
Abstract
Children with disabilities experience significantly poorer socio-emotional outcomes than their peers without disabilities. However, research evidence is scarce about children with both disability and migration background, the group which this study aimed to investigate using data from a national longitudinal study. Secondary data analyses were conducted on a sample of 7290 children (weighted with missing values imputed). Significant differences in socio-emotional outcomes were found in relation to impairment status but not in relation to migration. Having an impairment and activity limitation significantly increased the likelihood of experiencing poorer socio-emotional outcomes over time. Our findings highlight a higher risk of socio-emotional problems among children with disabilities, especially among children from lower income backgrounds and with parents with lower educational attainment. These findings clearly require policy development on two fronts: to raise professional and community awareness on these issues and to strengthen the capacity of health, education and social care systems to support schools, families, and communities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The importance of socio-emotional growth in children’s overall development has been well documented in research, situating socio-emotional competence as a key educational outcome (Ashdown and Bernard 2011; Becker and Luthar 2002; Humphrey 2013; Rose-Krasnor and Denham 2009), a significant predictor of adult life satisfaction and life course success (Layard et al., 2014), of health and health behaviours (Attanasio et al., 2020; Immordino-Yang et al., 2019) and of future outcomes, including adult education and labour market progress (Miyamoto et al., 2015; OECD, 2015), all of which are relevant well-being dimensions (OECD, 2015). The OECD emphasises the role that social and emotional skills, also known as “soft skills” and “non-cognitive skills”, play in goal achievement, collaborative work and emotional management (Miyamoto et al., 2015; OECD, 2015) and defines them as “individual capacities that can be (a) manifested in consistent patterns of thoughts, feelings and behaviours, (b) developed through formal and informal learning experiences, and (c) influence important socioeconomic outcomes throughout the individual’s life” (OECD, 2015, p. 35).
Research has demonstrated, however, that children with disabilities experience poorer socio-emotional outcomes than their peers without disabilities (Davis and Watson 2001; Emerson et al., 2019; Lindsay 2007). The research literature points at a number of factors underpinning such differences for children with disabilities. Various types of impairment and gender along with socio-economic factors such as family economic vulnerability and migration have been reported to influence socio-emotional outcomes, which are explored next.
Learning disability has been found to directly influence socio-emotional development (Bryan et al., 2004; Haft et al., 2019). McCoy et al. (2016b) and Smyth (2016) found that children with disabilities tend to have a more negative perception of themselves and this was more likely to be the case for children with intellectual disabilities and children with emotional behavioural difficulties compared to children with other disabilities. In Smyth’s study, children with disabilities appeared as more poorly behaved, more anxious, less happy, less confident as learners, more critical of their physical appearance and less popular than their peers without disabilities. These differences were even more pronounced at age 13 than at age 9 (Smyth, 2016). Cosgrove et al.'s (2014) findings resonate with the above studies and indicate that children with disabilities have lower well-being scores compared to children without disabilities and that children with emotional behavioural difficulties are those with the lowest scores. Similarly, language disorders have been associated with poorer socio-emotional outcomes (Bakopoulou and Dockrell 2016; Van Agt et al., 2011). For example, a large scale study conducted in the Netherlands reported that language disorders of 8 year old children were associated negatively with children’s attitude to school work, behaviours towards others, aggressive and withdrawn behaviour and a lower quality of life (Van Agt et al. 2011).
The role of contextual factors such as socio-economic status and migration on children’s socio-emotional outcomes has also been explored. Families’ lower economic status has been reported to impact negatively on the socio-emotional development of children with disabilities (Parish and Cloud 2006; Park et al., 2002; Van der Mark et al., 2017; Watson et al., 2015). McCoy et al. (2016a) scrutinised data from the Growing Up in Ireland study and found that the prevalence of special needs education (SEN) was significantly higher among children in families of semi-skilled or unskilled workers compared to skilled or professional workers, and a high prevalence rate was also found for children of families in inactive households experiencing unemployment. Interestingly, the latter group presented significantly higher levels of emotional-behavioural difficulties. High disability (or SEN) rates were consistently found in the lowest income groups.
The impact of migration on children and adolescents’ socio-emotional problems has also been reported in the literature. A study by Tomlinson (2015) has established the link between disability, migration and poorer socio-emotional outcomes in the UK. A systematic literature review conducted by Belhadj Kouider et al. (2014) found that there is an increased risk of immigrant children having internalised problem behaviour such as depression or anxiety. However, these authors indicate that migration was not the strongest risk factor for mental health problems. Other factors such as family functioning and parenting, lower socio-economic status, education level, language competency, cultural identity, and gender, among others, also influence the prevalence of mental health problems.
From a European perspective, exploring socio-emotional outcomes associated with migration is particularly timely as the number of immigrant children has increased in Europe over the past decade (Belhadj Kouider et al. 2014). The 2016 Census of Population in Ireland showed that migration of non-Irish nationals from outside the EU had increased to a 40.1% share of total immigrants (CSO, 2016). A study on the mental health of young migrants in Ireland found that there were no differences in mental health outcomes between migrant and Irish children, although a greater proportion of 9 year old children of migrant background presented abnormal hyperactivity levels (Cotter et al., 2019). Migrant children, another study found, are disadvantaged by national groups when compared to children not from a migrant background, mostly for those with lower income, resources and access to schools, and school context rather than by a migration background (Darmody et al., 2016). According to McCoy et al. (2016a), attending the most disadvantaged school contexts is strongly related with the identification of emotional-behavioural difficulties.
In sum, the presence of impairment and gender coupled with external factors such as economic vulnerability influences children’s socio-emotional outcomes, according to the literature reviewed. Previous studies have explored migration background and have identified that other associated family and socio-economic factors seem to have larger impact on socio-emotional outcomes than migration itself. However, on close examination of the research conducted in Ireland, all the studies reviewed have approached disability and migration separately and there is a dearth of research, firstly, examining the impact of the intersection between disability and migration, or other socio-economic factors, on children’s socio-emotional outcomes and, secondly, existing research is limited in the examination of impact over time, with a dearth of studies drawing on national representative samples.
This study aimed to explore (1) whether children who have both a disability and a migrant background experience additional socio-emotional challenges compared to their peers; and (2) what other factors (such as family background or gender) influence children's socio-emotional outcomes over time.
2 Methodology
2.1 Population in the Republic of Ireland
The population in the Republic of Ireland (Ireland) according to the census conducted in 2016 was 4,761,865 people. There were 535,475 non-Irish nationals living in the country (of which 103,113 were UK nationals), which meant a 1.6% decrease in relation to the previous census conducted in 2011. About 13.5% (643,131 people) of the Irish population indicated they had a disability. There were about 6.7% of children and young people under 20 years of age with disability, representing a 0.7% increase on the results for the 2011 census according to the Central Statistics Office (CSO) (2016). The 2006 Census identified 32,085 children usually resident in the State but who were born outside of Ireland, and who were between the ages of 5 and 9 years while this figure dropped to 20,926 in 2011 (CSO 2011).
2.2 Growing up in Ireland Study
The current paper draws on secondary data from the child cohort of Growing Up in Ireland – the National Longitudinal Study of Children in Ireland (GUI). Children in the child cohort (recruited at 9 years old, as distinct from the infant cohort who were recruited at 9 months old) were selected from a nationally representative, stratified sample of primary schools (including so-called ‘special schools’). This study used data regarding children’s social, economic and cultural development, collected at both age 9 and 13 years.
Although the GUI study was not specifically designed from the outset to facilitate analysis for any particular subgroup, such as children with a disability (Cosgrove et al. 2014), the initial target sample size of 8500 was believed by the GUI researchers to offer the potential for disaggregated analysis (Greene et al., 2010), a characteristic generally identified as a feature of large, population-based datasets (Bryman 2016). This potential has been explored in this paper, for two subgroups of interest, namely children of migrant background, and children with disabilities. This paper considers outcomes for GUI study children between waves one and two of the study. Of the 8568 children in the GUI child cohort, prevalence estimates for disability vary, in line with the variety of definitions in use; however a study with the specific aim of estimating disability prevalence suggested a rate of 25% at age 9 years (Banks and McCoy 2011; Cosgrove et al. 2014).
2.3 Participants
In total, 8568 children participated in the GUI child cohort study at Wave 1. This represented a school-level participation rate of 82%, and a somewhat low within-school response rate of 50% (Thornton et al., 2010). No additions were made to this sample between GUI waves, and the number of participants reduced to 7525 for Wave 2 (Thornton et al., 2016). Overall, the GUI researchers noted ‘strong social gradients in participation at Wave 2’, with socially disadvantaged families less likely to respond at the second wave (Thornton et al. 2016). The GUI researchers suggest that, of the 1043 children who no longer participated at Wave 2, at least 170 (16.3%) had moved out of the country (Thornton et al. 2016). A further 14.0% of children (n = 146) could not be contacted. The potential for bias to be introduced into the analysis from any asymmetric drop-out from the sample, particularly with regard to the migrant and impairment sub-samples of interest for this paper as explored later, should be borne in mind.
2.4 Procedure
Data collection for Wave 1 took place in both the school (with principals and class teachers), and home (with primary and secondary caregivers). Where English was not the participant’s first language, questionnaires were available in additional languages or alternatively a translator was provided on request (Thornton et al. 2016).
2.5 Measures
2.5.1 Socio-Emotional Outcomes
Socio-emotional outcomes for this study were measured using the Strengths and Difficulties Questionnaire (SDQ) (Goodman 1997), which has been used in a number of longitudinal studies (see for example, Dunn et al., 2018; Dearden et al., 2011; Emerson et al., 2019; Flouri et al., 2015; Hartas 2016; Parkes and Sweeting 2018). The SDQ is a brief, user-friendly, behavioural screening questionnaire for children between 3 and 16 years (Goodman 1997; Stone et al., 2010; Murray et al., 2010). The 25 item-questionnaire consists of five scales including emotional symptoms, conduct problems, hyperactivity/inattention, peer-relationship problems, and prosocial behaviour. This instrument has been used to measure psychopathology and mental health problems (Cotter et al., 2019; Goodman 1997; Elberling et al., 2010) although it is not considered a diagnostic tool. The SDQ has also been interpreted as a measure of positive child development (Attanasio et al., 2020). A total difficulties score ranging from 0 to 40 can be obtained by adding all the resulting scores from all scales except the prosocial behaviour scale (Murray et al., 2010).
The scale generating the total SDQ score has been found to have acceptable to high levels of reliability (Goodman 2001; Stone et al., 2010). However, limitations have been reported on the reliability of the parent version at the sub-scale level (Stone et al., 2010), and in relation to its clinical utility (Vaz et al., 2016) and gender bias (Bøe et al., 2016). Concurrent validity for the SDQ has been demonstrated with general populations (Goodman 1997; Goodman and Scott 1999) and also with specific populations such as multi-ethnic groupings (Mieloo et al., 2014) and young people with an intellectual disability (Rice et al., 2017). The tool has been shown to discriminate between clinical and normal settings (Goodman and Scott 1999), and also to be sensitive to changes in behaviour following intervention (Mathai et al., 2003).
For the purpose of this analysis, despite the availability of both primary caregiver and teacher responses to the SDQ questionnaire at Wave 1, only primary caregiver responses have been used, since they were the only respondents for whom data at both waves 1 and 2 was available. Given the superior reliability and validity levels of the SDQ total score versus the relevant sub-scales shown in the literature, only the total score has been used. Furthermore, a measure of change in SDQ score over time was created for each child, whereby a threshold of 17 and above was used to distinguish a group of children with ‘abnormal’ total scores from their peers, as recommended by Goodman (1997). This threshold, which Goodman recommends for low-risk samples where it is important to reduce the rate of false positives, was identified by Goodman to capture ‘roughly’ 10% of children within the community. When employed in our study this threshold identifies a rather more conservative 6–7% of children at both waves. We used the threshold to identify three groups of children: those with above-threshold scores at both time points; with below-threshold scores at both time points; and those who had an above-threshold score at either Wave 1 or Wave 2. This approach ensures that, while some information may be lost, the analysis focuses on children with consistently ‘abnormal’ scores (above 17) between waves, and therefore with more serious difficulties. For the sample of responses from primary caregivers participating in both waves of the GUI study, this analysis calculated reliability for the children’s total SDQ scores to be a relatively high 0.794 (Wave 1, n = 7335) and 0.815 (Wave 2, n = 7308).
2.5.2 Impairment and Activity Limitation
The operationalisation of disability is very complex (WHO and World Bank 2011) and has varied across studies, even when using the same datasets. There is no internationally agreed definition of disability and similarly to other social constructs, disability is defined according to purpose (Fujiura and Rutkowski-Kmitta 2001). International guidance from the World Health Organisation recommends that the International Classification of Functioning should be used to measure disability (WHO and World Bank 2011). In this vein, the Irish Census measured disability in the 2006 and subsequent 2011 and 2016 population census (CSO 2006; CSO 2011; CSO 2016) incorporating two variables, one on impairment (long-lasting conditions) and one on functioning (difficulty in everyday activities) (WHO and World Bank 2011).
Our approach to defining impairment was conservative and only those children who had a specific, named impairment that persisted between waves were included. This approach provided the most consistent identification of disability across waves 1 and 2. Once the group of children with/without a persistent impairment between 9 and 13 years of age was identified, this group was further sub-divided into categories of children with impairment only/impairment and activity limitation. The resulting three-category impairment variable was used for all analyses: (1) no impairment, (2) impairment, and (3) impairment and activity limitation.
Given the changes in the type of respondents between GUI waves (children, primary caregivers and teachers at Wave 1/primary caregivers and children only at Wave 2), and alterations to the questions concerning impairment, the measurement of ‘persistent impairment’ and activity limitation was challenging. It proved necessary to combine both primary caregiver and teacher perspectives at Wave 1, and to link non-identical questions between waves, to settle on a final measure of impairment that would best capture the position at ages 9 and 13 years. For example, children were identified as having a persistent physical disability between waves if their primary caregiver at Wave 1 had reported that their child had a ‘sight problem requiring correction’ or a ‘hearing problem requiring correction’ or an ‘on-going chronic physical or mental health problem, illness or disability’ that relates to sight or hearing, or required ‘ongoing support to move around’; and at Wave 2 that the child had a ‘physical disability or visual or hearing impairment’. Primary caregiver responses were privileged where possible, but also incorporating teacher responses at Wave 1 enabled a variable for general learning disability to be included, and allowed for a more inclusive approach to identifying activity limitation. The child/young person’s perspective was not incorporated into the measure due to the perceived lack of relevant questions in the child questionnaire.
Named impairments selected for inclusion were: Physical disability (n = 247); Speech or language difficulty (n = 121); General or specific learning disability (n = 539); or an Autism spectrum disorder (n = 55). Children whose teacher (at Wave 1) or primary caregiver (at Wave 2) had identified a persistent emotional and behavioural difficulty (even if these children had an additional impairment) were excluded from the analysis (n = 81). This approach avoided any possible conflation between the measure of impairment as predictor, and the SDQ outcome variable, although running the analysis with these children included in fact made little or no difference to our overall results and conclusions. Despite the use of specific impairments to build up the more general disability variable, no disaggregated analysis of outcomes by impairment type has been included in this analysis, due to the cross-wave comparability limitations outlined earlier.
2.5.3 Migrant Background
Approaches to defining a ‘child with migrant background’ in the literature using the GUI data are varied, with the birthplace of the primary and secondary caregivers, the study child, and to a lesser extent their self-reported ethnicity and citizenship, combining in various ways to produce a migrant variable for the study child (Darmody et al., 2016; Smyth 2016; Coughlan et al., 2014). In this analysis, a child with migrant background has been defined as one whose primary caregiver (in the vast majority of cases, their mother) reported at Wave 1 that they were born outside of either the UK or Ireland. The UK was included in the criteria for non-migrant background for its historical, cultural and linguistic proximity with Ireland.
2.5.4 Family Context
Two indicators of family context were included in the analysis: highest level of primary caregiver education (as reported by the primary caregiver themselves at Wave 1), and the primary caregiver report on the conflict sub-scale of the Pianta Child-Parent Relationship Scale (also measured at Wave 1) (Pianta 1992). The latter scale contains 12 items (e.g. ‘My child sees me as a source of punishment and criticism’), with a minimum possible score of 12 and a maximum possible score of 60. This analysis calculated reliability of this scale, for the sample of children whose primary caregivers responded at both waves, as an acceptable 0.787 (Wave 1, n = 7355) and 0.826 (Wave 2, n = 7358).
2.5.5 Sociodemographic Indicators
The child’s gender was included in the analysis and also a measure of household income, both as reported at Wave 1. Equivalised household income (that is, total gross household income less statutory deductions of income tax and social insurance contributions, divided by equivalised household size (persons in the household)) was used for the bivariate analyses conducted for this study, but as a log10 transformed continuous variable of equivalised household income divided by 100, for the multivariate analyses.
2.6 Missing Data
Analysis of the distribution of responses between waves, across the six independent predictor variables and the outcome variable, revealed that loss from the sample between waves was indeed asymmetrical. Children from a migrant background, or who have primary caregivers with comparatively lower levels of education, or who are from lower income households, were more likely to cease participation in GUI between ages 9 and 13 years than their peers in other groups. For the purpose of this analysis, the loss of 21.1% of children from a migrant background, in comparison with only 11.5% of children from a non-migrant background, is of particular note. However, there was no evidence of asymmetrical drop-out from the sample for children with impairment/activity limitation.
Data was missing for SDQ at one or both waves for only 0.6% (n = 44) of children. Data was missing for our impairment/activity limitation variables for 5.9% (n = 443) of study children. The remaining independent variables had fewer than 0.5% of missing data, except for household income, which had 7% (n = 523). The combined effect of this missing data would have been the loss of 962 cases from the final multivariate analysis (unweighted data). Consequently a multiple imputation procedure using fully conditional specification was performed which incorporated all seven study measures plus an additional nine variables as predictors, and which resulted in imputed cases for the five study variables with missing data. This produced an analytical dataset for the final models that included all 7468 cases (unweighted data) remaining in the Wave 2 GUI sample.
2.7 Weights
All analyses were tested both with and without the Wave 1 sample weights applied. While they made little difference to the results, for the purpose of this paper they have been applied throughout to mitigate any lack of representation between the sample, especially for Wave 2, and population. Application of the weights gives an analytical sample for the final models of 7290 cases.
2.8 Ethical Approval
The Growing Up in Ireland study received ethical approval by the Health Research Board’s Research Ethics Committee in 2006 and 2007 for Wave 1 and by the Department of Children and Youth Affairs for Wave 2 (Murray et al. 2010; Thornton et al. 2016). An individual agreement by the authors of this paper with the Census of Statistics Office established the terms for safe data storage and anonymised reporting of results.
3 Results
The purpose of this study was twofold. First, the study aimed to explore whether Irish children with both disabilities and migrant background experience poorer socio-emotional outcomes, over time, than their peers without disabilities and with no migrant background. A second aim of the study was to investigate whether other socio-economic factors influence children with disabilities’ socio-emotional outcomes over time.
3.1 Sample Profile
A total of 884 children (12.0% of the full, cross-wave sample) were identified with any one of the selected, named impairments. Of these children, 545 (7.4% of the full sample) also had an activity limitation. The sample arises from the application of Wave 1 sample weights and multiple imputation. The subgroup of children with a migrant background includes 414 children (5.6% of the full sample). There are 43 children from a migrant background in our study, who also have an impairment (10.4% of all children with a migrant background). Of these, the majority (58.1%, n = 25) also have an activity limitation. We sought to further explore the concept of socio-emotional outcomes over time by identifying groups of children with similar patterns of stability and change in total SDQ score between age 9 and 13 years. This approach identifies three categories: a small group of 216 children (2.9% of the full sample), who are of particular interest to this study and who experience persistently poor socio-emotional outcomes between age 9 and 13 years (that is, with SDQ scores at or above the suggested ‘abnormal’ threshold of 17). A further 6598 children (89.5%) had SDQ total scores below the ‘abnormal’ threshold at age 9 and 13 years, and finally 558 children (7.6%) experienced a change in SDQ outcomes (whether an improvement or dis-improvement) between GUI waves.
Impairment as defined in this study was significantly associated with gender (Χ2 (2) = 29.22, p < .001), the primary caregiver’s level of education (Χ2 (6) = 32.56, p < .001), equivalised household income (F (2, 7287) = 10.295, p < .001), and the Pianta conflict sub-scale (Welch F (2,610.707) = 50.456, p < .001), although in all cases the effect size, measured in terms of Cramer’s V and Eta squared, was weak (Cohen, 1988). Inspection of the standardised residuals and post hoc tests indicated that the group of children with impairment and activity limitation was significantly more likely to contain boys than girls, children with primary caregivers whose highest education level was at lower secondary level or below, and children from households with lower income. Both groups of children with impairment, whether or not they had an additional activity limitation, came from households with significantly greater levels of parent-child conflict.
Coming from a migrant background was significantly associated with the primary caregiver’s level of education (Χ2 (3) = 141.8, p < .001) and equivalised household income (t (7526) = −3.442, p < .01), with the migrant group significantly more likely to include children whose primary caregiver’s highest education level was at primary degree or postgraduate level, but conversely whose mean equivalised household income was significantly lower than their peers. However, tests of association again indicated that the strength of these relationships was weak. Coming from a migrant background was significantly but weakly associated with poorer (higher) scores on the Pianta Child-Parent Relationship Scale (conflict) (t (835) = 3.463, p < .01.
3.2 Socio-Emotional Outcomes at Ages 9 and 13
A Pearson product moment correlation coefficient was used to examine the relationship between total SDQ scores (parent report) at waves 1 and 2. There was a statistically significant positive correlation between the two scores suggesting that higher scores at wave 1 tend to be associated with higher scores at wave 2 (r = .647, n = 7372, p < .001). The coefficient of determination for this correlation was r2 = 0.42, indicating a large relationship (Cohen 1988).
3.2.1 Multivariate Analyses
A Factorial ANOVA analysis was run to test for any interaction effect between having an impairment or an impairment and an activity limitation, and coming from a migrant background, on socio-emotional outcomes for Irish children at age 9, and again at age 13 (measured in terms of the total SDQ score at each separate wave).
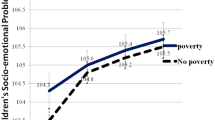
At Wave 1, our analysis did not find any statistically significant interaction between having an impairment and coming from a migrant background on SDQ total score, F (2, 6902) = .107, p = .899, partial η2 = .000 (n = 6908).
Similarly, at Wave 2, no interaction was found, F (2, 6929) = .979, p = .376, partial η2 = .000 (n = 6935) (see Tables 1 and 2).
Based on these findings we concluded that the GUI data did not suggest that children with an impairment and from a migrant background experienced additional challenges to those children with an impairment from a non-migrant background. However, ‘migrant background’ was retained in all subsequent investigations as this group was of interest to the study and no findings in relation to the SDQ have been reported for this sample.
We conducted a logistic regression to consider any possible associations between impairment and socio-emotional outcomes across waves (i.e., persistently poor scores, change of scores, scores below the threshold of 17), when account is taken of known predictors such as gender, primary caregiver education, conflict in the home, and household income, and retaining migrant background in the model. There was a good model fit on the basis of the migrant and disability variables (Model 1) (Χ2 (6) = 388.87, p < .001), and again with the addition of the four additional family and socio-demographic indicators (Model 2) (Χ 2(18) = 1407.89, p < .001). Model 1 explained only 9.9% (Nagelkerke R2) of the variance in socio-emotional outcomes over time, however Model 2 explained a much improved 33.4% (Nagelkerke R2) (see Tables 3 and 4).
In the final model (Model 2), neither gender nor coming from a migrant background had a statistically significant association either with children being in the ‘persistent difficulties’ category, or having an SDQ total score that changed above/below the ‘abnormal’ threshold between waves. Children whose primary caregivers had the lowest level of education had 2.6 times odds (95% CI, 1.8–3.8) of being in the category of children whose socio-emotional outcomes changed between waves, and 5.8 times odds (95% CI, 2.8–12.3) of being in the category of children with persistently poor outcomes between ages 9 and 13 years. An increase in parent-child conflict was also significant in predicting which children were in either the ‘persistent difficulties’ category or the group of children whose SDQ status had changed between waves, although the odds ratios were relatively small at 1.2 and 1.1 times odds respectively, for each point on the Pianta conflict scale. Lower household income also had a significant but small relationship with a child having abnormal socio-emotional difficulties at either age 9 or 13 years.
Most striking, however, is that children with impairment and activity limitation had up to 16.3 times greater odds (95% CI, 10.9–24.2) of being in the category of children with persistently poor outcomes, over and above the effects of known predictors such as child-parent conflict. The odds for children with impairment only of being in this category was somewhat lower (but still noteworthy) at 3.8 times odds (95% CI, 2.0–7.3). There did not appear to be a difference between the odds of children with impairment, and those with impairment and activity limitation, of being in the category of children with changing outcomes between waves, but children in either category had 3.1 (95% CI, 2.2–4.4) (impairment only) and 4.3 (95% CI, 3.3–5.8) (impairment and activity limitation) greater odds of being in this group than their peers with no impairment at all. In short, children with impairment alone, and in particular those with impairment and activity limitation, are much more likely than their peers without disability and non-migrant background to experience difficulties that persist between the ages of 9 and 13 years.
4 Discussion
This study aimed to explore longitudinal change in socio-emotional outcomes in children with disabilities and of migrant background using data from the Growing Up in Ireland study while also considering household income, primary caregiver’s level of education, gender, and conflict, due to their reported influence in socio-emotional outcomes in the literature. The study addresses gaps identified in the literature as it is one of the few studies, to the authors’ knowledge, to explore socio-emotional outcomes of children with both disability and migrant background, compared to their peers without disability and non-migrant background, using a national representative sample and following up the same children 5 years later. Given the sharp immigration increase in Europe and in Ireland, it is timely to use this European/Irish case as an exploration of the interaction between disability and migration. This was conducted in relation to socio emotional outcomes as both groups, disabled children, and children of migrant background, have been reported, albeit separately, as being more prone to experiencing poor socio-emotional outcomes.
The findings of this study resonate with previous research findings which have found significant relationships between disability and poor socio-emotional health (see Bakopoulou and Dockrell 2016; Bryan et al. 2004; Davis and Watson 2001; Emerson et al. 2019; Haft et al. 2019; Lindsay 2007; Van Agt et al. 2011) as disabled children were found to be up to 16.3 times more likely to experience poor socio-emotional outcomes over time than their peers without disability. This study found no significant interaction between migrant background and disability and poor socio-emotional outcomes, which is in line with previous findings (Cotter et al. 2019).
A number of migrant families left Ireland between the two data collection points in this study, and this sample reduction may have influenced the findings. There are additional issues that should be borne in mind: the sample of children with migrant background in GUI is dissimilar to the national population of migrant background. Migration to Ireland may be relatively recent compared to the profile of migrants in other nations and disabled children with more severe problems may be left in the country of origin (for example, with grandparents). However, evidence from the literature also suggests that other factors may have a stronger effect than migration background in children’s socio-emotional outcomes.
It is important to note that the present study found two socio-economic indicators, household income and primary caregivers’ level of education, to be significantly related to poor socio-emotional outcomes. The latter findings add to a growing evidence base pointing at socio-economic status as a main contributor to poor socio-emotional health for children with disabilities (Belhadj Kouider et al. 2014; Darmody et al. 2016). A recent study by Emerson and colleagues (2019) found a strong relationship between being a girl and experiencing poor socio-emotional outcomes, which does not resonate with the findings of the present study, in which gender was not a determining variable of socio-emotional outcomes. Sampling issues as well as age differences in the studies may account for the different findings in both studies.
The approach to defining disability used in this study provided nuanced results in relation to having an impairment and activity limitation versus an impairment only (WHO and World Bank 2011). The likelihood of having persistently poor socio-emotional outcomes was higher (almost 16.3 time odds) for children with impairment and activity limitation in contrast with children with impairment only. Although this study has not examined the role of support, the findings may imply that inadequate or lack of support (for example, school accommodations and professional services) may have a further influence in the experience of socio-emotional outcomes. Our findings highlight the importance of addressing socio-emotional outcomes in children with disabilities at an early age given their life-long impact on wellbeing, including health, employment, and education outcomes (Attanasio et al., 2020; Immordino-Yang et al., 2019; Layard et al., 2014; Miyamoto et al., 2015; OECD, 2015). The findings of this study suggest that using the categories of impairment versus impairment and activity limitation in large surveys provides a more nuanced understanding of the experience of disability.
4.1 Limitations
Two main limitations need to be considered in relation to this study. Firstly, Growing Up in Ireland is a national longitudinal study that was not developed with the specific purpose of measuring disability or migration and therefore, a number of possible items and item combinations could potentially have been used to better identify the combined sample of disabled children and children with migrant background. We therefore opted for a conservative approach in the definition of disability that provided the most consistent figures longitudinally. However, this disability definition may have left out of the sample some children living with impairment. Secondly, we used a liberal definition of migration to avail of a larger sample. The opposite effect may have taken place when identifying children with migrant background in our study: some children with migrant background in our study may not comply with more conservative definitions of “migrant background” and therefore we may have involved a relatively higher number of children. Related to the above limitation, identification of migrant national groups may have yielded more significant results as it has been documented that differences in academic and social outcomes may be influenced by national group rather than by migration background. An augmented sample of children with migrant background to further explore socio-emotional development of children with disability may address some of the issues identified above.
4.2 Recommendations for Future Research
Further research in relation to specific impairment types and children’s socio-emotional outcomes would enable better understanding of the problems and supports children may require. Similarly, this study has used a total socio-emotional score and details on specific emotional difficulties such as conduct disorders or depression may help fine tune mental health interventions and support required to address each socio emotional outcome.
4.3 Recommendations for Policy and Practice
This study brings to light an important area of focus for policy makers and service providers. Educational and social services need to be alert to the higher likelihood of children and adolescents with disability and their families requiring access to mental health support services in addition to other disability specific accommodations. Our results show that this is an even more important issue for such children living in lower income households and whose parents have lower levels of education.
References
Ashdown, D. M., & Bernard, M. E. (2011). Can explicit instruction in social and emotional learning skills benefit the social-emotional development, well-being, and academic achievement of young children? Early Childhood Education Journal, 39, 397–405. https://doi.org/10.1007/s10643-011-0481-x.
Attanasio, O., Blundell, R., Conti, G., & Mason, G. (2020). Inequality in socio-emotional skills: A cross-cohort comparison. Journal of Public Economics, https://doi.org/10.1016/j.jpubeco.2020.104171.
Bakopoulou, I., & Dockrell, J. (2016). The role of social cognition and prosocial behaviour in relation to the socio-emotional functioning of primary aged children with specific language impairment. Research in Developmental Disabilities, 49–50, 354–370.
Banks, J., & McCoy, S. (2011). A study on the prevalence of special educational needs. Trim: National Council for Special Education.
Becker, B., & Luthar, S. (2002). Social-emotional factors affecting achievement outcomes among disadvantaged students: Closing the achievement gap. Educational Psychologist, 37(4), 197–214.
Belhadj Kouider, E., Koglin, U., & Petermann, F. (2014). Emotional and behavioural problems in migrant children and adolescents in Europe: A systematic review. European Journal of Child and Adolescent Psychiatry, 23, 373–391. https://doi.org/10.1007/s00787-013-0485-8.
Bøe, T., Hysing, M., Skogen, J. C., & Breivik, K. (2016). The strengths and difficulties questionnaire (SDQ): Factor structure and gender equivalence in Norwegian adolescents. PLoS One, 11(5), e0152202. https://doi.org/10.1371/journal.pone.0152202.
Bryan, T., Burstein, K., & Ergul, C. (2004). The social-emotional side of learning disabilities: A science-based presentation of the state of the art. Learning Disability Quarterly, 27(1), 45–51.
Bryman, A. (2016). Social research methods. Oxford: Oxford University Press.
Central Statistics Office (CSO) (2006). Census 2006. Accessed November 2019 from https://www.cso.ie/en/census/.
Central Statistics Office (CSO) (2011). Census 2011. Accessed November 2019 from https://www.cso.ie/en/census/.
Central Statistics Office (CSO) (2016). Census 2016. Accessed November 2019 from https://www.cso.ie/en/census/.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum Associates.
Cosgrove, J., McKeown, C., Travers, J., Lysaght, Z., Ní Bhroin, O., & Archer, P. (2014). Educational experiences and outcomes for children with special educational needs: A secondary analysis of data from the growing up in Ireland study. Trim: National Council for Special Education.
Cotter, S., Healy, C., Ni Cathain, D., Williams, P., Clarke, M., & Cannon, M. (2019). Psychopathology and early life stress in migrant youths: An analysis of the ‘growing up in Ireland’ study. Irish Journal of Psychological Medicine, 36, 177–185. https://doi.org/10.1017/ipm.2018.53.
Coughlan, B., McKenna, P. P., Doherty, E., O'Neill, C., & McGuire, B. (2014). Minority status, social welfare status and their association with child participation in sporting, cultural and community activities. The Economic and Social Review, 45(1), 65–85.
Darmody, M., McGinnity, F., & Kingston, G. (2016). The experiences of migrant children in Ireland, chapter 9. In Williams et al. (Eds.), Cherishing all children equally? Dublin: Oak Tree Press.
Davis, M., & Watson, N. (2001). Where are the children’s experiences? Analysing social and cultural exclusion in ‘special’ and ‘mainstream’ schools. Journal of Disability and Society, 16, 671–687.
Dearden, L., Sibieta, L., & Sylva, K. (2011). The socio-economic gradient in early child outcomes: Evidence from the millennium cohort study. Longitudinal and Life Course Studies, 2(1), 19–40. https://doi.org/10.14301/llcs.v2i1.140.
Dunn, E. C., Crawford, K. M., Soare, T. W., Button, K. S., Raffeld, M. R., Smith, A. D. A. C., Penton-Voak, I. S., & Munafo, M. R. (2018). Exposure to childhood adversity and deficits in emotion recognition: Results from a large, population-based sample. Journal of Child Psychology and Psychiatry, 59(8), 845–854.
Elberling, H., Linneberg, A., Olsen, E. M., Goodman, R., & Skovgaard, A. M. (2010). The prevalence of SDQ-measured mental health problems at age 5-7 years and identification of predictors from birth to preschool age in a Danish birth cohort: The Copenhagen child cohort 2000. European Child and Adolescent Psychiatry, 19(9), 725–735.
Emerson, E., King, T., Llewellyn, G., Milner, A., Aitken, Z., Arciuli, J., & Kavanagh, A. (2019). Emotional difficulties and self-harm among British adolescents with and without disabilities: Cross sectional study. Disability and Health Journal, 12, 581–587. https://doi.org/10.1016/j.dhjo.2019.04.007.
Flouri, E., Narayanan, M. K., & Midouhas, E. (2015). The cross-lagged relationship between father absence and child problem behaviour in the early years. Child: Care, Health and Development. https://doi.org/10.1111/cch.12236.
Fujiura, G., & Rutkowski-Kmitta, V. (2001). Counting disability. In G. Albrecht, K. D. Seelman, & M. Bury (Eds.), Handbook of disability studies (pp. 69–96). Thousand Oaks: Sage.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology & Psychiatry & Allied Disciplines, 38(5), 581–586.
Goodman, R. (2001). Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337–1345.
Goodman, R., & Scott, S. (1999). Comparing the strengths and difficulties questionnaire and the child behavior checklist: Is small beautiful? Journal of Abnormal Child Psychology, 27, 17–24.
Greene, S., Williams, J., Layte, R., Doyle, E., Harris, E., McCrory, C., Murray, A., O’Dowd, T., Quail, A., Swords, L., Thornton, M., & Whelan, C. (2010). Growing up in Ireland National Longitudinal Study of children background and conceptual framework. Dublin: Office of the Minister for Children and Youth Affairs.
Haft, S., Chen, T., LeBlanc, C., Tencza, F., & Hoeft, F. (2019). Impact of mentoring on socio-emotional and mental health outcomes of youth with learning disabilities and attention-deficit hyperactivity disorder. Child and Adolescent Mental Health, 24, 318–328. https://doi.org/10.1111/camh.12331.
Hartas, D. (2016). Young people’s educational aspirations: Psychosocial factors and the home environment. Journal of Youth Studies, 19(9), 1145–1163. https://doi.org/10.1080/13676261.2016.1145634.
Humphrey, N. (2013). Social and emotional learning. London: SAGE Publications.
Immordino-Yang, M. H., Darling-Hammond, L., & Krone, C. R. (2019). Nurturing nature: How brain development is inherently social and emotional, and what this means for education. Educational Psychologist, 54(3), 185–204.
Layard, R., Clark, A. E., Cornaglia, F., Powdthavee, N., & Vernoit, J. (2014). What predicts a successful life? A life-course model of well-being. The Econometrics Journal, 124(580), F720–F738.
Lindsay, G. (2007). Educational psychology and the effectiveness of inclusive education/ mainstreaming. British Journal of Educational Psychology, 77, 1–24.
Mathai, J., Anderson, P., & Bourne, A. (2003). Use of the strengths and difficulties questionnaire as an outcome measure in a child and adolescent mental health service. Australasian Psychiatry, 11(3), 334–337.
McCoy, S., Banks, J., & Shevlin, M. (2016a). Insights into the prevalence of special educational needs. In J. Williams, E. Nixon, E. Smyth, & D. Watson (Eds.), Cherishing all the children equally? Ireland 100 years on from the Easter Rising. Cork: Oak Tree Press. Retrieved June 2019 from https://www.esri.ie/system/files/media/file-uploads/2016-10/CB201609.pdf.
McCoy, S., Maître, B., Watson, D., & Banks, J. (2016) The role of parental expectations in understanding social and academic well-being among children with disabilities in Ireland, European Journal of Special Needs Education, 31(4), 535-552. https://doi.org/10.1080/08856257.2016.1199607
Mieloo, C. L., Bevaart, F., Donker, M. C. H., Van Oort, F. V. A., Raat, H., & Jansen, W. (2014). Validation of the SDQ in a multi-ethnic population of young children. European Journal of Public Health, 24(1), 26–32.
Miyamoto, K., Huerta, M. C., & Kubacka, K. (2015). Fostering social and emotional skills for well-being and social progress. European Journal of Education, 50(2), 147–159.
Murray, A., McCrory, C., Thornton, M., Williams, J., Quail, A., Swords, L., Doyle, E., & Harris, E. (2010). Growing up in Ireland, National Longitudinal Study of children: Design, instrumentation and procedures for the child cohort. Dublin: Department of Health and Children.
OECD. (2015). Skills for social progress: The power of social and emotional skills. Paris: OECD Publishing Retrieved (June 29 2020) from https://read.oecd-ilibrary.org/education/skills-for-social-progress_9789264226159-en#page36.
Parish, S., & Cloud, J. (2006). Financial well-being of young children with disabilities and their families. Social Work, 51(3), 223–232.
Park, J., Turnbull, A., & Turnbull, H. (2002). Impacts of poverty on quality of life in families of children with disabilities. Exceptional Children, 68(2), 151–170.
Parkes, A., & Sweeting, H. (2018). Direct, indirect and buffering effects of support for mothers on children’s socioemotional adjustment. Journal of Family Psychology, 32(7), 894–903. https://doi.org/10.1037/fam0000438.
Pianta, R. C. (1992). Child-parent relationship scale. Unpublished measure. Charlottesville: University of Virginia.
Rice, L. J., Emerson, E., Gray, K. M., Howlin, P., Tonge, B. J., Warner, G. L., & Einfeld, S. L. (2017). Concurrence of the strengths and difficulties questionnaire and developmental behaviour checklist among children with an intellectual disability. Journal of Intellectual Disability Research, 62(2), 150–155. https://doi.org/10.1111/jir.12426.
Rose-Krasnor, L., & Denham, S. (2009). Social-emotional competence in early childhood. In K. H. Rubin, W. M. Bukowski, & B. Laursen (Eds.), Social, emotional, and personality development in context. Handbook of peer interactions, relationships, and groups (pp. 162–179). New York: The Guilford Press.
Smyth, E. (2016). Social relationships and the transition to secondary education. The Economic and Social Review, 47(4, Winter), 451–476.
Stone, L. L., Otten, R., Engels, R. C., Vermulst, A. A., & Janssens, J. M. (2010). Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4- to 12-year-olds: A review. Clinical Child and Family Psychology Review, 13(3), 254–274. https://doi.org/10.1007/s10567-010-0071-2.
Thornton, M., Williams, J., McCrory, C., Murray, A., & Quail, A. (2010). Sample design and response in wave 1 of the nine-year cohort of growing up in Ireland. Dublin: Office of the Minister for Children and Youth Affairs.
Thornton, M., Williams, J., McCrory, C., Murray, A., & Quail, A. (2016). Design, instrumentation and procedures for the child cohort at wave two. Dublin: Department of Children and Youth Affairs.
Tomlinson, S. (2015). Special education and minority ethnic young people in England: Continuing issues. Discourse: Studies in the Cultural Politics of Education, 37(4), 513–528.
Van Agt, H. M. E., Verhoeven, L., Van den Brink, G., & De Koning, H. J. (2011). The impact on socio-emotional development and quality of life of language impairment in 8-year-old children. Developmental Medicine & Child Neurology, 53(1), 81–88.
Van der Mark, E., Conradie, I., Dedding, C., & Broerse, J. (2017). How poverty shapes caring for a disabled child: A narrative literature review. Journal of International Development, 29(8), 1187–1206.
Vaz, S., Cordier, R., Boyes, M., Parsons, R., Joosten, A., Ciccarelly, M., Falkmer, M., & Flakmer, T. (2016). Is using the strengths and difficulties questionnaire in a community sample the optimal way to assess mental health functioning? PLoS One, 11(1), e0144039. https://doi.org/10.1371/journal.pone.0144039.
Watson, D., Whelan, C. T., Maitre, B., & Williams, J. (2015). Family economic vulnerability and the great recession: An analysis of the first two waves of the growing up in Ireland study. Longitudinal and Life Course Studies, 6(3), 230–244. https://doi.org/10.14301/llcs.v6i3.331.
WHO and World Bank (2011). World report on disability. Accessed on December 2019 from https://www.who.int/disabilities/world_report/2011/en/.
Funding
This study was conducted with funding from the Faculty of Arts, Social Sciences and Humanities Benefactions Fund and the Trinity Immigration Initiative (Trinity College Dublin).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Swift, A., Iriarte, E.G., Curry, P. et al. How Disability and Other Socio-Economic Factors Matter to Children’s Socio-Emotional Outcomes: Results from a Longitudinal Study Conducted in Ireland. Child Ind Res 14, 391–409 (2021). https://doi.org/10.1007/s12187-020-09768-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12187-020-09768-y