
Abstract
Purpose of review
The purpose of this review was to evaluate the literature regarding bundle payment reimbursement models for total joint arthroplasty (TJA).
Recent findings
From an economic standpoint, TJA are cost-effective, but they represent a substantial expense to the Centers for Medicare & Medicaid Services (CMS). Historically, fee-for-service payment models resulted in highly variable cost and quality. CMS introduced Bundled Payments for Care Improvement (BPCI) in 2012 and subsequently the Comprehensive Care for Joint Replacement (CJR) reimbursement model in 2016 to improve the value of TJA from the perspectives of both CMS and patients, by improving quality via cost control.
Summary
Early results of bundled payments are promising, but preserving access to care for patients with high comorbidity burdens and those requiring more complex care is a lingering concern. Hospitals, regardless of current participation in bundled payments, should develop care pathways for TJA to maximize efficiency and patient safety.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lower extremity total joint arthroplasty (TJA), including total knee arthroplasty (TKA) and total hip arthroplasty (THA), is one of the most frequently performed procedures in the USA, with nearly 1,000,000 performed annually [1, 2]. The incidence of these procedures is projected to rise to over 4,000,000 per year within the next two decades [3, 4]. Despite being cost-effective [5, 6] and reliable for regaining lower extremity joint function and improving quality of life [7], TJAs represented over seven billion dollars in cost to the Centers for Medicare & Medicaid Services (CMS) in 2014 [8], and they currently account for more Medicare expense than any other inpatient procedure [9]. As such, any increase in the number of TJAs performed annually threatens to impose an enormous economic burden on the US healthcare system.
Traditional fee-for-service (FFS) reimbursement models incentivize healthcare providers based on volume, rather than value of care delivered, leading to excessive use of services and increased expenditures [10]. A FFS model does little to incentivize resource stewardship or coordination across providers, since separate and unique payment systems exist for hospitals (medical severity adjusted diagnosis related group [MS-DRG]), physicians (current procedural terminology code [CPT]), and post-acute care providers, even when related to a single episode of care. Consequently, the quality and cost of care for TJA varies greatly among providers under FFS models [11, 12].
Several strategies have arisen to combat rising health care costs, and they are collectively referred to as alternative payment models, or APMs. Bundle payment models are a type of APM. Bundled payments incentivize providers to use a coordinated, multidisciplinary healthcare approach to enhance the quality and efficiency of care and improve patient satisfaction, while controlling cost [13•]. Paying a group of providers a single contracted price for all services provided within a defined episode of care [14, 15••], rather than separate piecemeal payments to individual providers, creates incentives to work collaboratively to improve quality and eliminate unnecessary services [16•]. Bundled payment initiatives in TJA have been shown to reduce costs while maintaining or even improving the quality of care provided [11, 17, 18]. Accordingly, multiple payer organizations have adopted bundled payment schemes for TJA [16•]. However, joint replacement surgeons and their representative advocacy groups have expressed reservations about their implementation, including perceived disincentives to care for high-risk patients and uncertainties around gain sharing [19•]. This article explores the history of bundled payment initiatives in TJA, their current form, and how this payment strategy can be utilized to provide value through affordable, high quality care.
The Evolution of Bundled Payment Models
Prior to the 1980s, hospitals were reimbursed retrospectively based on hospital costs incurred during a patient’s stay along a fee-for-service model. In 1983, CMS introduced the Inpatient Prospective Payment System (IPPS), which used Medicare Severity-Diagnosis Related Group (MS-DRG) payments to reimburse Medicare Part A services, inpatient hospital care, under a single price [20]. While hospitals received a single prospective per-discharge payment that included all of the facility costs, such as room and board, nursing, and costs associated with specialized care and ancillary services, orthopedic surgeons, and other medical professionals continued to receive separate fees for surgery and other services. Overall, the initiation of IPPS slowed the rate of increase in Medicare spending [21, 22], hospital resource utilization, and led to a decrease in the duration of lengths of stay [23]. However, the quality of inpatient care including mortality and readmission rates remained unchanged [24]. Though IPPS was a significant step toward bundling of medical services, it only focused on inpatient services, and payments for physician services, post-acute care, and readmissions were not included.
In 2009, CMS expanded IPPS by adding physician professional fees through the Acute Care Episode (ACE) demonstration program, in which physician-hospital organizations negotiated a prospective payment to cover both the inpatient facility, or Part A, and inpatient physician, or Part B, costs for patients undergoing seven orthopedic and cardiovascular episodes of care, including TJA, in five hospitals [25]. Though limited to facilities in the Southwestern USA, participating centers reported lower costs with no notable impact on patient outcomes [14, 26].
The Bundled Payment for Care Improvement (BPCI) initiative was developed by CMS in 2012 [13•]. Originally, a 3-year program, BPCI, was extended an additional 2 years until September 30, 2018 allowing participants to select from 48 episodes or DRG families, four program reimbursement models (three retrospective and one prospective), three levels of risk, and even define their own quality measures [14]. Unintentionally, the leniency of BPCI created a participation bias, because target prices and bonuses were predominantly based on a hospital’s improvement over its own past performance. BPCI attracted organizations with high-cost and/or low-performance histories, because it offered them the greatest opportunity for improvement. However, hospitals with low-cost and high-performance histories considered BPCI an unattractive option, because there was little room for improvement in their performance and thus little opportunity to offset their operational costs after the mandatory 2-3% discount to CMS.
In 2015, CMS announced the comprehensive care for joint replacement (CJR) model [8]. Implemented on April 1, 2016, CJR mandated the participation of nearly 800 hospitals in 67 Metropolitan Statistical Areas (MSAs), including hospitals in diverse settings such as academic and community, small and large, rural and urban. Modeled after BPCI, CJR differs in terms of participation, pricing, and risk. The CJR model covers all related items and services utilized within a 90-day episode of care. The episode of care is initiated with an admission to a participant hospital of a Medicare beneficiary who is ultimately discharged under MS-DRG 469 (major joint replacement with major complications or comorbidities) or 470 (major joint replacement without major complications or comorbidities). This is called the “anchor hospitalization”. The episode ends 90-days post-discharge. The episode of care includes all related items and services including the following: physician services, inpatient hospital services (including readmissions), inpatient psychiatric facility services, long-term care hospital services, inpatient rehabilitation facility services, skilled nursing facility services, home health agency services, hospital outpatient services, independent outpatient therapy services, clinical laboratory services, durable medical equipment, drugs, and hospice. Unrelated services excluded from the episode costs include acute clinical conditions not arising from existing episode-related chronic clinical conditions or complications of surgery and chronic conditions that are generally not affected by the procedure or post-surgical care [8].
The CJR model is a retrospective bundled payment model, meaning that participant hospitals retrospectively receive payment for all costs associated with an episode of care for each case. Participant hospitals are paid a “target price” for an episode. Target prices are stratified by MS-DRG (469 or 470) and the presence or absence of hip fracture, thus there are four target prices. Target prices are defined for each hospital and MSA based on historical average costs, less a 1.5–3% discount based on quality metrics. In years 1 and 2 of the model, two-thirds of the target price is derived from a hospital’s 2012 through 2014 claims data, with the remaining one-third coming from regional claims data. In year three, one-third of the target price will be derived from a hospital’s 2014 through 2016 claims data, with the remaining two-thirds coming from regional claims data. The mix then shifts to 100% regional claims data thereafter. Instead of competing against one’s own prior performance, CJR’s pricing creates regional competition. At the end of the performance year, hospitals that achieve spending below the target price and meet quality performance thresholds on three required quality measures are eligible to earn a reconciliation payment for the difference between the target price and actual episode spending, up to a specified cap (“stop-gain limit”). In contrast, hospitals with spending that exceeds the target price are financially responsible for the difference between the target price and actual episode spending, up to a specified repayment limit (“stop-loss limit”) which will increase from 5 to 20% between performance year 2 to 4 [8].
In addition to spending less than the target price, three quality measures must be met to qualify for a reconciliation payment. The first is national quality forum (NQF) #1550, the hospital-level risk-standardized complication rate (RSCR) [27]. This measure utilizes Medicare claims data to identify complications occurring from the date of admission to 90 days post-discharge. The RSCR is calculated as the ratio of the number of “predicted” to the number of “expected” admissions with a complication, multiplied by a national unadjusted complication rate. The denominator is the number of admissions with a complication expected based on the nation’s performance with that hospital’s case-mix. The numerator is a dichotomous (yes/no) outcome and includes the following: acute myocardial infarction, pneumonia, and sepsis within 7 days from the date of admission; death, surgical site bleeding, and pulmonary embolism within 30 days of admission; and mechanical complications and periprosthetic joint infection within 90 days of admission. The second quality measure is NQF #1551, which is the hospital-level 30-day risk-standardized readmission rate (RSRR) [28]. This outcome is defined as an unplanned readmission for any cause within 30 days of the discharge date. A specified set of planned readmissions does not count, including things like obstetrical delivery, transplant surgery, and maintenance chemotherapy, though admissions for acute illness or complications of care are never planned. The final quality measure is NQF #0166 or the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAPS) survey [29], which is a 27-item survey with seven domain level composites that patients complete to rate their hospital experience. A final method for adding points to a hospitals CJR composite score has recently been introduced and involves submitting voluntary patient-reported outcomes including the following: Veterans Rand 12 (VR-12), Patient Reported Outcomes Measurement Information System (PROMIS) 10-Global, the Hip disability and Osteoarthritis Outcomes Survey (HOOS), JR. and Knee injury and Osteoarthritis Outcome Score (KOOS), JR., or the full HOOS and KOOS subscales, on a predefined percentage of their cases.
Impact of Comorbidities and Complications on Cost
The immediate area of focus for hospitals participating in CJR is lowering episode costs. In addition to providing patients with a more complete informed consent, understanding the risk of 90-day postoperative complications is essential to anticipating potential postoperative care requirements, which directly correlate to profitability under the bundle. Although complication rates following TJA are low [30], the cost of complications can be staggering. For example, thromboembolic disease is associated with significantly increased cost [31], estimated at $18,000 when identified during the index hospitalization and nearly $6000 when diagnosed after discharge and stimulating a readmission [32]. Similarly, the economic burden of periprosthetic joint infection is astounding, with an average cost of $116,383 per episode [33•] and a total projected annual cost to the US healthcare system exceeding $1.62 billion by 2020 [34].
The cost of comorbidities has been repeatedly demonstrated. Bozic et al. [15••] evaluated all payments to Medicare providers up to 30 days postoperatively and found mean episode-of-care payments ranged from $25,568 for primary TJA in patients with no comorbidities to $50,648 for revision TJA in patients with major comorbidities or complications. They noted significant variance for each of the means. Other comorbidities have also been associated with increased postoperative complications (e.g., congestive heart failure, valvular heart disease, and chronic obstructive pulmonary disease) and cost (e.g., coagulopathy, congestive heart failure, and electrolyte imbalance) following TJA [35•]. Considering the influence of comorbidities on overall cost, it is not surprising that 94% of AAHKS members express concerns regarding the financial disincentive of operating on high-risk patients [19•]. Future research should focus on whether preoperative optimization of these chronic medical conditions can reduce postoperative complication rates and whether this reduces episode costs.
Lastly, risk factors can be classified as either modifiable or non-modifiable. It has been demonstrated that certain non-modifiable risk factors are associated with worse outcomes after TJA. For example, even after the introduction of a system-wide readmission reduction initiative, Keeney et al. found that minority patients and those with low socioeconomic status experienced higher 30-day readmission rates [36•, 37•]. These data underscore the notion that certain vulnerable populations may face access to care issues for joint replacement under bundled payment models, if there is not appropriate risk adjustment for these non-modifiable factors.
Current risk adjustment in the CJR is crude, such that target prices are anchored either to MS-DRG 469 or 470 and then modified only based upon the presence or absence of an acute hip fracture. Risk adjustment should be based on a wide number of relevant variables, including patient-related and procedure-related factors, to create well-functioning bundled payment models. If bundled payments are not appropriately risk-adjusted for case complexity and expected resource utilization, “cherry picking” (providing care to low-risk patients) and “lemon dropping” (denying care to high-risk patients) will occur, potentially restricting TJA access to at-risk patient populations and/or concentrating their care in a few number of safety net hospitals. Thus, future research should identify relevant variables for risk adjustment to optimize resource allocation and incentivize care for all TJA patients.
Optimizing Quality and Reducing Cost
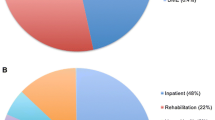
To determine where potential cost savings may come from, multiple studies have evaluated the impact of preoperative, intraoperative, and postoperative care on overall spending in TJA. The best opportunity to lower episode costs appears to be in the post-acute care (PAC) setting, where the greatest cost variation exists. In 2014, Bozic et al. [15••] demonstrated that post-discharge care accounted for 70% of the total episode payment and varied significantly between patients and procedures. This is similar to a report by Navathe et al. [38••] who found 49% of savings under ACE and BPCI programs came from PAC spending reductions on skilled care facilities post-discharge. Slover et al. [39•] performed a cost analysis study to evaluate strategies for minimizing post-discharge costs following TJA. They concluded that the cost of additional acute care hospital days was relatively small compared to an extended post-acute inpatient rehabilitation facility stay and that keeping patients in the hospital a few extra days and then discharging them directly to home may result in an overall lower cost than discharge after a shorter hospital stay to an expensive skilled care facility. While the ideal inpatient length of stay (LOS) remains unclear, skilled care facilities probably represent low value to patients, as it has been demonstrated that discharge to these facilities versus to home is associated with higher complications for THA [40•] and TKA [41•] with no associated functional benefit [42•, 43].
Readmissions are also a major cost driver. Bosco et al. [44] found that the 30-day readmission cost burden ranged from 3% for TKA to 12% for revision TKA. To cover episode costs related to readmissions, profit margins would have to exceed 4.3% for primary THA, 8.3% for revision THA, and nearly 12% for revision TKA. Similarly, Clair et al. [45] reported that medical- and procedural-related readmissions cost, on average, $11,682 and $27,979, respectively. Kurtz et al. [46] also identified readmission as a primary cost driver and concluded that nearly half of the total annual economic burden in the USA for readmissions following TJA was for a medical reason and unrelated to the joint replacement procedure. This underscores the importance of hospitals and doctors preoperatively optimizing, to the extent possible, patients with modifiable risk factors. In the same study, the authors identified infection, dislocation, and periprosthetic fractures as the most costly types of procedurally related readmissions, leading to the conclusion that prevention of these complications and readmissions will have the greatest impact on the overall economic burden [46].
The next best opportunity for episode of care savings appears to be implant cost, which remains highly variable and accounts for between 13% and 60% of hospital reimbursements [47,48,49]. The cost of primary TKA implants ranges from $1797 to $12,093, and the cost of primary THA implants ranges from $2392 to $12,651 [50]. Consequently, strategies for lowering implant costs should be a focus, especially considering many higher-cost prostheses frequently have unproven clinical benefit. An overall decrease in the variability and reduction in the cost of implants is possible through the creation of implant selection protocols and resource use committees, giving hospitals improved negotiating power with device manufacturers [5]. This was found to be true in a Canadian model in which higher-volume hospitals were able to minimize costs more effectively than low-volume hospitals through negotiating power [51]. Hospital-based strategies to reduce the cost of implants have been effectively demonstrated by Scranton [52] and Zuckerman et al. [53], who reported a 23% reduction in implant costs over 1 year. Alternatively, or in addition, some surgeons have proposed patient-cost sharing, which would allow patients to contribute directly toward covering the cost of their implants. This is a particularly intriguing response to direct-to-consumer marketing. Previous studies have demonstrated that patients in the USA are willing to pay for implants [54,55,56], although no current pathway exists for patients to share the cost of TJA implants.
A crucial step toward reducing the cost of implants nationally, while simultaneously improving the evidence of their efficacy, is the American Joint Replacement Registry [57]. Expansion of US national arthroplasty registry will facilitate comparative studies to evaluate the cost and performance of different prostheses and bearing surfaces, and it will aid identifying early implant complications and failures. It has been speculated that Sweden’s long-standing national registry for THA has improved Swedish surgeons’ selection of implants and surgical techniques, resulting in a revision rate for THA that is more than half of that for THA in the USA [58, 59].
Finally, as regional competition hastens, hospitals will likely be forced to focus on internal costs of care delivery, addressing surgeon productivity as well as hospital and operating room efficiency. The creation of multidisciplinary clinical pathways for perioperative care has been shown to improve quality and reduce cost by nearly 20% [60]. Accelerated rehabilitation protocols are another strategy to reduce cost and improve outcomes during the inpatient period. These protocols can reduce LOS, improve outcomes, and are estimated to save approximately $4000 per patient [61, 62]. A 2008 Cochrane review supports implementation of multidisciplinary clinical pathways, including early postoperative rehabilitation [63]. In terms of productivity, a study by Wilson et al. [64•] defined TKA volume thresholds associated with adverse outcomes for surgeons and hospitals. The authors found surgeons performing greater than 146 TKAs per year had significantly lower 90-day complication rates and 2-year revision rates than those surgeons performing fewer TKAs. Similarly, hospitals supplying more than 645 TKAs per year had significantly lower 90-day complication and 90-day mortality rates than lower volume hospitals [64•]. Thus, higher-volume surgeons and facilities appear to be both less costly and safer for patients and should improve the value of TJA.
Early Evidence for Bundled Payment Models
It remains to be seen whether the CJR model will improve the quality and decrease the cost of TJA in a manner similar to that observed following initiation of the BPCI, which some reports show decreased Medicare episode payments between $1166–$2443 with no change in claims-based quality outcome measures [38••, 65••]. The impact of CJR on overall utilization of TJA nationally is also uncertain, as ultra-high performing centers may take advantage of the margins early in the program, initially increasing overall expenditures. Additionally, the expense of managing bundled payments is also indeterminate and may make offering TJA cost prohibitive for smaller institutions. While these changes will most directly and immediately impact the 800 CJR participant hospitals, representing approximately 25% of lower extremity joint replacements performed annually in the USA, they will likely have a national effect as the program is extended.
Early results of bundled payments are promising, demonstrating a reduction in cost and an improvement in quality. In a study of 271 patient episodes [66], the creation of a “complete care” program resulted in decreased LOS (3.4 to 2.7 days), a reduction in catheter-associated urinary tract infections (5.2 per 1000 to 0), and a reduction in 30-day readmissions (5.0 to 1.6%). The frequency of discharge to home increased from 39 to 75%. The group also improved their HCAHPS (9 or 10) from a baseline of 74 to 88%. Within the first year of their program, they reduced the total cost of care and showed financial value creation of $522,389 (9.8%) for the hospital system [66].
Froemke et al. [16•] reported their approach to standardizing a care pathway for TJA, incentivized by a gain sharing opportunity, that brought together best-practices for quality care and patient engagement across the entire episode of care from preoperative planning through patient discharge. Coordinating care among providers resulted in an 18% reduction in average LOS and a shift from home health and skilled facility discharge to home self-care (54.1 to 63.7%), which resulted in a 6% reduction in cost over the study period. Similarly, in 2016 another large academic institution reported its results after implementing hospital wide changes following the adoption of a bundled payment model [67]. The authors reported a decrease in the average hospital LOS from 4.27 to 3.58 days and discharges to skilled care facilities decreased from 71 to 44%. The same authors showed that over the same period, there was a decrease in the average episode of care cost from $34,249 to $27,541, with the largest decrease in cost resulting from a reduction in PAC costs per episode, from $6228 at baseline to $742 [68]. A follow-up study 3 years after the project began reported a continued decrease in LOS from 3.58 to 2.96 days, and the rate of discharge to skilled care facilities also decreased from 44 to 28% [69•]. All-cause readmission rates at 30, 60, and 90 days decreased from 7 to 5%, 11 to 6%, and 13 to 8%, respectively. Finally, the authors reported a 20% decrease in 90-day cost over the 3-year study period [69•].
Practical Strategies for Success Under Bundled Payment Models
Successfully managing bundled payments will require hospitals to invest in new or enhanced capabilities, including improved data collection and analysis, technology upgrades, and care coordination resources. Thus, there will be incremental costs necessary to manage a 90-day episode of care in the face of declining target prices for the episode. As a result, TJA may become impractical and unaffordable for low-volume hospitals, resulting in consolidation or closure of low-volume programs. Those hospitals not participating in CJR should begin building the infrastructure necessary to manage bundled payments, as it will likely be difficult to adapt to the bundled payment model once regional competitors have overcome their own inefficiencies.
Van Citters et al. [70•] described their recommendations for developing a pathway for high-value, patient-centered TJA care through quantitative and qualitative methods, which may be generalizable to hospitals seeking a strategy to prepare for bundled payments. Specific factors essential for success in managing bundled payments include engaging physicians from all involved specialties to be a part of designing the care pathway. Creating a care coordinator position, as the point of contact for patients throughout the episode, can reduce costly emergency room visits and readmissions. The hospital and care providers should also invest in patient education strategies to set and manage expectations, particularly focusing on what to expect after surgery and how to increase discharge to home and prevent readmissions. Incentives to improve operating room and hospital efficiency are also target areas.
Conclusions
Alternative payment models, including bundled payments, represent a major change in the reimbursement landscape for TJA, departing from traditional fee-for-service paradigms. Early results of bundled payments are promising. Hospitals, regardless of current participation in bundled payments, should develop care pathways for TJA to maximize efficiency and patient safety. Appreciating the fact that post-acute care and readmissions are associated with the greatest variance in episode costs for TJA, initial efforts under bundled payments should focus on encouraging discharge to home and devoting resources toward preventing readmissions, including creation of care coordinators and optimizing modifiable preoperative risk factors. As bundled payments move toward regional pricing, preserving access to care for patients with high comorbidity burdens and those requiring more complex care is a lingering concern. Risk-adjusted pricing will become an even more important feature for these models to protect access to TJA for all patients.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Nwachukwu BU, O’Donnell E, McLawhorn AS, et al. Episode of care payments in total joint arthroplasty and cost minimization strategies. HSS J. 2016;12(1):91–3.
Centers for Disease Control and Prevention. 2013 National hospital discharge survey: 2010 table, procedures by selected patient characteristics. Centers for Disease Control and Prevention, Atlanta, GA: Available at: http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberprocedureage.pdf. 2017(02/07).
Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–5.
Cram P, Lu X, Kates SL, et al. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991–2010. JAMA. 2012;308(12):1227–36.
Bumpass DB, Nunley RM. Assessing the value of a total joint replacement. Curr Rev Musculoskelet Med. 2012;5(4):274–82.
Daigle ME, Weinstein AM, Katz JN, et al. The cost-effectiveness of total joint arthroplasty: a systematic review of published literature. Best Pract Res Clin Rheumatol. 2012;26(5):649–58.
Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;370(9597):1508–19.
Centers for Medicare Medicaid Services. Comprehensive Care for Joint Replacement Payment Model for Acute Care Hospitals Furnishing Lower Extremity Joint Replacement Services; Final Rule 2015:1–282.
Hawker GA, Badley EM, Croxford R, et al. A population-based nested case-control study of the costs of hip and knee replacement surgery. Med Care. 2009;47(7):732–41.
Miller HD. From volume to value: better ways to pay for health care. Health Aff (Millwood). 2009;28(5):1418–28.
Luft HS. Economic incentives to promote innovation in healthcare delivery. Clin Orthop Relat Res. 2009;467(10):2497–505.
Tomek IM, Sabel AL, Froimson MI, et al. A collaborative of leading health systems finds wide variations in total knee replacement delivery and takes steps to improve value. Health Aff (Millwood). 2012;31(6):1329–38.
• Centers for Medicare & Medicaid Services. Bundled Payments for Care Improvement (BPCI) Initiative: General Information. Available at: https://innovation.cms.gov/initiatives/bundled-payments. 2017. This website summarizes the various bundled payment models CMS employs under the Bundled Payments for Care Improvement (BPCI) Initiative.
Froimson MI, Rana A, White RE Jr, et al. Bundled payments for care improvement initiative: the next evolution of payment formulations: AAHKS Bundled Payment Task Force. J Arthroplast. 2013;28(8 Suppl):157–65.
•• Bozic KJ, Ward L, Vail TP, et al. Bundled payments in total joint arthroplasty: targeting opportunities for quality improvement and cost reduction. Clin Orthop Relat Res. 2014;472(1):188–93. This study examined Medicare episode-of-care payments for 250 lower extremity TJAs performed at one institution. The authors found wide variance in costs depending on procedure type, patient comorbidities, complications, discharge destination, and readmission. Post-acute care, including use of skilled facilities, accounted for greater than one-third of total episode payments.
• Froemke CC, Wang L, ML DH, et al. Standardizing care and improving quality under a bundled payment initiative for total joint arthroplasty. J Arthroplast. 2015;30(10):1676–82. The authors describe their care pathway and gain-sharing arrangement under a bundled payment pilot program. Comparisons between pre-pilot and pilot cohorts demonstrated an 18% reduction in average length of hospital stay and decreased utilization of home health and skilled care facilities after hospital discharge to home self-care.
Cutler DM, Ghosh K. The potential for cost savings through bundled episode payments. N Engl J Med. 2012;366(12):1075–7.
Lansky D, Nwachukwu BU, Bozic KJ. Using financial incentives to improve value in orthopedics. Clin Orthop Relat Res. 2012;470(4):1027–37.
• Kamath AF, Courtney PM, Bozic KJ, et al. Bundled Payment in Total Joint Care: Survey of AAHKS Membership Attitudes and Experience with Alternative Payment Models. J Arthroplast. 2015;30(12):2045–56. The authors surveyed the American Association of Hip and Knee Surgeons membership about their participation in and attitudes toward alternative payment models (APM). At the time of the survey, 61% of members were planning to participate in or already participating in an APM. 45% of respondents believed that bundled payments would be most effective at improving quality and reduce costs associated with lower extremity arthroplasty. There were concerns about disincentives to provide care to high-risk patients and uncertainty about gain-sharing.
Shih T, Chen LM, Nallamothu BK. Will bundled payments change health care? Examining the evidence thus far in cardiovascular care. Circulation. 2015;131(24):2151–8.
Chulis GS. Assessing Medicare’s prospective payment system for hospitals. Med Care Rev. 1991;48(2):167–206.
White C. Why did Medicare spending growth slow down? Health Aff (Millwood). 2008;27(3):793–802.
Feinglass J, Holloway JJ. The initial impact of the Medicare prospective payment system on US health care: a review of the literature. Med Care Rev. 1991;48(1):91–115.
Lave JR. The effect of the Medicare prospective payment system. Annu Rev Public Health. 1989;10:141–61.
Centers for Medicare and Medicaid Services. Medicare Acute Care Episode (ACE) Demonstration. Available at: http://innovation.cms.gov/initiatives/ACE. 2017(02/05)
Davis C. Bundled payments: Lessons learned from the ACE demo. Available at: http://www.fiercehealthfinance.com/story/bundled-payments-lessons-learned-ace-demo/2010-06-30. 2010;2017(02/05).
National Quality Forum. 1550: Hospital-level risk-standardized complication rate (RSCR) following elective primary total hip arthroplasty (THA) and/or total knee arthroplasty (TKA). STEWARD: Centers for Medicare & Medicaid Services Available at: http://www.qualityforum.org/QPS/1550. 1/25/2017;2017(02/07).
National Quality Forum. 1551: Hospital-level 30-day risk-standardized readmission rate (RSRR) following elective primary total hip arthroplasty (THA) and/or total knee arthroplasty (TKA). STEWARD: Centers for Medicare & Medicaid Services. Available at: http://www.qualityforum.org/QPS/1551. 1/25/2017;2017(02/07).
National Quality Forum. 0166: HCAHPS. STEWARD: Centers for Medicare & Medicaid Services. Available at: http://www.qualityforum.org/QPS/0166. 1/25/2017;2017(02/05).
SooHoo NF, Lieberman JR, Ko CY, et al. Factors predicting complication rates following total knee replacement. J Bone Joint Surg Am. 2006;88(3):480–5.
Ollendorf DA, Vera-Llonch M, Oster G. Cost of venous thromboembolism following major orthopedic surgery in hospitalized patients. Am J Health Syst Pharm. 2002;59(18):1750–4.
Oster G, Ollendorf DA, Vera-Llonch M, et al. Economic consequences of venous thromboembolism following major orthopedic surgery. Ann Pharmacother. 2004;38(3):377–82.
• Kapadia BH, MJ ME, Issa K, et al. The economic impact of periprosthetic infections following total knee arthroplasty at a specialized tertiary-care center. J Arthroplast. 2014;29(5):929–32. The authors reviewed an institutional periprosthetic joint infection (PJI) registry to identify total knee PJI treated between 2007 and 2011 with a 2-stage exchange arthroplasty. Twenty one patients with PJI were matched 1:1 with primary TKA patients. PJI patients had significantly longer length of hospital stay, more readmissions, and more outpatient visits. The mean annual cost was $116,383 for the PJI cohort, compared to $28,249 for the primary TKA cohort.
Kurtz SM, Lau E, Watson H, et al. Economic burden of periprosthetic joint infection in the United States. J Arthroplast. 2012;27(8 Suppl):61–5. e1
• Hustedt JW, Goltzer O, Bohl DD, et al. Calculating the cost and risk of comorbidities in total joint arthroplasty in the United States. J Arthroplast. 2017;32(2):355–361.e1. The authors reviewed the National Inpatient Sample to identify primary and revision hip and knee arthroplasty patients treated between 2008 and 2012. Comorbid conditions were recorded, and their associations with complications and costs were determined. They found that patients with congestive heart failure (CHF), valvular heart disease and chronic obstructive pulmonary disease had the greatest risk for postoperative complications, while patients with coagulopathy, CHF, and electrolyte disorders had the highest cost after total joint arthroplasty.
• Keeney JA, Nam D, Johnson SR, et al. Socioeconomically disadvantaged CMS beneficiaries do not benefit from the readmission reduction initiatives. J Arthroplast. 2015;30(12):2082–5. The authors analyzed 3,825 primary total hip arthroplasties and 3,118 primary total knee arthroplasties performed at a single institution, and found that minority patients and those of lower socioeconomic status had higher readmission rates after total knee and hip arthroplasty, despite risk reduction initiatives.
• Keeney JA, Nam D, Johnson SR, et al. The impact of risk reduction initiatives on readmission: THA and TKA readmission rates. J Arthroplast. 2015;30(12):2057–60. The authors examined the impact of risk reduction initiatives on 30-day readmissions after primary total knee and total hip arthroplasty at a single institution. They found that these initiatives resulted in a significant reduction in readmission frequency after total knee arthroplasty, but not after total hip arthroplasty.
•• Navathe AS, Troxel AB, Liao JM, et al. Cost of joint replacement using bundled payment models. JAMA Intern Med. 2017;177(2):214–22. The authors analyzed 3,942 patients receiving primary hip and knee replacement under the Acute Care Episodes (ACE) and Bundled Payments for Care Improvement (BPCI) demonstration projects. Mean episode expenditures declined over 20%, for joint replacement episodes without complications, whereas they declined approximately 14% joint replacement episodes with complications. Readmissions and emergency department visits declined insignificantly. Over 50% of hospital savings came from internal cost reductions, and the balance came from post-acute care spending reductions by reducing skilled care facility utilization. Reductions in implant costs, contributed the most to hospital savings.
• Slover JD, Mullaly KA, Payne A, et al. What is the best strategy to minimize after-care costs for total joint arthroplasty in a bundled payment environment? J Arthroplast. 2016;31(12):2710–3. The authors used decision analysis techniques to explore the feasibility of extending hospital length of stay to avoid discharge to skilled care facilities after lower extremity joint replacement. They found that extending the acute hospitalization for up to 5.2 extra days to permit discharge to home, may be financially preferable over discharge to a skilled care facility.
• Fu MC, Samuel AM, Sculco PK, MacLean CH, Padgett DE, McLawhorn AS. Discharge to inpatient facilities after total hip arthroplasty is associated with increased postdischarge morbidity. J Arthroplast. 2017. The authors used the American College of Surgeons National Surgical Quality Improvement Program registry from 2011 to 2014 to identiy all primary total hip arthroplasty (THA) patients. They found that discharge to skilled care facilities following THA is associated with increased odds for septic complications, urinary complications, readmission, wound complications, and respiratory complications.
• McLawhorn AS, Fu MC, Schairer WW, Sculco PK, MacLean CH, Padgett DE. Continued inpatient care after primary total knee arthroplasty increases 30-day post-discharge complications: a propensity score-adjusted analysis. J Arthroplast. 2017. The authors used the American College of Surgeons National Surgical Quality Improvement Program registry from 2011 to 2014 to identiy all primary total knee arthroplasty (TkA) patients. They found that discharge to skilled care facilities following TKA is associated with increased odds for unplanned hospital readmission, and for respiratory, septic, thromboembolic and urinary complications.
• Buhagiar MA, Naylor JM, Harris IA, Xuan W, Kohler F, Wright R, et al. Effect of inpatient rehabilitation vs a monitored home-based program on mobility in patients with total knee arthroplasty: The HIHO Randomized Clinical Trial. JAMA. 2017;317(10):1037–46. This randomized controlled trial demonstrated that use of skilled care facilities for rehabilitation following total knee arthroplasty did not improve mobility at 26 weeks after surgery compared to patients receiving a monitored home-based program.
Mahomed NN, Davis AM, Hawker G, et al. Inpatient compared with home-based rehabilitation following primary unilateral total hip or knee replacement: a randomized controlled trial. J Bone Joint Surg Am. 2008;90(8):1673–80.
Bosco JA 3rd, Karkenny AJ, Hutzler LH, et al. Cost burden of 30-day readmissions following Medicare total hip and knee arthroplasty. J Arthroplast. 2014;29(5):903–5.
Clair AJ, Evangelista PJ, Lajam CM, et al. Cost analysis of total joint arthroplasty readmissions in a bundled payment care improvement initiative. J Arthroplast. 2016;31(9):1862–5.
Kurtz SM, Lau EC, Ong KL, Adler EM, Kolisek FR, Manley MT. Which clinical and patient factors influence the national economic burden of hospital readmissions after total joint arthroplasty? Clin Orthop Relat Res. 2017; doi:10.1007/s11999-017-5244-6.
Boniforti F. Assessing hospital cost of joint arthroplasty. Joints. 2016;3(4):186–90. doi:10.11138/jts/2015.3.4.186.
Maradit Kremers H, Visscher SL, Moriarty JP, et al. Determinants of direct medical costs in primary and revision total knee arthroplasty. Clin Orthop Relat Res. 2013;471(1):206–14.
Mercuri JJ, Bosco JA, Iorio R, et al. The ethics of patient cost-sharing for total joint arthroplasty implants. J Bone Joint Surg Am. 2016;98(24):e111.
Robinson JC, Pozen A, Tseng S, et al. Variability in costs associated with total hip and knee replacement implants. J Bone Joint Surg Am. 2012;94(18):1693–8.
Martineau P, Filion KB, Huk OL, et al. Primary hip arthroplasty costs are greater in low-volume than in high-volume Canadian hospitals. Clin Orthop Relat Res. 2005;(437):152–6.
Scranton PE Jr. The cost effectiveness of streamlined care pathways and product standardization in total knee arthroplasty. J Arthroplast. 1999;14(2):182–6.
Zuckerman JD, Kummer FJ, Frankel VH. The effectiveness of a hospital-based strategy to reduce the cost of total joint implants. J Bone Joint Surg Am. 1994;76(6):807–11.
Sharkey PF, Sethuraman V, Hozack WJ, et al. Factors influencing choice of implants in total hip arthroplasty and total knee arthroplasty: perspectives of surgeons and patients. J Arthroplast. 1999;14(3):281–7.
Schwarzkopf R, Katz JN, Chen SP, et al. Patients’ willingness to contribute to cost of novel implants in total joint arthroplasty. J Arthroplast. 2014;29(9 Suppl):143–6. e4
Schwarzkopf R, Sagebin FM, Karia R, et al. Factors influencing patients' willingness to pay for new technologies in hip and knee implants. J Arthroplast. 2013;28(3):390–4.
American Joint Replacement Registry. Available at: www.ajrr.net. 2017(02/05).
Wilson NA, Schneller ES, Montgomery K, et al. Hip and knee implants: current trends and policy considerations. Health Aff (Millwood). 2008;27(6):1587–98.
Kurtz S, Mowat F, Ong K, et al. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Joint Surg Am. 2005;87(7):1487–97.
Healy WL, Iorio R, Ko J, et al. Impact of cost reduction programs on short-term patient outcome and hospital cost of total knee arthroplasty. J Bone Joint Surg Am. 2002;84-A(3):348–53.
Larsen K, Hansen TB, Thomsen PB, et al. Cost-effectiveness of accelerated perioperative care and rehabilitation after total hip and knee arthroplasty. J Bone Joint Surg Am. 2009;91(4):761–72.
Larsen K, Hvass KE, Hansen TB, et al. Effectiveness of accelerated perioperative care and rehabilitation intervention compared to current intervention after hip and knee arthroplasty. A before-after trial of 247 patients with a 3-month follow-up. BMC Musculoskelet Disord. 2008;9:59. doi:10.1186/1471-2474-9-59.
Khan F, Ng L, Gonzalez S, et al. Multidisciplinary rehabilitation programmes following joint replacement at the hip and knee in chronic arthropathy. Cochrane Database Syst Rev. 2008;(2):CD004957.
• Wilson S, Marx RG, Pan TJ, Lyman S. Meaningful thresholds for the volume-outcome relationship in total knee arthroplasty. J Bone Joint Surg Am. 2016;98(20):1683–90. The authors examined a New York State administrative claims database to identify 289,976 patients undergoing primary total knee arthroplasty. They analyzed surgeon procedure volume thresholds at which there were significant differences in 90-day complications and 2-year revision rates, and they analyzed hospital procedure volume thresholds at which there were significant differences in 90-day complications and 90-day mortality. They identified four volume categories for surgeons: 0 to 12, 13 to 59, 60 to 145, and ≥146 total knee arthroplasties per year. They also identified four volume categories for hospitals: 0 to 89, 90 to 235, 236 to 644, and ≥645 total knee arthroplasties per year.
•• Dummit LA, Kahvecioglu D, Marrufo G, et al. Association between hospital participation in a medicare bundled payment initiative and payments and quality outcomes for lower extremity joint replacement episodes. JAMA. 2016;316(12):1267–78. The authors reviewed the efficacy of Medicare's BPCI iniative during its first 21 months, comparing hospitals within BPCI and hospitals not participating in bundled payment models. Medicare payments significantly declined for lower extremity joint replacement episodes provided in BPCI-participating hospitals, without a significant change in quality outcomes.
Mouille B, Higuera C, Woicehovich L, Deadwiler M. NEW RISK, NEW BUSINESS MODELS: How to Succeed in Bundled Payments for Total Joint Replacement. Available at: http://catalyst.nejm.org/how-to-succeed-in-bundled-payments-for-total-joint-replacement/. NEJM Catalyst. 2016; 2017(07/2017).
Iorio R, Clair AJ, Inneh IA, et al. Early results of Medicare's bundled payment initiative for a 90-day Total joint arthroplasty episode of care. J Arthroplast. 2016;31(2):343–50.
NYU Langone Medical Center. Bundled payments for total joint replacements improve quality of care, outcomes in Medicare patient. Available at: http://www.news-medical.net/news/20160302/Bundled-payments-for-total-joint-replacements-improve-quality-of-care-outcomes-in-Medicare-patient.aspx. 2016; 2017(07/2017).
• Dundon JM, Bosco J, Slover J, et al. Improvement in total joint replacement quality metrics: year one versus year three of the bundled payments for care improvement initiative. J Bone Joint Surg Am. 2016;98(23):1949–53. The authors compared lower extremity total joint arthroplasty outcomes between the first and third years of participation in Medicare's BPCI program. They found significantly decreased hospital length of stay, decreased frequency of discharge to skilled care facilities, decreased readmissions, and decreased cost per episode of care in the third year compared to the first year.
• Van Citters AD, Fahlman C, Goldmann DA, et al. Developing a pathway for high-value, patient-centered total joint arthroplasty. Clin Orthop Relat Res. 2014;472(5):1619–35. The authors published their development of a clinical care pathway for lower extremity total joint arthroplasty. The pathway spanned 14 months, from the pre-surgical visit to one year after hospital discharge. Creation of the pathway required input from a multidisciplinary team of stakeholders. The care pathway included over 130 techniques to improve care, focusing principally on standardization and process improvement, interdisciplinary collaboration, and patient engagement and education.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Both authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Quality and Cost Control in TJA
Rights and permissions
About this article

Cite this article
McLawhorn, A.S., Buller, L.T. Bundled Payments in Total Joint Replacement: Keeping Our Care Affordable and High in Quality. Curr Rev Musculoskelet Med 10, 370–377 (2017). https://doi.org/10.1007/s12178-017-9423-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12178-017-9423-6