
Abstract
The COVID-19 pandemic has dramatically affected mental health, creating an urgent need for convenient and safe interventions to improve psychological distress. A comprehensive meta-analysis aims to systematically analyze whether randomized controlled trials of online mindfulness interventions could enhance mental health during the COVID-19 pandemic. Following a thorough database search, we included 34 randomized controlled studies that satisfied the criteria. The study quality score we included was based on the risk of bias assessment tool recommended by the Cochrane Collaboration. The Comprehensive Meta-Analysis Version 3.3 (CMA 3.3) was used in this study for the meta-analysis. Online mindfulness intervention programs had a small to medium impact on the results of interventions for stress (g = 0.278, p < 0.001; 95% CI = 0.119–0.437), anxiety (g = 0.459, p < 0.001; 95% CI = 0.218-0.700), and depression (g = 0.458, p < 0.001; 95% CI = 0.239–0.676). The study shows that online mindfulness intervention can be useful in reducing people’s mental health issues during the epidemic. The quality assessment of the most of studies included was evaluated as “unclear”. It may affect the results of the meta-analysis. To confirm the intervention’s influencing variables, more research is required.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During the Covid-19 pandemic, the number of individuals suffering from common mental health problems such as stress, anxiety, and depression is increasing globally. Lockdowns, the fear of Covid-19, and the variety of activities that had been heavily restricted may have had an impact on mental health. The psychological impact on mental health during Covid-19 that was reported in many countries was similar. It was estimated that during the Covid-19 epidemic, 54% of Chinese people assessed the psychological impact of the pandemic as moderate to severe, with 29% experiencing anxiety symptoms (Wang et al., 2020). Similarly, a survey conducted in Europe revealed that 32.4% of persons had depressive illnesses, 23.8% have anxiety disorders, and 31.9% have stress (Salari et al., 2020). The impact of the pandemic on mental health problems also increased in different populations. The survey conducted by the French National Public Health Agency found that young adult (18–24 year) was the most psychologically impacted with 28.25% of these age groups on depression and 26.9% on anxiety (French Public Health Agency, 2021). Dai et al. (2020)reported that 18.6% of patients with Covid-19 suffered from anxiety symptoms, and 13.4% were affected by depressive symptoms. The mental health problems caused by the virus and isolation urgently need to be tackled.
However, isolation made the difficult for being delivered in a face-to-face format, and online-based intervention can tackle these problems. The online-based mental intervention has several advantages, such as being easily accessible, flexible time, suitable for any environment, and no direct involvement of the therapist is required, compared to being delivered in a face-to-face format. A meta-analysis during the Covid-19 pandemic demonstrated that online base mental intervention has been efficient in alleviating general anxiety, but the effects of different intervention methods were not reported. And the article pointed out that intervention methods may impact the long-term sustainability of intervention at the end (Kurniawan et al., 2022).
The two most commonly utilized mindfulness-based therapies, mindfulness-based stress reduction (MBSR) and mindfulness-based cognitive therapy (MBCT), successfully reduce problems with mental health. There is considerable evidence showing that mindfulness-based intervention has beneficial effects on stress, anxiety, and depression (Fischer et al., 2020). Given the efficacy of online mindfulness-based intervention before the Covid-19 outbreak, it may be worthwhile to investigate the efficacy of online mindfulness intervention as a potential alternative intervention during the Covid-19 pandemic may be as effective as before (Flett et al., 2018).
There is a recently published meta-analysis, which included 8 studies investigating the efficacy of the online mindfulness intervention on stress, anxiety, and depression (Witarto et al., 2022). This meta-analysis included studies that recruited adults and studies designed with RCT in the early Covid-19 pandemic, and thus fewer studies were included, and lack of the potential effect influencing factor. Although this meta-analysis provided a piece of valuable evidence that online MBIs have beneficial effects on mental health during the Covid-19 pandemic. Despite its limitations, the research discussed earlier support the intervention’s effectiveness. As a result, hypothesis 1 is proposed: During the epidemic, mindfulness online intervention programs have proven effective for stress, depression, and anxiety.
Some researchers argue that the acceptability of mindfulness interventions differs between the East and the West (Chen et al., 2012). Therefore, the geographical region of the participants may influence the effectiveness of mindfulness-based psychological therapy. As a result, hypothesis 2 is proposed: intervention in the East is better than intervention in the West. Furthermore, studies have shown that persons like cancer patients and pregnant women are more vulnerable to infection during an outbreak than the general population. Strict control measures, such as isolation, have a direct impact on the university and people in the community (Vione & Kotera, 2023; Weis et al., 2021). As a result, the effect of intervention might differ by group (Chiesi et al., 2022; Güney et al., 2022; Smith et al., 2021). We propose hypothesis 3 based on this: there is a difference in the intervention effects of college students, community residents, and clinical samples. Aside from area and sample type, a variety of factors have been demonstrated to influence the effectiveness of mental health interventions. According to Kabat-Zinn, cultivating mindfulness is similar to strengthening muscles (Kabat-Zinn, 2003). The medical term “dose” was coined by researchers in the realm of mental health research to denote “the number and intensity of exercises received.“ The degree of mindfulness education and practice in a mindful mental intervention is commonly characterized as the dose. As a result, the dose is a concern in mindfulness intervention research (Strohmaier, 2020). Therefore, we propose hypothesis 4: dose significantly modifies the intervention effect. Furthermore, as people age, cognitive function decline affects the level of mindfulness in the elderly, and hence the effect of psychological intervention on them (de Frias & Whyne, 2015). The epidemic’s health hazard will generate panic and worry among the elderly (Smith et al., 2020), which may lead to the elderly dealing with negative emotions in a confrontational manner. As a result, we suggest Hypothesis 5: age can significantly regulate the intervention effect. Finally, most researchers agree that women are more likely than men to experience negative emotions (Liu et al., 2020; Wenham et al., 2020). And gender variations in intervention effects are frequently studied by researchers (Smit & Stavrulaki, 2021; Wang & Chopel, 2017). Therefore, we suggest Hypothesis 6: The intervention impact is strongly moderated by gender. In this study, we focused on the influence of the following elements as moderating variables on the intervention effect based on the findings of previous studies and treatments.
In conclusion, the present meta-analysis focuses on the RCT during the overall Covid-19 pandemic, delivered non-face-to-face, on stress, anxiety, and depression in adults. The meta-analysis also explores identifying potential moderating factors that may influence the efficacy of the online mindfulness intervention (e.g., region, sample type, dose, age, and gender) to provide wider implications for psychological intervention management of major health events. The goal of this study also is to give a practical reference for future psychological interventions in significant health and safety emergencies.
Method
This meta-analysis followed the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Search strategies
Between December 1, 2022, and March 14, 2023, three electronic databases were searched (Web of Science, PubMed, and PsycINFO). Furthermore, two methods of collecting articles were used as extra information sources: hand searches on the reference list of relevant systematic reviews or meta-analyses, and supplemented papers in Google Scholar.
Search terms were used for online mindfulness intervention (online mindfulness intervention OR mindfulness-based intervention OR online-based intervention), psychological outcomes (mental health OR stress OR depression OR anxiety OR distress), the Covid-19 pandemic (Covid-19), and random controlled trial (RCT).
Selection study
A checklist was developed to facilitate the screening by the first author (FX). After eliminating duplicates, three authors (WZ, QC, and YT) evaluated each of the titles and abstracts and rejected 4140 articles in the first screening. After that, 98 articles were evaluated in the full-text screening stage independently by two authors (WZ and QC). WZ and QC coded with the “yes” and “no” for these articles and gave the excluded reason. Studies with a code of “yes” consistently underwent data extraction, while studies with a code of “no” consistently underwent removal. The first author determined whether to include the study based on the excluded reason was gave by the two coders if the two coders’ evaluations were different. The process records of the full-text screening were recorded and sorted by YT. The supplementary material contains more information on the selection study (Supplementary Table 1).
Inclusion criteria
The following criteria had to be met by the articles.
Population
Participants have to be at least 18 years old. Both college (e.g., young adult students), clinical (e.g., hospitalized people), and community (e.g., healthy population) populations were eligible.
Intervention
Participants were allocated to either the treatment or control condition at random. Mindfulness-based approaches are required to be included in treatment conditions and presented in a non-face-to-face format at the very least. Treatment conditions that used mindfulness-based techniques in conjunction with other treatments were also considered.
Comparator
Conditions that were both active and non-active and did not involve any mindfulness-based techniques were eligible.
Outcome
As one of the outcome measures, studies were required to report the intervention’s efficacy on stress, anxiety, and depression. These outcomes are required to be evaluated using a standardized measure that has been validated. Studies were also required to report on post-intervention outcomes. The article only included studies that were written in English and published in peer-reviewed publications.
Study design
Only randomized controlled trials were included, study protocol for a randomized controlled trial, mixed methods papers, and review papers were excluded from the meta-analysis.
Data extraction
The first author prepared the preliminary coding rules for the study purpose. The five articles included in the analysis were pre-coded following the preliminary coding rules by two authors (WZ and QC). And then the first author discussed with the two authors (WZ and QC) to determine the final coding rules. The last two authors formally coded all articles following the final coding rules. In general, the effect size of each article was coded only once; If more than one effect size was reported in the articles, multiple coding was performed. Two authors (WZ and QC) coded independently to ensure the accuracy of the coding of article information and data. It is important to note that we included the findings from two distinct studies that were published in two articles (Ahmad et al., 2020). We think that these studies were independent of one another and entered independently given the differences in intervention substance, trial implementation, and participants reported in the literature. The supplementary material contains the data analyzed finally (Supplementary Table 2).
Quality assessment tool
The study quality score we included was based on the risk of bias assessment tool recommended by the Cochrane Collaboration (Higgins & Green, 2019), including the following six aspects: (1) random assignment method; (2) The distribution scheme is hidden; (3) Blinding the study subjects, the implementors of the treatment plan, and the study outcome measure; (4) Data integrity; (5) selective reporting of research outcomes; (6) Additional sources of bias (Liu, 2011). For the aforementioned six aspects, assessments of “low” (low bias), “high” (high bias), and “unclear” (lack of relevant knowledge or uncertainty about bias) were made. The final score of each study was calculated. The standard was that the “low bias” of each item was 1 point, and the “high bias” and “unclear” were both 0 points.
The Cochrane Collaboration also provides a detailed explanation of the relevant risk of bias assessment criteria and three assessment levels (Higgins & Green, 2019). Following a full explanation by two separate authors, the methodological quality of the included studies was first reviewed (WZ and QC), and then the assessed reason of the two authors was given in every article (mark or highlight). Any disagreement was resolved through discussion by two authors (WZ and QC). To guarantee the accuracy of ratings, one author (YT) assessed the methodological quality of three randomly selected papers. The supplementary material contains more information on the quality assessment (Supplementary Table 3).
Data analysis
Publication bias of analysis
This analysis first looks at the distribution of literature in the funnel plot and then looks at the results of the Egger linear regression test to conclusively identify publication bias. We can see the effect size distribution of each study from the funnel plot, preliminarily check the literature with relatively asymmetric distribution, and discuss if it should be removed. The Egger linear regression test was also performed to examine the included literature for publication bias.
Synthesis analysis
The Comprehensive Meta-Analysis Version 3.3 (CMA 3.3) was used in this study for the meta-analysis (Borenstein et al., 2009). Due to the pre-and post-measurement data of the included literature in the included study. The measurements were taken before and after had a link. There will be bias if SMD is utilized as the effect size. As a result, this analysis used Hedges’s g. Hedges’s g was directly calculated by CMA 3.3. The heterogeneity analysis was evaluated using the Q and I2 indices. Given the possibility of high heterogeneity, a random effect model analysis was carried out.
Additional analysis
If the data were heterogeneous, the sources of heterogeneity were also investigated. Participants’ region and type (college, clinical, and community) were examined by subgroup analysis, and dose (length of the program), gender (the percentage of women), and age (the mean age of the participants) were examined by meta-regression. In addition, the Knapp-Hartung adjustment which is based on t distribution would reduce false positives in our analysis and was used in the meta-regression analysis to test our moderating variables if the analysis included a small number of effect sizes.
Results
Study characteristics
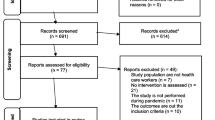
A total of 34 papers were identified as eligible for inclusion. Figure 1 shows the identification and screening process based on PRISMA guidelines. 17 studies documented the efficacy of stress, 28 studies documented the efficacy of anxiety and 18 research that documented the efficacy of depression. Table 1 shows the characteristics of the included studies.
The 34 studies include a total of 4714 participants, ranging from 26 to 587. Most studies were conducted in Asia (n = 14), followed by North America (n = 11) and Europe (n = 9). 50% of studies that included 2 studies’ participant was graduate student recruited college student as their participant (n = 17), 9 studies recruited healthy people and 8 studies’ participant is patient. The average age of the participants was reported in 32 studies. In ten studies, the average age of the participants was between 18 and 25 years, while in only one study, the average age was 58.2 recruited older adults. In the majority of studies (n = 27), women made up more than half of the participants. In a word, the most participants in the analysis were college females living in Asia and North America.
The dose was described in 33 studies, ranging from 1 day to 26 weeks, and most interventions took place over 4 weeks or 8 weeks. Most sessions took place once a week. 19 interventions were delivered in groups, and 32% of interventions had homework after the intervention. Therefore, the majority of the format utilized were group-delivered weekly, with no homework, taking place 4 weeks or 8 weeks.
The most of included studies utilized a non-active control group (n = 30), and it included waitlist control (n = 21), treat as usual (n = 9). 17 studies reported the efficacy of stress. Most studies used the Perceived Stress Scale (PSS), while others study used Depression, Anxiety, and Stress Scale (DASS). 28 studies reported the efficacy of anxiety. 8 different measures were used in included studies. Depression, Anxiety, and Stress Scale (DASS) (29%) was a commonly used measure in these studies, followed by Generalized Anxiety Disorder-7 (GAD-7) (21%). 18 studies reported the efficacy of depression. 7 different measures were used in included studies. Patient Health Questionnaire-9 (PHQ-9) (39%) was a commonly used measure in these studies, followed by Depression, Anxiety, and Stress Scale (DASS) (33%).

PRISMA flow diagram of the different phases of the meta-analysis
Methodological quality and risk of bias assessment
The quality of the studies included in the analysis varied. Therefore, before quantitative analysis, we conducted a quality assessment for each randomized controlled trial. For detailed information, see Supplementary Table 2. Ten of the studies were of low quality, scoring 1–2 points; By comparison, nine studies scored between 5 and 6. In each assessment item, the scoring rate of the blind method is low (only 12% for subjects and researchers, and 23.53% for results evaluation), while the scoring rate of the random allocation method is relatively high (79%), which may be due to researchers’ emphasis on the randomness of the experiment and the control group used in the literature (Fig. 2). On the contrary, the important indicators of randomized controlled trials such as blind method and assigned concealment are reported less.
Publication bias
In the analysis of stress, we first looked at the funnel plot, which showed that the distribution of effect size was more uniform, and the initial judgment was a small publication bias. The Egger linear regression test result was p = 0.102. The Egger linear regression test results larger than 0.05 indicates that there is no major publication bias in the study of pressure in this analysis.

Bias potential (presented by percentage across all included studies)
In the analysis of anxiety, we first looked at the funnel plot, which showed that the distribution of effect size was more uniform and the initial judgment was small publication bias. The Egger linear regression test result p = 0.110. The Egger linear regression test results larger than 0.05 indicates that there is no major publication bias in the study of anxiety in this analysis.
In the analysis of depression, we first looked at the funnel plot, in which the effect sizes were distributed asymmetrically, and the preliminary judgment was that there might be publication bias. The result of the Egger linear regression test was p = 0.001. Egger’s test result of less than 0.05 indicates that there may be major publication bias in the study on depression in this analysis. While much of the research included in the meta-analysis had small sample sizes, asymmetry may also be connected to the fact that there are fewer studies on depression.
Main results
Stress
The efficacy of the online mindfulness intervention on stress was documented in 17 studies. One study had two different test groups (both online mindfulness-based), resulting in 18 comparisons included in the meta-analysis. The effect size on stress was evaluated using a random effect model. Stress had a modest to big overall effect size (g = 0.278, p < 0.001; 95% CI = 0.119–0.437). The study effect sizes were highly heterogeneous (Q = 64.550, I2 = 73.664, p < 0.001).
Anxiety
The efficacy of the online mindfulness intervention on anxiety was documented in 28 studies. One study had two different test groups (both online mindfulness-based), resulting in 29 comparisons to be included in the meta-analysis. A random effect model was used to evaluate the effect size on anxiety. Anxiety had a modest to big overall effect size (g = 0.459, p < 0.001; 95% CI = 0.218-0.700). The study effect sizes were highly heterogeneous (Q = 317.467, I2 = 91.180, p < 0.001).
Depression
The efficacy of the online mindfulness intervention on depression was documented in 18 studies. One of those studies, which used two different test groups (both based on online mindfulness), led to the inclusion of 19 comparisons in the meta-analysis. The extent of the effect on depression was assessed using a random effect model. Depression had a modest to big overall effect size (g = 0.458, p < 0.001; 95% CI = 0.239–0.676). The study effect sizes were highly heterogeneous. (Q = 114.062, I2 = 84.219, p < 0.001).
Additional analysis
Stress regulation analysis
Subgroup analysis showed no significant differences in intervention effectiveness (p = 0.555) between North America (g = 0.322), Europe (g = 0.177), and Asia (g = 0.299). Intervention programs varied significantly (p = 0.026) among college students (g = 0.257), the community (g = 0.177), and the clinical population (g = 0.671). The study included a small clinical population, so the results should be interpreted with caution.
Meta-regression analysis showed that dose (β = 0.007, 95% CI = -0.025-0.040, SE = 0.015, p = 0.630), age (β = 0.001, 95% CI = -0.022-0.023, SE = 0.011, p = 0.956), and gender (β = -0.006, 95% CI = -0.021-0.009, SE = 0.007, p = 0.435) did not significantly regulate the effect of the intervention on stress.
Anxiety regulation analysis
Subgroup analysis revealed significant differences (p = 0.004) across regions. The intervention effect was the best in Asia (g = 0.956), followed by Europe (g = 0.487), and the least in North America (g = -0.052). However, there was no significant difference (p = 0.063) in the effectiveness of intervention among college students (g = 0.202), the community (g = 0.808), and the clinical population (g = 0.752).
Meta-regression analysis showed that dose (β = -0.110, 95% CI = -0.227-0.006, SE = 0.057, p = 0.063), age (β = 0.027, 95% CI = -0.014-0.067, SE = 0.020, p = 0.187) and gender (β = -0.021, 95% CI = -0.045-0.003, SE = 0.012, p = 0.081) did not significantly modulate the effect of the intervention on anxiety.
Depression regulation analysis
Similar to the results of the anxiety analysis, subgroup analysis showed significant differences (p = 0.038) across regions. The intervention effect was the best in Asia (g = 1.103), followed by Europe (g = 0.293), and the least in North America (g = 0.179). However, there was no significant difference (p = 0.055) in the effectiveness of intervention among college students (g = 0. 223), the community (g = 1.856), and the clinical population (g = 0.494).
Meta-regression analysis showed that neither dose (β = -0.083, 95% CI = -0.226-0.060, SE = 0.068, p = 0.236) nor age (β = 0.044, 95% CI = -0.002-0.089, SE = 0.022, p = 0.058) significantly moderated the effect of the intervention on anxiety. But gender (β = -0.029, 95% CI = -0.055–0.002, SE = 0.013, p = 0.036) is significantly moderated.
Discussion
Using a meta-analysis approach, the study investigated the efficacy of an online mindfulness intervention on stress, anxiety, and depression in adults. The analysis outcome indicated that online mindfulness intervention had a small effect on stress, a small to medium effect on anxiety, and a small to medium effect on depression. The analysis results confirm hypothesis 1. The study also looked into potential moderating factors that could affect the effectiveness of the online mindfulness intervention. In general, the findings support certain hypotheses 2, 4, and 6. The online mindfulness intervention was significantly effective different in different populations on stress, while these effects were no longer statistically significantly different for region, dose, age, and gender. The difference is that online mindfulness intervention was significantly effective different in different regions on anxiety, while these effects were no longer statistically significantly different for the sample type, dose, age, and gender. In contrast, the online mindfulness intervention was significantly effective different in different regions and gender on depression, while these effects were no longer statistically significantly different for the sample type, dose, and age.
The efficacy of the intervention in the current study is larger than the meta-analytic results from Spijkerman et al. (2016) on online mindfulness intervention for adults (anxiety, g = 0.22; depression, g = 0.29). It indicates that online mindfulness intervention may be a better way for people who were isolated during the pandemic. Furthermore, online mindfulness intervention can be a main delivery to assist psychological crisis intervention workers to deal with the mental health problems of isolated residents.
The research from Witarto et al. (2022) only included the articles that the intervention method was mindfulness-based interventions (MBIs), while the current study also included the articles that the intervention method was multiple component interventions. Therefore, the current study suggests that the intervention including mindfulness train can have a larger efficacy during the epidemic.
In the analysis of the overall model and publication bias of the 34 articles included, it was found that the effect size studied by Zhang et al. (2021) had a significant deviation. It is most likely since the actual sample size did not reach the sample estimate, that is, Zhang et al. reported that their minimum sample estimate was 84, while the actual sample size was 57. This may have impaction on the results to overestimate the actual treatment effect. As this study can be regarded as a small sample pilot study and there is no reasonable reason to exclude it, we ultimately decided to include the article. In addition, some of the included studies had small effect sizes (Kranenburg et al., 2022; Pheh et al., 2020; Rackoff et al., 2022; Sun et al., 2022). After reviewing the relevant articles, we found that most of these articles reported a high attrition rate in research. Although missing data are common in online intervention studies, missing data may impair data efficiency. Therefore, it is a particular concern in longitudinal and intervention studies. From the current study, we found that only two of these articles explicitly mentioned this limitation in their studies and provided their statistical treatment of this problem (Rackoff et al., 2022; Sun et al., 2022).
The results for anxiety and depression suggest that online interventions are still influenced by cultural differences. Analyses revealed that the Eastern intervention performed more effectively than the Western one. The finding suggests that the acculturation of mindfulness interventions still exists in online interventions during the pandemic. As a result, when utilizing mindfulness online intervention to deal with psychological crises in comparable occurrences in the future, greater thought should be paid to the locations from which the intervention objects emanate, as well as the cultural variations that they affect. Of course, improving online mindfulness psychotherapy programs to better serve people from different cultures and countries is an additional vital topic for clinical psychology researchers to address in the future.
The finding also suggests that online mindfulness interventions were effective in reducing anxiety and depression in college students (e.g., postgraduate students, young adult students, medical students), the community population (e.g., healthy people, nonclinical population, health care workers), or the clinical population (e.g., emotional disorder Patients, patients with fever, obstetrics and gynecology patients). It demonstrated that Online mindfulness interventions were effective in treating anxiety symptoms and depressive symptoms in broader populations. Mindfulness online intervention projects for similar events can be widely used in universities, communities, and hospitals to assist college mental health education teachers, community psychological intervention workers, and doctors in alleviating mental health problems caused by the epidemic and isolation measures.
These findings from the meta-analysis suggest that online mindfulness interventions can be effective during a pandemic. The results of this analysis further support that online mindfulness interventions are culturally influenced but can be universally applicable to different populations. To summarize, the online mindfulness intervention program has a small to moderate effect on the impact of the epidemic and isolation, and it can be used as an auxiliary means of psychological crisis intervention to assist psychological intervention workers in schools, communities, and hospitals in dealing with people’s mental health problems. It should be noted that the intervention effect differs by region. As a result, before employing the online mindfulness intervention program, psychological crisis intervention workers should consult the intervention effect report in the same region.
Limitations and future research
The study has some significant limitations. First, the most of participants in the meta-analysis were 60 or younger. One study looked into online mindfulness interventions for older adults (Herschel et al., 2022). Given the growing number of older adults worldwide, more research focusing on this population is required. Furthermore, the mean age of the participant included in the meta-analysis was under 60 years old. It may be indicated that online mindfulness intervention has an aged limit. The elderly are a vulnerable group in the pandemic. Future research should focus on testing the efficacy of older adults and developing online intervention programs tailored to their needs.
Second, the meta-analysis did not examine how the effects of an online mindfulness intervention varied according to participant income. The availability of online mindfulness is the advantage of online intervention, the psychological intervention was cost-effective and can be further considered (Witarto et al., 2022). However, it is not clear whether these findings in the meta-analysis can be generalized to people of different income levels. Therefore, focusing on the effect of online mindfulness intervention in low- and middle-income groups can be considered as a research question to be discussed in future analysis.
There are some limitations to comparing treatment characteristics in the meta-analysis that should be considered when interpreting the results. The online program allows the combination of different techniques into one intervention program. There may be differences in intervention effects between multicomponent programs and traditional single-technology programs. However, because the included studies’ research characteristics were reported inconsistently, further subgroup analysis was not possible in the study (e.g., session duration, the calculation method of the proportion of mindfulness technology in the project).
Finally, ethnicity during the pandemic may be a potential moderating variable that impacts the effect of psychological therapies, based on the study of area as a potential variable. However, because several of the studies included in this analysis failed to report participants’ ethnicity or were inconsistent in their representation, we did not examine this moderating variable.
Future studies can consider comparing the impact of differences in intervention content on intervention effectiveness, testing differences in intervention effectiveness between active and non-active intervention groups, and exploring whether the intervention effect persisted after a longer follow-up period. Finally, future research needs to focus more on improving the quality of research. The article should more clearly describe the method of allocation concealment, whether researchers and data evaluators are informed about the allocation scheme, and more specifically a statistical method for missing values.
Conclusion
The findings confirm the efficacy of an online mindfulness intervention to address stress, anxiety, and depression in adults during the Covid-19 pandemic. However, the intervention content of online intervention needs more exploration. More study is required to establish the efficacy of the online mindfulness intervention in low- and middle-income populations, as well as older adults. The future study also should improve the quality of research such as clearly describing the method of allocation concealment and more specifically statistical method for missing values.
Data availability
All data supporting the findings of this study are available within the paper and its Supplementary Information. Data are provided in Supplementary Table 2.
References
Ahmad, F., Morr, E., Ritvo, C., Othman, P., Moineddin, N., & Team, M. V. C. (2020). An eight-week, web-based mindfulness virtual community intervention for students’ mental health: Randomized controlled trial. JMIR Mental Health, 7(2), e15520. https://doi.org/10.2196/15520
Al-Alawi, M., McCall, R. K., Sultan, A., Al Balushi, N., Al-Mahrouqi, T., Ghailani, A., & Sinawi, A. (2021). Efficacy of a six-week-long therapist-guided online therapy versus self-help internet-based therapy for COVID-19-induced anxiety and depression: Open-label, pragmatic, randomized controlled trial. JMIR Mental Health, 8(2), e26683. https://doi.org/10.2196/26683
Alibak, F., & Alibak, M. (2021). Comparing online cognitive behavioural therapy versus online positive psychotherapy, well-being theory (PERMA) on test anxiety of online learning students: A randomised control study. Journal of the Australian and New Zealand Student Services Association, 29(1), 6–17.
Borenstein, M., Hedges, L. V., & Higgins, J. P. (2009). Introduction to meta-analysis. Wiley.
Catuara-Solarz, S., Skorulski, B., Estella-Aguerri, I., Avella-Garcia, C. B., Shepherd, S., Stott, E., & Dix, S. (2022). The efficacy of foundations, a digital mental health app to improve mental well-being during COVID-19: Proof-of-principle randomized controlled trial. JMIR Mhealth and Uhealth, 10(7), e30976. https://doi.org/10.2196/30976
Chen, K. W., Berger, C. C., Manheimer, E., Forde, D., Magidson, J., Dachman, L., & Lejuez, C. W. (2012). Meditative therapies for reducing anxiety: A systematic review and meta-analysis of randomized controlled trials. Depression and Anxiety, 29(7), 545–562. https://doi.org/10.1002/da.21964
Chiesi, F., Vizza, D., Valente, M., Bruno, R., Lau, C., Campagna, M. R., ... Bruno, F. (2022). Positive personal resources and psychological distress during the COVID-19 pandemic: Resilience optimism hope courage trait mindfulness and self-efficacy in breast cancer patients and survivors Abstract. Supportive Care in Cancer, 30(8), 7005–7014. https://doi.org/10.1007/s00520-022-07123-1
Dai, L. L., Wang, X., Jiang, T. C., Li, P. F., Wang, Y., Wu, S. J., Cheng, Z., Dai, L.-L., Wang, Xi., Jiang, T.-C., Li, P.-F., Wang, Yu., Wu, S.-J., Jia, L.-Q., Liu, M., An, L., & Cheng, Z. (2020). Anxiety and depressive symptoms among COVID-19 patients in Jianghan Fangcang Shelter Hospital in Wuhan, China. PLoS ONE, 15(8), e0238416. https://doi.org/10.1371/journal.pone.0238416
de Frias, C. M., & Whyne, E. (2015). Stress on health-related quality of life in older adults: the protective nature of mindfulness. Aging & Mental Health, 19(3), 201-206. doi: 10.1080/13607863.2014.924090
Devillers-Reolon, L., Mascret, N., & Sleimen-Malkoun, R. (2022). Online mindfulness intervention, mental health and attentional abilities: A randomized controlled trial in university students during COVID-19 lockdown. Frontiers in Psychology, 13, 889807. https://doi.org/10.3389/fpsyg.2022.889807
Dorais, S., & Gutierrez, D. (2021). The effectiveness of a centering meditation intervention on college stress and mindfulness: A randomized controlled trial. Frontiers in Psychology, 12, 720824. https://doi.org/10.3389/fpsyg.2021.720824
El Morr, C., Ritvo, P., Ahmad, F., Moineddin, R., & Team, M. V. C. (2020). Effectiveness of an 8-week web-based mindfulness virtual community intervention for university students on symptoms of stress, anxiety, and depression: Randomized controlled trial. JMIR Mental Health, 7(7), e18595. https://doi.org/10.2196/18595
Fiol-DeRoque, M. A., Serrano-Ripoll, M. J., Jimenez, R., Zamanillo-Campos, R., Yanez-Juan, A. M., Bennasar-Veny, M., Ricci-Cabello, I., Fiol-DeRoque, M. A., Serrano-Ripoll, M. J., Jiménez, R., Zamanillo-Campos, R., Yáñez-Juan, A. M., Bennasar-Veny, M., Leiva, A., Gervilla, E., García-Buades, M. E., García-Toro, M., Alonso-Coello, P., Pastor-Moreno, G., … Ricci-Cabello, I. (2021). A mobile phone-based intervention to reduce mental health problems in health care workers during the COVID-19 pandemic (PsyCovidApp): Randomized controlled trial. JMIR mHealth and uHealth, 9(5), e27039. https://doi.org/10.2196/27039
Fischer, R., Bortolini, T., Karl, J. A., Zilberberg, M., Robinson, K., Rabelo, A., Mattos, P., Fischer, R., Bortolini, T., Karl, J. A., Zilberberg, M., Robinson, K., Rabelo, A., Gemal, L., Wegerhoff, D., Nguyễn, T. B. T., Irving, B., Chrystal, M., & Mattos, P. (2020). Rapid Review and Meta-Meta-Analysis of Self-Guided interventions to address anxiety, Depression, and stress during COVID-19 Social Distancing. Frontiers in Psychology, 11, 563876. https://doi.org/10.3389/fpsyg.2020.563876
Flett, J. A. M., Hayne, H., Riordan, B. C., Thompson, L. M., & Conner, T. S. (2018). Mobile mindfulness meditation: A randomised controlled trial of the effect of two popular apps on mental health. Mindfulness, 10(5), 863–876. https://doi.org/10.1007/s12671-018-1050-9
French Public Health Agency (2021). CoviPrev: une enquête pour suivrel’évolution des comportements et de la santé mentale pendant l’épidémiede COVID-19. Retrieved from https://www.santepubliquefrance.fr/etudes-etenquetes/coviprev-une-enquete-pour-suivre-l-evolution-des-comportementset-de-la-sante-mentale-pendant-l-epidemie-de-covid-19#block-249162. Accessed 28 Feb 2022.
Güney, E., Cengizhan, S. O., Karatas Okyay, E., Bal, Z., & Ucar, T. (2022). Effect of the mindfulness-based stress reduction program on stress, anxiety, and childbirth fear in pregnant women diagnosed with COVID-19. Complementary Therapies in Clinical Practice, 47, 101566. https://doi.org/10.1016/j.ctcp.2022.101566
Herschel, E., Hennessy, S., Cahn, B. R., Goldsworthy, R., & Habibi, A. (2022). Effects of online choir or mindfulness interventions on auditory perception and well-being in middle- and older-aged adults during the COVID-19 pandemic: A randomized controlled trial. Music and Science, 5, 205920432211405. https://doi.org/10.1177/20592043221140524
Higgins, J. P., & Green, S. (2019). Cochrane handbook for systematic reviews of interventions. Wiley.
Hoover, E. B., Butaney, B., Bernard, K., Coplan, B., LeLacheur, S., Straker, H., LaRue, A., Hoover, E. B., Butaney, B., Bernard, K., Coplan, B., LeLacheur, S., Straker, H., Carr, C., Blesse-Hampton, L., Naidu, A., & LaRue, A. (2022). Comparing the effectiveness of virtual and in-person delivery of mindfulness-based skills within healthcare curriculums. Medical Science Educator, 32(3), 627–640. https://doi.org/10.1007/s40670-022-01554-5
Hosseinzadeh Asl, N. R. (2021). A randomized controlled trial of a mindfulness-based intervention in social workers working during the COVID-19 crisis. Current Psychology, 1–8. https://doi.org/10.1007/s12144-021-02150-3
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past present and future. Clinical Psychology: Science and Practice, 10(2), 144–156. https://doi.org/10.1093/clipsy.bpg016
Kam, J. W. Y., Javed, J., Hart, C. M., Andrews-Hanna, J. R., Tomfohr-Madsen, L. M., & Mills, C. (2022). Daily mindfulness training reduces negative impact of COVID-19 news exposure on affective well-being. Psychological Research Psychologische Forschung, 86(4), 1203–1214. https://doi.org/10.1007/s00426-021-01550-1
Komariah, M., Ibrahim, K., Pahria, T., Rahayuwati, L., & Somantri, I. (2022). Effect of mindfulness breathing meditation on depression, anxiety, and stress: A randomized controlled trial among university students. Healthcare, 11(1), 26. https://doi.org/10.3390/healthcare11010026
Kranenburg, L. W., Gillis, J., Mayer, B., & Hoogendijk, W. J. G. (2022). The effectiveness of a nonguided mindfulness app on perceived stress in a nonclinical dutch population: Randomized controlled trial. JMIR Mental Health, 9(3), e32123. https://doi.org/10.2196/32123
Kurniawan, K., Yosep, I., Maulana, S., Mulyana, A. M., Amirah, S., Abdurrahman, M. F., Rahayuwati, L., Kurniawan, K., Yosep, I., Maulana, S., Mulyana, A. M., Amirah, S., Abdurrahman, M. F., Sugianti, A., Putri, E. G., Khoirunnisa, K., Komariah, M., Kohar, K., & Rahayuwati, L. (2022). Efficacy of online-based intervention for anxiety during COVID-19: A systematic review and meta-analysis of randomized controlled trials. Sustainability, 14(19), 12866. https://doi.org/10.3390/su141912866
Li, Y., Zhang, A. J., Meng, Y., Hofmann, S. G., Zhou, A. Y., & Liu, X. H. (2023). A randomized controlled trial of an online self-help mindfulness intervention for emotional distress: Serial mediating effects of mindfulness and experiential avoidance. Mindfulness. https://doi.org/10.1007/s12671-023-02083-x
Liang, L., Feng, L., Zheng, X., Wu, Y., Zhang, C., & Li, J. (2021). Effect of dialectical behavior group therapy on the anxiety and depression of medical students under the normalization of epidemic prevention and control for the COVID-19 epidemic: A randomized study. Annals of Palliative Medicine, 10(10), 10591–10599. https://doi.org/10.21037/apm-21-2466
Liu, M. (2011). Systematic review, meta-analysis design and implementation methods. Beijing: People's Medical Publishing House.
Liu, N., Zhang, F., Wei, C., Jia, Y., Shang, Z., Sun, L., ... Liu, W. (2020). Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Research, 287,112921. 10.1016/j.psychres.2020.112921
Liu, Y., Huyang, S., Tan, H., He, Y., Zhou, J., Li, X., Wu, D., Liu, Y., Huyang, S., Tan, H., He, Y., Zhou, J., Li, X., Ye, M., Huang, J., & Wu, D. (2021). Using mindfulness to reduce anxiety and depression of patients with fever undergoing screening in an isolation ward during the COVID-19 outbreak. Frontiers in Psychology, 12, 664964. https://doi.org/10.3389/fpsyg.2021.664964
Mirabito, G., & Verhaeghen, P. (2022). Remote delivery of a koru mindfulness intervention for college students during the COVID-19 pandemic. Journal of American College Health, 1–8, 1–8. https://doi.org/10.1080/07448481.2022.2060708
Pheh, K. S., Tan, H. C., & Tan, C. S. (2020). Effects of an ultra-brief online mindfulness-based intervention on mental health during the coronavirus disease (COVID-19) outbreak in Malaysia: A randomized controlled trial. Makara Human Behavior Studies in Asia, 24(2). https://doi.org/10.7454/hubs.asia.2140920
Rackoff, G. N., Fitzsimmons-Craft, E. E., Taylor, C. B., Eisenberg, D., Wilfley, D. E., & Newman, M. G. (2022). A randomized controlled trial of internet-based self-help for stress during the COVID-19 pandemic. Journal of Adolescent Health, 71(2), 157–163. https://doi.org/10.1016/j.jadohealth.2022.01.227
Ritvo, P., Ahmad, F., El Morr, C., Pirbaglou, M., Moineddin, R., & Team, M. V. C. (2021). A mindfulness-based intervention for student depression, anxiety, and stress: Randomized controlled trial. JMIR Mental Health, 8(1), e23491. https://doi.org/10.2196/23491
Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Khaledi-Paveh, B., Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Rasoulpoor, S., & Khaledi-Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Globalization and Health, 16(1), 57. https://doi.org/10.1186/s12992-020-00589-w
Serrat, M., Coll-Omana, M., Albajes, K., Sole, S., Almirall, M., Luciano, J. V., & Feliu-Soler, A. (2021). Efficacy of the FIBROWALK multicomponent program moved to a virtual setting for patients with fibromyalgia during the COVID-19 pandemic: A proof-of-concept RCT performed alongside the state of alarm in Spain. International Journal of Environmental Research and Public Health, 18(19), 10300. https://doi.org/10.3390/ijerph181910300
Shabahang, R., Aruguete, M. S., & McCutcheon, L. (2021). Video-based cognitive-behavioral intervention for COVID-19 anxiety: A randomized controlled trial. Trends Psychiatry Psychother, 43(2), 141–150. https://doi.org/10.47626/2237-6089-2020-0056
Shaygan, M., Yazdani, Z., & Valibeygi, A. (2021). The effect of online multimedia psychoeducational interventions on the resilience and perceived stress of hospitalized patients with COVID-19: A pilot cluster randomized parallel-controlled trial. BMC Psychiatry, 21(1), 93. https://doi.org/10.1186/s12888-021-03085-6
Simonsson, O., Bazin, O., Fisher, S. D., & Goldberg, S. B. (2021). Effects of an eight-week, online mindfulness program on anxiety and depression in university students during COVID-19: A randomized controlled trial. Psychiatry Research, 305, 114222. https://doi.org/10.1016/j.psychres.2021.114222
Smit, B., & Stavrulaki, E. (2021). The efficacy of a mindfulness-based intervention for college students under extremely stressful conditions. Mindfulness, 12(12), 3086–3100. https://doi.org/10.1007/s12671-021-01772-9
Smith, M. L., Steinman, L. E., & Casey, E. A. (2020). Combatting social isolation among older adults in a time of physical distancing: The COVID-19 social connectivity paradox. Frontiers in Public Health, 8. https://doi.org/10.3389/fpubh.2020.00403
Smith, R. B., Mahnert, N. D., Foote, J., Saunders, K. T., Mourad, J., & Huberty, J. (2021). Mindfulness effects in obstetric and gynecology patients during the coronavirus disease 2019 (COVID-19) pandemic: A randomized controlled trial. Obstetrics & Gynecology, 137(6), 1032–1040. https://doi.org/10.1097/AOG.0000000000004316
Spijkerman, M. P., Pots, W. T., & Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clinical Psychology Review, 45, 102–114. https://doi.org/10.1016/j.cpr.2016.03.009
Strohmaier, S. (2020). The relationship between doses of mindfulness-based programs and depression anxiety stress and mindfulness: a dose-response meta-regression of randomized controlled trials. Mindfulness, 11(6), 1315–1335. https://doi.org/10.1007/s12671-020-01319-4
Sun, S., Lin, D., Goldberg, S., Shen, Z., Chen, P., Qiao, S., Operario, D., Sun, S., Lin, D., Goldberg, S., Shen, Z., Chen, P., Qiao, S., Brewer, J., Loucks, E., & Operario, D. (2022). A mindfulness-based mobile health (mHealth) intervention among psychologically distressed university students in quarantine during the COVID-19 pandemic: A randomized controlled trial. Journal of Counseling Psychology, 69(2), 157–171. https://doi.org/10.1037/cou0000568
Suranata, K., Ifdil, I., Gading, I. K., & Permana, A. A. J. (2021). Self-help online psychoeducation to overcome anxiety during covid-19 outbreak. COUNS-EDU: The International Journal of Counseling and Education, 6(1), 11–18. https://doi.org/10.23916/0020210634010
Vione, K. C., & Kotera, Y. (2023). Mindfulness-based approaches for COVID-19 mental health in working from home abstract. International Journal of Mental Health and Addiction, 21(2), 1132–1138. https://doi.org/10.1007/s11469-021-00647-3
Wang, W. L., & Chopel, T. (2020). Mindfulness and gender: A pilot quantitative study. Issues In Information Systems, 18(4), 105–115. https://doi.org/10.48009/4_iis_2017_105-115
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. https://doi.org/10.3390/ijerph17051729
Wei, N., Huang, B. C., Lu, S. J., Hu, J. B., Zhou, X. Y., Hu, C. C., & Hu, S. H. (2020). Efficacy of internet-based integrated intervention on depression and anxiety symptoms in patients with COVID-19. Journal of Zhejiang University-SCIENCE B (Biomedicine & Biotechnology), 21(5), 400–404. https://doi.org/10.1631/jzus.B2010013
Weis, R., Ray, S. D., & Cohen, T. A. (2021). Mindfulness as a way to cope with COVID-19-related stress and anxiety. Counselling and Psychotherapy Research, 21(1), 8–18. https://doi.org/10.1002/capr.12375
Wenham, C., Smith, J., & Morgan, R. (2020). COVID-19: the gendered impacts of the outbreak. The Lancet, 395(10227), 846-848. 10.1016/S0140-6736(20)30526-2
Witarto, B. S., Visuddho, V., Witarto, A. P., Bestari, D., Sawitri, B., Melapi, T. A. S., & Wungu, C. D. K. (2022). Effectiveness of online mindfulness-based interventions in improving mental health during the COVID-19 pandemic: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE, 17(9), e0274177. https://doi.org/10.1371/journal.pone.0274177
Xiong, Y. Y., Prasath, P. R., Zhang, Q. Y., & Jeon, L. (2022). A mindfulness-based well‐being group for international students in higher education: A pilot study. Journal of Counseling & Development, 100(4), 374–385. https://doi.org/10.1002/jcad.12432
Yildirim, D., & Ciris Yildiz, C. (2022). The effect of mindfulness-based breathing and music therapy practice on nurses’ stress, work-related strain, and psychological well-being during the COVID-19 pandemic: A randomized controlled trial. Holistic Nursing Practice, 36(3), 156–165. https://doi.org/10.1097/HNP.0000000000000511
Zhang, H., Zhang, A. A., Liu, C. B., Xiao, J., & Wang, K. P. (2021). A brief online mindfulness-based group intervention for psychological distress among chinese residents during COVID-19: A pilot randomized controlled trial. Mindfulness, 12(6), 1502–1512. https://doi.org/10.1007/s12671-021-01618-4
Funding
This study was supported by the National Natural Science Foundation of China (grant nos. 72,164,028 and 71,971,103).
Author information
Authors and Affiliations
Contributions
The original idea was provided and led by Fuming Xu. Wanling Zhu and Qian Chen searched and screened articles, input articles information, and extracted data. Youmei Tang collated and proofread the materials in this process. Wanling Zhu finishes the initial manuscript, Qian Chen proofreads it, and Fuming Xu finally revises it. All the authors contributed to the final manuscript.
Corresponding author
Ethics declarations
Ethical approval statement and informed consent
All analyses were based on previous published studies, thus no ethical approval and patient consent are required.
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Meta-analysis registration number: INPLASY202330103.
Supplementary Information
Supplementary Table 1
(XLSX 28.8 kb)
Supplementary Table 2
(XLSX 14.9 kb)
Supplementary Table 3
(XLSX 11.4 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xu, F., Zhu, W., Chen, Q. et al. Online mindfulness interventions for improving people’s mental health during the COVID-19 pandemic: a meta-analysis of randomized controlled trials. Curr Psychol 43, 17751–17765 (2024). https://doi.org/10.1007/s12144-023-05188-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-023-05188-7