
Abstract
Secretory carcinoma (SC) of the salivary gland is a new entity that shares the unique morphologic features and cytogenetic characteristics of the ETV6-NTRK3 fusion gene with its breast counterpart. Before identification of SC of the salivary gland, it was most frequently diagnosed as acinic cell carcinoma (AciCC). We retrospectively reviewed our own database of salivary gland tumors harboring microcystic and papillary architecture and/or secretory features that were originally diagnosed as AciCC. We selected nine cases of AciCC showing diffuse S-100 expression on immunohistochemistry (IHC). A recently diagnosed case of SC was included in the study as a reference sample. We performed IHC of S-100 and mammaglobin and ETV6 gene fluorescence in situ hybridization (FISH) in all cases. Seven cases were positive for both S-100 and mammaglobin, while five of the seven (71.4%) demonstrated ETV6 gene translocation by FISH. In the cases which did not co-express either S-100 or mammaglobin on IHC, ETV6 gene rearrangement was not shown on FISH. In conclusion, if a salivary gland tumor has morphologic features of SC with co-expression of S-100 and mammaglobin, ETV6 FISH can be performed to confirm the diagnosis of SC of the salivary gland.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Secretory carcinoma (SC) of the salivary gland is a recently described tumor type with unique characteristics. The first description of SC of the salivary gland reported by Skalova et al. [1] in 2010 included 16 cases of this new entity that shares morphologic and cytogenetic characteristics with its breast counterpart, including the ETV6-NTRK3-fusion gene, the product of t(12;15)(p13;q25). The morphologic features of SC described in previous studies include a microcystic and/or papillary-cystic architecture with abundant eosinophilic cytoplasm and uniform bland nuclei, and intraluminal secretory material [1, 2].
Following the initial publication describing SC of the salivary gland, a succession of studies has tried to reanalyze and reclassify some salivary gland tumor cases. Acinic cell carcinoma (AciCC); adenocarcinoma, not otherwise specified (NOS); polymorphous low-grade adenocarcinoma; mucoepidermoid carcinoma; and cystadenocarcinoma are candidate initial classifications of cases re-evaluated in a small number of recently published studies that were ultimately reclassified as SC of the salivary gland. The majority of these cases had been initially classified as AciCC [3,4,5,6,7].
The combination of S-100 and mammaglobin immunohistochemistry (IHC) has emerged as a primary screening tool to differentiate SC from its mimics. The majority of SCs show strong and diffuse cytoplasmic staining for S-100 and mammaglobin [8, 9]. However, detection of ETV6 gene translocation by fluorescence in situ hybridization (FISH) is still considered the gold standard for the diagnosis of SC. But when considering the high price of FISH, it is important to select the appropriate candidate cases.
The purpose of this study was to reanalyze our institutional database of salivary gland tumor cases for the presence of SC using morphologic criteria, IHC for mammaglobin and S-100, and FISH for detection of the ETV6-NTRK3 fusion gene product. These analyses suggest an appropriate approach for the diagnosis of salivary gland tumors showing secretory and microcytic features.
Materials and Methods
Case Selection
From a total of 60 cases of salivary gland tumors originally diagnosed as AciCC from 2005 to 2016 in the Department of Pathology, Severance Hospital, Korea, we selectively retrieved and reviewed nine cases. The selection criteria were (1) diffuse S-100 expression on IHC or (2) microcytic and papillary architecture and/or intraluminal eosinophilic material. One case of SC, which was diagnosed in 2016 by IHC for S-100 and mammaglobin and FISH for ETV6-NTRK3 gene translocation, was included in the study as a reference sample.
Immunohistochemistry
Immunohistochemical staining for mammaglobin (clone 31A5, 1:100 dilution, Cell Marque, Rocklin, CA, USA), S-100 (clone Z0311, 1:2000 dilution, Dako, Glostrup, Denmark) and DOG1 (clone SP31, Ready-to-Use, Cell Marque, Rocklin, CA, USA) was performed on 4-μm sections prepared from formalin-fixed, paraffin-embedded (FFPE) tissue using standard autostaining protocols on a Ventana Benchmark XT autostainer (Ventana Medical Systems, Inc., Tucson, AZ, USA) [10]. The samples were evaluated as whole section. All 10 cases, including nine candidates (cases 1–9) and one reference sample case (case 10), were subjected to IHC for S-100 and mammaglobin.
Fluorescence In Situ Hybridization (FISH)
FISH was performed on FFPE tissue sections using a commercially available ETV6 dual-color break-apart probe (07j77-001; Abbott Molecular, Des Plaines, IL, USA), as previously described [11, 12]. Cells with rearrangements for ETV6 had one normal fusion signal, one orange, and one green signal that were at a distance from each other. Tumors with more than 15% of cells exhibiting rearrangement were considered positive. All 10 cases, including nine candidates (cases 1–9) and one reference sample case (case 10), were subjected to FISH analyses for ETV6 gene translocation.
Statistical Analysis
The pathological data were analyzed with IBM SPSS version 20.0 (IBM, Armonk, NY, USA). Fisher’s exact test was applied in the statistical analyses. Statistical significance was defined as p < 0.05.
Results
SC with ETV6 Gene Translocation and Its Clinicopathologic Characteristics (Cases 6–10)
FISH studies revealed ETV6 gene translocation in five of the 10 cases, four of which were initially diagnosed as AciCC (Table 1; Fig. 1).

Evidence of ETV6 gene on FISH in SC (case 10) and a case mimicking SC (case 2). a SC showing one fused (yellow) and one split (red and green) signal, indicative of ETV6 gene translocation. b Mimic SC showing a negative ETV6 gene on FISH as evident by two fused signals in each cell
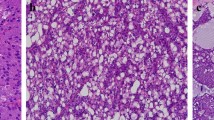
The ages of the five patients with tumors harboring ETV6 gene translocation ranged from 21 to 65 years (average: 42.8 years). Three of the patients were female. One of the tumors originated from the submandibular gland. Grossly, the tumors were generally well demarcated but not encapsulated, tan and light yellow cystic masses, and ranged from 0.9 to 2.9 cm across the greatest dimension. Histologically, all cases demonstrated a mixture of micropapillary, macro/microcystic, and solid architecture. The microcystic spaces were filled with characteristic eosinophilic material. The tumor cells had minimal nuclear atypia, with abundant eosinophilic or vacuolated cytoplasm (Fig. 2). No necrosis, perineural, or lymphovascular invasion was identified in any of the cases in our series.

SC with ETV6 gene translocation (case 10). a A photograph showing a well-demarcated, light yellowish mass with cystic changes. b, c Prominent macro/microcystic and papillary growth patterns. d Tumor cells with bland uniform nuclei, eosinophilic or vacuolated cytoplasm, and intraluminal secretory material. IHC profiles of the SC cases identified in this study. e All tumors show diffuse, strong positive staining for S-100. f Mammaglobin is positive in SC of the salivary gland, as this entity represents the salivary gland counterpart of breast secretory carcinoma
IHC studies demonstrated that all of the cases that had ETV6 gene translocation were positive for S-100 and mammaglobin (Fig. 2). In most cases, the staining was diffuse and strongly positive for both markers, except case 6, which was only focally positive for mammaglobin (Fig. 3). All cases were negative for DOG1 on IHC. However, ETV6 gene translocation measured by FISH and morphological analyses confirmed that all five of these cases were compatible with the diagnostic criteria for SC.

a Another SC (case 6) with cystic and papillary architecture. b, c The tumor consists of microcystic spaces filled with eosinophilic material, and some of the tumor cells are enlarged with abundant eosinophilic cytoplasm. The tumor shows diffuse, strong positive staining for S-100 (d), but only focally positive staining for mammaglobin (e). f However, it was confirmed as SC by ETV6 gene translocation on FISH
Lymph node metastasis was absent in both of the two confirmed cases on which node dissection was performed. No distant metastasis was identified at the time of diagnosis or during the follow-up period in any patients.
AciCC with no ETV6 Gene Translocation and Its Clinicopathologic Characteristics (cases 1–5)
In the remaining five cases mimicking SC morphology and S-100 expression, the original diagnosis of AciCC was not changed due to the lack of ETV6 gene translocation on FISH. In addition, two of five cases showed positive DOG1 immunoreactivity. The ages of these five patients ranged from 14 to 78 years (average 40.6 years). Two of the patients were female. Three of the tumors originated from the non-parotid salivary gland. Grossly, the tumors were well circumscribed masses and ranged from 1.0 to 2.4 cm across the greatest dimension. Histologically, diverse morphological features were observed, including areas of micropapillary and papillary architecture and cells with clear to eosinophilic cytoplasm.
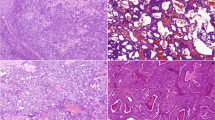
Among these five cases, two (cases 1 and 5) showed diffuse, strong positive staining for both S-100 and mammaglobin on IHC, but were ultimately negative for ETV6 gene translocation on FISH (Fig. 4). Case 1 was a solid mass from a minor salivary gland of a 43-year-old man. Histologically, this tumor was composed of papillary structures lined with bland uniform tumor cells. Case 5 was a cystic and solid mass from a parotid gland of a 78-year-old man. Histologically, it showed an overall architecture with papillary and micropapillary patterns, and it was surrounded by noticeable lymphocytic infiltration.

a A case mimicking SC (case 5) showing cystic and papillary structures. b Microcystic spaces with intraluminal materials. c Some tumor cells show abundant eosinophilic and vacuolated cytoplasm. The tumor shows diffuse, strong positive staining for both S-100 (d) and mammaglobin (e). f However, it was negative for ETV6 gene translocation on FISH
Expression Status of S-100 and Mammaglobin According to ETV6 Gene Translocation Status
A comparison of the S-100 and mammaglobin IHC and ETV6 FISH results is summarized in Table 2. Among the 10 cases of morphological candidates for SC, eight were positive for S-100 and seven were positive for mammaglobin on IHC. Seven cases showed co-expression of both markers. Of these seven cases that showed co-expression, five (71.4%) were positive for ETV6 gene translocation and two (28.6%) were negative for ETV6 gene translocation. None of the remaining three cases that did not co-express S-100 and mammaglobin on IHC showed ETV6 gene rearrangement on FISH. These three cases were either negative for both S-100 and mammaglobin (cases 3 and 4) or expressed only S-100 (case 2). The positive predictive value of S-100 and mammaglobin co-expression to predict EVT6 translocation was determined to be only 71.4%; however, the negative predictive value of no co-expression of S-100 and mammaglobin was determined to be 100% (Table 2).
Discussion
Secretory carcinoma (SC) is a newly described tumor that harbors recurrent translocation t(12;15)(p13;q25)/ETV6-NTRK3 similar to that of mesoblastic nephroma, infantile fibrosarcoma, acute myeloid leukemia, and secretory carcinoma of the breast [13, 14].
The first report of SC focused on features reminiscent of breast secretory carcinoma [1]. Recently, several studies have extended the clinical, histological, and immunohistochemical properties of SC [3, 5, 15, 16]. Indeed, some morphological features of SC overlap with those of other salivary gland tumors [1, 15, 17], including Acinic cell carcinomas(AciCC) and adenocarcinomas [15, 18]. Therefore, SC diagnosis in routine practice remains difficult by histological examination only. Using IHC of S-100 and mammaglobin along with appropriate morphological analysis has appeared to be a proxy method for a diagnosis of SC in most cases [9, 19]. However, the molecular detection of ETV6 gene rearrangement is the only confirmative diagnostic method of SC.
In this study, we retrospectively reviewed salivary gland tumor cases originally diagnosed as AciCC in our department from 2005 to 2016. Among a total of 60 AciCC specimens, we retrieved nine cases as SC candidates and performed IHC for S-100 and mammaglobin and ETV6 gene break-apart FISH. As a result of these analyses, seven cases demonstrated co-expression of S-100 and mammaglobin by IHC, five of which were positive for ETV6 gene translocation by FISH. Most cases (four of five) with ETV6 gene translocation revealed both diffuse and strong positive staining for S-100 and mammaglobin by IHC, apart from one case showing only focal positivity for mammaglobin. All cases that were negative for one or both of these markers were also negative for ETV6 gene translocation by FISH. In two cases, even though diffuse, strong expression of S-100 and mammaglobin on IHC was noted, ETV6 gene translocation by FISH was negative.
From the present findings, the positive predictive value of S-100 and mammaglobin co-expression to predict ETV6 gene translocation was determined to be no more than 71.4%; however, the negative predictive value of no co-expression of S-100 and mammaglobin was determined to be 100%. Therefore, an additional FISH study should be performed to confirm the occurrence of ETV6 gene translocation when salivary gland tumors show SC-like features and co-expression of S-100 and mammaglobin. If co-expression of S-100 and mammaglobin is not noted in the tumors with SC-like features, the possibility of EVT6 translocation is negligible, and an additional FISH study may be unnecessary.
Our study has some limitations, including that the sample size was too small to make statistical significance and only cases showing SC-like features and diffuse S-100 expression were included for further IHC analysis of mammaglobin and FISH analysis of EVT6 translocation. However, this enrichment process may have inadvertently caused a selection bias.
We tried to provide a practical approach for the diagnosis of these salivary tumors, especially regarding the necessity of further FISH in the case of a salivary gland tumor mimicking SC in daily practice, rather than robustly investigating EVT6 gene status for all salivary gland tumors regardless of morphological and immunohistochemical characteristics. As for cases that would be selected as candidates of SC after an initial enrichment process using S-100 and mammaglobin IHC, applying additional immunohistochemical and histochemical markers, such as discovered on gastrointestinal stromal tumor 1 (DOG1), amylase, and/or α-1-antitrypsin, would be also helpful to specify AciCC, which is a top differential diagnosis of SC [20,21,22]. In effect, we noted that DOG1 was expressed only in AciCC, and that no single case was expressed in SC cases. Thus, DOG1 immunostaining may also be helpful in determining SC candidates.
In agreement with several previous studies, our results indicate that the frequency of SC is highly underestimated. When diagnosing salivary gland tumors, especially with microcystic and papillary structures and intraluminal secretory material, it is important to consider the possibility of SC. In conjunction with morphological criteria, application of IHC for S-100 and mammaglobin can be a useful screening tool for SC. If the tumor is immunoreactive for both markers, the diagnosis of SC should be confirmed by the molecular detection of ETV6 gene translocation by FISH.
References
Skalova A, Vanecek T, Sima R, Laco J, Weinreb I, Perez-Ordonez B, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34:599–608.
Tavassoli FA, Norris HJ. Secretory carcinoma of the breast. Cancer. 1980;45:2404–13.
Chiosea SI, Griffith C, Assaad A, Seethala RR. Clinicopathological characterization of mammary analogue secretory carcinoma of salivary glands. Histopathology. 2012;61:387–94.
Chiosea SI, Griffith C, Assaad A, Seethala RR. The profile of acinic cell carcinoma after recognition of mammary analog secretory carcinoma. Am J Surg Pathol. 2012;36:343–50.
Connor A, Perez-Ordonez B, Shago M, Skalova A, Weinreb I. Mammary analog secretory carcinoma of salivary gland origin with the ETV6 gene rearrangement by FISH: expanded morphologic and immunohistochemical spectrum of a recently described entity. Am J Surg Pathol. 2012;36:27–34.
Fehr A, Loning T, Stenman G. Mammary analogue secretory carcinoma of the salivary glands with ETV6-NTRK3 gene fusion. Am J Surg Pathol. 2011;35:1600–2.
Lei Y, Chiosea SI. Re-evaluating historic cohort of salivary acinic cell carcinoma with new diagnostic tools. Head Neck Pathol. 2012;6:166 – 70.
Pinto A, Nose V, Rojas C, Fan YS, Gomez-Fernandez C. Searching for mammary analogue [corrected] secretory carcinoma of salivary gland among its mimics. Mod Pathol. 2014;27:30 – 7.
Bishop JA, Yonescu R, Batista D, Begum S, Eisele DW, Westra WH. Utility of mammaglobin immunohistochemistry as a proxy marker for the ETV6-NTRK3 translocation in the diagnosis of salivary mammary analogue secretory carcinoma. Hum Pathol. 2013;44:1982–8.
Li W, Lee MR, Choi E, Cho MY. Clinicopathologic significance of survivin expression in relation to CD133 expression in surgically resected stage II or III colorectal cancer. J Pathol Transl Med. 2017;51:17–23.
Bishop JA, Yonescu R, Batista D, Eisele DW, Westra WH. Most nonparotid “acinic cell carcinomas” represent mammary analog secretory carcinomas. Am J Surg Pathol. 2013;37:1053–7.
Bishop JA, Yonescu R, Batista DA, Westra WH, Ali SZ. Cytopathologic features of mammary analogue secretory carcinoma. Cancer Cytopathol. 2013;121:228–33.
Tognon C, Knezevich SR, Huntsman D, Roskelley CD, Melnyk N, Mathers JA, et al. Expression of the ETV6-NTRK3 gene fusion as a primary event in human secretory breast carcinoma. Cancer Cell. 2002;2:367–76.
Bourgeois JM, Knezevich SR, Mathers JA, Sorensen PH. Molecular detection of the ETV6-NTRK3 gene fusion differentiates congenital fibrosarcoma from other childhood spindle cell tumors. Am J Surg Pathol. 2000;24:937–46.
Skalova A. Mammary analogue secretory carcinoma of salivary gland origin: an update and expanded morphologic and immunohistochemical spectrum of recently described entity. Head Neck Pathol. 2013;7(Suppl 1):S30–6.
Urano M, Nagao T, Miyabe S, Ishibashi K, Higuchi K, Kuroda M. Characterization of mammary analogue secretory carcinoma of the salivary gland: discrimination from its mimics by the presence of the ETV6-NTRK3 translocation and novel surrogate markers. Hum Pathol. 2015;46:94–103.
Wang L, Liu Y, Lin X, Zhang D, Li Q, Qiu X, et al. Low-grade cribriform cystadenocarcinoma of salivary glands: report of two cases and review of the literature. Diagn Pathol. 2013;8:28.
Bishop JA. Unmasking MASC: bringing to light the unique morphologic, immunohistochemical and genetic features of the newly recognized mammary analogue secretory carcinoma of salivary glands. Head Neck Pathol. 2013;7:35–9.
Shah AA, Wenig BM, LeGallo RD, Mills SE, Stelow EB. Morphology in conjunction with immunohistochemistry is sufficient for the diagnosis of mammary analogue secretory carcinoma. Head Neck Pathol. 2015;9:85–95.
Said-Al-Naief N, Carlos R, Vance GH, Miller C, Edwards PC. Combined DOG1 and mammaglobin immunohistochemistry is comparable to ETV6-breakapart analysis for differentiating between papillary cystic variants of acinic cell carcinoma and mammary analogue secretory carcinoma. Int J Surg Pathol. 2017;25:127–40.
Chenevert J, Duvvuri U, Chiosea S, Dacic S, Cieply K, Kim J, et al. DOG1: a novel marker of salivary acinar and intercalated duct differentiation. Mod Pathol. 2012;25:919–29.
Hemminger J, Iwenofu OH. Discovered on gastrointestinal stromal tumours 1 (DOG1) expression in non-gastrointestinal stromal tumour (GIST) neoplasms. Histopathology. 2012;61:170–7.
Acknowledgements
The study was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2015R1D1A1A09059399).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest or funding to disclose.
Research Involving Human and Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
12105_2017_864_MOESM1_ESM.tif
Representative images of DOG1 immunohistochemical staining. A) Showed negative expression of DOG1 (case 6); B) Showed diffuse cytoplasmic expression of DOG1 (case 5). (TIF 12912 KB)
Rights and permissions
About this article

Cite this article
Woo, H.Y., Choi, E.C. & Yoon, S.O. Diagnostic Approaches for Salivary Gland Tumors with Secretory and Microcystic Features. Head and Neck Pathol 12, 237–243 (2018). https://doi.org/10.1007/s12105-017-0864-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-017-0864-4