
Abstract
Previous studies suggest marital sexual infidelity (MSI) is growing among men and women. Also, social sciences literature has indicated that religious involvement and values reduce MSI occurrence. Religious persuasions and values remain critical in social life in Ghana and Nigeria, but little is known about religious influence on MSI and protection in both countries. In this study, the 2014 standard Demographic and Health Survey (DHS) data for Ghana (GDHS2014: 3,808 women and 1,967 men) and that of 2013 in Nigeria (NDHS2013: 22,220 women 8,292 men) were analysed within the framework of Durkheim’s theory of religion. Results suggest that MSI occurred more among women than men in Ghana (women = 12.9%, men = 9.9%) and Nigeria (women = 6.0%, men = 5.0%). Adjusted logistic regression analysis indicated that religion significantly predicted MSI in Ghana (p < 0.05) and Nigeria (p < 0.001). In Ghana, Other Christian women (OR = 0.5(CI0.4-0.7), p < 0.001; men (OR = 0.6(CI0.4-0.9), p < 0.05) and in Nigeria, Other Christian women (OR = 0.7(CI0.6-0.9), p < 0.001, and Muslims (women, OR = 0.3(CI0.3-0.4), p < 0.001; men (OR = 0.6(CI0.4-0.8), p < 0.01) had lower odds of reporting MSI experience relative to Catholic Christians. Women are likely more vulnerable to STIs in both countries due to higher MSI prevalence and relatively poor protective behaviour. Therefore, marriage counsellors should focus more on women and men across all religious persuasions. However, women and Catholic Christians require more attention to address the MSI and condom use challenges in Ghana and Nigeria. Social campaigns aiming to prevent MSI and STIs should be intensive in both countries across all religious persuasions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Infidelity is a global social phenomenon with varied dimensions, and it is a behaviour with health and social consequences. Infidelity increases the risk of sexually transmitted infections (STIs), domestic violence, separation and divorce among married partners (de Walque & Kline, 2011; Finchman & May, 2017; Nemeth et al., 2012; Okere & Ubani, 2020). As a result, focusing on MSI predictors is an important research goal. Evidence on the influencers of MSI is rich in non-African societies. Some of the influencers observed in previous studies include age at marriage, imposition of partner and marital satisfaction (Balderrama-Durbin et al., 2017; Jackman, 2015; Bahnaru et al., 2019). However, the subject has not been well explored in sub-Saharan Africa, with indications that it is on the rise among men and women (Okere & Ubani, 2020; Okobia, 2015).
Ghana and Nigeria are societies where religious persuasions and values remain essential in social life. The majority of the population are Christians and Muslims (National Population Commission [Nigeria] and ICF International, 2019; Ghana Statistical Services, Ghana Health Services, and ICF International, 2015). These popular religious groups are averse to MSI (as enshrined in various holy books). However, the potency of religious influence is unclear. In particular, little is known about religious influence on MSI and condom use during the act of MSI in Ghana and Nigeria. The choice of both countries rested on social and cultural congruence between the two countries. This study analysed nationally representative data sets in Ghana and Nigeria. One main objective and a sub-objective guided the analysis. It examined the potency of the influence of religious affiliation (an indicator of religion) on the occurrence of MSI and considered religious affiliation differentials in the association between MSI and condom use.
Background
Cheating, unfaithfulness, affairs, or stepping out are words/phrases describing various MSI forms (Finchman & May, 2017). Various terminologies suggest a behaviour wherein a married man or woman engages in sexual activities, including physical, emotional attachment (including on the internet), cuddling, kissing and virginal penetration outside his/her marriage (Finchman & May, 2017; Fye & Mims, 2019). Fye and colleagues gave an embracing definition of MSI as a violation of the ‘vow to remain sexually exclusive’ (p. 23). It is a growing reality that exposure to MSI among women and men is similar (Finchman & May, 2017). However, a relatively recent study suggests that the practice is more frequent among men than women, especially among the educated and civil servants (Asadu & Egbuche, 2020). Thus, further studies are required to reconcile the two positions on MSI experience sex differentials.
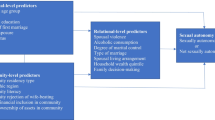
Predictors of MSI reported in the social science literature are age at marriage, imposition of partners, sexual incompatibility (Okere & Ubani, 2020), attitudes to infidelity and partners’ co-residency (Balderrama-Durbin et al., 2017; Jackman, 2015). Other predictors are the degree of commitment in marriage (Finchman & May, 2017; Selterman et al., 2018), level of satisfaction in marriage (Bahnaru et al., 2019; Finchman & May, 2017; McAllister et al., 2020; Onyekachi et al., 2015), alcohol consumption (Finchman & May, 2017; Selterman et al., 2018), cheating in previous relationships, partners individual personality (Finchman & May, 2017; Knopp et al., 2017; Selterman et al., 2018), lack of love and outright neglect of partner (Selterman et al., 2018).
In the research cycle, religious influence on MSI has not enjoyed much attention (Tuttle & Davis, 2015). A few studies on the role of religion in MSI have suggested that religious involvement and values are negatively associated with incidence of infidelity in romantic relationships (Dollahite & Lambert, 2007; Jeanfreau & Mong, 2018; Burdette et al., 2007; Esselmont & Bierman, 2014; Okobia, 2015). Also, Finchman and colleague observed in the United States that religious attendance prevents or reduces infidelity in romantic relationships (Finchman & May, 2017). In addition, studies have suggested that religious teachings and beliefs promote marital commitment, satisfaction, and attitude towards MSI; and marital commitment, satisfaction, and attitude prevent MSI experience (Bahnaru et al., 2019; Onyekachi et al., 2015; Yoosefi et al., 2016).
Moreover, studies have observed a negative association between religiosity and MSI. More religious couples are more likely to experience less incidence of MSI (Bahnaru et al., 2019; Finchman & May, 2017; Tuttle & Davis, 2015). Furthermore, studies have indicated that religiosity influences the occurrence of MSI indirectly. For instance, couples who indulge in praying together are likely to harvest better marital quality, including a higher degree of satisfaction, happiness and commitment that are inversely related to MSI (Bahnaru et al., 2019; McAllister et al., 2020; Jackman, 2015; Rayesh & Kalantar, 2018; Onyekachi et al., 2015).
The review has demonstrated that the hypothesis underpinning studies on religion and MSI is that religious involvement could directly or indirectly predict infidelity in sexual relationships. Nevertheless, an essential aspect of infidelity in marriage (or any romantic relationship) is the risk of STIs. Of course, condom use during such sexual acts can protect actors against the risk (Fiaveh, 2011). Generally, the ability of a woman to negotiate condom use varies by the nature of power relations in a relationship, the features of a woman and other behavioural factors (Feyisetan & Oyediran, 2020). The same considerations are likely to affect their male counterparts. For instance, a man’s perception that female sexual partners may object to his sexual demand if he does not agree to condom use could encourage use (Fiaveh, 2012). In addition, previous studies identified perception of sexual partners’ involvement with multiple sexual partners, concurrent sexual partnerships (Bowelo et al., 2019) as well as sexual-control perception in younger and middle age and risk perception (especially among males) (Fiaveh, 2011; Rodrigues et al., 2019) as factors influencing condom use during sex. How does condom use during sex (in a stable relationship or cheating sexual encounter) vary across religious persuasions, and are MSI and condom use related? Religion appears independently unrelated to modern contraceptive use (of which condom is part), but it does influence through socio-economic characteristics of women and men (Wusu, 2015). However, given the significance of religious values in West African societies and the health risks of MSI, a gap exists in the literature on the relationship between MSI and condom use variation across various religious persuasions. This study has it as a sub-objective to address this gap.
Therefore, to build on previous studies, this investigation examined the role of religious affiliation in MSI in the contexts of Ghana and Nigeria within the Durkheim’s theory of religion framework. In this light, the study sought to answer two questions. First, how potent is the influence of religious affiliation on MSI in Ghana and Nigeria? Second, what is the level of condom use during MSI in various religious affiliations in both countries?
Theoretical Underpinning
The Emile Durkheim’s theory of religion guided this study. In his sociology of religion, Durkheim described the aspects of social life classified as sacred as the essence of religion, and any social reality set apart (as sacred) draws reverence, awe and obligations amongst participants (Durkheim, 1912[1995]; Turner, 1999). In Durkheim’s view, the non-sacred aspects of social life are identified as profane; they are mundane or common. Sacredness is a function of definition, particularly concerning the profane. Any objective reality could be set apart and defined as sacred and society adores such as objects of worship (Evans-Pritchard, 1965). Durkheim argued that there is a ‘superior moral power’ that serves as the ultimate all religions look up to, and he posited it must be the society (Maryanski, 2014; Ritzer, 2008: 96) because it is what societies define as sacred that draws reverence and worship. However, the contemporary reality is that most religions consider that this superior moral power is God.
Furthermore, religious rituals and ceremonies in an overarching community (such as Church or Mosque) stand as the rallying point for participants and reinforce religious beliefs through regular reminders. In consonance with the functionalist perspective, Durkheim assumed that society is the superior moral power that institutes and keeps the sacred in place. It is central to every religion. In the light of the sacred, religion serves as the origin of morality (Alayi & Faridi, 2017). To Alayi and Faridi, various religious activities and ceremonies possess the capacity to promote religious beliefs, which, in most cases, has the doctrine of morality as an essential component. Thus, in the perspective of Durkheim, religion is an integration force in society through a mechanical solidarity mechanism that engenders the enthronement of morality and ethical values. Although most of the assumptions underlying Durkheim’s theory of religion have been heavily criticised (for instance, Goldenweiser 1917), the fundamental ideas are still relevant in modern society.
Thus, MSI is an inauspicious behaviour that falls into the profane relative to acceptable behaviour. What society considers acceptable behaviour exerts a controlling influence on individual participants (Evans-Pritchard, 1965). Virtually all religions are averse to infidelity in marriage. Therefore, one of the postulations verified in this study is that Christianity, Islam and Other religious persuasions in Ghana and Nigeria are most likely opposed to MSI. Their regular activities are likely to reinforce the profanity of such behaviour through constant reminders. Nevertheless, because the degree of sacredness attached to fidelity in marriage may vary from one religious’ group to the other, the influence of religious affiliations on MSI incidence is likely to vary (Burdette et al., 2007). As a result, different degrees of aversion to MSI may account for variability across religious groups and between countries. Thus, two hypotheses are tested in the study. Firstly, religious affiliation is likely to predict MSI in Ghana and Nigeria. Secondly, across religious persuasions, MSI experience and condom use are likely associated in Ghana and Nigeria.
Data and Methods
The 2014 standard DHS data sets for Ghana (GDHS 2014) and 2013 in Nigeria (NDHS 2013) were analysed, having obtained permission for use. The NDHS 2013 was selected to ensure an acceptable year gap between the two surveys analysed because GDHS 2014 was the latest in Ghana. The study population included women of reproductive age (15–49) and men aged 15 to 59. The DHS obtained ethical approval in both countries before conducting the surveys that generated the data sets analysed. Therefore, this study draws its ethical approval from that which the Measure DHS obtained in Ghana and Nigeria to conduct the surveys. The DHS used a probability sampling procedure to select nationally representative samples in Ghana and Nigeria (National Population Commission [Nigeria] and ICF International, 2014; Ghana Statistical Services, Ghana Health Services, and ICF International, 2015). This analysis involved 3,808 women and 1,967 men in Ghana and 22,220 women and 8,292 men in Nigeria who were currently in union. Currently in union here connotes women and men in formal marriage as at when Measure DHS conducted the surveys. The mentioned samples were extracted from individual women and men files in both countries. The data files analysed were derived by selecting female and male respondents of reproductive age in formal marriage. In addition, the analysis excluded pregnant female respondents to concentrate only on those who were presumed to be sexually active.
Religious affiliation was the indicator of religion used in this analysis, it was the study’s main independent variable and was derived from var/mv 130. The variable was recoded into four categories: Catholic Christians, Other Christians, Muslims and Others (representing all religious persuasions outside the mentioned affiliations). Unfortunately, the DHS did not measure religiosity in the two surveys, which could have been an additional indicator of religion. Nevertheless, religious affiliation sufficed as a measure of religion. The affiliation categories capture the religious persuasions and values predominant among respective adherents. Furthermore, the main dependent variable, MSI, was measured as sexual intercourse (anal, virginal or oral) with any other sexual partner other than the spouse. The indicator was derived from var/mv 767A (relationship with most recent sex partner). It was recoded ‘No = 0’ (with spouse) and ‘Yes = 1’ (with others).
Data analysis at univariate, bivariate, and multivariate levels was conducted. The analysis involved the SPSS software (version 20). The univariate level of analysis highlighted the respondent profiles encompassing all variables involved in the analysis, including independent, dependent and confounding factors. The bivariate analysis tested the association between religious affiliation and MSI using the Chi-square statistical technique. Similarly, a bivariate test was conducted on the association between MSI and condom use among respondents in the four religious’ affiliations. Unadjusted and adjusted logistic regression models examined the influence of religious affiliations on MSI. The adjusted logistic regression model controlled for the likely moderating influence of the confounding characteristics on the association between religion and MSI. Note that the confounding variables adjusted for were selected based on social sciences literature and rigorous analytical process. These factors include age, age at first marriage, condom use, currently working, highest level of education, household wealth index, living together with partner, place of residence, and Total Children Ever Born (CEB).
Results
Table 1 shows the percentage distribution of the respondents by selected characteristics and by sex and country. More than half of females and near half of males in Ghana were of Other Christian religious persuasion (non-Catholic Christians), while the majority indicated Islam religious persuasion in Nigeria. Others religious category constituted the minority of male and female respondents in Ghana and Nigeria. The table shows that more women than men in Ghana (women 12.9%) and in Nigeria (women = 6.0%) engaged in MSI. However, amongst the male respondents, the prevalence of MSI was higher in Ghana than in Nigeria. The poorest and poorer quantiles of household wealth recorded relatively higher proportions among women and men in Ghana. Conversely, the poorest and poorer categories had the highest proportions among women in Nigeria. However, higher proportions of men indicated the richer and richest wealth quantiles.
Also, most of the respondents were rural dwellers and lived together with their spouses. Most men and women in both countries indicated they were currently working. Condom use among men was higher than amongst women and higher in Nigeria than in Ghana amongst both women and men. The average age of respondents was higher among females and males in Ghana than in Nigeria. However, the mean ages for women and men exhibited large dispersions (with large standard deviations). A similar pattern was recorded in both countries concerning the age at first marriage. Conversely, the standard deviations for age at first marriage were relatively moderate. Also, the average CEB ranged between 3.9 and 4.7. Incidentally, the lower and upper limits of the fertility indicator emanated from Ghana.
Table 2 shows the results of the bivariate test of the association between religious affiliation and MSI in Ghana and Nigeria. The bivariate results suggested that religious affiliation and MSI were statistically and significantly associated among women in both countries (p < 0.001) and men in Ghana (P < 0.01) and Nigeria (p < 0.001). The results showed that more than one-third of females of Other Christians and Muslims reported exposure to MSI. In contrast, those of the Others religious category indicated the lowest level of exposure in Ghana. A similar pattern occurred among female respondents in Nigeria. Near half of Other Christians reported MSI experience, and more than one-third of Muslims indicated exposure to MSI. The Others religious category indicated the lowest exposure to MSI. Also, among male respondents, above one-third of Other Christians and one-fourth of Muslims in Ghana, about half of Other Christians and about one-third of Muslims reported MSI experience in Nigeria. Both Catholic Christians and Others religious category reported the lowest exposure to MSI.
Table 3 shows the logistic regression odds ratios on the association between religious affiliation and exposure to MSI. It is apparent that religious affiliation statistically and significantly predicted MSI amongst women and men in Ghana and Nigeria in unadjusted logistic regression models. Surprisingly, males and females of Other Christian religious persuasion in Ghana, Other Christian women and female and male Muslims in Nigeria indicated lower odds for reporting MSI compared to Catholic Christians in both countries. Similarly, after adjusting for the confounding factors (see Table 4), religious affiliation remained statistically and significantly related to MSI experience compared with Catholic Christians in Ghana and Nigeria. The odds ratios revealed that males and females in Other Christian religious group had lower odds of reporting exposure to MSI in Ghana relative to their Catholic Christian counterparts. In Nigeria, Other Christian females and Muslim female and male respondents were less likely to report MSI experience compared to the Catholic Christians. Across the two countries, it is striking to note that while Islam was not a significant predictor of MSI in Ghana it significantly predicted MSI among women and men in Nigeria. Also, the influence of Christianity (excluding Catholics) significantly influenced MSI in both countries.
Moreover, some confounding factors were statistically and significantly related to exposure to MSI that merit considering. There was a positive association between education and MSI experience amongst women and men in Ghana. The association was negative among men in Nigeria. Also, women and men who were currently working and those of rural residence were less likely to report exposure to MSI relative to those not working and of urban residence, respectively, only in Ghana. In addition, age at first marriage significantly predicted MSI experience (negatively) in Nigeria amongst women and wealth index significantly and positively predicted MSI among female respondents in both countries. Men who used condom in the last sex before respective surveys were three times (in Ghana) and five times (in Nigeria) more likely to report MSI experience compared to their counterparts who did not use it. Conversely, women who used condom in Nigeria were less likely to report MSI relative to those who did not indicate condom use.
Table 5 shows the results of the bivariate test of the association between engagement in MSI and condom use by the religious persuasions in Ghana and Nigeria. MSI and condom use were significantly associated among male Catholic Christians, Other Christians, and Others religious group in Ghana. In the case of Nigeria, exposure to MSI was significantly related to condom use among Catholic Christians and Other Christian women. The two variables were significantly associated in the four religious affiliations among their male counterparts. First, in Ghana, among male respondents who experienced MSI, members of Others and Catholic Christian persuasions reported the highest proportion of condom use. Their Other Christian counterparts indicated the lowest uptake of condom during last MSI. Second, amongst female respondents in Nigeria, about two of every hundred Catholic Christians and about one-tenth of Other Christians who engaged in MSI indicated condom use. Also, among male respondents, more than one-fifth of Other Christians, Catholic Christians and Muslims who experienced MSI indicated condom use in the last MSI act. The three religious categories reported the highest proportions of condom use in last MSI exposure in Nigeria (the magnitude of proportion in order of mention from first to third). The lowest proportion occurred among Others religious category.
Discussion
This study’s main objective was to examine the potency of religious influence on MSI occurrence in Ghana and Nigeria within the framework of Emile Durkheim’s theory of religion. First, the analysis in both countries reinforced the assertion that Ghana and Nigeria are societies where religious persuasions and values are still significant in social life. Most women and men reported affiliation with one of the two popular religious groups, namely Christianity (consisting of Catholic and non-Catholic Christians) and Islam. Second, MSI prevalence in the samples suggests that This analysis shows that the self-reported level of MSI was higher among women than men. Thus, the prevalence in Ghana and Nigeria deviated from the indication in social sciences literature. Previous studies reported that MSI was either similar or higher among men than women (Asadu & Egbuche, 2020; Finchman & May, 2017). A plausible explanation for this deviation could be that women disproportionately suffer the predisposing factors of MSI (Okere & Ubani, 2020; Finchman & May, 2017; Selterman et al., 2018). As a result, they are motivated to embrace MSI disproportionately too.
The bivariate analysis revealed that the association between religious affiliation and MSI was statistically significant in Ghana and in Nigeria. The general pattern was that MSI experience was slightly higher in Nigeria than in Ghana across the popular religious persuasions. Also, except for females in Ghana, Other Christians reported higher proportions of MSI experience than Muslims in both countries. An interesting angle of the result was the religious differential between both countries. First, the pattern in Ghana was inconsistent, whereas Other Christians reported consistently higher MSI experience than Muslims in Nigeria. Second, Other Christian men indicated higher MSI experience than their female counterparts. However, the reverse was the case among Muslims in Ghana and Nigeria.
The logistic regression models made the picture of the results more evident on the influence of religious persuasions on MSI experience in Ghana and Nigeria among women and men. The first point is that religious affiliation significantly predicted MSI exposure in both countries. Thus, the logistic regression models corroborated the bivariate analysis results. Therefore, the first hypothesis of the study is confirmed. Religious affiliation and exposure to MSI are statistically and significantly associated. The odds ratios indicated that women and men of non-Catholic Christianity in Ghana, female and male Muslims and non-Catholic Christian women in Nigeria were less likely to report MSI compared to their Catholic Christian counterparts. The inverse association was sustained after adjusting for the confounding factors. Therefore, findings suggest that the religious persuasions and values practised among Other Christians and Muslims are inversely related to MSI exposure relative to practice among Catholic Christians in Ghana and Nigeria. Thus, this study’s findings are consistent with previous studies that reported that involvement in religion is inversely associated with MSI prevalence (Dollahite & Lambert, 2007; Jeanfreau & Mong, 2018).
Furthermore, in the context of Emile Durkheim’s theory of religion, the results imply that the teachings and beliefs emphasised in the religious activities, ceremonies and rituals of non-Catholic Churches and Mosques are likely more potent to discourage involvement in MSI than in Catholic Churches (Burdette et al., 2007). In addition, the frequency of religious activities, ceremonies and rituals in the overarching communities of Churches, Mosques and other sacred places that are the rallying points for members of various religions vary. During the activities, ceremonies, and rituals, the campaign of aversion to MSI takes place. So more frequent activities, ceremonies, and rituals may guarantee regular reminders on the aversion to MSI, which may engender lower exposure to MSI. For instance, relative to Catholic Christianity, Islam usually has more obligatory daily religious activities, ceremonies, and rituals in Mosques. Similarly, non-Catholic Christian Churches engage more frequently in rituals and ceremonies. The variations in the opportunities for religious activities, ceremonies and rituals across the religious categories could account for differences in MSI prevalence among the participants.
Moreover, a sub-objective of this study was to examine condom use amongst respondents who engaged in MSI in Ghana and Nigeria. The analysis indicated that MSI experience and condom use across religious affiliations were statistically and significantly associated. Thus, the study’s second hypothesis that MSI experience and condom use are likely associated is confirmed. The analysis results suggested that condom use in MSI was generally poor across the four religious persuasions and among women and men in both countries. Yet the situation was poorer among women in Ghana and Nigeria. Conversely, in both countries, condom use in MSI experience in male samples was relatively striking. Catholic Christians and Others religious categories reported more condom use during MSI in Ghana. Other Christians, Catholics, and Muslims in Nigeria indicated more protective behaviour during MSI. Thus, the findings suggest that men who engaged in MSI in Ghana and Nigeria are less vulnerable compared to their women counterparts. A plausible explanation for men’s better protective behaviour in MSI experience is that they are likely to yield more to adopting condoms under the pressure of preventing sex refusal (Fiaveh, 2012). In addition, men are likely to dominate decision-making process in sexual relationships and possess a relatively higher socioeconomic status in West Africa. Consequently, men tend to be more assertive in negotiating condom use for protection during MSI (Feyisetan & Oyediran, 2020; Wusu, 2015).
Before concluding, this study suffered three limitations highlighted here to guide interpretation of the findings and further studies on the subject of religion and MSI in sub-Saharan Africa. First, because the data sets analysed were generated through cross-sectional surveys, the study did not aim to establish a cause-and-effect relationship. Hence, the focus is on proportions, associations and likelihood as portrayed by the odds ratios. Therefore, the interpretation of the findings should not assume cause-effect-relationship between religious affiliation and MSI. Second, the cross-sectional survey data analysed may appear relatively older. However, the analysis had to use the 2014 GDHS and 2013 NDHS because the 2014 GDHS was the last conducted in Ghana. To reduce the gap in years between Ghana and Nigeria data sets, the analysis involved the 2013 NDHS despite the existence of a newer data set (that is 2018NDHS). Third, religiosity was not measured in the data sets analysed, so the study was limited to using one indicator of religion. As a result, the study concentrated on the influence of religious affiliation on MSI and condom use in MSI experience across religious affiliations. Further studies on religious influence on MSI in sub-Saharan Africa should build on this analysis by measuring religiosity as an additional measure of religion, maybe more insights could be realised. Also, further studies may consider using qualitative methodology to explore needs in a marriage that spouses seek to address through MSI.
Conclusions
Despite the limitations highlighted above, the findings have contributed to knowledge on the potency of the influence of religious persuasions on MSI that further studies can build upon to generate further insights. The study has shown that a higher proportion of women reported MSI experience than men in Ghana and in Nigeria. Also, the indicator of religion significantly predicted MSI in both countries. Thus, religious influence on MSI prevalence was potent in Ghana and Nigeria. Religious persuasions such as what obtains among non-Catholic Christianity and Islam were inversely related to MSI in Ghana and Nigeria among women and men compared to Catholic Christians. Thus, spouses who identify with non-Catholic Christianity and Islam are less likely to experience MSI relative to their Catholic counterparts in Ghana and Nigeria. Also, women are likely more vulnerable to STIs in both countries due to higher MSI prevalence and relatively poor protective behaviour among them in both countries. Therefore, marriage counsellors should focus more on women and men across all religious persuasions. However, more attention should be concentrated on women and adherents of Catholic religious affiliation to address the growing MSI experience and poor condom use in Ghana and Nigeria. In addition, social campaigns to prevent MSI and STIs should be intensive in both countries across all religious persuasions among women and men. Religion may be an effective vehicle for actualising such campaign goals in Ghana and Nigeria.
References
Asadu, N., & Egbuche, M. (2020). Effect of marital infidelity on the family in Enugu State: A perception study of Ihe Owerri in Nsukka Local Government. RUJMASS, 6(1), 21–31
Alayi, M., & Faridi, A. (2017). Investigating marital infidelity from the perspective of Payame Noor and Azad Universities’ students in Bileh Savar county in 2015. Modern Applied Science, 11(8), 124–135. https://doi.org/10.5539/mas.v11n8p124
Bahnaru, A., Runcan, R., & Runcan, P. L. (2019). Religiosity and marital satisfaction. Revista de Asistenta Sociala, XVlll, 107–114
Balderrama-Durbin, C., Stanton, K., Snyder, D. K., Cigrang, J. A., Talcott, G. W., Slep, S. … Cassidy, D. G. (2017). The risk of marital infidelity across a year-long deployment. Journal of Family Psychology, 31(5), 629–634. https://doi.org/10.1037/fam0000281
Bowelo, M., Rakgoasi, S. D., & Keetile, M. (2019). Partner faithfulness and sexual reproductive health practices in Botswana: does perception of partner infidelity influence sexual risk behaviours of people aged 10–34 years? Journal of Biosocial Science (2019), 1–13. doi: https://doi.org/10.1017/S0021932019000622
Burdette, A. M., Ellison, C. G., Sherkat, D. E., & Gore, K. A. (2007). Are there religious variations in marital infidelity? Journal of Family Issues, 28(12), 1553–1581. https://doi.org/10.1177/0192513X07304269
de Walque, D., & Kline, R. (2011). Variations in condom use by type of partner in 13 subSaharan African countries. Studies in Family Planning, 42(1), 1–10
Dollahite, D. C., & Lambert, N. M. (2007). Forsaking all others: How religious involvement promotes marital fidelity in Christians, Jewish and Muslim Couples. Review of Religious Research, 48(3), 290–307
Durkheim, E. (1995). [1912]. The Elementary Forms of Religions, Translated by Karen Fields. New York: The Free Press
Esselmont, C., & Bierman, A. (2014). Marital formation and infidelity: an examination of the multiple roles of religious factors. Sociology of Religion, 75(3), 463–487. https://doi.org/10.1093/socrel/sru036
Evans-Pritchard, E. (1965). Theories of primitive religion. London: Oxford University Press
Feyisetan, B., & Oyediran, K. A. (2020). Can married or cohabiting women negotiate protective sex? Findings from Demographic and Health Surveys of two West African countries. Journal of Biosocial Science, 52(6), 785–808. https://doi.org/10.1017/S0021932019000798
Finchman, F. D., & May, R. W. (2017). Infidelity in romantic relationships. Current Opinion in Psychology, 13, 70–74
Fiaveh, D. Y. (2012). Condom myths and misconceptions: the male perspectives. Global Journal of Medical Research, 12(5), 42–52
Fiaveh, D. Y. (2011). Male perspective(s) on condom use: context of STI/HIV prevention in the University of Ghana community. Journal of Public Health and Epidemiology, 3(1), 17–27
Fye, M. A., & Mims, G. A. (2019). Preventing infidelity: A theory of protective factors. The Family Journal Counselling and Therapy for Couples and Families, 27(1), 22–30. https://doi.org/10.1177/1066480718809428
Ghana Statistical Service (GSS), Ghana Health Service (GHS), & ICF International (2015). Ghana Demographic and Health Survey 2014. Rockville, Maryland, USA: GSS, GHS, & ICF International
Goldenweiser, A. A. (1917). Religion and society: a critique of Emile Durkheim’s theory of the origin and nature of religion. The Journal of Philosophy, Psychology and Scientific Methods, 14(5), 113–124
Jackman, M. (2015). Understanding the Cheating Heart: What Determines Infidelity Intentions? Sexuality & Culture, 19, 72–84
Jeanfreau, M. M., & Mong, M. (2018). Barriers to marital infidelity. Marriage & Family Review, 55(1), 23–37
Knopp, K., Scott, S., Ritchle, L., Rhoades, G. K., Markman, H. J., & Stanley, S. M. (2017). Once a cheater, always a cheater? Serial infidelity across subsequent relationships. Arch Sex Behaviour, 46(8), 2301–2311. Doi: https://doi.org/10.1007/s10508-017-1018-1
Maryanski, A. (2014). The birth of the gods: Robertson Smith and Durkheim’s turn to religion as the basis of social integration. Sociological Theory, 32(4), 352–376. Doi: https://doi.org/10.1177/0735275114558943
McAllister, P., Henderson, E., Maddock, M., Dowdle, K., Fincham, F. D., & Braithwaite, S. R. (2020). Sanctification and cheating among emerging adults. Archives of Sexual Behaviour, 49, 1177–1188
National Population Commission [Nigeria], & ICF International. (2019). Nigeria Demographic and Health Survey 2018. Nigeria and Rockville, Maryland, USA: NPC & ICF International: Abuja
Nemeth, J. M., Bonomi, A. E., Lee, M. A., & Ludwin, J. M. (2012). Sexual infidelity as trigger for intimate partner violence. Journal of Women’s Health, 21(9), https://doi.org/10.1089/jwh.2011.3328
Okere, R. O., & Ubani, S. N. (2020). Rapid increase of infidelity among married women in Nigeria-causes and effects: Implication for counselling. European Journal of Education Studies, 7(10), 507–525
Okobia, F. N. (2015). Curbing promiscuous habits among Nigerians through religious studies. Journal of Religion and Human Relations, 7(1), 167–175
Onyekachi, B. N., Mbadugba, I. M., & Amazue, L. O. (2015). Roles of assertiveness, religious commitment and intimacy in marital satisfaction in a Nigerian sample. Nigerian Journal of Psychological Research, 11, 25–37
Rayesh, N., & Kalantar, S. M. (2018). The role of praying for the spouse and satisfaction of marriage in reducing infidelity. Mental Health, Religion and Culture, 21(1), 65–76. DOI: https://doi.org/10.1080/136746.2018.1447555
Ritzer, G. (2008). Sociological Theory. New York: McGraw-Hill Higher Education
Rodrigues, D. L., Prada, M., & Lopes, D. (2019). Perceived sexual sexual-control and condom use with primary and casual sex partners: age and relationship agreement differences in a Portuguese sample. Psychology & Health, 34(10), 1231–1249. doi: https://doi.org/10.1080/08870446.2019.1603384
Selterman, D., Garcia, J. R., & Tsapelas, I. (2018). Motivations for extradyadic infidelity revisited. The Journal of Sex Research, 56(3), 273–286. https://doi.org/10.1080/00224499.2017.1393494
Tuttle, J. D., & Davis, S. N. (2015). Religion, infidelity, and divorce: reexamining the effect of religious behaviour on divorce among long-married couples. Journal of Divorce & Remarriage, 56(6), 475–489. https://doi.org/10.1080/10502556.2015.1058660
Wusu, O. (2015). Religious influence on non-use of modern contraceptives among women in Nigeria: comparative analysis of 1990 and 2008 NDHS. Journal of Biosocial Science, 47(5), 593–612. doi: https://doi.org/10.1017/S0021932014000352
Yoosefi, N., Karimipour, B., & Amani, A. (2016). The study of religious beliefs, conflict resolution styles, and marital commitment with attitudes toward marital infidelity. Biannual Journal of Applied Counseling, 6(1), 47–64. https://doi.org/10.22055/jac.2017.20212.1380
Acknowledgements
A previous version of this paper was presented at the 29th IUSSP International Population Conference (Virtual) held in New Delhi, India, 5th -10th December 2021.
Funding
The study was not supported by any funding organisation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
I declare that there is no conflict of interest as far as this study is concerned.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wusu, O. The Potency of Religious Influence on Marital Sexual Infidelity: Evidence from Demographic and Health Surveys in Ghana and Nigeria. Sexuality & Culture 26, 1804–1818 (2022). https://doi.org/10.1007/s12119-022-09972-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12119-022-09972-8