
Abstract
Purpose of Review
The purpose of this scoping literature review was to summarize the current evidence on techniques and outcomes following MPFL reconstruction including sources of evidence, key concepts, and gaps in the literature.
Recent Findings
A thorough electronic database search included studies published from 2016 to April 26, 2021, identified a total of 144 peer reviewed articles. Of the 144 identified clinical papers, 80 (56%) were of level IV evidence, 49 (34%) were of level III evidence, 11 (8%) were level II evidence, and 4 (3%) were level I evidence. Overall, 10,710 patients (11,466 knees) were included with 6871 (64%) female. The mean age of patients included in these studies was 23.5 years (range=5 to 59).
Summary
In recent years, there has been a substantial quantity of evidence published on MPFL reconstruction from a variety of different countries and journals and of variable methodological design. Isolated MPFL reconstruction results in a decrease in patellar height postoperatively. Indications for isolated MPFL reconstruction versus concomitant procedures to address bony morphology is still incompletely defined. When failure does occur after MPFL reconstruction, femoral tunnel malposition is the most commonly cited cause. Despite several recent studies focused on optimal MPFL reconstruction techniques, there is currently no consensus on optimal graft type (most common being hamstring autografts, allografts, and recently synthetic grafts) or femoral fixation strategies, with similar results reported with each technique. Future studies should focus on optimal techniques for each patient population as well as specific indications for additional concomitant realignment procedures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Patellar instability is a common problem affecting adolescents and young adults. Population-based studies have estimated that patellar dislocations occur with an incidence of 23 per 100,000 person-years, with the most common ages of dislocation being those between 14 and 18 years [1]. Although the standard of care for most first-time patellar dislocations involves nonoperative management with rest and rehabilitation [2, 3], patellar dislocations can result in articular cartilage injuries, osteochondral fractures, and recurrent instability [4, 5]. Success after nonoperative treatment of first-time dislocation varies with recurrence rates between 15% and 80% previously reported [4, 6]. The medial patellofemoral ligament (MPFL) is the most commonly injured soft tissue structure following lateral patellar dislocations, having shown to occur in more than 90% of individuals having acute patellar dislocations [7].
Indications for surgical intervention include recurrent patellar instability with failure to improve after a trial of nonoperative management, as well as the presence of unstable osteochondral fractures or loose bodies [2, 3]. Surgical management includes medial patellofemoral ligament (MPFL) reconstruction alone or in combination with other procedures such as a lateral retinacular release, tibial tubercle osteotomy (TTO), or trochleoplasty [8]. Recent literature has aimed to determine the optimal surgical management for patients with and without concurrent osseous anatomical risk factors such as patella alta, abnormal tibial tubercle–trochlear groove (TT-TG) distance, trochlear dysplasia, and patellar tilt [9,10,11]. Furthermore, several debates in the recent literature pertain to the optimal tunnel location, graft fixation angle, and graft tension in order to optimize outcomes and prevent graft failure [12].
The purpose of this scoping literature review was to summarize the current evidence on techniques and outcomes following MPFL reconstruction including sources of evidence, key concepts, and gaps in the literature.
Anatomy and Biomechanics
The patella is most prone to dislocation in 0–30° of knee flexion, prior to engagement within the femoral trochlear groove, where the MPFL functions as the primary restraint to lateral patellar subluxation [13]. In order to preserve the native biomechanics of the patellofemoral joint, it has been suggested that after MPFL reconstruction, the graft should be tightest in extension to prevent recurrent dislocation, and isometric from 0 to 30° of knee flexion [14]. The origin of the MPFL is on the femur between the adductor tubercle and the medial epicondyle and inserts at the proximal third of the medial patella [15]. Schöttle et al. first described the radiographic landmarks for anatomic femoral tunnel placement (now commonly referred to as Schöttle’s point). On a true lateral radiograph, the point is located one millimeter anterior to a tangent line to the posterior femoral cortex, proximal to the most posterior part of Blumensaat’s line, and 2.5 mm distal to the posterior origin of the medial femoral condyle (Fig. 1). However, this anatomic femoral insertion site is not identical in every individual and can vary by as much as 5mm [16].

Lateral radiograph depicting the anatomic femoral tunnel placement site as per Schöttle et al. (blue circle). The blue lines represent the tangent line to the posterior femoral cortex, as well as two perpendicular lines at the most posterior part of Blumensaat’s line, and at the posterior origin of the medial femoral condyle, respectively
The importance of anatomical graft placement has been reported in several studies, as non-anatomic placement on the femoral side can cause recurrent instability or increased medial patellofemoral contact pressures and overloading the medial cartilage leading to premature degenerative changes [15, 17]. Malpositioning of the femoral tunnel has been reported to be the most common indication for MPFL reconstruction failure requiring revision surgery, occurring up to 40% of the time [18]. A femoral tunnel that is malpositioned too anterior, in particular, has been shown to lead to overloading of the medial patellofemoral cartilage [17]. A femoral tunnel that is malpositioned too proximally leads to a graft that is too lax in extension, and too tight in flexion. Conversely, a femoral tunnel that is too distal leads to an overtight graft in extension, and an excessively lax graft in flexion, leading to a clinical extension lag [19].
State of the Current Evidence
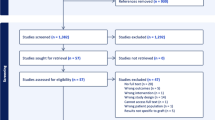
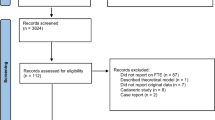
A thorough search of 3 electronic databases (MEDLINE, Embase, and PubMed) identified all studies published over the past 5 years (2016 to April 26, 2021) on techniques and outcomes following MPFL reconstruction. A total of 144 peer reviewed articles were identified. Of these studies, 26 (18%) were conducted in China, 24 (17%) in the USA, 15 (10%) in Germany, 12 (8%) in Japan, and 8 (6%) in each of Canada, the UK, and Brazil. The most common journals of publication were Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA) (41 studies, 28%), Orthopaedic Journal of Sports Medicine (OJSM) (15 studies, 10%), The American Journal of Sports Medicine (AJSM) (13 studies, 9%), and Arthroscopy (9 studies, 6%).
Of the 144 clinical studies, 80 (56%) were of level IV evidence, 49 (34%) were of level III evidence, 11 (8%) were level II evidence, and 4 (3%) were level I evidence (high quality RCT with >80% follow-up) (Fig. 2). Ninety percent (129 studies) employed methodology using a retrospective design, 6% (9 studies) used a prospective, non-randomized design, while 4% (6 studies) were randomized controlled trials (RCTs). Overall, 10,710 patients (11,466 knees) were included with 6871 (64%) female. The mean age of patients included in these studies was 23.5 years (range, 5 to 59 years) and the mean follow-up across the studies was 35.6 months. An isolated MPFL reconstruction was performed in 83 studies (58%), MPFL reconstruction combined with a tibial tubercle osteotomy (TTO) in 20 studies (14%), and in combination with trochleoplasty in 13 studies (9%).

Number of publications on MPFL reconstruction by year and level of evidence
Key Literature
Postoperative Patellar Height
Luceri et al. assessed 89 patients who had undergone isolated MPFL reconstruction using hamstring autografts and found that patellar height was significantly reduced after surgery from a mean Caton-Deschamps (CD) ratio of 1.19 to a mean post-operative CD ratio of 0.99 (mean reduction of CD of 0.19, P<0.0001). Of 35.8% of cases that had patella alta pre-operatively, 79.4% of these patients had a reduction of patellar height 18-months post-operatively to within normal limits [20].
Similar findings were reported by Hiemstra et al. after isolated MPFL reconstruction in 283 patients, where the Caton-Deschamps (CD) ratio was significantly reduced (CD reduction of 0.03, p<0.001) across the entire cohort postoperatively, with a larger effect size (CD reduction of 0.10, p<0.001) in those who had preoperative patellar alta (CD>1.2) [21].
Impact of Patellar Height and Trochlear Dysplasia
A study of 90 patients undergoing isolated MPFL reconstruction regardless of concomitant bony pathology such as TT-TG distance, patellar height, and trochlear depth, reported strong clinical and functional outcomes at 2 years with 0 failures, 88% rate of return to sport, and significantly improved Knee injury and Osteoarthritis Outcome Score–Quality of Life (32.7 to 72.0, P < .001) [11]. Similarly, Blake et al. retrospectively assessed 52 patients who had undergone isolated MPFL reconstruction regardless of concomitant bony pathology and reported strong functional outcomes. There was no significant correlation between the functional outcome scores (Lysholm and Tegner) and the anatomic risk factors [22].
In contrast, a retrospective analysis of 211 isolated MPFL reconstructions at a mean follow-up of 5.8 years found that pre-operative patella alta (CDI ≥1.3) was associated with a higher risk of failure postoperatively (odds ratio, 4.9; P = .02) [23]. However, another study assessing 121 patients without significantly elevated TT-TG distances or significant patella alta found that isolated MPFL reconstruction, even in patients with trochlear dysplasia, resulted in significant improvements in Kujala score (55.0 preoperatively to 90.0, P < .001), with most patients (94.5%) able to return to sports at 1 year [24].
Impact of Femoral Version
Zhang et al. retrospectively assessed 66 patients who had undergone MPFL reconstruction with a concomitant TTO for the prognosticative impact of femoral version on postoperative outcomes. The study found that patients with femoral anteversion > 30 degrees (mean +/- SD age 19.4 +/- 4.4 years) had significantly worse Kujala (75 ± 8 vs. 84 ± 8, P = 0.003), Lysholm (81 ± 9 vs. 87 ± 7, P = 0.021), and IKDC scores (78 ± 6 vs. 85 ± 7, P = 0.001) compared to patients (mean +/- SD age 19.8 +/- 6.2 years) with femoral anteversion < 20 degrees [25].
The same group subsequently reported on 126 patients with increased femoral anteversion undergoing either MPFL reconstruction with or without a derotational distal femoral osteotomy. The derotational distal femoral osteotomy group had significantly higher Kujala (82.3 vs 76.7; P = .001) and Lysholm (83.7 vs 77.7; P = .034) scores post-operatively [26•].
Additional Soft Tissue Procedures
An RCT of 43 patients by Malatray et al. compared isolated MPFL reconstruction with MPFL reconstruction in addition to arthroscopic lateral retinacular release. The study found no significant difference in mean +/- SD post-operative subjective IKDC scores (82 +/- 15 vs. 86 +/-20, P=0.45) or patellar tilt at 24 months post-operative between groups [27••].
Predictors of Outcomes
Hiemstra et al. assessed 224 patients who had undergone isolated MPFL reconstruction for risk factors that predict lower patient reported outcomes using a multivariable regression model. The study found that bilateral symptoms (P = .004), older age at first dislocation (P = .024), and femoral tunnel position malposition (P = .042) were significant predictors of lower Banff Patellofemoral Instability Instrument (BPII) scores [28•].
Another study by Neri et al. assessed 107 patients undergoing isolated MPFL reconstruction and found that only malpositioning of the femoral tunnel (p=0.002), and a larger (>20 degrees) residual patellar tilt (P=0.009), were associated with lower functional outcomes [29].
Zhang et al. similarly reported that in 312 patients undergoing MPFL reconstruction, only a high-grade preoperative J-sign (odds ratio, 11.9 [95% CI, 1.7–82.8]; P = 0.012) and femoral tunnel malposition (odds ratio, 8.2 [95% CI, 1.2–58.0]; P = 0.036) were independently predictive of residual graft laxity postoperatively [30].
Graft Type
Kumar et al. evaluated fifty-nine adolescents under age 18 in a retrospective study following MPFL reconstruction with either hamstring autograft or hamstring allografts. No significant differences were noted in rates of return to sport or rates of failure (3 of 36 in allograft group vs. 6 of 23 in autograft group, p=0.064) between the two groups [31]. Flanigan et al. similarly retrospectively assessed 115 patients undergoing MPFL reconstruction with either hamstring autografts or allografts. The study found no significant difference in the rate of recurrent dislocation (3.3% vs. 3.5%) or patient reported outcomes between groups [32•].
Another prospective study of 50 patients undergoing MPFL reconstruction compared the use of gracilis tendon autograft to a synthetic graft of modern ultra-high molecular weight polyethylene with a braided jacket of polyester tape. They reported significant improvements in knee function scores in both groups, with no significant difference in knee functional outcomes (Kujala, Bartlett, Tegner, Lysholm scores) between the two groups [33].
Graft Fixation
Lind et al. assessed 60 patients in a prospective RCT comparing two femoral fixation strategies. The bone femoral fixation technique used an interference screw in the femur, while the soft-tissue fixation technique looped the graft around the adductor magnus tendon. The study found no difference in outcomes between the two groups, with similar postoperative Kujala scores (89 vs. 88, P=0.73), fixation site morbidity (12% vs. 13%) and re-dislocation rates (0%) [34••].
MPFL Reconstruction in Adolescents
Malecki et al. assessed 65 patients with a median age of 14 years and compared two surgical techniques for recurrent patellar dislocation. The first technique involved MPFL reconstruction using the adductor magnus tendon, whereby the distal insertion on the femur is left intact, and the harvested tendon is attached to its anatomic footprint on the patella The second technique utilized a retinacular plasty including a lateral release, vastus medialis advancement, as well as a Roux Goldthwait procedure involving a medial transfer of the lateral patellar tendon. Although the rate of recurrent dislocation, and functional outcomes (Lysholm and Kujala scores) were similar between the two groups, the proportion of patients with continued pain was significantly higher in the soft tissue proximal and distal realignment group (24/33, 73%), than in the MPFL reconstruction group (13/32, 41%) (P<0.01) [35].
Another study by Nelitz et al. described a technique for MPFL reconstruction in 25 skeletally immature patients with a mean age of 12.8 years using a pedicled quadriceps autograft. The technique keeps the patellar attachment of the quadriceps graft intact, with the femoral attachment site verified on anteroposterior and true lateral planes with fluoroscopy to ensure it is truly distal to the physis. The authors have previously described that lateral radiographs can be misleading on their own in determining the position of the distal femoral physis in relation to the MPFL given the curvature of the physis [36]. The authors also advocate angling the guide wire 15-20 degrees distally and anteriorly to minimize damage to the physis and cartilage. The graft was secured to the femur with a bioresorbable interference screw. Promising outcomes were reported at 2 years, with no patients having recurrent instability, strong Kujala and Tegner scores, and 21/25 (84%) returning to sport at their previous level. There were no complications reported by the authors [37].
Lafave et al. found that the Banff Patellofemoral Instability Instrument 2.0 (BPII 2.0) was valid, reliable and disease specific within the adolescent population for lateral patellofemoral instability in a multicentered study of 140 adolescent patients. Two other scores that have been previously validated in the adolescent population include the Pediatric International Knee Documentation Committee (Pedi-IKDC) [38], as well as the original BPII [39, 40]. Other commonly used scores including the Kujala score, and the Norwich Patellar Instability Score have not been validated for use in the adolescent population [39].
Conclusion
In recent years, there has been a substantial quantity of evidence published on MPFL reconstruction from a variety of different countries and journals and of variable methodological design and levels of evidence. Although the clinical implications are not fully understood, it has been demonstrated that isolated MPFL reconstruction results in a decrease in patellar height postoperatively. Overall, the promising results reported after isolated MPFL reconstruction in recent years suggest that not all patients with bony pathology require additional surgical correction beyond isolated MPFL reconstruction. However, some studies have shown that substantial patella alta or femoral anteversion preoperatively is associated with a higher risk of failure after isolated MPFL reconstruction. Patients with significant femoral anteversion may benefit from consideration of concomitant derotational femoral osteotomy. When failure does occur after MPFL reconstruction, femoral tunnel malposition is the most commonly cited cause. Despite several recent studies focused on optimal MPFL reconstruction techniques, there is currently no consensus on optimal graft type or femoral fixation strategies, with similar results reported with each technique. The most commonly used graft types are hamstring autografts, hamstring allografts, and, more recently, synthetic grafts. Our recommendations based on the current literature are for patients with recurrent patellar dislocations to have a thorough clinical and radiographic assessment for the presence of significant osseous pathology that may be contributing as an underlying cause to patellar dislocations. In the absence of clear osseous pathology, or those with minor abnormalities, isolated MPFL reconstruction can be performed with either autograft or allograft with particular attention to ensure that the femoral tunnel is positioned appropriately. Concomitant soft tissue procedures are rarely required. In adolescents and those skeletally immature, alternative procedures could be considered including the use of adductor magnus or quadriceps autografts whereby the attachment to the femur or patella are left intact. Given the gaps identified within the literature thus far, future studies should focus on specific indications for when additional realignment procedures are needed concomitantly with MPFL reconstruction. Furthermore, future prospective studies would be useful to clarify patient populations (such as those who are young and active) that may benefit from consideration of specific graft type or fixation techniques for MPFL reconstruction.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Sanders TL, Pareek A, Hewett TE, Stuart MJ, Dahm DL, Krych AJ. Incidence of First-Time Lateral Patellar Dislocation: A 21-Year Population-Based Study. Sport Heal A Multidiscip Approach. 2018;10:146–51.
Weber AE, Nathani A, Dines JS, Allen AA, Shubin-Stein BE, Arendt EA, Bedi A. An Algorithmic Approach to the Management of Recurrent Lateral Patellar Dislocation. J Bone Jt Surg. 2016;98:417–27.
Duerr RA, Chauhan A, Frank DA, DeMeo PJ, Akhavan S. An Algorithm for Diagnosing and Treating Primary and Recurrent Patellar Instability. JBJS Rev. 2016;4.
Fithian DC, Paxton EW, Lou SM, Silva P, Davis DK, Elias DA, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004.
Arendt EA, Fithian DC, Cohen E. Current concepts of lateral patella dislocation. Clin Sports Med. 2002;21:499–519.
Palmu S, Kallio PE, Donell ST, Helenius I, Nietosvaara Y. Acute patellar dislocation in children and adolescents: a randomized clinical trial. J Bone Joint Surg Am. 2008;90:463–70.
Nomura E, Horiuchi Y, Inoue M. Correlation of MR imaging findings and open exploration of medial patellofemoral ligament injuries in acute patellar dislocations. Knee. 2002;9:139–143.
Sherman SL, Erickson BJ, Cvetanovich GL, Chalmers PN, Farr J, Bach BR, et al. Tibial Tuberosity Osteotomy: Indications, Techniques, and Outcomes. Am J Sports Med. 2014;42:2006–17.
Clifton B, Richter DL, Tandberg D, Ferguson M, Treme G. Evaluation of the Tibial Tubercle to Posterior Cruciate Ligament Distance in a Pediatric Patient Population. J Pediatr Orthop. 2017;37:e388–93.
Askenberger M, Janarv P-M, Finnbogason T, Arendt EA. Morphology and Anatomic Patellar Instability Risk Factors in First-Time Traumatic Lateral Patellar Dislocations: A Prospective Magnetic Resonance Imaging Study in Skeletally Immature Children. Am J Sports Med. 2017;45:50–8.
Erickson BJ, Nguyen J, Gasik K, Gruber S, Brady J, Shubin Stein BE. Isolated Medial Patellofemoral Ligament Reconstruction for Patellar Instability Regardless of Tibial Tubercle–Trochlear Groove Distance and Patellar Height: Outcomes at 1 and 2 Years. Am J Sports Med. 2019;47:1331–7.
Patel NK, de Sa D, Vaswani R, Kay J, Musahl V, Lesniak BP. Knee Flexion Angle During Graft Fixation for Medial Patellofemoral Ligament Reconstruction: A Systematic Review of Outcomes and Complications. Arthroscopy. 2019;35:1893–904.
Warren LA, Marshall JL, Girgis F. The prime static stabilizer of the medical side of the knee. J Bone Joint Surg Am. 1974;56:665–74.
Thaunat M, Erasmus PJ. The favourable anisometry: An original concept for medial patellofemoral ligament reconstruction. Knee. 2007;14:424–8.
Steensen RN, Dopirak RM, McDonald WG. The anatomy and isometry of the medial patellofemoral ligament: implications for reconstruction. Am J Sports Med. 2004;32:1509–13.
Schöttle PB, Schmeling A, Rosenstiel N, Weiler A. Radiographic Landmarks for Femoral Tunnel Placement in Medial Patellofemoral Ligament Reconstruction. Am J Sports Med. 2007;35:801–4.
Bollier M, Fulkerson J, Cosgarea A, Tanaka M. Technical failure of medial patellofemoral ligament reconstruction. Arthroscopy. 2011;27:1153–9.
Walker M, Maini L, Kay J, Siddiqui A, Almasri M, de SA D. Femoral tunnel malposition is the most common indication for revision medial patellofemoral ligament reconstruction with promising early outcomes following revision reconstruction: a systematic review. Knee Surgery, Sport Traumatol Arthrosc. 2021. https://doi.org/10.1007/s00167-021-06603-x
Thaunat M, Erasmus PJ. Management of overtight medial patellofemoral ligament reconstruction. Knee Surgery, Sport Traumatol Arthrosc. 2009;17:480–3.
Luceri F, Roger J, Randelli PS, Lustig S, Servien E. How Does Isolated Medial Patellofemoral Ligament Reconstruction Influence Patellar Height? Am J Sports Med. 2020;48:895–900.
Hiemstra LA, Kerslake S, Lafave MR, Tucker A. Patella alta is reduced following MPFL reconstruction but has no effect on quality-of-life outcomes in patients with patellofemoral instability. Knee Surgery, Sport Traumatol Arthrosc. 2021;29:546–52.
Blanke F, Watermann K, Haenle M, Feitenhansl A, Camathias C, Vogt S. Isolated Medial Patellofemoral Ligament Reconstruction Can Be an Effective Procedure in Patellofemoral Instability with Risk Factors. J Knee Surg. 2020;33:992–7.
Sappey-Marinier E, Sonnery-Cottet B, O’Loughlin P, Ouanezar H, Reina Fernandes L, Kouevidjin B, Thaunat M. Clinical Outcomes and Predictive Factors for Failure With Isolated MPFL Reconstruction for Recurrent Patellar Instability: A Series of 211 Reconstructions With a Minimum Follow-up of 3 Years. Am J Sports Med. 2019;47:1323–30.
Liu JN, Brady JM, Kalbian IL, Strickland SM, Ryan CB, Nguyen JT, Shubin Stein BE. Clinical Outcomes After Isolated Medial Patellofemoral Ligament Reconstruction for Patellar Instability Among Patients With Trochlear Dysplasia. Am J Sports Med. 2018;46:883–9.
Zhang Z, Zhang H, Song G, Zheng T, Ni Q, Feng H. Increased femoral anteversion is associated with inferior clinical outcomes after MPFL reconstruction and combined tibial tubercle osteotomy for the treatment of recurrent patellar instability. Knee Surgery, Sport Traumatol Arthrosc. 2020;28:2261–9.
Zhang Z, Song G, Li Y, Zheng T, Ni Q, Feng H, et al. Medial Patellofemoral Ligament Reconstruction With or Without Derotational Distal Femoral Osteotomy in Treating Recurrent Patellar Dislocation With Increased Femoral Anteversion: A Retrospective Comparative Study. Am J Sports Med. 2021;49:200–6 The study assesses 126 patients with increased femoral anteversion undergoing either MPFL reconstruction with or without a derotational distal femoral osteotomy. The derotational distal femoral osteotomy group had significantly higher Kujala and Lysholm scores post-operatively.
Malatray M, Magnussen R, Lustig S, Servien E. Lateral retinacular release is not recommended in association to MPFL reconstruction in recurrent patellar dislocation. Knee Surgery, Sport Traumatol Arthrosc. 2019;27:2659–64 This prospective randomized study compares isolated MPFL reconstruction with MPFL reconstruction in addition to arthroscopic lateral retinacular release.
Hiemstra LA, Kerslake SA, Lafave MR. Influence of Risky Pathoanatomy and Demographic Factors on Clinical Outcomes After Isolated Medial Patellofemoral Ligament Reconstruction: A Regression Analysis. Am J Sports Med. 2019;47:2904–9 Using a multivariable regression model, the study found that bilateral symptoms, older age at first dislocation, and femoral tunnel position malposition were significant predictors of lower Banff Patellofemoral Instability Instrument scores.
Neri T, Parker DA, Putnis S, Klasan A, Trombert-Paviot B, Farizon F, Philippot R. Clinical and Radiological Predictors of Functional Outcome After Isolated Medial Patellofemoral Ligament Reconstruction at Midterm Follow-up. Am J Sports Med. 2019;47:1338–45.
Zhang Z, Song G, Zheng T, Ni Q, Feng H, Zhang H. The presence of a preoperative high-grade J-sign and femoral tunnel malposition are associated with residual graft laxity after MPFL reconstruction. Knee Surgery, Sport Traumatol Arthrosc. 2021;29:1183–90.
Kumar N, Bastrom TP, Dennis MM, Pennock AT, Edmonds EW. Adolescent Medial Patellofemoral Ligament Reconstruction: A Comparison of the Use of Autograft Versus Allograft Hamstring. Orthop J Sport Med. 2018;6:232596711877427.
Flanigan DC, Shemory S, Lundy N, Stitgen M, Long JM, Magnussen RA. Medial patellofemoral ligament reconstruction with allograft versus autograft tissue results in similar recurrent dislocation risk and patient-reported outcomes. Knee Surgery, Sport Traumatol Arthrosc. 2020;28:2099–104 The study assesses patients undergoing MPFL reconstruction with either hamstring autografts or allografts. The study found no significant difference in the rate of recurrent dislocation (3.3% vs. 3.5%) or patient reported outcomes between groups.
Lee PYF, Golding D, Rozewicz S, Chandratreya A. Modern synthetic material is a safe and effective alternative for medial patellofemoral ligament reconstruction. Knee Surgery, Sport Traumatol Arthrosc. 2018;26:2716–21.
Lind M, Nielsen T, Miller L, Sørensen OG, Mygind-Klavsen B, Faunø P. No Difference in Outcome Between Femoral Soft-Tissue and Screw Graft Fixation for Reconstruction of the Medial Patellofemoral Ligament: A Randomized Controlled Trial. Arthrosc J Arthrosc Relat Surg. 2019;35:1130–7 RCT assessing two femoral fixation strategies. The bone femoral fixation technique used an interference screw in the femur, while the soft-tissue fixation technique looped the graft around the adductor magnus tendon. No differences were identified between groups.
Malecki K, Fabis J, Flont P, Lipczyk Z, Niedzielski K. Preliminary results of two surgical techniques in the treatment of recurrent patellar dislocation. Int Orthop. 2016;40:1869–74.
Nelitz M, Dreyhaupt J, Reichel H, Woelfle J, Lippacher S. Anatomic Reconstruction of the Medial Patellofemoral Ligament in Children and Adolescents With Open Growth Plates. Am J Sports Med. 2013;41:58–63.
Nelitz M, Dreyhaupt J, Williams SRM. Anatomic reconstruction of the medial patellofemoral ligament in children and adolescents using a pedicled quadriceps tendon graft shows favourable results at a minimum of 2-year follow-up. Knee Surgery, Sport Traumatol Arthrosc. 2018;26:1210–1215.
Kocher MS, Smith JT, Iversen MD, Brustowicz K, Ogunwole O, Andersen J, Yoo WJ, McFeely ED, Anderson AF, Zurakowski D. Reliability, Validity, and Responsiveness of a Modified International Knee Documentation Committee Subjective Knee Form (Pedi-IKDC) in Children With Knee Disorders. Am J Sports Med. 2011;39:933–9.
Lafave MR, Hiemstra LA, Parikh SN, Peterson D, Kerslake S. Validity and Reliability of the Banff Patellofemoral Instability Instrument 2.0 in an Adolescent Population. J Pediatr Orthop. 2020;40:e103–8.
Lafave MR, Hiemstra LA, Kerslake S. Validity, Reliability, and Responsiveness of the Banff Patellar Instability Instrument (BPII) in a Adolescent Population. J Pediatr Orthop. 2018;38:e629–33.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
No conflicts of interest to disclose.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Outcomes Research in Orthopedics
Rights and permissions
About this article

Cite this article
Kay, J., Memon, M., Ayeni, O.R. et al. Medial Patellofemoral Ligament Reconstruction Techniques and Outcomes: a Scoping Review. Curr Rev Musculoskelet Med 14, 321–327 (2021). https://doi.org/10.1007/s12178-021-09719-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12178-021-09719-2