
Abstract
Emotion dysregulation is considered a central feature of gambling disorder. However, research has mainly focused on the examination of the role played by negative emotional states, neglecting processes related to positive emotionality. Recently, some authors developed a useful tool to measure dysregulation of positive emotions, the Difficulties in Emotion Regulation Scale-Positive (DERS-P), which has been successfully used in a study investigating substance use disorder. The role played by dysregulation of positive emotions in gambling disorder was investigated in order to bridge the gap in the literature. We administered the Impulsive Behavior Scale Short Form (UPPS-P) and the DERS-P to a sample of disordered gamblers (n = 95) using the South Oaks Gambling Screen (SOGS) as well as group of non-gamblers or non disordered gamblers (n = 105). We found that disordered gamblers, compared to controls, scored higher on the negative and positive urgency subscale of the UPPS-P as well as on the impulse and non-acceptance subscales of the DERS-P. Moreover, these scales positively correlated with the severity of gambling disorder. However, in a unique model of multiple regression analysis, only the positive urgency dimension was a significant predictor of the SOGS scores. Dysregulation of positive emotions seems to be involved in gambling disorder. Specifically, our study suggested that the difficulty to accept positive emotional states in non-judgmental way accounts for the disorder. However, the proneness to act rashly under the influence of positive emotional states appears to be the stronger predictor of gambling disorder severity in this sample.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gambling is considered a leisure activity by a majority of people who occasionally gamble without it having a negative impact on their well-being (Pallanti and Salerno 2014). However, the number of cases of Gambling Disorder (GD) has exponentially grown in the last 20 years, sufficient to endorse a greater empirical and clinical focus on this condition. Calado and Griffiths (2016) estimate that from 0.1% to 5–8% of people from five continents meet the criteria to receive a diagnosis of GD. The DSM5 defines GD as “Persistent and recurrent problematic gambling behavior,” identifying impulsivity, loss of control and chasing as the core of this pathology (APA - American Psychiatric Association 2013).
The motivations that lead to the development and persistence of the disorder remain unclear. In line with the principle of equifinality, people who develop an addiction do not do it for the same reasons (Suissa 2011). Blaszczynski and Nower (2002) move in this direction with the formulation of the pathways model. In their influential pathways model, they hypothesize the existence of three subgroups of disordered gamblers (i.e. individuals suffering from GD): behaviorally conditioned problem gamblers, emotionally vulnerable problem gamblers and antisocial impulsivist problem gamblers. This schema is partially similar to Lesieur’s (2001) distinction between escape seekers and action seekers. The first subgroup gambles to avoid negative affect, the second does so to reach psychophysiological activation whereas the group of behaviorally conditioned disordered gamblers of Blaszczynski and Nower would not suffer from difficulties to cope with emotional states. Interestingly, both models, in addition to ecological variables, cognitive and personality factors, indirectly consider failures in Emotion Regulation (ER) as a key aspect of GD (Rogier and Velotti 2018a).
Gratz and Roemer (2004) suggest an integrative conceptualization of ER that involves not just the modulation of emotions but also their awareness, understanding and acceptance and the capacity to act in a finalized manner regardless of emotional arousal. Research recently highlighted that diverse symptom presentations are related to emotion dysregulation (Dryman 2018; Dimaggio et al. 2017; Garofalo et al. 2018; Velotti et al. 2017a, b). From a meta-analytic review (Aldao et al. 2010), considering the co-occurrence of psychiatric conditions with GD (Dryman 2018; Hellberg et al. 2018), emerged a significant effect size for a wide range of maladaptive ER strategies. Considering this evidence, Rogier and Velotti (2018a) suggested that actual deficits of ER processing affect disordered gamblers (DGs) in different ways and different moments of the ER timeline. They also hypothesize that dysregulation of positive emotions plays a key role in GD. Nevertheless, the association between dysregulation of positive emotions and GD is neglected by most of GD and ER studies, which more often have shown a significant correlation between dysregulation of negative emotions and GD (e.g., Atkinson et al. 2012; Daughters et al. 2005; Navas et al. 2017; Rogier and Velotti 2018b).
Dysregulation of positive emotions has increasingly been associated with psychopathology, but this relationship remains unclear (Carl et al. 2013; Hechtman et al. 2013). Recently, literature highlighted that the tendency to behave impulsively under intense positive emotional states (Cyders and Smith 2008a, b) predicts maladaptive behaviors such as substance-related abuse and risky sexual behavior (Zapolski et al. 2009).
Although some personality traits related to frequent experiences of positive emotions are associated with high levels of well-being (Caprara et al. 2017; Catalino et al. 2014; Lauriola and Iani 2017), positive emotional states have been noted to naturally elicit a drive to action (Fredrickson 1998). In that sense, it may be asserted that a difficulty to adequately manage positive emotions may lead to an excessive persistence of pleasant activities such as gambling. For instance, Cummins et al. (2009) found that winning and positive affect can lead to reckless gambling. Similarly, some authors tested the hypothesis that a proneness to act impulsively in response to positive emotional states is associated with GD. For this purpose, the positive urgency construct (Cyders and Smith 2008a) was used in an attempt to integrate Whiteside and Lynam’s (2001) multidimensional model, which included four distinct traits: negative urgency, sensation seeking, premeditation, and perseverance. This theoretical effort led to a revised version of the model, adding a fifth subscale measuring levels of positive urgency. Results obtained using the Impulsive Behavior Scale (UPPS), derived from the model, have been promising. To date, six studies (Cyders and Smith 2008a, b; Kim et al. 2019; Lutri et al. 2018; Savvidou et al. 2017; Steward et al. 2017) that have explored the correlations between scores obtained on the positive urgency subscale and measures of GD’s severity and only two did not find significant relationships (Lutri et al. 2018; Steward et al. 2017). Results of studies that compared groups of DGs with groups of community participants are more homogenous, observing higher levels of positive urgency among DGs (Albein-Urios et al. 2012; Boothby et al. 2017; Cyders and Smith 2008a; Michalczuk et al. 2011). Finally, studies that tested the predictive role of this factor on GD’s severity, controlling for the others dimensions, converge in the observation of a positive and significant effect (Blain et al. 2015; Canale et al. 2017; Haw 2017) with an unique exception (Savvidou et al. 2017).
Regarding Negative Urgency, in an excellent meta-analysis MacLaren et al. (Maclaren et al. 2011) adopted the original multidimensional model of impulsivity to analyze results towards the relationship between NU and GD. It was found that the NU facet was the most discriminative UPPS dimension that differentiated between groups of Disordered Gamblers and controls. This observation has been successively supported by studies using the UPPS (Boothby et al. 2017; Cyders et al. 2014; Kräplin et al. 2014; Albein-Urios et al. 2012; Billieux et al. 2012; Michalczuk et al. 2011). Also, data brought by this line of recent research has frequently shown that Negative Urgency is a significant predictor of GD’s severity (Blain et al. 2015; Haw 2017; Cyders and Smith 2008a, b; Whiteside et al. 2005).
However, existing research are yet to exhaustively investigate the relationship between different facets of dysregulation of positive emotions and addictions, with a focus on the role of positive urgency. Indeed, some other domains of this complex construct have been neglected in previous research such as the difficulty to accept positive emotional states non-judgmentally and a difficulty to engage in a goal-directed behavior when experiencing positive emotions (Weiss et al. 2015). These very recent lines of research were explored by Weiss and colleagues in relation to drug and alcohol use among community participants (Weiss et al. 2018, 2019). Specifically, the authors argued for a role of non-acceptance of positive emotions for two reasons. Some individuals may negatively judge their own positive emotional states, not accepting them, while others may want to avoid arousal related to positive emotions, experienced as distress. Hence, such individuals may use alcohol or drugs in an attempt to alleviate or distract themselves from positive emotions, which is perceived as an aversive state. Moreover, Weiss et al. (2018) found significant and positive associations between non-acceptance of positive emotions and both alcohol addiction and drug misuse. To our knowledge, no previous studies have investigated this topic in the field of GD; however, some data, evidencing a link between dampening of positive emotions and GD’s severity (Rogier and Velotti 2018b), suggest that Weiss et al.’s (2018) conclusions may be valid also among DGs.
Moreover, difficulties engaging in goal-directed behaviors when experiencing positive emotions have been thought to lead to substance misuse because of increased distractibility, impaired decision-making with an interference in the pursuit of long-term goals, and proneness to use immediate rewards as an escape-based strategy (Weiss et al. 2018). In this sense, qualitative material highlighted that stories of DGs are characterized by a difficulty to pursue long-term social achievements and a preference for short-term rewarding activities such as gambling (Rogier et al. 2019). Indeed, Weiss et al.’s (2018) preliminary findings evidenced a positive association between this facet of dysregulation of positive emotions and substance use disorders among community participants.
The relationship between emotion dysregulation and impulsivity is hard to disentangle and still a matter of debate. This may be partially due to the multidimensional nature of both constructs. To consider the impulsiveness feature throughout a cognitive perspective stresses the differences between the two constructs. The cognitive components of impulsivity (e.g. difficulties to plan consequences of own behavior or to persevere in goal directed behavior) do not appear necessarily connected to a difficulty to moderate emotional responses. In contrast, the Urgency facet of impulsivity appears to greatly overlap with the Impulse dimension of Emotion Dysregulation. Actually, both features refer to a central loss of control over own behavior while experiencing intense emotional arousal. Focusing on the topic of positive emotions, the items comprising to the Positive Urgency subscale and the Impulse subscale of the DERS-P shed light on this similarity. However, The Positive Urgency items measure additional components related to the proneness to impulsively react to positive emotions. For instance, in addition to a loss of control over behavior, these items stress the difficulty to plan for consequences of ones own behavior while experiencing positive emotions as such as the proneness to use up-regulation strategies in response to positive emotional states (Cyders and Smith 2008a). Last but not least, a central difference between these two operationalization of emotional impulsivity is that the DERS-P only refers to the happiness emotional states while the Positive Urgency’s items also refer to a generic emotional state of excitement.
In light of the existing gaps in current literature, this study primarily aimed to investigate the role played by different dimensions of dysregulation of positive emotions in GD. Throughout the cross-sectional study, we aimed to test the following hypotheses:
-
H1 DGs, compared to a group of community participants, will score higher on the measures of dysregulation of positive emotions.
-
H2 All dimensions of dysregulation of positive emotions will be positively and significantly related to gambling severity.
-
H3 In addition to positive urgency, the other dimensions of dysregulation of positive emotions will positively and significantly predict gambling severity.
Material and Methods
Participants
The study was comprised of a total of 206 Italian adults. The clinical group (n = 99; Mage = 47.61 years, SD = 12.97; 83.8% males) included DGs with a clinician-based current diagnosis using an interview based on the DSM-5 criteria. The participants were recruited in three clinical centers specialized in GD treatment all located in center of XXX.
The community group (n = 105; Mage = 46.88 years, SD = 10.08; 71.4% males) was drawn from the general population, and all participants were recruited using a purposive sampling technique (i.e. recruiting a major proportion of males who were over the age of 18).
Measures
Demographic Information
such as gender and age were asked using two questions (e.g. “What is your gender?”; “Please indicate your age in years”) in an initial questionnaire created for the study.
Severity of GD and Information Related to Gambling Activity
We used the SOGS (Lesieur and Blume 1987; Guerreschi and Gander 2002), a self-report questionnaire that evaluates the severity of GD, summing the score obtained on 20 specific items. The instrument also provides complementary information related to the frequency of involvement in different types of gambling activity. In our study, the reliability of such an instrument was confirmed with a Cronbach’s alpha reaching .94.
Impulsive Behavior
We used the UPPS-P (Whiteside and Lynam 2001; D'Orta et al. 2015), which is a 20-item self-report instrument that uses a 4-point Likert scale ranging from 1 (“Totally agree”) to 4 (“Totally disagree”). In the first development of the UPPS, four factors were extracted namely lack of premeditation, negative urgency, lack of perseverance and sensation-seeking. Each subscale contains 10 to 12 items. A revised version of the scale, the UPPS-P (Lynam et al. 2007), also includes positive urgency as distinct from the already-existing negative urgency scale. In our study, Cronbach’s alphas ranged from .72 (Lack of Premeditation subscale) to .87 (Total Score), indicating a good reliability.
Dysregulation of Positive Emotion
We used the DERS-P (Weiss et al. 2015; Velotti et al. 2020), which is a 15-item self-report measure developed to assess clinically relevant difficulties in the regulation of positive emotions. This measure was developed from the original DERS (Gratz and Roemer 2004), with items modified to assess difficulties generated by the experience of positive emotions (vs. negative emotions). Rather than beginning with the phrase “When I’m upset” like many of the original DERS items, the DERS-Positive items begin with the phrase “When I’m happy.” DERS-Positive items reflect difficulties within the following subscale of ER: (a) acceptance of positive emotions (Non acceptance); (b) ability to engage in goal-directed behavior when experiencing positive emotions (Goals); and (c) ability to control impulsive behaviors when experiencing positive emotions (Impulse). Participants are asked to indicate how often the items apply to themselves, with responses ranging from 1 (“Almost never”) to 5 (“Almost always”). Higher scores indicate greater difficulties in the regulation of positive emotions. In our study, the instrument demonstrated excellent reliability with a Cronbach coefficient ranging from .82 (Goals) to .92 (DERS-P Total score).
Procedure
This study’s aims and scopes as well as information on privacy and anonymity were briefly discussed to participants before the procedure. Participants then gave written consent. Finally, participants were asked to complete self-report questionnaires under the supervision of a psychologist. All procedures complied with the official directions established by the American Psychological Association and were approved by the Research Ethic Board of the Sapienza University of Rome.
Results
Differences between groups
First, a t-test for independent samples was conducted and revealed that the control and clinical group did not differ for age (p = .650). Similarly, a Chi-squared test revealed that groups did not differ on gender composition (p = .160).
Subsequently, we performed a multivariate analysis of variance showing that DGs scored significantly higher on the negative and positive urgency subscale of the UPPS-P as well as on the impulse and non-acceptance subscales of the DERS-P compared to the control group. These results have been displayed in Table 1.
Predictors of GD Severity
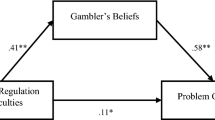
Results of bivariate correlations are displayed in Table 2. We found that GD severity was significantly correlated with the difficulty to control impulsive behavior when experiencing positive emotions (r = .16, p < .05) and with the difficulty to accept positive emotions (r = .14, p < .05). Finally, we aimed to identify the strongest predictors of GD severity. In line with this purpose, we performed a multiple linear regression entering variables significantly correlated with GD severity. As the positive urgency subscale of the UPPS-P and the impulse subscale of the DERS-P were redundant (measuring the same construct), we decided to exclude the latter of the DERS-P from the current analysis. Results, as illustrated in Table 3, uncovered that only the positive urgency factor was a significant predictor of GD severity.
Discussion
The main goal of our study was to investigate the role of the regulation of positive emotions in GD. To date, literature on ER and GD has more often shown a significant correlation between dysregulation of negative emotions and GD (Daughters et al. 2005; Atkinson et al. 2012; Navas et al. 2017).
Impulsivity is a complex construct, and our aim was to further investigate which factors affect GD more than others. We found that DGs scored higher on both the negative and positive urgency subscales of the UPPS-P. Our results align with previous studies (Cyders and Smith 2008a, b; Zapolski et al. 2009) that provide evidence that positive and negative urgency are distinct from other dispositions toward rash action and that they predict behaviors such as alcohol consumption, binge eating, drug use, and risky sexual behavior. This finding should not be surprising since impulsivity has been considered one of the main features of GD (APA 2013a, b).
When we looked at other facets of dysregulation of positive emotions, we found that difficulty to accept positive emotions in non-judgmental way was significantly associated with GD severity and that DGs scored higher on this dimension compared to controls. As discussed in the field of alcohol and drug misuse (Weiss et al. 2018, 2019), we may speculate that DGs may negatively judge their positive emotional states and/or avoid arousal related to positive emotions experienced as distressing throughout gambling activities. This converges with the conceptualization of gambling as a strategy to escape from aversive internal states.
However, we found that non-acceptance of positive emotions was no more a significant predictor of GD severity when controlling for the variance explained by positive urgency levels. This result, indicating the predominant role of impulsivity, should be interpreted with caution. Indeed, the pathways linking these two facets of dysregulation of positive emotions to GD may differ across subtypes of DGs. For instance, avoiding positive emotions throughout gambling may be characteristic of escape seekers while acting rashly when experiencing positive emotions may be associated with action seekers.
As a whole, our findings align with other researches highlighting the role of dysregulation of positive emotions in psychopathology (Cyders and Smith 2008a, b). Furthermore, our study supports and extends previous results about addiction, which are observed in community samples (Weiss et al. 2018, 2019), by assessing data from a clinical population.
Importantly, in line with the theoretical conceptualization of GD within the process model of ER (Rogier and Velotti 2018a; Sheppes et al. 2015), these findings support the idea that dysregulation of positive emotions contributes to the disorder. This study sheds light on the relevance of the difficulty to accept, in a non-judgmental way, positive emotional states. As asserted in the model, this difficulty would account for a failure in the identification step of the ER process.
Despite some important limitations (purposive sampling technique and absence of control variables such as alcohol and drug assumption), this study provides useful suggestions for future studies. For instance, as recently suggested, dysregulation of positive and negative emotions may not be independent (Rogier et al. 2019). Indeed, future studies should examine the possible interaction between these components or the existence of common mechanisms accounting for these similar impairments. Moreover, longitudinal research is necessary to understand the complex association between regulation of positive emotions and DG, evaluating the trajectory of the disorder. Researchers should investigate the control of impulsive behavior in conditions of emotional arousal, through specific laboratory tasks. Clinically, this line of research appears to be very promising for the future tailoring of psychological treatments on the mechanisms which contribute to GD.
References
Albein-Urios, N., Martinez-González, J. M., Lozano, Ó., Clark, L., & Verdejo-García, A. (2012). Comparison of impulsivity and working memory in cocaine addiction and pathological gambling: Implications for cocaine-induced neurotoxicity. Drug and Alcohol Dependence, 126(1–2), 1–6.
Aldao, A., Nolen-Hoeksema, S., & Schweizer, S. (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237.
APA - American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Atkinson, J., Sharp, C., Schmitz, J., & Yaroslavsky, I. (2012). Behavioral activation and inhibition, negative affect, and gambling severity in a sample of young adult college students. Journal of Gambling Studies, 28(3), 437–449.
Blain, B., Richard Gill, P., & Teese, R. (2015). Predicting problem gambling in Australian adults using a multifaceted model of impulsivity. International Gambling Studies, 15(2), 239–255.
Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and pathological gambling. Addiction, 97, 487–499.
Boothby, C. A., Kim, H. S., Romanow, N. K., Hodgins, D. C., & McGrath, D. S. (2017). Assessing the role of impulsivity in smoking & non-smoking disordered gamblers. Addictive Behaviors, 70, 35–41.
Billieux, J., Rochat, L., Ceschi, G., Carré, A., Offerlin-Meyer, I., Defeldre, A-C., Khazaal, Y., Besche-Richard, C., Van der Linden, M. (2012). Validation of a short French version of the UPPS-P Impulsive Behavior Scale. Comprehensive Psychiatry, 53(5), 609–615.
Calado, F., & Griffiths, M. D. (2016). Problem gambling worldwide: An update and systematic review of empirical research (2000-2015). Journal of Behavioral Addictions, 5(4), 592–613.
Canale, N., Vieno, A., Bowden-Jones, H., & Billieux, J. (2017). The benefits of using the UPPS model of impulsivity rather than the big five when assessing the relationship between personality and problem gambling. Addiction, 112(2), 372–373.
Caprara, G. V., Eisenberg, N., & Alessandri, G. (2017). Positivity: The dispositional basis of happiness. Journal of Happiness Studies, 18(2), 353–371.
Catalino, L. I., Algoe, S. B., & Fredrickson, B. L. (2014). Prioritizing positivity: An effective approach to pursuing happiness? Emotion, 14(6), 1155–1161.
Cummins, L. F., Nadorff, M. R., & Kelly, A. E. (2009). Winning and positive affect can lead to reckless gambling. Psychology of Addictive Behaviors, 23(2), 287–294.
Cyders, M. A., & Smith, G. T. (2008a). Emotion-based dispositions to rash action: Positive and negative urgency. Psychological Bulletin, 134(6), 807–828.
Cyders, M. A., & Smith, G. T. (2008b). Clarifying the role of personality dispositions in risk for increased gambling behavior. Personality and Individual Differences, 45(6), 503–508.
Cyders, M. A., Littlefield, A. K., Coffey, S., & Karyadi, K. A. (2014). Examination of a short English version of the UPPS-P impulsive behavior scale. Addictive Behaviors, 39(9), 1372–1376.
Carl, J. R., Soskin, D. P., Kerns, C., Barlow, D. H. (2013). Positive emotion regulation in emotional disorders: a theoretical review. Clinical Psychology Review 33(3), 343–360. https://doi.org/10.1016/j.cpr.2013.01.003.
Daughters, S. B., Lejuez, C. W., Strong, D. R., Brown, R. A., Breen, R. B., & Lesieur, H. R. (2005). The relationship among negative affect, distress tolerance, and length of gambling abstinence attempt. Journal of Gambling Studies, 21(4), 363–378.
Dimaggio, G., Popolo, R., Montano, A., Velotti, P., Perrini, F., Buonocore, L., Garofalo, C., D’Aguanno, M., & Salvatore, G. (2017). Emotion dysregulation, symptoms and interpersonal problems as independent predictors of a broad range of personality disorders in an outpatient sample. Psychology and Psychotherapy: Theory, Research and Practice, 90(4), 569–599. https://doi.org/10.1111/papt.12126.
D'Orta, I., Burnay, J., Aiello, D., Niolu, C., Siracusano, A., Timpanaro, L., Khazaal, Y., & Billieux, J. (2015). Development and validation of a short Italian UPPS-P impulsive behavior scale. Addictive Behaviors Reports, 2, 19–22.
Dryman, M., T., (2018). The role of emotion regulation in the relationship between social anxiety and depression: a daily diary study. Dissertation Abstracts International: Section B: The Sciences and Engineering, Vol 80(1-B)(E) Publisher: ProQuest Information & Learning.
Fredrickson, B. L. (1998). What good are positive emotions? Review of General Psychology, 2(3), 300–319.
Garofalo, C., Velotti, P., & Zavattini. (2018). Emotion regulation and aggression: The incremental contribution of alexithymia, impulsivity, and emotion Dysregulation facets. Psychology of Violence, 8(4), 470–483.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54.
Guerreschi, C., & Gander, S. (2002). Versione Italiana del South Oaks Gambling Screen (SOGS) di H.R. Lesieur e S.B. Blume. In C. Guerreschi (Ed.), Giocati dal gioco (pp. 137–142). San Paolo: Quando il divertimento diventa una malattia: il gioco d’azzardo patologico Milano.
Haw, J. (2017). Impulsivity predictors of problem gambling and impaired control. International Journal of Mental Health and Addiction, 15(1), 154–165.
Hechtman, L. A., Raila, H., Chiao, J. Y., & Gruber, J. (2013). Positive emotion regulation and psychopathology: A transdiagnostic cultural neuroscience approach. Journal of Experimental Psychopathology, 4(5), 502–528.
Hellberg, S. N., Russell, T. I., & Robinson, M. J. (2018). Cued for risk: Evidence for an incentive sensitization framework to explain the interplay between stress and anxiety, substance abuse, and reward uncertainty in disordered gambling behavior. Cognitive, Affective, & Behavioral Neuroscience, 1-22.
Kim, H. S., Poole, J. C., Hodgins, D. C., McGrath, D. S., & Dobson, K. S. (2019). Betting to deal: Coping motives mediate the relationship between urgency and problem gambling severity. Addiction Research & Theory, 27(2), 95–103. https://doi.org/10.1080/16066359.2018.1455188.
Kräplin, A., Dshemuchadse, M., Behrendt, S., Scherbaum, S., Goschke, T., Bühringer, G. (2014). Dysfunctional decision-making in pathological gambling: Pattern specificity and the role of impulsivity. Psychiatry Research, 215(3), 675–682.
Lauriola, M., & Iani, L. (2017). Personality, positivity and happiness: A mediation analysis using a bifactor model. Journal of Happiness Studies, 18(6), 1659–1682.
Lesieur, H. R. (2001). Cluster analysis of types of inpatient pathological gamblers. Dissertation Abstracts International: Section B: The Sciences and Engineering, 62(4-B), 2065.
Lesieur, H. R., & Blume, S. B. (1987). The south oaks gambling screen (SOGS): A new instrument for the identification of pathological gamblers. The American Journal of Psychiatry, 144(9), 1184–1188.
Lutri, V., Soldini, E., Ronzitti, S., Smith, N., Clerici, M., Blaszczynski, A., & Bowden-Jones, H. (2018). Impulsivity and gambling type among treatment-seeking disordered gamblers: An explorative study. Journal of Gambling Studies, 34(4), 1341–1354.
Lynam, D., Smith, G. T., Cyders, M. A., Fischer, S., & Whiteside, S. A. (2007). The UPPS-P: A multidimensional measure of risk for impulsive behavior. Unpublished technical report.
Michalczuk, R., Bowden-Jones, H., Verdejo-Garcia, A., & Clark, L. (2011). Impulsivity and cognitive distortions in pathological gamblers attending the UK National Problem Gambling Clinic: A preliminary report. Psychological Medicine, 41(12), 2625–2635.
MacLaren, V. A., Fugelsang, J. A., Harrigan, K. A., Dixon, M. J. (2011). The personality of pathological gamblers: A meta-analysis. Clinical Psychology Review, 31(6), 1057–1067.
Navas, J. F., Contreras-Rodríguez, O., Verdejo-Román, J., Perandrés-Gómez, A., Albein-Urios, N., Verdejo-García, A., & Perales, J. C. (2017). Trait and neurobiological underpinnings of negative emotion regulation in gambling disorder. Addiction, 112(6), 1086–1094.
Pallanti, S., & Salerno, L. (2014). Il gioco d'azzardo patologico. In A. Siracusano (Ed.), Manuale di Psichiatria (2nd ed., pp. 523–545). Roma: Il Pensiero Scientifico Editore.
Rogier, G., & Velotti, P. (2018a). Conceptualizing gambling disorder with the process model of emotion regulation. Journal of Behavioral Addictions, 7(2), 239–251.
Rogier, G., & Velotti, P. (2018b). Narcissistic implications in gambling Disorder: The Mediating Role of Emotion Dysregulation. Journal of Gambling Studies. https://doi.org/10.1007/s10899-018-9759-x.
Rogier, G., Picci, G., & Velotti, P. (2019). Struggling with happiness: A pathway leading depression to gambling disorder. Journal of Gambling Studies, 1–13.
Savvidou, L. G., Fagundo, A. B., Fernández-Aranda, F., Granero, R., Claes, L., Mallorquí-Baqué, N., et al. (2017). Is gambling disorder associated with impulsivity traits measured by the UPPS-P and is this association moderated by sex and age? Comprehensive Psychiatry, 72, 106–113.
Sheppes, G., Suri, G., & Gross, J. J. (2015). Emotion regulation and psychopathology. Annual Review of Clinical Psychology, 11, 379–405.
Steward, T., Mestre-Bach, G., Fernández-Aranda, F., Granero, R., Perales, J. C., Navas, J. F., et al. (2017). Delay discounting and impulsivity traits in young and older gambling disorder patients. Addictive Behaviors, 71, 96–103.
Suissa, A. J. (2011). Vulnerability and gambling addiction: Psychosocial benchmarks and avenues for intervention. International Journal of Mental Health and Addiction, 9, 12–23.
Velotti, P., Garofalo, C., Bottazzi, F., & Caretti, V. (2017a). Faces of shame: Implications for self-esteem, emotion regulation, aggression, and well-being. The Journal of Psychology, 151(2), 171–184.
Velotti, P., Garofalo, C., Callea, A., Bucks, R. S., Roberton, T., Daffern, M. (2017b). Exploring Anger Among Offenders: The Role of Emotion Dysregulation and Alexithymia. Psychiatry, Psychology and Law, 24(1), 128–138.
Velotti, P., Rogier, G., Civilla, C., Garofalo, C., Serafini, G. Amore, M. (2020). The Italian version of the DERS-P and levels of dysregulation of positive emotions across clinical samples. British Journal of Clinical Psychology. Manuscript under revision.
Weiss, N. H., Gratz, K. L., & Lavender, J. M. (2015). Factor structure and initial validation of a multidimensional measure of difficulties in the regulation of positive emotions: The DERS-positive. Behavior Modification, 39(3), 431–453.
Weiss, N. H., Forkus, S. R., Contractor, A. A., & Schick, M. R. (2018). Difficulties regulating positive emotions and alcohol and drug misuse: A path analysis. Addictive Behaviors, 84, 45–52.
Weiss, N. H., Risi, M. M., Bold, K. W., Sullivan, T. P., & Dixon-Gordon, K. L. (2019). Daily relationship between positive affect and drinking to cope: The moderating role of difficulties regulating positive emotions. The American Journal of Drug and Alcohol Abuse, 45(2), 189–198.
Whiteside, S. P., & Lynam, D. R. (2001). The five factors model and impulsivity: Using a structural model of personality to understand impulsivity. Personality and Individual Differences, 30(4), 669–689.
Whiteside, S. P., Lynam, D. R., Miller, J. D., Reynolds, S. K. (2005). Validation of the UPPS impulsive behaviour scale: a four-factor model of impulsivity. European Journal of Personality, 19(7), 559–574.
Zapolski, T. C., Cyders, M. A., & Smith, G. T. (2009). Positive urgency predicts illegal drug use and risky sexual behavior. Psychology of Addictive Behaviors, 23(2), 348–354.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The author declares that she has no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki declaration and its later amendments, or comparable ethical standards.
Informed Consent
was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rogier, G., Colombi, F. & Velotti, P. A brief report on dysregulation of positive emotions and impulsivity: Their roles in gambling disorder. Curr Psychol 41, 1835–1841 (2022). https://doi.org/10.1007/s12144-020-00638-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-020-00638-y