818.
Bosaeus, L., Mani, K., Wanhainen, A., & Liungman, K. (2016). Novel device, a temporary guidewire fixator. Vascular, 24(6), 604–609. https://doi.org/10.1177/1708538116629265.
Landry, G. J., Lau, I. H., Liem, T. K., Mitchell, E. L., & Moneta, G. L. (2010). Adjunctive renal artery revascularization during juxtarenal and suprarenal abdominal aortic aneurysm repairs. American Journal of Surgery, 199(5), 641–645. https://doi.org/10.1016/j.amjsurg.2010.01.010.
Behrendt, C. A., Rieß, H. C., Schwaneberg, T., Heidemann, F., Tsilimparis, N., Larena-Avellaneda, A. A., et al. (2018). Complex endovascular treatment of intact aortic aneurysms: an analysis of health insurance claims data. Gefasschirurgie : Zeitschrift fur vaskulare und endovaskulare Chirurgie : Organ der Deutschen und der Osterreichischen Gesellschaft fur Gefasschirurgie unter Mitarbeit der Schweizerischen Gesellschaft fur Gefasschirurgie, 23, 32–38. https://doi.org/10.1007/s00772-018-0387-7.
Kim, K., Ko, Y. G., Ahn, C. M., Min, P. K., Lee, J. H., Yoon, C. H., et al. (2018). Clinical outcomes of subintimal vs. intraluminal revascularization approaches for long femoropopliteal occlusions in a Korean multicenter retrospective registry cohort. Circulation journal : official journal of the Japanese Circulation Society, 82(7), 1900–1907. https://doi.org/10.1253/circj.CJ-17-1464.
Akamatsu, D., Fujishima, F., Goto, H., Hashimoto, M., Tsuchida, K., Kawamura, K., et al. (2017). Histological analysis of a new route after subintimal crural angioplasty. Annals of Vascular Surgery, 45, 262.e215–262.e219. https://doi.org/10.1016/j.avsg.2017.06.038.
Spinosa, D. J., Leung, D. A., Harthun, N. L., Cage, D. L., Fritz, A. J., Hagspiel, K. D., et al. (2003). Simultaneous antegrade and retrograde access for subintimal recanalization of peripheral arterial occlusion. Journal of Vascular and Interventional Radiology, 14(11), 1449–1454. https://doi.org/10.1097/01.rvi.0000096764.74047.21.
Ikushima, I., Hirai, T., Ishii, A., Iryo, Y., & Yamashita, Y. (2011). Confluent two-balloon technique: an alternative method for subintimal recanalization of peripheral arterial occlusion. Journal of Vascular and Interventional Radiology, 22(8), 1139–1143. https://doi.org/10.1016/j.jvir.2011.04.001.
Umemura, A., Sasaki, A., Nitta, H., Takahara, T., Hasegawa, Y., & Wakabayashi, G. (2014). Magnetic compression anastomosis for the stricture of the choledochocholedochostomy after ABO-incompatible living donor liver transplantation. Clinical Journal of Gastroenterology, 7(4), 361–364. https://doi.org/10.1007/s12328-014-0507-1.
Uygun, I., Okur, M. H., Cimen, H., Keles, A., Yalcin, O., Ozturk, H., et al. (2012). Magnetic compression ostomy as new cystostomy technique in the rat: magnacystostomy. Urology, 79(3), 738–742. https://doi.org/10.1016/j.urology.2011.11.048.
Rivas, H., Robles, I., Riquelme, F., Vivanco, M., Jiménez, J., Marinkovic, B., et al. (2018). Magnetic surgery: results from first prospective clinical trial in 50 patients. Annals of Surgery, 267(1), 88–93. https://doi.org/10.1097/sla.0000000000002045.
Mitselos, I. V., Christodoulou, D. K., Katsanos, K. H., & Tsianos, E. V. (2015). Role of wireless capsule endoscopy in the follow-up of inflammatory bowel disease. World journal of gastrointestinal endoscopy, 7(6), 643–651. https://doi.org/10.4253/wjge.v7.i6.643.
Keller, J., Fibbe, C., Volke, F., Gerber, J., Mosse, A. C., Reimann-Zawadzki, M., et al. (2010). Remote magnetic control of a wireless capsule endoscope in the esophagus is safe and feasible: results of a randomized, clinical trial in healthy volunteers. Gastrointestinal Endoscopy, 72(5), 941–946. https://doi.org/10.1016/j.gie.2010.06.053.
Best, S. L., & Cadeddu, J. A. (2010). Use of magnetic anchoring and guidance systems to facilitate single trocar laparoscopy. Current Urology Reports, 11(1), 29–32. https://doi.org/10.1007/s11934-009-0087-7.
Sarriegui, G., Martin, J. M., Ipatov, M., Zhukov, A., & González, J. (2018). Magnetic properties of NdFeB alloys obtained by gas atomization technique. IEEE Transactions on Magnetics, 1–5. https://doi.org/10.1109/TMAG.2018.2839906.
Acknowledgments
We want to thank Yongchun Cui and Boqing Yang in National Experimental Center for cardiovascular diseases (China) for their help with setting up the experimental systems.
Funding
Manufacture of the magnetic guidewire was supported by BIOVAS Medical Technology Co., Ltd.
Animal experiment was funded by funding from National Natural Science Foundation of China (81570431).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
Human: No human studies were carried out by the authors for this article. Animal: All institutional and national guidelines for the care and use of laboratory animals were followed and approved by the committee of animal research ethics, Fuwai Hospital, Chinese Academy of Medical Science (No. 0096-2-18-GZ(X)).
Additional information
Associate Editor Craig Stolen oversaw the review of this article
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, X., Zhang, H., Zhang, M. et al. Development of a Magnetic Kissing Guidewire and Animal Experiment: a Preliminary Study. J. of Cardiovasc. Trans. Res. 14, 589–594 (2021). https://doi.org/10.1007/s12265-020-09980-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12265-020-09980-9