
Abstract
Based on findings of Stevens and Vollebergh [69], who analyzed cross-cultural topics, this review considers the current prevalence of emotional and behavioral problems of native children and adolescents in comparison with children with a migration background in European countries. 36 studies published from 2007 up to 2013 chosen from a systematic literature research were included and analyzed in their perspective design in detail. Previous studies showed great differences in their results: Especially in Germany, many studies compare the heterogeneous group of immigrant children with native children to analyze an ethnic minority or migration process effect. Only a British and Turkish study demonstrates the selection effect in migration. Most Dutch or British studies examined different ethnic groups, e.g. Turkish, Moroccan, Surinamese, Pakistani, Indian or Black migrant children and adolescents. Migrant childhood in Europe could be declared a risk in increasing internalizing problem behavior while the prevalent rate in externalizing problem behavior was comparable between native and migrant children. A migration status itself can often be postulated as a risk factor for children’s mental condition, in particular migration in first generation. Furthermore, several major influence factors in migrant children’s mental health could be pointed out, such as a low socio-economic status, a Non-European origin, an uncertain cultural identity of the parents, maternal harsh parenting or inadequate parental occupation, a minority status, the younger age, gender effects or a specific culture declaration in diseases.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the past emigration dominated in many European countries, but in recent years immigration has increased. As a result, the treatment of immigrated families constitutes a growing challenge in many European societies [66, 67]. In consequence, the proportion of children with an immigrant background continues to rise in many European countries: in Switzerland there are already 39 %, in Germany about 26 %, in UK and France about 17 % [34]. On the one hand migration is often associated with a familiar and traditional dislocation; on the other hand, adaptation to the new society represents a major challenge [43]. Integration problems, a low life satisfaction or a difficult identity formation are the results for subsequent generations. Furthermore, discrimination against persons with a migration background is a common phenomenon in host societies [13]. The impact of potential psychological stress due to migration or an immigration background in children’s and adolescents’ development is increasingly discussed. To provide a better understanding of mental health in European migrant children they should be looked at in more detail to examine whether prevalence rates in mental disorders of migrant and host children differ. Due to the increase of migrant children in recent years, this review will present the current state of their mental health in European countries.
Migrants in Europe
The accurate definition of migration background often remains vague. In general, an immigrant background is defined if national frontiers were crossed [66]. In public debates words like foreigners, immigrants, migrant background or ethnic origin are understood to be equivalent. Immigrant people are increasingly referred to as “people with or without an immigrant/migrant background”. However, this expression is not always defined equally. The Federal Statistic Office of Germany integrates information on personal characteristics and features of parents for the definition of a migration status. This includes information about time of immigration, naturalization or nationality. In Germany people who immigrated after 1950 and their descendants are described as people with immigrant background. In each case the first migration generation is separated from following generations (second and higher). In addition, since 2005 the definition of an immigrant background is separated into a narrow or a broader sense. This means that immigrants in a narrow sense are born abroad and decided to immigrate to Germany or gained German citizenship at birth while living in a household with one parent from abroad. Immigrant backgrounds in a broader sense refer to persons with foreign roots who do not live with their parents [66, 67]. In contrast to the German definition, only the first and second generation and another country of birth are defined as a migration status by the European Commission. All subsequent generations are not covered. About 6.5 % (32.5 million) of the total population in 2010 among the 27 European Union countries have foreign nationalities. The country of birth is also used as a feature of ethnicity by the European Commission while the nationality may change. According to this classification 9.4 % (47.3 million) of the total population in 2010 lives in Europe with foreign roots, approximately 31.3 million were not born in an EU country and 16.0 million are from another EU country [74].
Cross-cultural differences or migration as influence in mental health
Cultural differences in prevalence rates of mental disorders exist generally worldwide, irrespective to migration experiences [78]. Already in early childhood, general ethnic differences in temperament are evident: Bornstein and Cote [12] showed that Latin and Japanese children 20 months of age are more pleasant than the Europeans; at the same time Japanese are significantly more choleric than European young children. Particularly, cross-cultural differences in parenting styles could be demonstrated in Turkish and German mothers. This varying education can result in different child behavior [42]. Additionally, even European countries may be different in prevalence of mental disorders in childhood: an advantage in mental health from Norwegian 8- to 10- year-old children in comparison with British children is ascertained [33].
Beyond cross-cultural differences as these, the question can be raised whether in addition a migration or an immigrant background changes mental health. Development of deviant behavior in childhood is suggested to be very complex [53]. Opportunities in the environmental living situation of children with immigrant background differ for various reasons from those without immigrant backgrounds [23]. Special conditions in migrant children may result in more psychological stress than in their host children counterparts. One possible reason is that the population of migrant children and adolescents is generally in minority in European host societies. Particularly, many migrant families in European countries are living in low socioeconomic circumstances in often deprived neighborhoods. Many migrant children have, therefore, limited skills in the language of the host country which can result in less social competence and lower school success [17]. As a consequence, isolation from host society and turning to the origin ethnic group may increase. Furthermore, results of large-scale student surveys in Germany show that one in six young people with migration background describe discriminatory experience [7]. Discrimination itself is shown as a factor which provokes internalizing problems in migrants [51]. Due to differences in culture migrant children may face special challenges in development: the quest for identity and the cultural affiliation or orientation towards family and school standards differ in many aspects [23]. Psychosocial stressors may result in higher mental prevalence rates in European migrant children. Significant differences between native and migrant youths are already demonstrated by surveys of German students in 2005: In robbery, personal injury, extortion and the number of recorded violent acts, native children are less represented [6].
These results raise the question whether in the prevention, diagnosis or therapy of children and adolescents with an immigrant background, special attention should be paid to certain development tasks in migrant children. Showing different results in this context, a review article from Stevens and Vollebergh [69] integrated studies published up to 2006. To analyze cross-cultural topics in a suitable manner, these authors showed various perspectives in study designs with migrant children. Based on these findings, this present review will provide a topical overview of all peer reviewed studies (externally assessed) since January 2007 up to March 2013. In comparison with native children or to other immigrated groups, the prevalence of emotional and behavioral problems in migrant children and adolescents living in Europe will be inspected.
Mental disorders of children and adolescents
This review reports issues of emotional or behavioral problems such as mental disorders of children and adolescents with immigrant background in comparison with native children. The criteria for mental health are the following: a membership to a majority, living without grave mental problems, compliance with daily hassles and sufficient adaption in society [53]. To notice possible mental disorders, information about deviating behavior should be found in psychological diagnostics. The presence of specific symptoms, usually a clinical significance, specific exclusion criteria and the onset and development of diseases are defined as mental disorders in the international categorical classification by the world health organization (WHO) [39]. Even in early childhood deviations from a positive development can result in somatic and psychological relevant forms of disease [52]. This present review focuses on behavioral and emotional problems: based on the definition of Achenbach [1], externalizing behavior includes aggressive and hyperactive behavioral problems, whereas internalizing problems comprise depressive or anxiety symptoms. Other behavioral problems or disorders as psychoses or personality disorders are not especially covered in this review. Compared with native children, however, the description of mental disorders and migration itself suggests that orientation in host society represents a great challenge for children with an immigrant background.
Methods
Literature search
Based on manual searches and systematic literature research in databases such as Pubmed, PsychInfo and Web of Science (July 2012–April 2013) this review detected original studies comparing children with and without immigrant background and their behavioral problems in European countries. This present study is in accordance with the methodic standards for the conception of systematic reviews [15]. To filter out all relevant studies and integrate all definitions of mental disorders/behavioral problems or an immigrant background, many terms are selected. The following key-words were used in the search:
-
Mental disorders (emotional and behavioral problems): [mental disorders OR mental health OR behavior disorders OR behavio(u)r(al) problems OR problem behavior OR internalizing OR externalizing OR emotional problems OR psychopathology OR psychiatric problems OR affective disorders OR anxiety disorders OR attention-deficit-disorder OR hyperactivity OR chronic-mental-illness OR conduct-disorder OR impulse-control-disorders OR neuroses] AND
-
Childhood: [children OR adolescents OR youth] AND
-
Immigrant background: [migration background OR immigrant background OR migrant OR culturally and linguistically diverse populations OR linguistic and cultural diverse background OR ethnic minority population].
Study selection
Different aspects of mental health analysis of children with immigrant background are shown in the results of Stevens and Vollebergh [69]. They describe four perspective designs of studies in migrant children, of which three perspectives are included in the present analysis. The cross-cultural perspective is reported by Stevens and Vollebergh [69], but excluded in this review. In this context, cross-cultural comparison defines cultural differences in general, such as different behavior for cultural reasons, different parenting or in general different ways of life, but not the comparison between different behavior problems caused by migration. Based on findings by Stevens and Vollebergh [69] the following perspectives are integrated into the present analysis:
-
1.
Selection effects of migration: Comparison of random samples comprised of children and adolescents with an immigrant background in the host country with random population samples in the original country.
-
2.
Migration process effects: Comparison of samples comprised of children and adolescents with an immigrant background in the host country with matched groups in the original/host country. In this perspective, the generation of migration (first, second, third) is included as factor.
-
3.
Ethnic minority effects: Comparison of samples comprised of migrant children and adolescents in the host country with native samples in the host country. Studies comparing different immigrated ethnic groups in the host country are also included in this category.
The use of perspective for each study is evaluated and the following further criteria are defined as a restriction:
-
Studies with children and adolescents aged up to 20 years are included.
-
All studies show children and adolescents with and without immigrant background or in general different immigrated ethnic groups in comparison. Analyses exclusively of one ethnic group are not accepted.
-
An immigrant background is defined if national frontiers were crossed.
-
Children and adolescents with immigrant background represent the first, second or third generation. All other generations are not taken into consideration.
-
Peer reviewed publications in English or German since January 2007 up to March 2013 are included.
-
Differences between groups have to be statistically safeguarded; the sample size amounts at least N = 50 and differences are tested for statistical significance.
-
The studies analyze prevalence of mental disorders or behavioral problems of children and adolescents. The mental disorders have to be classified in a valid form: with expert diagnosis based on ICD-10 [39] or with validated questionnaires as measure instruments, e. g. CBCL [1] or SDQ [29]. Studies with self-devised questionnaires required a sample size of at least N = 500 (large-scale studies).
-
Studies with pervasive or circumscribed developmental disorders such as autism or language development disorders are excluded. These kind of mental disorders are due to genetic aetiology [31, 63] and not caused by migration or developmental reasons.
-
Given their high specificity, analyses about eating disorders, psychoses, personality disorder or suicide are excluded.
-
Furthermore, studies especially on asylum seekers/refugees in the context of migrant children or adolescent are excluded because these kinds of issues are also very specific. Suffering from traumatic experiences, these populations often undergo certain psychological crises which differ from labour migrants.
Results
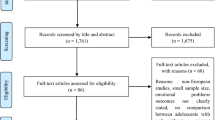
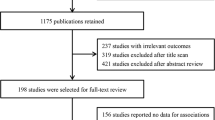
The systematic literature search identified 1,625 potential studies. Taking due account of all listed criteria, 36 studies were finally integrated (Fig. 1). Only one of these studies analyzed the selective perspective (a Turkish and British study), two studies especially deal with the migration process (Swiss studies), and four include a combination of migration process and ethnic minority perspective (one German, Dutch, Italian and Norwegian study). The majority of the included studies (29) report the differences between native and migrant children exclusively in the ethnic minority perspective (four German, nine Dutch, one Belgian, one Swiss, one French, one Italian, three Swedish, three Norwegian and six British studies).

Flow on study selection
The age of analyzed children and adolescents varied: one study observed babies aged one, six studies report mental health of preschoolers (age 3–6), three studies examined elementary school children (age 6–10), 18 studies analyzed adolescents (age 11–20) and nine studies comprised another or greater spectrum from age one up to 20. Information about the mental development of the children comes from different sources, depending on the age of the children: In total one study is a report from professional diagnostics, eight studies are parents reports, in five studies, parents and teachers described mental health of children, two studies are teacher- or caregiver-reports, one study is a teacher- and self-report, three analyses are parent- and self-reports and the majority of 16 studies are self-reports of adolescents. All studies in the following result descriptions are listed in the tables (Tables 1 and 2).
Description of included studies with selective and migration process perspective
Selection effect
Table 1 reports studies describing the selection effect, the migration process and the combination of migration process and ethnic minority effect. The first study of Daglar, Melhuish and Barnes [18] analyzed preschool behavior among Turkish immigrants in UK, other migrants and non-migrant families from Turkey. The results show that migration itself can be defined as a risk factor. Turkish children who immigrated to the UK and other migrant children in Turkey showed significantly more parent- and teacher-reported externalizing problems than children of the non-migrated Turkish subsample. The difference between the groups of migrant children is also significant: Turkish immigrant preschoolers in UK had the highest score in externalizing and internalizing problems and they additionally showed emotional dysregulation and less social competence.
Migration process effect
Two Swiss studies [41, 72] exclusively show the migration process perspective in emotional and behavioral problems in migrant adolescents in relation to time of migration. With regard to the generation of migration, the youths of second and first generation do not differ in mental health in the first Swiss study [41]. Furthermore, no generation effect in migration was evident in the Italian [52] and Norwegian [29] study. In contrast to these results, one German, one Dutch and the other Swiss study [31, 64, 72] found higher emotional and behavioral problem rates of first-generation immigrated children and adolescents compared with second-generation migrant children. In findings of self- and parent-reported Dutch, Swiss and German studies, the personal migration experience in childhood can be identified as a factor that is likely to increase vulnerability for internalizing and/or externalizing problematic behavior.
Description of included studies with ethnic minority perspective
Combination of ethnic minority and migration process
Four studies assessed the ethnic minority perspective in combination with the migration process, as reported in Table 1 [25, 27, 48, 62]. The ethnic groups analyzed differ between the host countries. The German study [62] examined children with an origin in the Former Soviet Union. In the Dutch study [27], the ethnic background was related to the colonial history of the Netherlands from Antillean, Cape Verdean, Surinam (Creole and Hindu) and in addition to other European countries, Morocco and Turkey. In the Italian study [48], the ethnic origin of the samples covered Mauritian, Albanian, Chinese, Romanian, Georgian and Moroccan immigrants. Without ethnic differentiation, the Swiss [38, 69] and Norwegian [25] studies only differentiated between native and migrant children. Results of ethnic groups in emotional or behavioral problems are different. The German study [62] shows high self-reported internalizing problem behavior in former Soviet Union. The externalizing problem behavior is most conspicuous in first-generation migrated adolescent groups in comparison with native children and children with former Soviet Union background in general. In the Dutch study [27] differences between migrant and native children were found to be significant, except in Surinamese Creole children. The parent-reported problem behavior rate was higher in migrant children for almost all ethnic groups. Margari et al. [48] analyzed a teacher report of the behavior of migrant elementary school children. Comparing native and migrant children in Italy, more externalizing and internalizing problems were manifest in the native group. In a detailed analysis of ethnic differences, Moroccans had significantly higher scores in externalizing behavioral problems in comparison with all other ethnic migrant groups. Furthermore, the Norwegian study [25] compared first and second generations with refugees. No differences in self-reported depressive symptoms could be made out between any of the three migrant groups, but migrant children have significantly more depression symptoms in comparison with natives.
Ethnic minority perspective: natives and migrants in general
All studies analyzing the ethnic minority perspective in general are shown in Table 2. Many studies [10, 19, 20, 28, 36, 37, 40, 45, 47, 59, 61, 63, 76, 77] only reported differences between native and migrant children in general. The German studies often noted higher prevalence in problem behavior in migrant children. The Children and Adolescent-Health-Survey (KIGGS) determined a decreasing contrast with age in behavior problems; the difference between migrant and native children in early childhood is higher. Furthermore, the pro-social behavior in migrant childhood increases in adolescence [35]. In a German study of Schreyer and Petermann [62] preschoolers with immigrant background showed higher externalizing behavior problems whereas Kuschel et al. [45] identified no differences in externalizing behavior in 4-year-old children, but significant disparities in internalizing problem behavior in comparison with native children. Inspecting adolescents with conduct disorders in a German clinical sample, migrant youths are not disproportionately represented [10]. These results are confirmed by a sample of outpatients in a forensic psychiatric clinic and non-violent peers in the Netherlands, showing no self-reported differences of Dutch and migrants [36]. In relation to ethnic density in school classes, Gieling, Vollebergh and van Dorsselaer [28] conclude that with regard to externalizing behavior, there is more problem behavior in migrant children if the majority of class members are Dutch. In reverse, Dutch children showed higher externalizing problem behavior in classes with high migrant density. However, being in minority seems to affect mental health in a negative way. One Belgian study showed higher self-reported prevalence rates in externalizing behavior and anxiety in native youths, whereas in migrant adolescents there were increased rates in disorders such as traumatic stress, avoidance symptoms and in addition more problems with peers [20]. Comparing Swiss and migrant adolescents, the native group was more represented in externalizing behavior, but not in internalizing behavior problems [37]. Excluding suicidal thinking in this Swiss study, the prevalence rate changes and native youths reveal significantly more internalizing symptoms. These results indicate a higher risk for suicidal thoughts in migrant youths. Vieno et al. [76] describe a self-reported higher prevalence in mental problems in migrant youths in Italy. The South East Sweden Birth Cohort-study does not notice any differences among children aged twelve due to migration or an immigrant background. In contrast to these results, comparisons between native and migrant adolescents in Norway identified higher externalizing behavior problems in migrant boys [47]. In general, more problems of migrant youths in comparison to native Norwegians are shown in the study of Sagatun et al. [59]. They report poorer mental health than natives with the exception of hyperactivity and prosocial behavior; within these disorders no ethnic differences were found. In a large-cross-cultural study in the UK, Canada, the US and Australia, migrant preschool children showed even the same externalizing problem behavior as all native groups [77] whereas internalizing problem behavior was higher in migrant children in the US and the UK [40]. In addition Jackson et al. [40] ascertained differences between the US and the UK in externalizing problem behavior: in the US native children are more prevalent while there are no ethnic differences in the UK. In conclusion, regarding natives and migrants in general, it is not possible to say that migrant children have generally higher prevalence rates in mental disorders.
Ethnic minority perspective: natives, European and non-European migrants
A comparison of native, other migrant European and migrant non-European studies can be obtained in Table 2. These groups were examined solely by Dutch, French and Swedish studies [16, 41, 58]. In a sample of the Generation R study conducted in the Netherlands [41], parents reported higher emotional and behavioral problems already in early childhood in second- and third-generation migrant children in comparison with native children. In these findings the non-Western migrant babies were significantly more vulnerable to externalizing and internalizing problem behavior [41]. The difference between the migrant groups (non-European and European) is solely significant in internalizing problems. The same findings on highly non-European migrants’ prevalence in ODD as ADHD and in general unhealthy behavior in adolescents were evident in self- and parent-reported studies in France and Sweden [16, 58]. These findings indicate a non-European origin in migrant children in Europe as a great challenge. This seem to be a danger to expand a vulnerability in children development. However, even young non-European migrant children showed more emotional and behavioral problems in comparison with native children. Similar to this, analyses with older children and adolescents showed the same higher prevalence in non-European migrant adolescents.
Ethnic minority perspective: differentiation in ethnic origin
Especially the Dutch studies, one Norwegian and several British studies compared native and migrant groups by differing the ethnic groups [5, 11, 24, 30, 47, 54, 56, 59, 70, 72, 73, 75, 79]. With respect to the migrant situation, Dutch studies analyzed the groups of Surinamese, Antillean, Moroccan and Turkish migrant children. Bevaart et al. [11] showed different findings dependent on which person reports. Measured with the SDQ [29], were reported no significant ethnic differences in total child problem behavior by teachers. In contrast to this teacher description Dutch parents confirmed more problem behavior in their children than all migrant counterparts. Observing migrant groups more closely, Surinamese parents described more problems in their children behavior than Antillean and Moroccan migrant parents, but the lowest prevalence rate was identified by Turkish migrant parents. Zwirs et al. [79] showed differences in the kind of children’s mental disorders in parent- and self–reported ethnic analyses. While in externalizing behavior problems there were no significant ethnic differences, Moroccan migrant children had a higher prevalence rate in affective disorders. In the context of anxiety disorders, Dutch native children showed higher symptoms than all other ethnic migrant groups [79]. Similar to other studies [12, 20], Van de Loij-Jansen et al. [70] filtered out detailed differences in type of disorder and the person reporting. In a sample of the Youth Health Monitor in the Netherlands parents reported higher internalizing symptoms in Surinamese and Moroccan children in general. Assessing anxiety or depression, 9- and 10-year-old Turkish children reported the highest rate of symptoms. Furthermore, the self-report in emotional problems is equal to the parent report: the Surinamese migrant children felt significantly more sensitive than all other analyzed ethnic groups [70]. One other Dutch study considered migrant Moroccan children in the Netherlands more closely. Boys of general population and incarcerated boys were compared with respect to their ethnic differences in mental health. In comparison to natives, Moroccan boys themselves and their parents reported lower internalizing and externalizing problem behavior. However, these ethnic disparities are lower than the comparison between the general and the incarcerated group. Furthermore, the authors of this study reflect differences in the implication: Dutch youths seem to need more clinical interventions, whereas for Moroccans other forms of adequate support as educational training may be required [75]. Two other studies listed detailed differences between migrant Turkish and native Dutch children [72, 73]. In both studies the Turkish children were less represented in internalizing problem behavior compared with native Dutch. The youths are not similar in externalizing behavior problems: certain findings show higher rates in Dutch adolescents [73] while in other results Turkish boys are similar to Dutch boys [72].
The Norwegian study observed more closely Pakistani youths in comparison with natives and other migrants. In internalizing problem behavior, there was no difference in these three groups whereas in hyperactivity and conduct disorders, native adolescents were more strongly affected compared to the ethnic minority subsample [59]. In these findings Pakistanis are not particularly noticeable in mental disorders. In contrast to this, Pakistani second generation migrants in the UK are more obvious in mental health in comparison to 7-year old Indian migrant children [56]. Another study makes in-depth analyses with an Indian subgroup in comparison to native white UK children and adolescents and confirmed previous measures: Indian migrants had fewer externalizing disorders and there were no differences in internalizing disorders in comparison to the white UK group [34]. These findings are not proved in a parent-reported sample in London: Indians were equal to British children in externalizing problem behavior while Indian migrants had more internalizing problems [5]. One further British study specifies differences in mental health between ethnic groups. A teacher-report identified ethnic differences in children with intellectual disabilities. This specific sample shows higher emotional and behavioral problems in Black British first-, second- and third-generation immigrated groups compared with South Asian migrants in Birmingham, UK [24]. In conclusion, these findings demonstrate that there is no consistent prevalence of one ethnic group. Based on these results, in cannot be determined if cross-cultural differences influence in particular migrant children's problem behavior.
Discussion
Advantage in internalizing problem behavior in migrant children in Europe
In comparing all included studies, it could be shown that there is a high risk in increasing internalizing problems in migrant children in Europe, much higher than in externalizing problems. All studies analyzing in detail externalizing problem behavior had break-even results: 11 studies [18, 24, 35, 40, 41, 54, 59 , 62, 63, 69, 72] noticed higher prevalence rates in migrant children in general or specifically in one ethnic group; nine studies [20, 30, 37, 40, 47, 48, 75, 77] determinated lower rates in migrant children, and ten studies [5, 10, 28, 36, 38, 45, 47, 72, 77, 79] found externalizing problem behavior equally in migrant and in native children groups. Some studies provided different findings, e.g. Van Oort et al. [72] showed no differences in boys, but migrant girls showed higher externalizing behavior than their native counterparts. In most of the included studies describing internalizing problem behavior a higher rate in migrant children in Europe is clearly shown: only four studies [20, 48, 75, 79] reported more internalizing problems for native children and five studies [28, 30, 37, 38, 56] showed no ethnic differences. The majority amounting to 16 studies [18, 20, 24, 25, 35, 40, 41, 45, 47, 59, 62, 69, 70, 72, 73, 79] reported higher internalizing problem rates in migrant children, irrespective of the country.
This review describes emotional and behavioral problems in migrant children in Europe. Study designs and findings in current European studies of the included studies are very different. Therefore, it is not possible to notice equal results in migrant children’s mental health in Europe in a uniform way. Furthermore, these various findings give rise to many questions. The results of the studies suggest that migration background is not the strongest risk factor for mental health. The following section shows further influencing factors in migrant children’s development beyond the perspective regards of migration.
Further factors influencing mental health in migrant children
Living situation and family background: parenting and family’s functioning
The migration background in the included studies suggests that this aspect is not causally the highest impact factor in migrants’ mental condition. Cross-cultural differences as in parenting style of origin country may collide with standard values in host countries. In multiple analyses, family functioning or parenting was further associated with emotional and behavioral problems in migrant children [18]. For example, maternal harsh parenting could be identified in the mediator analysis of Flink et al. [27] to have a strong relation to overall problems and migration background. Furthermore, parental occupation in the Netherlands was significantly lower in Turkish boys than in native Dutch or in female Turkish migrants. Otherwise, it could be shown in a clinical sample by Belhadj Kouider et al. [10] that inadequate parenting predict higher aggressive symptoms. Family functioning is in addition important for migrant children’s mental health [11, 58]. A family structure with one-adult-household was identified as a risk factor in emotional and behavioral conditions in migrant youths in Sweden [14]. Results of a Belgian study showed that the actual living situation in a host country and traumatic experiences are particularly influencing factors in migrant children’s mental health [20].
Education level, language competence or socio-economic status
A low level of education or a low SES is in general a risk factor for emotional or behavioral problems in children. In this sense, most studies show a negative association between a low level of education and mental health problems for children with and without immigrant background. Migration often results in a decrease of socio-economic status. As an example, one German study found that a high population in migrant children lives with low socio-economic background conditions [62]. The degree of language competence of the host country’s language may even affect social competence or mental conditions in migrant children’s development in different ways. Schreyer and Petermann [62] report that in a migrant subsample in preschool children only about 40 % of migrant families spoke German as preferred language.
Cultural identity, acceptance and integration in host country
In addition, cultural identity is filtered out as impact factor in mental health in a Dutch study: especially non-Western migrant parents often do not feel part of the Dutch culture and they reported low feelings of acceptance by Dutch natives. Both factors, culture identity and acceptance feelings of the parents, correlate significantly in overall problem rate in migrant young children [41]. However, more detailed Swiss analyses could show that inadequate social integration strongly increases mental risk behavior [37]. Further, an Italian study showed that experiences with bullying victimization in migrant children may result in a higher prevalence in psychosomatic symptoms and lower self-reported health, as well as life satisfaction and happiness [76]. Often, the identity search in adolescents differs in two ways in comparison with native youths: they develop neither the identity of the host society, nor that of their parent’s origin culture. Many migrant youths create a personal third, sometimes hybrid, identity [23]. Cultural identity often develops in dependence of the religious affiliation. With regard to the type of mental problem and religious background, the ethnic groups showed no similar prevalence rates in mental disorders. Many studies with the same ethnic groups presented different results [5, 11, 30, 54, 70, 72, 73, 75, 77]. Nevertheless, in their Swiss studies, Hüsler and Werlen [38] identified lower alcohol consumption, less conflicts with parents and lower suicidal tendencies in Muslim youths than in their majority Christian counterparts. A non-European background as well as being Black or with an Islamic membership was perhaps not as accepted in the current host European societies as in other European or Christian migrant counterparts. This subjectively experienced distance between native and migrant children may also explain higher emotional and behavioral problem rates in aforementioned migrant groups.
Special development tasks in dependence to age
In relation to age the decreasing risk in internalizing and externalizing behavioral problems is discussed by Hölling et al. [35]. The differences in migrant and native youths’ mental risk behavior vary, but not as high as in young children disparities. Migrant families with young children often prefer the language of their original country at home [62]. With their entry in kindergarten or school the capabilities of the host country language often increase in migrant children. This may result in better mental health or social competence over the years. Nevertheless, it should not be forgotten, as discussed previously, that especially adolescence is a difficult stage in forging identity. Family, peer and school standards vary and may collide. While in many European schools and native families’ individualistic values as autonomy, self-employment and regulation dominate, migrants often prefer other standards in parenting [42]. In migrant’s education more collectivistic aspects are often pointed out such as obedience, solidarity, loyalty, reliability and higher controlling of parents. These family and personal standards differ often from standards of host countries at school and thus the forming of a personal identity is a great challenge for migrant youths. As mentioned above, they often adopt neither the identity of parent origin country nor the identity of host country, but a third and mostly instable identity [23]. This challenge in migrant adolescence may further result in mental problems.
Gender education
In gender education also differences between migrant and native children exist [27]. For example, Carlerby et al. [14] proved that in girls with parents born abroad the prevalent rate is higher than that in native Swedish adolescents. In contrast to this, in the same sample, migrant boys with binational parents had more emotional and behavioral problems than their Swedish native counterparts. Being foreign may be a greater challenge for girls, but finding orientation in a host society in combination with two standard values in the personal family seem to be more challenging for boys. Many other studies show gender differences in mental health [10, 11, 14, 16, 18, 19, 24, 25, 27, 35, 38, 41, 45, 48, 58, 59, 62, 68, 70, 73, 75–77] and many of them proved higher internalizing problems in girls and in reverse higher externalizing problem behavior in boys [10, 14, 16, 18, 25, 38, 41, 59, 62, 68, 75–77], mostly in independence to a migration background. Steinhausen et al. [68] showed that also the interaction between gender and nationality may be significant: male double-citizens perceived more paternal warmth whereas the opposite was true in females.
Clarification of diseases
Beyond age and gender, the type of report is of importance. In a Dutch study of Bevaart et al. [11], teachers had other impressions of the same children population than their parents. Teacher in general reported higher problem perception without any significant ethnic differences, whereas parents reported lower problem rates, and thus, here ethnic differences were significant. Teachers as professionals may interpret children’s behavior in a different way. Teachers in host countries are actually often natives and stick to the standard values of the host country regarding emotional and behavioral problems in children development. However, they observed no ethnic differences. The ethnic differences in parents’ interpretation of the same children may be reasoned in cross-culturally different symptom awareness and a different way of labeling risk behavior as problematic. Native Dutch parents may show more sensitivity in acknowledging emotional and behavioral problems in their children. On the other hand, migrant parents are more likely to interpret the same symptoms differently. In dealing with psychological problems, there is often the fear of stigmata and further special declarations in migrant families. Emotional problems were commonly observed in a physical, religious or mystical way [44]. In consequence, this may result in describing lower mental symptoms and a lower utilization of psychiatric health care in migrant families [10].
Dependence on European country
Comparing migrant and native children, results in the Netherlands, Switzerland, Norway or Great Britain showed equal or lower prevalence rates in mental disorders, while in Germany, Italy or Sweden there are mostly higher prevalence rates in the migrant group. Therefore, it raises the question if in Germany, Italy or Sweden living conditions are worse which in consequence would declare the higher problem rates in migrant children. Especially in the Netherlands and Great Britain many studies analyzing migrant’s mental health were found. This additionally shows a high interest in their migrant children and adolescents’ mental condition, more than in other European countries.
Main results
Migration as a risk factor?
As a conclusion of this review, it may be stated that a migration background in Europe is not in general a predictor for higher behavioral or emotional problems. Being in minority is surely a great challenge for all migrant children. Netherland measures confirmed the dependence of the membership of a minority in increasing externalizing symptoms in school classes. In reverse, when there was a high ethnic density in classes, the authors detected that also native Dutch children had higher problem behavior if they were in minority [28]. However, several studies showed [27, 61, 68] that personal migration in childhood may be a great challenge in development, increasing the danger of generating mental disorders. In these results higher prevalence rates are obvious in emotional and behavioral problems in first generation immigrated children in comparison to second generation migrants. Nevertheless, these results could not be generalized because other studies found no differences between generations [25, 38, 48]. Only one study analyzing selection topics of migration was found [18]: Turkish migrants were more vulnerable in mental health if they migrate to Europe than otherwise migrant children in Turkey. Concurrently it could be demonstrated that Turkish children are not in general more prevalent in mental disorders because the non-migrant Turkish subsample had fewer externalizing and internalizing problems in comparison to all migrant groups. These results indicate that migration itself may function as risk factor, meaning that cross-cultural differences are not the reason for different prevalence rates in mental health in general. In contrast to these results, many studies compare the native and migrant group without ethnic differentiation and have no consistent results [10, 19, 20, 28, 35–37, 40, 45, 47, 59, 62, 76, 77]. The migration group in general is in consequence as different as the native group and migration itself does not necessarily function as risk factor.
Important symptoms in migrant children
It could be proved that migrant children and adolescents in Europe have in tendency many more internalizing problems such as depression or anxiety. Furthermore, one Belgian study was able to show that the migrant group had more traumatic stress, problems with peers and avoidance symptoms [20].
Higher foreignness leads to higher prevalence rates in problem behavior
Other studies in European countries in ethnic minority perspectives showed that especially non-European migrants had a disadvantage in mental health compared with European migrant or native children and adolescents [16, 41, 58]. These migrant children seemed to be more foreign than other European migrant groups and these non-European children populations are accompanied by higher problem behavior. Additionally, a study with black subsample groups [24] substantiate that the black origin can build a risk factor in children’s development.
Ethnic groups varied in mental health in Europe
In the distinction between native and migrant groups, the ethnic differentiation has in consequence more valid results. These results could point out that high variations with regard to ethnic origins exist. Especially the Dutch and British studies differ in ethnic origin. Turkish migrant children often showed more problem behavior in European countries, particularly in externalizing problem behavior [18, 70, 72, 73]. In contrast to this, Zwirs et al. [79] found a tendency towards lower prevalence rates of mental disorders in Turkish migrant children. Moroccan migrant children in the Netherlands tend to have less psychiatric symptoms in comparison with native Dutch or other analyzed ethnic migrant groups [11, 75], but even in this ethnic group the findings are not to be generalized [79]. Additionally, other analyzed ethnic groups varied similar to previous differences in other measures [5, 24, 30, 54]. Apart from migration aspects, the cross-cultural perspective is also not sufficient to explain mental disorders of migrant children in Europe.
Strong influence factors
In addition to cross-cultural differences and migration reasons, results of the present review indicate that other aspects influence at least or even more strongly mental health in migrant children and adolescents in Europe. Similar to native children, environmental risk factors as actual living situation, family situation and family’s functioning, socioeconomic status and educational level of parents are further reasons for mental disorders. However, in addition, special aspects are relevant for mental health of migrant children. If parents do not have a clear cultural identity, either from their host or origin country, this may affect mental health in migrant children negatively. Furthermore, development tasks such as the integration in a peer group (with sometimes low host language capabilities), or forming a personal identity in adolescence, are special challenges for migrant children. Discrimination or bullying of migrants may additionally increase the risk of mental problems.
Finally, based on all results of the present review, it can be noted that in general migrant children do not have a higher prevalence in mental disorders. Many special further factors in their living environment can influence their mental health in a negative way. These further challenges and efforts in European societies in migrant childhood development are not to be underestimated and kept in mind in psychiatric work. It should be noted, however, that the risk of higher prevalence in migrant children does not consequently result, as often discussed, in higher aggressive behavior. Especially notable is the danger of internalizing problems as depression or anxiety for migrant children and adolescents in Europe. However, as a future direction it should be noted that there is still a strong demand for further analysis in migrant children. Many countries, e.g. Germany, have to take a closer look at different ethnic groups in their migrant children and adolescents. If there is a correlation between ethnic origin and the type of mental disorder this has to be tested more extensively.
Limitations
In the previous discussion the present situation in mental health in migrant children of many European countries could be pointed out. It could be demonstrated that there are often not only huge differences in emotional and behavioral problems in migrant childhood in comparison with native children, but also parallels in several results. However, these results focus on internalizing and externalizing behavior in many, but not all European countries. We did not find any studies in fulfilling the listed criteria from Finland, Denmark, Luxembourg, Greece, Spain, Portugal and Eastern Europe or in countries of former Yugoslavia. The situation of migrant children in the included countries is probably not comparable with those in other countries. Furthermore, a lower interest of these countries in their migrant children is possible. It thus remains unclear whether the results in this review are comparable to other European countries or not. In the present studies, problem behavior was measured by valid and reliable questionnaires. It also remains unclear whether the understanding and interpretation of mental health of all children in the different ethnic groups is covered. The SDQ [29], for example, is often utilized in many studies. Cross-cultural differences of measures in SDQ-structures suggest that a measurement of mental disorders in different ethnic groups is more valid if only the total problem score is interpreted, not the subscale scores [56]. Particularly, the language capability is mostly not evaluated in included studies. In consequence it remains unclear if children or their parents always understand the items adequately. The different ethnic understanding of diseases may also be evaluated to understand the information given correctly. Further migrant studies should take these aspects into account to assess the mental condition of migrants more reliably. This review focused on the comparison between migrant and native children. It has to be evaluated if these reflections are sufficient. In a detailed analysis in one specific ethnic group, more relevant factors in migrant children’s health may become apparent. In addition, only a limited choice of all possible mental disorders could be analyzed. There also may be more than internalizing and externalizing classical disorders or unhealthy behavior such as psychoses, alcohol abuse or personality disorders which are not included in the present review. Furthermore, many children immigrated in acute danger situations due to refugee experiences. Almost all studies do not differ in labour and refugee migrants. The validity in refugee migrant children problems might not be similar to other children’s problems. Whether the analyzed studies included refugee children in their sample was mostly not reported; therefore, the declaration of migrant children’s mental health remains vague.
References
Achenbach TM (1991) Manual for the child behavior checklist/4–18 and 1991 profiles. University of Vermont Department of Psychiatry, Burlington
Achenbach TM (1991) Manual for the youth self report and 1991 profiles. University of Vermont Department of Psychiatry, Burlington
Aman MG, Tasse MJ, Rojahn J, Hammer D (1996) The Nisonger CBRF: a child behavior rating form for children with development disabilities. Res Dev Disabil 17:41–57
Arbeitsgruppe Deutsche Child behavior Checklist (2000) Elternfragebogen über das Verhalten von Klein- und Vorschulkindern (CBCL 1½–5). Arbeitsgruppe Kinder- und Jugenddiagnostik (KJFD), Köln
Atzaba-Poria N, Pike A (2007) Are ethnic minority adolescents at risk for problem behaviour? Acculturation and intergenerational acculturation discrepancies in early adolescence. Brit J Dev Psychol 25:527–541
Baier D, Pfeiffer C (2007) Gewalttätigkeit bei deutschen und nichtdeutschen Jugendlichen: Befunde aus der Schülerbefragung 2005 und Folgerungen für die Prävention. Kriminologisches Forschungsinstitut Niedersachsen, Hannover
Baier D, Pfeiffer C, Simonson J, Rabold S, Kappes C (2010) Kinder und Jugendliche in Deutschland: Gewalterfahrungen, Integration, Medienkonsum, Zweiter Bericht zum gemeinsamen Forschungsprojekt des Bundesministeriums des Innern und des KFN. Kriminologisches Forschungsinstitut Niedersachsen, Hannover
Bean T, Eurelings-Bontekoe EHM, Derluyn I, Spinhoven PH (2004) Stressful life events (SLE). User’s manual. Stichting Centrum, Oestgeest
Bean T, Eurelings-Bontekoe EHM, Derluyn I, Spinhoven PH (2004) Reactions of adolescents to traumatic stress questionnaire (RATS). User’s manual. Stichting Centrum, Oestgeest
Belhadj Kouider E, Koglin U, Lorenz AL, Dupont M, Petermann F (2013) Conduct disorders in adolescents with immigrant background. Kindh Entwickl 22:113–122
Bevaart F, Mieloo CL, Jansen W, Raat H, Donker MCH, Verhulst FC, van Oort FVA (2012) Ethnic differences in problem perception and perceived need for young children with problem behaviour. J Child Psychol Psyc 53:1063–1071
Bornstein MH, Cote LR (2009) Child temperament in three US cultural groups. Inf Mental Hlth J 30:433–451
Carbello M, Nerukar A (2001) Migration, refugees, and health risks. Emerg Infect Dis 7:556–560
Carlerby H, Viitasara E, Knutsson A, Gillander Gadin K (2011) Subjective health complaints among boys and girls in the Swedish HBSC study: focussing on parental foreign background. Int J Public Health 56:457–464
Centre for Reviews and Dissemination (2009) Systematic Reviews: CRD’s guidance for undertaking reviews in health care. University of York, York
Chau K, Baumann M, Kabuth B, Chau N (2012) School difficulties in immigrant adolescent students and roles of socioeconomic factors, unhealthy behaviours, and physical and mental health. BMC Public Health 12:453–466
Clauss S, Nauck B (2009) The situation among children of migrant origin in Germany. United Nations Children’s Fund (UNICEF): Innocenti Research Centre
Daglar M, Melhuish E, Barnes J (2011) Parenting and preschool child behaviour among Turkish immigrant, migrant and non-migrant families. Eur J Dev Psychol 8:261–279
Dekeyser L, Svedin CG, Agnaförs S, Sysdjö G (2011) Self-reported mental health in 12-year-old second-generation immigrant children in Sweden. Nord J Psychiat 65:389–395
Derluyn I, Broekaert E, Schuyten G (2008) Emotional and behavioural problems in migrant adolescents in Belgium. Eur Child Adoles Psy 17:54–62
Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L (1974) The Hopkins symptom checklist (HSCL): a self-report symptom inventory. Behav Sci 19:1–15
De Wit C (1987) Depressive Vragenlijst voor Kinderen, DVK en KDVK: Handleiding [manual of the (short) depression inventory for children]. Acco, Amersfoort/Leuven
El-Mafaalani A, Toprak A (2011) Muslimische Kinder und Jugendliche in Deutschland. Eine Veröffentlichung der Konrad-Adenauer Stiftung e.V Pfaffenholz GmbH, Bornheim
Emerson E, Robertson J, Wood J (2007) The association between area-level indicators of social deprivation and the emotional and behavioural needs of black and south Asian children with intellectual disabilities in a deprived urban environment. J Appl Res Intellect Disabil 20:420–429
Fandrem H, Sam DL, Roland E (2009) Depressive symptoms among native and immigrant adolescents in Norway: the role of gender and urbanization. Soc Indic Res 92:91–109
Fisher P, Lucas L (2003) Diagnostic Interview Schedule for Children (DISC): an introduction and applications. Seventh annual conference of the society for social work and research, Washington
Flink IJE, Jansen PW, Beirens TMJ, Tiemeier H, van Ijzendoorn MH, Jaddoe VWV, Hofmann A, Raat H (2012) Differences in problem behaviour among ethnic minority and majority preschoolers in the Netherlands and the role of family functioning and parenting factors as mediators: the Generation R Study. BMC Public Health 12:1092
Gieling M, Vollebergh W, van Dorsselaer S (2010) Ethnic density in school classes and adolescent mental health. Soc Psychiat Epidemiol 45:639–646
Goodman R (1997) The strengths and difficulties questionnaire: a research note. J Child Psychol Psyc 38:581–586
Goodman A, Patel V, Leon DA (2010) Why do british Indian children have an apparant mental health advantage? J Child Psychol Psyc 51:1171–1183
Hahn A, Neubauer BA (2005) Autism and metabolic disorders: a rational approach. Z Kinder Jug-Psych 33:259–271
Hare RD (1991) The Hare-Psychopathy checklist-revised. Multi-Health Systems, Toronto
Heiervang E, Goodman A, Goodman R (2008) The nordic advantage in child mental health: separating health differences from reporting style in a cross-cultural comparison of psychopathology. J Child Psychol Psyc 49:678–685
Hernandez DJ (2010) Internationally comparable indicators for children of immigrants. Child Indic Res 3:409–411
Hölling H, Erhart M, Ravens-Sieberer U, Schlack R (2007) Verhaltensauffälligkeiten bei Kindern und Jugendlichen. Erste Ergebnisse aus dem Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundhbl Gesundh Gesundh 50:784–793
Hornsfeld RHJ, Cuperus H, De Vries ET, Kraaimaat W (2008) An evaluation of behavioural and personality differences between native and non-native adolescents in the Netherlands ordered into treatment in a forensic psychiatric outpatient clinic, and their non-violent peers. Crim Behav Mental Health 18:177–189
Hüsler G, Plancherel B (2007) Social integration of adolescents at risk: results from a cohort study. Vuln Child Youth Stud 2:215–226
Hüsler G, Werlen E (2010) Swiss and migrant adolescents: similarities and differences. Vuln Children Youth Stud 5:244–255
ICD-10: International Statistical Classification of Diseases and Health Related Problems (1994) Tenth Revision (ICD-10), vol III. Alphabetical Index, World Health Organisation
Jackson M, Kiernan K, McLanahan S (2011) Immigrant-native differences in child health: does maternal education narrow or widen the gap?. Princeton University, Mimeo
Jansen PW, Raat H, Mackenbach JP, Jaddoe VWV, Hofman A, van Oort F, Verhulst FC, Tiemeier H (2010) National origin and behavioural problems of toddlers: the role of family risk factors and maternal immigration characteristics. J Abnorm Child Psych 38:1151–1164
Jäkel J, Leyendecker B (2009) Parenting of Turkish migrant and German mothers with preschool children. Psych Erz Unterr 56:1–15
Kirkcaldy B, Wittig U, Furnham A, Merbach M, Siefen RG (2006) Migration und Gesundheit. Bundesgesundhbl Gesundh Gesundh 49:873–883
Kobelt A, Göbber J, Petermann F (2011) Needs in rehabilitation and rehabilitative care of new target groups. Immigrants in psychosomatic rehabilitation. Bundesgesundhbl 54:475–481
Kuschel A, Heinrichs N, Bertram H, Naumann S, Hahlweg K (2008) Emotional and behavioral disorders of kindergarten children from parents’ and teachers’ perspectives in dependency on demographic characteristics. Kindh Entwickl 17:161–172
Ladd GW, Profilet SM (1996) Child behavior scale: a teacher-report measure of young children’s aggressive, withdrawn and prosocial behaviours. Dev Psychol 32:1008–1024
Lien L (2008) The association between mental health problems and inflammatory conditions across gender and immigrant status: a population-based cross-sectional study among 10th-grade students. Scand J Public Healt 36:353–360
Margari L, Pinto F, Lafortezza ME, Lecce PA, Craig F, Grattagliano I, Zagaria G, Margari F (2013) Mental health in migrant schoolchildren in Italy: teacher-reported behavior and emotional problems. Neuropsyc Dis Treat 9:231–241
McConaughy SH, Achenbach TM (2001) Manual for the semistructured clinical interview for children and adolescents. University of Vermont, Burlington
Merrell KW (1994) Preschool and kindergarten behavior scales. PRO-ED, Austin
Montgomery E, Foldspang A (2008) Discrimination, mental problems and social adaption in young refugees. Euro J Public Health 18:156–161
Petermann F, Koglin U (2008) Early childhood. Kindh Entwickl 17:137–142
Petermann F, Noeker M (2008) Developmental psychopathology. ZKPPP 56:239–241
Prady SL, Kiernan KE (2012) The effect of post-natal mental distress amongst Indian and Pakistani mothers living in England on children’s behavioural outcomes. Child Care Hlth Dev 39(5):710–721
Ravens-Sieberer U, Bullinger M (2000) KINDL-R. Ein Fragebogen zur Erfassung der gesundheitsbezogenen Lebensqualität von Kindern. Unveröffentlichtes Manuskript, Universitätsklinikum Eppendorf, Hamburg
Richter J, Sagatun A, Heyerdahl S, Oppedal B, Roysamb E (2011) The strengths and difficulties questionnaire (SDQ): self report. An analysis of its structure in a multiethnic urban adolescent sample. J Child Psychol Psyc 52:1002–1011
Robinson CC, Mandleco B, Olsen SF, Hart CH (2001) The parenting styles and dimensions questionnaire (PSDQ). In: Perlmutter BF, Touliatos J, Holden GW (eds) Handbook of family measurement techniques, Instruments & index, vol 3. Sage, Thousand Oaks, pp 319–321
Rydell AM (2010) Family factors and children’s disruptive behaviour: an investigation of links between demographic characteristics, negative life events and symptoms of ODD and ADHD. Soc Psych Epidem 45:233–244
Sagatun A, Lien L, Sogaard AJ, Bjertness E, Heyerdahl S (2008) Ethnic Norwegian and ethnic minority adolescents in Oslo, Norway: a longitudinal study comparing changes in mental health. Soc Psych Psych Epidem 43:87–95
Schenk L, Ellert U, Neuhauser H (2007) Kinder und Jugendliche mit Migrationshintergrund in Deutschland. Methodische Aspekte im Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundhbl Gesundh Gesundh 50:590–599
Schmitt-Rodermund E, Silbereisen RK (2008) The prediction of delinquency among immigrant and non-immigrant youth: unwrapping the package of culture. Int J Comp Soc 49:87–109
Schreyer I, Petermann U (2010) Behavior problems and quality of life in preschool children and their mothers: comparing native children and children of immigrant families. Z Gesundhe 18:119–129
Schulte-Körne G, Warnke A, Remschmidt H (2006) Genetics of dyslexia. Z Kinder Jug-Psych 34:435–444
Shaffer D, Fisher P, Lucas CP, Duldan MK, Schwab-Stone ME (2000) NIMH diagnostic interview schedule for children version 2.3 (DISC-2.3). J Am Acad Child Adolesc Psychiatry 39:28–38
Skevington SM, Lotfy M, O’Connell KA (2004) The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WOQOL group. Qual Life Res 13:229–310
Statistisches Bundesamt (2013). Personen mit Migrationshintergrund. https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/Bevoelkerung/MigrationIntegration/Migrationshintergrund/Aktuell.html. Accessed 25 January 2013
Statistisches Bundesamt (2012) Bevölkerung und Erwerbstätigkeit. Bevölkerung mit Migrationshintergrund: Ergebnisse des Mikrozensus 2011. Statistisches Bundesamt, Wiesbaden
Steinhausen HC, Bearth-Carrari C, Winkler Metzke C (2009) Psychosocial adaption of adolescent migrants in a Swiss community survey. Soc Psych Psych Epidem 44:308–316
Stevens GWJM, Vollebergh WAM (2008) Mental health in migrant children. J Child Psychol Psyc 49:276–294
Van de Looji-Jansen PM, Jansen W, de Wilde EJ, Donker MCH, Verhulst FC (2011) Discrepancies between parent-child reports internalizing problems among preadolescent children: relationships with gender, ethnic background, and future internalizing problems. J Early Adolesc 31:443–462
Van der Ploeg HM, Defares PB, Spielberger CD (1982) Handleiding bij de Zelf-Analyse Vragenlijst, ZAV [manual for the self-analysis questionnaire, ZAV]. Swets & Zeitlinger, Lisse
Van Oort FVA, Joung IMA, Mackenbach JP, Verhulst FC, Bengi-Arslan L, Crijnen AAM, van der Ende J (2007) Development of ethnic disparities in internalizing and externalizing problems from adolescence into young adulthood. J Child Psychol Psyc 48:176–184
Van Oort FVA, van der Ende J, Crijnen AAM, Verhulst FC, Mackenbach JP, Joung IMA (2007) Ethnic disparities in mental health and educational attainment: comparing migrant and native children. Int J Soc Psychiatr 53:514–525
Vasileva K (2011) Population and social conditions. Eurstat Stat Focus 34:1–8
Veen VC, Stevens GWJM, Doreleijers TAH, van der Ende J, Vollebergh WAM (2010) Ethnic differences in mental health among incarcerated youths: do Moroccan immigrant boys show less psychopathology than native Dutch boys? Eur Child Adolesc Psy 19:431–440
Vieno A, Santinello M, Lenzi M, Baldarassi D, Mirandola M (2009) Health status in immigrants and native early adolescents in Italy. J Commun Health 34:181–187
Washbrook E, Waldfogel J, Bradbury B, Corak M, Ghangro AA (2012) The development of young children of immigrants in Australia, Canada, the United Kingdom, and the United States. Child Dev 83:1591–1607
WHO International Consortium in Psychiatric Epidemiology (2000) Cross-national comparisons of the prevalences and correlates of mental disorders. Bull World Health Organ 78:413–426
Zwirs BWC, Burger H, Schulpen TWJ, Witznitzer M, Fedder H, Buitelaar JK (2007) Prevalence of psychiatric disorders among children of different ethnic origin. J Abnorm Child Psych 35:556–566
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Belhadj Kouider, E., Koglin, U. & Petermann, F. Emotional and behavioral problems in migrant children and adolescents in Europe: a systematic review. Eur Child Adolesc Psychiatry 23, 373–391 (2014). https://doi.org/10.1007/s00787-013-0485-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-013-0485-8