
Abstract
Bleeding in the adrenal glands can be bilateral or unilateral. While it is most common in infants, it can also be observed in young adults and adults and is seven times more common in adolescents than in adults. Idiopathic unilateral hemorrhage is a very rare condition that occurs due to an idiopathic spontaneous rupture or an undetected adrenal mass. The main signs of adrenal bleeding are hemorrhagic shock, flank pain, and fever. Adrenal bleeding is rarely reported, and the ideal treatment is not clear. We present a patient with unilateral idiopathic adrenal bleeding who presented to the hospital with left flank pain and hemorrhagic shock.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bleeding in the adrenal glands can be bilateral or unilateral. While it is most common in infants, it can also be observed in young adults and adults and is seven times more common in adolescents than in adults. Bilateral hemorrhage is generally associated with anticoagulant use, stress due to surgery, sepsis, or hypotension [1] and less often with trauma and pregnancy. Idiopathic unilateral hemorrhage is a very rare condition that occurs due to an idiopathic spontaneous rupture or an undetected adrenal mass [2]. While many authors agree that it can be caused by blunt abdominal trauma, it has also been reported in liver transplant recipients or those with primary or metastatic adrenal tumors. Unilateral adrenal bleeding can rarely be observed in pregnancy, type 1 neurofibromatosis, and long-term users of nonsteroidal anti-inflammatory drugs [3]. The main signs of adrenal bleeding are hemorrhagic shock, flank pain, and fever. Adrenal bleeding is rarely reported, and the ideal treatment is not clear. We present a patient with unilateral idiopathic adrenal bleeding who presented to the hospital with left flank pain and hemorrhagic shock.
Case
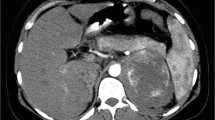
A 38-year-old female was taken to the hospital with increasing abdominal pain lasting more than 15 h, nausea, abdominal distention, and somnolence. On physical examination, she was somnolent and pale, with cold, sweaty skin, and had a blood pressure of 80/50 mm/Hg and a pulse of 116/min. Her abdomen was distended, and she had guarding and rebound. After the patient responded to initial resuscitation, her laboratory results showed hemoglobin (Hb) of 9.1 g/dL, platelets of 101,000, and white blood cells (WBC) of 15,000. Other routine laboratory parameters and bleeding and coagulation factors were normal. Abdominal tomography showed a 70 × 80 × 11-cm lesion with the density of blood in the perirenal area continuing to the iliac crest (Figs. 1 and 2).

Hematoma in the left adrenal area

Hematoma in the left adrenal area
She had no history of trauma or pregnancy. At an emergency laparotomy, there was approximately 500 mL of hemorrhagic liquid in the abdomen and a 10 × 10 cm hematoma in the left retroperitoneal area. The kidney was normal. A left adrenalectomy was performed. Histological examination showed massive non-specific bleeding in the adrenal tissue.
Discussion
Adrenal bleeding can be traumatic or non-traumatic, and is rare, but life-threatening. The adrenal gland is an important organ for regulating electrolytes, hemostasis, the stress response, and blood pressure. The clinical indications of spontaneous adrenal hemorrhage are not well known, so it is often missed. In autopsy studies, the rate of adrenal hemorrhage is 0.3–1.8%. Moreover, in 15% of the deaths due to shock, bilateral extensive adrenal hemorrhage was seen. Unilateral adrenal hemorrhage due to penetrating trauma is observed at a rate of 2% [4]. In 2% of liver transplantation patients, right adrenal hemorrhage is seen. Hemorrhage due to infarction of a primary or metastatic tumor can cause unilateral bleeding [5]. There have been a few cases resulting from long-term non-steroidal drug use, pregnancy, and neurofibromatosis. An idiopathic unilateral adrenal hemorrhage like the one in our patient is rare and can be observed as acute retroperitoneal bleeding or an adrenal mass.
Vella classified adrenal hematomas into seven categories: incidentaloma, spontaneous hemorrhage, related to anticoagulant treatment, occurring after surgery, related to heparin, related to sepsis, and related to trauma. There are many reasons for the pathogenesis of adrenal bleeding, including necrosis and hemorrhage caused by stress and hypotension due to ischemia or lack of venous drainage of the gland and adrenal stimulation because of stasis that occur in the gland [6]. Clinically, the presentation ranges from abdominal discomfort, nausea, and vomiting to hemorrhagic shock and coma. Hemorrhagic shock, flank pain, and fever can be observed. Since the adrenal gland is a retroperitoneal organ, defense and rebound, which indicate an acute abdomen, are observed only in 15–20% of the cases. In 50% of patients with adrenal bleeding, the biochemical findings are normal. Adrenal bleeding is generally observed in the medulla of the gland [7]. Since the gland is highly vascular, it is prone to bleeding. The differential diagnosis includes abdominal aortic aneurism rupture, renal cell carcinoma, angiomyolipoma, or renal artery aneurism.
Radiologically, ultrasonography (USG), computed tomography (CT), and magnetic resonance imaging (MRI) can be performed. CT is easier to perform on critically ill patients. MRI can be more useful for diagnosing non-traumatic spontaneous bleeding [8] . In bleeding that does not respond to blood transfusion, endovascular embolization of the bleeding adrenal arteries can be lifesaving. In unstable patients, immediate surgical treatment might become inevitable.
Conclusion
Idiopathic spontaneous adrenal hemorrhage is a rare condition that is difficult to diagnose unless the patient has a history of anticoagulant usage or trauma. Therefore, in patients with vague abdominal pain, tachycardia, and shock, it should be considered.
References
Xarli VP, Steele AA, Davis PJ, Buescher ES, Rios CN, Garcia-Bunuel R (1978) Adrenal hemorrhage in the adult. Medicine 57(3):211–221
Kobayashi T, Uenoyama S, Miura K, Takehara Y (2004) Idiopathic unilateral adrenal hematoma: report of a case. Surg Today 34(3):279–282
Carter JS, Kothari R, Jonson AL (2011) Idiopathic adrenal hemorrhage in a patient with gestational trophoblastic neoplasia. J Gynecol Surg 27(1):53–55
Gavrilova-Jordan LP et al (2005) Spontaneous adrenal hemorrhage during pregnancy: a review of the literature and a case report of successful conservative management. Obstetrical & gynecological survey 60(3):191–195
Hiroi N, Yanagisawa R, Yoshida-Hiroi M, Endo T, Kawase T, Tsuchida Y, Toyama K, Shibuya K, Nakata K, Yoshino G (2006) Retroperitoneal hemorrhage due to bilateral adrenal metastases from lung adenocarcinoma. J Endocrinol Investig 29(6):551–554
Siu, S., D. Kitzman, and P. Sheedy, II, Northcutt RC. Adrenal insufficiency from bilateral adrenal hemorrhage. Mayo Clin Proc, 1990. 65: p. 664–670
Catalano O (1996) Retroperitoneal hemorrhage due to a ruptured adrenal myelolipoma: a case report. Acta Radiol 37(5):688–690
Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P (1995) Spontaneous unilateral adrenal hemorrhage: computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol 154(5):1647–1651
Funding
This work has not received any funds.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
This work has been approved by the directorate of the institution.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Catal, O., Ozer, B. & Sit, M. Rare Unilateral Spontaneous Adrenal Hemorrhage. Indian J Surg 82, 1244–1246 (2020). https://doi.org/10.1007/s12262-020-02152-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-020-02152-8